
Abstract
Ethiopia has made improvements in the reduction of maternal mortality; the high burden of preeclampsia remains a concern in the Sidama region. This study aimed to measure the effect of preeclampsia on adverse maternal outcomes and identify risk factors among women with preeclampsia in Sidama region. A prospective open cohort study was conducted from August 8, 2019, to October 1, 2020. We enrolled a total of 1015 the pregnant women who had preeclampsia and normotensive women at ≥ 20 weeks of gestation and followed them until 42 days after delivery. A log-binomial logistic regression model was used to estimate the incidence of adverse maternal outcomes and its risk factors. There were 276 adverse maternal outcomes observed in the preeclampsia group compared to 154 adverse maternal outcomes in the normotensive group (P < 0.001). Women with severe features of preeclampsia had a 43% (aRR = 1.43, 95% CI 1.3–1.58) higher risk for adverse maternal outcomes compared to women without severe features of preeclampsia. Women without severe features of preeclampsia had a 39% (aRR = 1.39, 95% CI 1.2–1.76) higher risk for adverse maternal outcomes compared to women in the normotensive group. More adverse maternal outcomes occurred among women with preeclampsia after controlling for confounders.
Similar content being viewed by others
Introduction
Preeclampsia and eclampsia are two of the most common hypertensive disorders of pregnancy (HDPs)1. It is the second leading cause of direct maternal death and is directly responsible for 70,000 maternal deaths annually at the global level2. In low-and middle-income countries (LMICs), 10–15% of direct maternal mortalities were associated with preeclampsia and eclampsia in 20181. In Ethiopia in 2019, the pooled prevalence of maternal death was 4%3.
In Ethiopia, in 2018, the overall pooled prevalence of HDPs was 6.07%4. The same study identified variations in the level of HDPs across different geographical areas: the lowest prevalence was observed in Addis Ababa, the capital city of Ethiopia (5.41%), while the Sidama region in southern Ethiopia had a pooled prevalence of 10.13%4. Furthermore, in Ethiopia in 2020, the overall pooled prevalence of preeclampsia was 4.74%5.
Adverse maternal outcomes were noted in a study conducted in Ethiopia in 2020 that found a higher proportion of maternal deaths (4.5%) were observed among women with preeclampsia compared to normotensive women (1%)6. Another study conducted in Ethiopia in 2019 revealed that the top three adverse maternal outcomes were reported as maternal death (2.8%), eclampsia (6.6%), and renal failure (1.1%)7. Also in 2019, HDPs were the third leading causes of maternal deaths in southern Ethiopia (16%), followed by obstetric hemorrhage (39%), and anemia (28%)8. The majority of maternal deaths occurred after the pregnant women developed convulsions and delays in care seeking behavior9.
The overall pooled prevalence of HELLP (Haemolysis, elevated liver enzymes, low platelet count) syndrome was 13% in 20193. In southern Ethiopia, the main complications for admission were severe preeclampsia (51.8%), followed by postpartum hemorrhage (24.9%) in 2019. Eclampsia accounted for (70%) of pregnancy complications that occurred after 12 h of admission8. Women with severe preeclampsia have higher rates of organ dysfunctions, including kidneys, liver, brain, and the vascular system7.
A number of factors account for high rates of adverse maternal outcomes, including poor infrastructure, poor health-seeking behaviors and low socioeconomic conditions, shortage of supply and skilled manpower, weak referral systems, poor quality of care and access to timely obstetric care have all contributed to a higher proportion of maternal mortality in Ethiopia10,11.
The third Sustainable Development Goal plans to reduce the global maternal mortality rate to less than 70 per 100, 000 live births by 203012. In line with this, the government of Ethiopia has a plan to reduce maternal mortality from 401 to 140 per 100,000 live births in 203013. It has taken steps to strengthen engagement with key local and international sectors and stakeholders to address determinants of health14. Ethiopia recently replaced the previous four-visit focused antenatal care (ANC) model with the new ANC eight-contact model14. Furthermore, health facilities in Ethiopia have adopted a number of quality improvement measures such as providing 24-h services, including access to ambulances, and integrating the maternal deaths and near misses into regular practice to provide accurate information on causes of maternal deaths11.
Studies conducted in Ethiopia have not generated evidence that could be used by policymakers or practitioners because they did not include control groups or measure the risk of outcomes of interest and did not include socio-demographic variables such as maternal education status8,15,16. Another study done in southern Ethiopia was limited in estimating the risk of preeclampsia on adverse maternal outcomes because of poor ascertainment of exposures and outcomes using purposive sampling techniques17.
Moreover, this study’s findings will provide statistically valid epidemiological evidence for policy makers and implementers to reduce adverse maternal outcomes among women with preeclampsia and normotensive women. We aimed to measure the effect of preeclampsia on adverse maternal outcomes and identify risk factors among women with preeclampsia in Sidama region of southern Ethiopia.
Results
Socio-demographic and economic characteristics of study participants
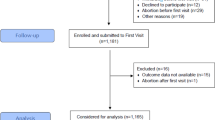
We enrolled 1,015 pregnant women out of 1,586 pregnant women who were approached to participate in the study. Thirty-one (1.6%) of the participants were lost-to follow up. Of these, 10 were from the preeclamptic group and 21 from the normotensive group. Fifty-five women refused to participate in the study. During the follow-up, eight normotensive women developed preeclampsia. We, thus, included these eight women in the exposed group (Fig. 1).

Flow-diagram of the overall study process in Sidama region, southern Ethiopia, August 8, 2019, to October 1, 2020.
The mean age of women with preeclampsia was 25.35 ± 4.76 years old, and 24.62 ± 4.55) for normotensive women. More than half (55.9%, 229/410) of women with preeclampsia were 16–24 years old compared to normotensive women (36.7%, 222/605), P < 0.001). Compared to normotensive women (4.5%, 27/605), a higher proportion of women with preeclampsia (10%, 41/410), P < 0.001) did not attend school. Compared to employed women (17.8%, 73/410) house wives had a higher proportion of preeclampsia (51.4% 211/410), P < 0.05) (Table 1).
Obstetric characteristics of women with preeclampsia and normotensive
A higher proportion of women with preeclampsia (45.6%, 187/410) was observed among women who were admitted at < 34 weeks compared to the normotensive group (10.9%, 66/605), P < 0.001). Compared to the normotensive group (36.5%, 221/605), a higher proportion of women with preeclampsia (41%, 168/410), P < 0.001) was observed in Yirgalem hospital. A higher proportion of cesarean delivery was observed among women with preeclampsia (45.1%, 185/410) compared to normotensive group (29.9%, 181/605), P < 0.001) (Table 2).
Incidence of adverse maternal outcomes among women with preeclampsia and normotensive women
There were 276 adverse maternal outcomes observed in the 410 preeclampsia group compared to 154 adverse maternal outcomes in the 605 normotensive group (P < 0.001). There were 4 maternal deaths were reported in the preeclampsia group compared to 0 deaths in the normotensive group (P < 0.05). Also, there were 53 antepartum hemorrhage was observed in the preeclampsia group compared to 24 antepartum hemorrhages in the normotensive group (P < 0.001). There were 90 acute kidney injury reported in the preeclampsia group compared to 12 acute kidney injury in the normotensive group (P < 0.001) (Table 3).
Women with or without severity features of preeclampsia on adverse maternal outcomes and other risk factors
In the bivariable log-binomial logistic regression model, the following variables were identified as candidate variables for multivariable log-binomial logistic regression analysis: age of women, women without severe features of preeclampsia, women who were admitted to the hospital at < 34 weeks, women with severe features of preeclampsia, maternal education and occupation, husband’s education, place of residence, wealth index, mode of delivery, gravidity, parity, eclampsia, magnesium sulphate treatment, and antihypertensive treatment.
After controlling for confounders, we identified significant risk factors for adverse maternal outcomes as women with severe features of preeclampsia, women without severe features of preeclampsia, age, wealth status, and place of residence.
Women with severe features of preeclampsia had a 43% (aRR = 1.43, 95% CI 1.3–1.58) higher risk for adverse maternal outcomes compared to women without severe features of preeclampsia. Women without severe features of preeclampsia had a 39% (aRR = 1.39, 95% CI 1.2–1.76) higher risk for adverse maternal outcomes compared to women in the normotensive group. Women who were admitted to the hospital at < 34 weeks had a 25% (aRR = 1.25, 95% CI 1.1–1.46) higher risk for adverse maternal outcomes compared to women who were admitted between 34 and 37 weeks.
Women whose age group was 16–24 years old were 76% (aRR = 1.76, 95% CI 1.3–2.4) at a higher risk for adverse maternal outcomes compared to women whose age group was ≥ 35 years old. Women with preeclampsia whose age group was 25–34 years old were 73% [aRR = 1.73, 95% CI 1.2–2.3] at a higher risk for adverse maternal outcomes compared to women whose age group was ≥ 35 years old. Women from lower wealth quintiles were 40% [aRR = 1.40, 95% CI 1.3–1.70] more at risk for adverse maternal outcomes compared to women from higher wealth quintiles. Women who resided in rural areas were 24% [aRR = 1.24, 95% CI 1.2–1.5] at risk for adverse maternal outcomes compared to women who resided in urban areas (Table 4).
Discussion
In this study, higher level of adverse maternal outcomes was observed in the preeclampsia group compared to normotensive group in the Sidama region after controlling for confounders. Maternal death, maternal ICU admission, postpartum hemorrhage, antepartum hemorrhage, and blood transfusion were higher in the preeclampsia group compared to the normotensive group. We identified significant risk factors for adverse maternal outcomes such as women who had severe features of preeclampsia, who were admitted to hospital at < 34 weeks of gestations, with low wealth status, younger women and who lived in rural areas.
More women with preeclampsia had adverse maternal outcomes compared to normotensive women. Our finding was higher than another prospective study in Uganda in 2020 that found 19.4% of adverse maternal outcomes18 and higher than a 2018 South African study that found 17.6% had kidney injury19. The variation among studies regarding incidence proportion of adverse maternal outcomes has been linked to the season the study was conducted in the severity of preeclampsia, and gestational age at diagnosis.
More maternal deaths were observed among women with preeclampsia compared to normotensive women in our study. This finding was lower than another study in Ethiopia in 2015 that found that (5%) of mothers died9, but lower than another study in Uganda in which 20 mothers died20. Raising awareness at community level among mothers during ANC visits regarding early signs of adverse outcomes and informing them of the referral system could help reduce delays in accessing treatment.
Maternal ICU admission was higher in the preeclampsia group compared to normotensive group. This finding was lower than the finding of another study conducted in the Brazil in 2014 (74.2% vs 21.9%)21, in Ghana (10.7%)22, and in Uganda (3%)23. This might due to poor knowledge of the communities on emergency obstetric conditions and their management and readiness among health facilities and preference for cultural remedies. Educating women on the importance of attending ANC services and the advantages of using such services can reduce maternal mortality. Understanding the physical and psychological stress that might make a woman at risk of the occurrence of preeclampsia could improve attendance.
Higher level of postpartum hemorrhage was reported in the preeclampsia group compared to normotensive group. This finding was supported by other studies21,24. Postpartum bleeding was more frequent in women with preeclampsia (22.9%) compared to normotensive women (13.9%)24. This finding was higher than another study conducted in Kenya in 2020 (4.4 versus 3.7%)25. This variation might be due to the introduction of magnesium-sulphate to treat women who have severe preeclampsia/eclampsia, thus leading to a reduction of incidence proportion of postpartum hemorrhage.
Higher level of antepartum hemorrhage was observed in the preeclampsia group compared to normotensive group. This finding was higher than another study done in Ethiopia in 2011 (5.1%) of APH26, and in Nigeria in 2020 (3.5%) of APH27. This could be because of women with severe preeclampsia associated with uterine blood vessel problems and higher risk for arterial dysfunction28. It is important to re-design and re-package existing interventions in the region that focus on improving ANC services, screening of elevated blood pressure and proteinuria in early pregnancy.
More women with preeclampsia had blood transfusions compared to normotensive women. This finding was similar with other studies conducted in Brazil in 2014, which showed that a higher proportion of blood transfusion was reported among women with preeclampsia compared to women in the normotensive group (52.9% vs 7.9%)21 and in southern Ethiopia in 2019 (57.8%)8. This could be because severe preeclampsia is related to a significant cause of cesarean delivery and cesarean delivery is also related to excessive blood loss which can be due to underlying preeclampsia-induced coagulopathy as well24. One of the important contributing factors to high maternal mortality in low-income countries is the late arrival to hospital at an irreversible stage of the disease29. It is essential at the health facility level to design a better tracking system for pregnant women for ANC visits and provide health facilities with MgSO4, which could prevent convulsions and severe outcomes in mothers.
Women with severe features of preeclampsia had a higher risk for adverse maternal outcomes compared to women without severe feature of preeclampsia. This finding was similar to a several other studies30,31,32. However, this finding was also lower than a study in Uganda in 2020 that found women with severe preeclampsia had higher rates of (93.2%) of adverse maternal outcomes compared to those without severe preeclampsia18. This could be because the women accessed ANC visits too late or too near their delivery date. The increased risk of maternal complications that was observed might be explained by the progression of preeclampsia to severe features and women who developed preeclampsia before 34 weeks30. Thus, the maternity care providers should ensure that the pregnant woman and her family are aware of the common dangerous symptoms and signs related to preeclampsia and are ready to act without delay to seek care in a health care facility.
Women who were admitted to the hospital at < 34 weeks had a higher risk for adverse maternal outcomes compared to women who were admitted between 34 and 37 weeks. This finding was supported by another study33 showed the early onset of preeclampsia was associated with an increased risk for adverse maternal outcomes compared to late-onset of preeclampsia33. Early-onset of preeclampsia is associated with severe placental dysfunction and fetal growth restriction compared to late-onset of preeclampsia33. Thus, maternal health care providers should be aware of screening and identifying high-risk pregnant women with respect to preeclampsia, which is used for timely initiation of appropriate management to reduce further adverse maternal complications.
Women with low wealth status were at higher risk for adverse maternal outcomes compared to women with a high wealth status. This finding was supported by another study in Zimbabwe in 2019 found that women having a low wealth status were a higher risk for adverse maternal outcomes37. This finding was supported by another study in Ethiopia the wealthiest women were 2 times more likely to have ANC visits than women in the poorest quintile38. This could be due to adolescent age group where the endocrinological and the immunological systems are yet immature and also due to poor nutrition.
Younger women were at higher risk for adverse maternal outcomes compared to older women. This finding was agreed with another study34. Younger, as evidence suggests that teenaged women are more likely to develop preeclampsia. Also, the ones who conceive immediately after coitarche too are at risk34. Women, who are younger or lower socioeconomic status, may be vulnerable to poorer quality of care and mistreatment during childbirth. This finding is contradicted with other studies study conducted in Tanzania and Ethiopia found that mothers aged > 35 years old had 2.6 and 2 times more likely to develop preeclampsia compared to younger mothers35,36. The variation among studies might be due to differences in marriage culture, believe and religious teachings on marriage which varies from one country to another and age categorization among studies also varied.
Women who resided in rural areas were higher risk for adverse maternal outcomes compared to women who reside in urban areas. This finding was similar with another study in Ethiopia29 found that women who lived in rural areas were might be a lower socioeconomic status than urban residents, which could lead to less health-seeking behavior. Low health-seeking behavior among pregnant women makes them less likely to attend antenatal care clinics, resulting in a delay in diagnosis and treatment associated with preeclampsia29. Other study in Ethiopia in 2022 showed that the odds of optimal ANC visit is 42% lower in rural women compared to women living in urban areas38. There is a need to focus on awareness creation on antepartum and intrapartum care and risk preparedness so rural women can seek care when they experience preeclampsia symptoms.
One limitation could be recall bias linked to gestational age, which was calculated based on the women’s recall of their last menstrual period. However, women who could not remember the approximate gestational age were given an ultrasound scan. Social desirability could have been present because data were collected in face-to-face interviews, which could have led to socially acceptable answers. This study is not generalizable as it was limited to one region of the country, and it was limited to women who received hospital care. It also measured short-term adverse maternal outcomes and the development of preeclampsia in among pregnant women, but it did not assess the risk of preeclampsia in later life, the risk of chronic hypertension, chronic renal failure, venous thromboembolism, ischemic heart disease, and cardiovascular events in later life, or other important health outcomes. However, it is unlikely that this limitation substantially affected our results. Because our study focused on one region and so is not representative of the whole country, but we carefully identified the potential sources of bias early in the design, validated the tool before data collection, and the percentage of pregnant women engaged in the study. Furthermore, this study has enabled us to identify the effect of preeclampsia on adverse maternal outcomes and risk factors in our setting, which can be used to predict and be used as a source of information in the whole country of Ethiopia in a similar socioeconomic setting.
Conclusion
In this study, more adverse maternal outcomes occurred among women with preeclampsia after controlling for confounders. A higher risk of maternal outcomes was observed among women with preeclampsia, especially among women with severe features of preeclampsia, and those admitted to hospital at < 34 weeks. This paper highlights the significantly elevated maternal risks associated with pre-eclampsia, especially when it has severe features. These effects could be detected and controlled early in pregnancy. Other risk factors for adverse maternal outcomes were identified as younger women, with low wealth status, and who lived in rural areas. Healthcare providers should raise awareness of preeclampsia in antenatal care clinics, focusing on younger women, low wealth status, and those living in rural areas.
Implications for future research
This study provides epidemiological evidence for the effect of preeclampsia on adverse maternal outcomes in clinical and public health practices. We recommend early screening of preeclampsia during pregnancy to facilitate more timely referral and initiation of early treatment of severe features of preeclampsia. Furthermore, a large cohort study should be conducted to evaluate other types of hypertensive disorders of pregnancy on the incidence of adverse maternal outcomes.
Methods
Study design and setting
A prospective open cohort study was conducted from August 8, 2019, to October 1, 2020 in the Sidama region of Ethiopia. In 2020, the population of the region was approximately 4 million. At that time, there were thirteen public hospitals, 138 health centers, and 540 health posts providing maternal, newborn, and child health services. In 2020, approximately 132,031 pregnant women attended ≥ 4 antenatal care visits (ANC), and 127,585 births were assisted by skilled birth attendants. Out of the 13 hospitals that are found in the region, we enrolled participants from seven of the hospitals, including Adare, Hawassa, Yirgalem, Hula, Bona, Chuko, and Daye hospitals.
Study population
The participants of this study were women with preeclampsia and normotensive women who were enrolled at ≥ 20 weeks of gestation until the 37th week and they were followed until 42 days after delivery the enrolled woman’s outcome status was ascertained. During the follow-up, 253 women with preeclampsia and normotensive women were admitted to the hospitals at < 34 weeks of gestation, and 762 women with preeclampsia and normotensive women were admitted to the hospitals at 34–37 weeks of gestation.
Eligibility criterion
Inclusion criteria
Pregnant women with hypertension plus proteinuria, mild hypertension and evidence of organ dysfunction, severe hypertensive without proteinuria, and evidence of organ dysfunction were included in the study39,40. Pregnant women with preeclampsia and normotensive women were selected by health care providers: general medical practitioners, emergency surgical officers, or obstetricians/gynecologists during the follow-up.
Exclusion criteria
Pregnant women who had known chronic hypertension before 20 weeks of gestation or women who were already on antihypertensive medication, women who had known chronic renal disease, known history of diabetes mellitus, known history of preeclampsia, family history of diabetes mellitus, family history of preeclampsia, and family history of hypertension were excluded from the study41,42.
Operational definitions
The diagnosis of adverse maternal outcomes was supported by guidelines of the Obstetrics Management Protocol for Hospitals in Ethiopia and was based on the recent International Society for the Study of Hypertension in Pregnancy in 202139,40. Antepartum hemorrhage was defined as vaginal bleeding during labor beginning in the 28th week of pregnancy39. Postpartum hemorrhage was defined as vaginal bleeding lasting more than 500 ml after childbirth and was diagnosed by any of the following: visual estimation, 10% reduction of hemoglobin from antepartum, a blood loss that needs transfusion39.
Acute kidney injury (AKI) was defined as a syndrome characterized by a rapid (hours to days) deterioration of kidney function or was a clinical syndrome characterized by an abrupt decline in glomerular filtration rate and the accumulation of nitrogenous waste products. AKI was defined as an increase in serum creatinine of 0.3 mg/dl within 48 h or in urine volume of 0.5 ml/kg/hr for 6 h. Although AKI diagnosis also depends on the decision-making process of the clinician rather than underlying renal function43. Maternal ICU admission was defined as admission to a critical care area providing at least additional monitoring and interventions for women who had severe complications44. Maternal death was defined as the death of a woman while pregnant or within forty-two completed days of termination of pregnancy, irrespective of duration and site of pregnancy, from any cause related to or aggravated by the pregnancy or by its management but not due to accidental or incidental causes40.
Sample size and sampling
The sample size was calculated using EPINFO version 7. We considered the following assumptions for sample size calculations: women who had anemia45, the ratio of exposed to unexposed group (1 to 1), the proportion of anemia among women with preeclampsia was 10.835%, the proportion of anemia among normotensive women was 16%. The sample size was estimated to be 1,586 cohort of pregnant women were enrolled, accounting for a design effect of two and 10% loss to follow-up. We also assumed a two-sided confidence level of 95% with a power of 80%.
A two-stage cluster sampling techniques were used to recruit study participants. In the first stage, seven of the thirteen hospitals were selected using the simple random sampling technique. In the second stage, women with preeclampsia and normotensive women and maternal conditions were selected from the cohort of pregnant women using a cluster sampling technique.
Exposure ascertainments
We ascertained exposure of interest supported by guidelines of the Obstetrics Management Protocol for Hospitals in Ethiopia in 2021 and on the recent International Society for the Study of Hypertension in Pregnancy39,40. The main exposure variable for this study was preeclampsia (preeclampsia with or without severity features). Preeclampsia was defined as the presence of proteinuria (≥ 1 + or 0.3 g/L) and hypertension (≥ 140/90 mmHg) on two occasions at least 4 h apart detected after the 20th week of gestation in a previously normotensive woman. Preeclampsia without severe features was defined as one or more of the following conditions: absence of systemic involvement and raised BP ≥ 140/90 mmHg plus 24-h urine protein ≥ 300 mg/24 h or urine dipstick > + 1after 20 weeks of gestation in previously normotensive women. Preeclampsia with severe features was defined as one or more of the following conditions: BP ≥ 160/110 mmHg, hepatic dysfunction, pulmonary edema and/altered mental status, headache, blurred vision, right upper quadrant pain, blindness, seizures and disseminated intravascular coagulation, and elevated liver enzymes39. Eclampsia was diagnosed as the presence of convulsions that could not be attributed to other causes in a woman with preeclampsia. Normotensive women were pregnant women having a (BP) < 140/90 mmHg with ≥ 20 weeks of gestation or who did not develop preeclampsia and proteinuria. Gestational age was calculated based on a woman’s recall of her last menstrual period. However, an ultrasound scan was used for those women who could not remember their last menstrual period39.
Outcome variable
Adverse maternal outcomes were defined as the occurrence of at least one of the following conditions: maternal death, maternal ICU admission, blood transfusion, postpartum hemorrhage, acute kidney injury and antepartum hemorrhage.
Data collection
Before data collection, we validated the data collection tool46. Two bilingual translators (speakers of both Sidamic and English languages) were selected to translate the information into the Sidamic language in a way that more accurately reflected the tone of the language. The translations were compared and discrepancies were noted during the translation process. Poorer wording choices were identified and resolved in a discussion between the translators.
The back translations were done by two experts in the source language (English). Face and content validation of the tool was done by a panel of experts (midwife experts, epidemiologists, and gynecologists). The panel of experts independently assessed the tool for readability, intelligibility, clarity, and ease of use. The internal consistency for each dimension was checked using Cronbach’s alpha (Cronbach’s alpha = 0.98).
In the first pilot test, conducted in a non-study area, all participants responded to all items in the data collection tool and marked them correctly. No missing items were found. Data collectors also reported no difficulty in asking the questions, and no participant reported having any problem understanding the items. The tool was tested for the second time two weeks after the first measurement. The two-week test–retest reliability result was shown to have a good correlation with reliable strategies to assess these point scores (Intraclass Correlation Coefficients (ICC) for agreement of 0.78; P < 0.001) because the ICC value was found to be in the range of 0.75 to 0.9, indicating good reliability47.
Trained midwives conducted face-to-face interviews at antenatal care clinics using the pre-tested validated tool. Besides, a checklist was used to collect information from the maternal records of women with preeclampsia and normotensive women in each hospital. We collected socio-demographic information and clinical and laboratory variables linked to maternal and perinatal outcome status. The data collection procedures were supervised by three Maternal and Child Health maternity and reproductive health professionals.
Outcome ascertainments
Adverse maternal outcome was ascertained by an obstetrician and gynecologist and trained midwives. Client medical registration was also used to retrieve adverse maternal outcome status. For those discharged, maternal condition was ascertained on the postnatal care follow up appointment and those who did not show up for this follow up, phone call was used.
Confounders ascertainment
Covariates
These confounders were identified by prior theoretical knowledge and literatures. Potential confounding variables are those variables that have an association with an exposure variable and the outcomes. The following covariates were considered as possible confounders: Women who developed preeclampsia differed in maternal age, gravidity, history of chronic hypertension (personal or family), personal history of preeclampsia, history of diabetes, and family history of preeclampsia from those who did not develop preeclampsia (P > 0.05)48,49,50,51.
Strategy to control confounders at the design stage
When pregnant women disappear from either the exposed or non-exposed group or both, might bias be introduced? In our study, pregnant women's loss means dropping out of the follow-up because of death or complications during ANC visits, which was considered as missing completely at random. We used the following solution to minimize it. Maternal condition was determined for those discharged to home at the postnatal care follow-up appointment, and those who did not show up for this follow-up were contacted by phone. To minimize misclassification bias, consideration was given at the design stage and by using different sources of information for exposure and outcome ascertainment. In those who couldn’t recall their last normal menstrual period, gestation age was estimated by using ultrasound. To minimize confounds, study restrictions were implemented during the design stage.
Statistical analysis
Data were cleaned, coded and analyzed using Stata 14. We identified outliers and missing values and checked data consistency using the original questionnaire for the responses using participants’ code numbers. Mean and standard deviations were computed for continuous variables. Frequencies and percentages were computed for categorical variables. An incidence proportion of adverse maternal outcomes were conducted on women who had preeclampsia and normotensive women. Cross tabulation was also performed to test the relationship of exposure variables with the outcome variable. A chi-squared test was used to compare categorical variables between women with preeclampsia and normotensive women.
Principal component analysis was computed and used for wealth index computation and was ranked into three groups as low, middle, and high. A composite measure of the household's cumulative living standard was calculated by using data on household ownership of selected assets, like various household assets and means of transportation. Different items for urban and rural areas were computed separately. We included 21 items for rural residents and 16 items for urban residents. The suitability of data was computed by using Bartlett’s test of Sphericity and the Kaiser–Meyer–Olkin (KMO) measure of sample adequacy52. The KMO > 0.6 was used to confirm the sample adequacy for factor analysis52.
A multivariable log-binomial logistic regression model was performed to identify the risk factors for adverse maternal outcomes. According to Hosmer and Lemeshow, a variable with a P value < 0.25 was recommended as a screening criterion for the selection of candidate variables used in a multivariable log-binomial logistic regression model53. This confirmed that insignificant variables from the first step were reanalyzed in later steps. Moreover, the candidate variables were also considered based on the subject matter expertise of professionals such as gynecologists, obstetricians, epidemiologists, and statisticians who were working as supervisors and who provided more subject matter expertise to improve the modeling process substantially. Indeed, this insight from subject matter experts substantially improved the modeling process53. A variable with a P value of < 0.05 was used to identify statistically significant risk factors for adverse maternal outcomes. Relative risk with a 95% confidence interval was reported.
We checked for multicollinearity among contributing factors using a variance inflation factor at a cutoff point of ten54. We confirmed that there was no collinearity among predictors. The goodness of fit was tested using the Hosmer–Lemeshow test. The predictor that was greater than the significance level (P value > 0.05) was accepted55. This indicates that the observed model did not significantly differ from the expected model.
Ethical considerations
This study was reviewed and ethical approval was issued by the Institutional Review Board of the University of Gondar with R.No.O/V/P/RCS/044/2019 in March 2019. All participants signed an informed consent document before study participation began. Pregnant women having abnormal clinical and laboratory results were referred for treatment. Women with severe hypertension were provided with antihypertensive treatment; those with convulsions were given appropriate treatment. We confirmed that all methods were carried out in accordance with relevant guidelines and regulations.
Data availability
The data that supports the findings of this study is available from the corresponding author upon reasonable request in the form of Stata Version 14.
References
Anselmini, M. et al. Perinatal outcome of hypertensive pregnant women is related to the severity of preeclampsia. Clin. Biomed. Res. 38(2), 116–122 (2018).
Townsend, R., O’Brien, P. & Khalil, A. Current best practice in the management of hypertensive disorders in pregnancy. Integr. Blood Press. Control 9, 79–94 (2016).
Mersha, A. G., Abegaz, T. M. & Seid, M. A. Maternal and perinatal outcomes of hypertensive disorders of pregnancy in Ethiopia: Systematic review and metaanalysis. BMC Pregnancy Childbirth 19(458), 1–12 (2019).
Berhe, A. K., Kassa, G. M., Fekadu, G. A. & Muche, A. A. Prevalence of hypertensive disorders of pregnancy in Ethiopia: A systemicreview and meta-analysis. BMC Pregnancy Childbirth. 181, 34. https://doi.org/10.1186/s12884-018-1667-7 (2018).
Tesfa, E. et al. Prevalence and determinants of hypertensive disorders of pregnancy in Ethiopia: A systematic review and meta-analysis. PLoS ONE 15(9), e0239048 (2020).
Hinkosa, L., Tamene, A. & Gebeyehu, N. Risk factors associated with hypertensive disorders in pregnancy in Nekemte referral hospital, from July 2015 to June 2017, Ethiopia: Case-control study. BMC Pregnancy Childbirth 20, 16 (2020).
Legesse, A. Y., Berhe, Y., Mohammednur, S. A., Teka, H. & Goba, G. Prevalence and determinants of maternal and perinatal outcome of preeclampsia at a tertiary hospital In Ethiopia. Ethiop. J. Reprod. Health (EJRH) 11(4), 8 (2019).
Wakgar, N., Dulla, D. & Daka, D. Maternal near misses and death in Southern Ethiopia: A retrospective study. Ethiop. J. Reprod. Health 11(2), 9 (2019).
Berhan, Y. & Endeshaw, G. Maternal mortality predictors in women with hypertensive disorders of pregnancy: A retrospective cohort study. Ethiop. J. Health Sci. 25(1), 89–98 (2015).
National Strategy for Newborn and Child Survival in Ethiopia Maternal and Child Health Directorate Federal Ministry of Health 2015/16–2019/20
Gebrehiwot, Y. & Tewolde, B. T. Improving maternity care in Ethiopia through facility based review of maternal deaths and near misses. Int. J. Gynecol. Obstet. 127, S29–S34 (2014).
Liu, L. et al. Global, regional, and national causes of under-5 mortality in 2000–15: An updated systematic analysis with implications for the Sustainable Development Goals. Lancet 388(10063), 3027–3035 (2016).
Health Sector Transformation Plan II HSTP II 2020/21–2024/25 Minstry of Health Ethiopia 2021
National Antenatal Care Guideline in Ethiopia | February 2022. available at accessed at October 4. https://e-library.moh.gov.et/library/wp-content/uploads/2022/03/Anc-Guideline_Feb-24-2022
Melese, M. F., Badi, M. B. & Aynalem, G. L. Perinatal outcomes of severe preeclampsia/eclampsia and associated factors among mothers admitted in Amhara Region referral hospitals, North West Ethiopia. BMC Res. Notes. 12, 147. https://doi.org/10.1186/s13104-019-4161-z (2019).
Asseffa, N. A. & Demissie, B. W. Perinatal outcomes of hypertensive disorders in pregnancy at a referral hospital, Southern Ethiopia. PLoS ONE 14(2), e0213240 (2019).
Deneke, Y. S., Afework, M. F., Tessema, T. T., Misganaw, C. & Taye, H. Cause, magnitude and contributing factors for maternal death in selected hospitals in snnpr between 2007/2008 and 2009/2010. Int. J. Med. Health Sci. Res. 1(12), 155–167 (2014).
Lugobe, H. M. et al. Risks of adverse perinatal and maternal outcomes among women with hypertensive disorders of pregnancy in southwestern Uganda. PLoS ONE 15(10), e0241207 (2020).
Nathan, H. L. et al. Maternal and perinatal adverse outcomes in women with pre-eclampsia cared for at facility-level in South Africa: A prospective cohort study. J. Global Health 8(2), 020401 (2018).
Nakimuli, A. et al. The burden of maternal morbidity and mortality attributable to hypertensive disorders in pregnancy: A prospective cohort study from Uganda. BMC Pregnancy Childbirth 16(205), 1–8 (2016).
Zanette, E. et al. Maternal near miss and death among women with severe hypertensive disorders: a Brazilian multicenter surveillance study. Reprod. Health 11(4), 1–11 (2014).
Adu-Bonsaffoh, K., Obed, S. A. & Seffah, J. D. Maternal outcomes of hypertensive disorders in pregnancy at Korle BuTeaching Hospital, Ghana. Int. J. Gynecol. Obstet. 127, 238–242 (2014).
Oliveira-Neto, A., Parpinelli, M. A., Cecatti, J. G., Souza, J. P. & Sousa, M. H. Sequential organ failure assessment score for evaluating organ failure and outcome of severe maternal morbidity in obstetric intensive care. Sci. World J. 2012, 172145 (2012).
Eskild, A. & Vatten, L. J. Abnormal bleeding associated with preeclampsia: A population study of 315,085 pregnancies. Acta Obstetricia et Gynecologica 88, 154–158 (2009).
Gupta, M., Greene, N. & Kilpatrick, S. J. Timely treatment of severe maternal hypertension and reduction in severe maternal morbidity. Pregnancy Hypertens. 14, 55–58 (2018).
Johnson, K. M. et al. Hypertensive disease in pregnancy in Botswana: Prevalence and impact on perinatal outcomes. Int. J. Women’s Cardiovasc. Health 6, 418–422 (2016).
Ayogu, M. E., Akaba, G. O., Offiong, R. A., Adewole, N. D. & Ekele, B. A. Risk factors for hypertensive disorders of pregnancy in Abuja, Nigeria: A prospective case-control study. Trop. J. Obstet. Gynaecol. 37, 46–52 (2020).
Debelew, G. T. Magnitude and determinants of perinatal mortality in Southwest Ethiopia. Hindawi J. Pregnancy Article ID 6859157, 7 (2020).
Gedefaw, G., Alemnew, B. & Demis, A. Adverse fetal outcomes and its associated factors in Ethiopia: A systematic review and meta-analysis. BMC Pediatr. 20(269), 1–12 (2020).
Maqueo, M., Chavezazuela, J. & Dosaldelavega, M. Placental pathology in eclampsia and preeclampsia. Obstet. Gynecol. 24, 350–356 (2007).
Belay Tolu, L., Yigezu, E., Urgie, T. & Feyissa, G. T. Maternal and perinatal outcome of preeclampsia without severe feature among pregnant women managed at a tertiary referral hospital in urban Ethiopia. PLoS ONE 15(4), e0230638 (2020).
Chen, Q., Shen, F., Gao, Y. F. & Zhao, M. An analysis of expectant management in women with early-onset preeclampsia in China. J. Hum. Hypertens. 29(6), 379–384 (2015).
Kaze, F. F. et al. Post-partum trend in blood pressure levels, renal function and proteinuria in women with severe preeclampsia and eclampsia in sub-Saharan Africa: A 6-months cohort study. BMC Pregnancy Childbirth 14, 134 (2014).
Endeshaw, G. & Berhan, Y. Perinatal outcome in women with hypertensive disorders of pregnancy: A retrospective cohort study. Int. Sch. Res. Not. 2015, 8. https://doi.org/10.1155/2015/208043 (2015).
Mrema, D., Lie, R. T., Ostbye, T., Mahande, M. J. & Daltveit, A. K. The association between prepregnancy body mass index and risk of preeclampsia: A registry based study from Tanzania. BMC Pregnancy Childbirth 18(1), 56 (2018).
Mohammedseid, S. I., Megersa, T. N., Kumbi, S. & Ayalew, M. B. Maternal outcomes of pre-eclampsia in an Ethiopian Gynecologic Hospital. Ann. Med. Health Sci. Res. 7(3), 16–21 (2017).
Ngwenya, S., Jones, B. & Mwembe, D. Determinants of adverse maternal and perinatal outcomes in severe preeclampsia and eclampsia in a low-resource setting, Mpilo Central Hospital, Bulawayo, Zimbabwe. BMC Res. Notes 12, 298 (2019).
Yehualashet, D. E., Seboka, B. T., Tesfa, G. A., Mamo, T. T. & Seid, E. Determinants of optimal antenatal care visit among pregnant women in Ethiopia: A multilevel analysis of Ethiopian minidemographic health survey 2019 data. Reprod. Health 19, 61 (2022).
Obstetrics Management Protocol for Hospitals. MOH, Ethiopia 2021.
The International Society for the Study of Hypertension in Pregnancy. The hypertensive disorders of pregnancy: ISSHP classification, diagnosis & management recommendations for international practice (Pregnancy Hypertension, 2018). http://www.isshp.org/guidelines.ISSHP
Gunnarsdottir, J., Akhter, T., Högberg, U., Cnattingius, S. & Wikström, A. K. Elevated diastolic blood pressure until mid-gestation is associated with preeclampsia and small-for-gestational-age birth: a population-based register study. BMC Pregnancy Childbirth 19, 186 (2019).
Nguefack, C. T. et al. Comparison of materno-fetal predictors and short-term outcomes between early and late onset preeclampsia in the low-income setting of Douala, Cameroon. Int. J. Gynaecol. Obstet. 142(2), 228–234 (2018).
Ostermann, M. & Joannidis, M. Acute kidney injury 2016: Diagnosis and diagnostic workup. Ostermann Joannidis Crit. Care 20, 299 (2016).
Intensive Care Society, Levels of Critical Care for Adult Patients (2009).
Tura, A. K. et al. Severe hypertensive disorders of pregnancy in Eastern Ethiopia: comparing the original WHO and adapted sub-Saharan African maternal near-miss criteria. Int. J. Women’s Health 12, 255–263 (2020).
Jikamo, B. Adefris, M. Azale, T. et al. Cultural adaptation and validation of the Sidamic version of the World Health Organization Quality-of-Life-Bref Scale measuring the quality of life of women with severe preeclampsia in southern Ethiopia. Health Qual. Life Outcomes. 19, 239. https://doi.org/10.1186/s12955-021-01872-z (2021).
Terry, K., Koo, P., Mae, Y. & Li, B. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J. Chiropr. Med. 15, 155–163. https://doi.org/10.1016/j.jcm.2016.02.012 (2016).
Ahmed, A., Rezai, H. & Broadway-Stringer, S. Evidence-based revised view of the pathophysiology of preeclampsia. Adv. Exp. Med. Biol. 956, 355–374 (2016).
Endeshaw, M., Abebe, F., Bedimo, M. & Asart, A. Diet and pre-eclampsia: A prospective multicentre case–control study in Ethiopia. Midwifery 31, 617–624 (2015).
Kyembwa Mulyumba, M., Juakali Sihalikyo, K. V., Katenga Bosunga, G., Manga Okenge, P., Kakoma Sakatolo, J. B. Risk factors of pre-eclampsia in Goma (Democratic Republic of the Congo). Afr. J. Health Issues 3(12) (2018).
Kiondo, P. et al. Adverse neonatal outcomes in women with preeclampsia in Mulago Hospital, Kampala, Uganda: A cross-sectional study. Pan Afr. Med. J. 17(1), 7 (2014).
Liew, L. C. & Noraini, I. Validity and Reliability of The Instrument Using Exploratory Factor Analysis and Cronbach’s alpha. International Journal of Academic Research in Business and Social Sciences 7(10), 400–410 (2017)
Hosmer, D. W. Jr. & Lemeshow, S. Applied Logistic Regression (Wiley, 1989).
G.David Garson. Testing Statistical Assumptions 44–45 (2012). Available from: http://www.statisticalassociates.com
Hansen, A. M. Goodness-of-Fit Tests for Autoregressive Logistic Regression Models and Generalized Linear Mixed Models (2012).
Acknowledgements
We thank the University of Gondar, Institute of Public Health, College of Medicine and Health Sciences for providing us with the opportunity to conduct this study. We also thank the supervisors for reviewing and editing the report of this PhD project. We thank Dorothy L. Southern for her critical review of this paper and for her support in editing and training in scientific writing. We also thank the study participants who participated in this study.
Funding
The current study was funded by a Grant with R.No: (O/V/P/RCS/044/2019 in March 2019) from the University of Gondar, Ethiopia.
Author information
Authors and Affiliations
Contributions
This study was carried out by all authors collaboratively. B.J., M.A. and K.A. contributed to conceptualizing and designing the study, curating and analyzing data, and writing the first draft. Also, B.J., M.A., T.A., and K.A. managed the investigation, literature searches, methodology review, writing, and contributed to data collection; B.J., M.A., T.A., and K.A. contributed to the manuscript review, resource, preparation, and editing. All the authors have read and agreed to the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Jikamo, B., Adefris, M., Azale, T. et al. The effect of preeclampsia on adverse maternal outcomes in Sidama region, Ethiopia: a prospective open cohort study. Sci Rep 12, 19300 (2022). https://doi.org/10.1038/s41598-022-24034-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-24034-7
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
