
Abstract
A few reports have described increasing trends and spatial distribution of multiple myeloma (MM). We used a validated database including the 1606 cases of MM diagnosed in Sardinia in 1974–2003 to explore its time trend, and we applied Bayesian methods to plot MM probability by administrative unit on the regional map. Over the 30 years of observation, the MM standardized incidence rate (standard world population, all ages) was 2.17 × 10–5 (95% CI 2.01–2.34), 2.29 (95% CI 2.06–2.52) among men, and 2.06 (95% CI 1.83–2.28) among women. MM incidence increased by 3.3%/year in 1974–2003, in both males and females, particularly among the elderly and in the high incidence areas. Areas at risk tended to cluster in the north-eastern part of the region. A higher proportion of elderly in the resident population, but not socioeconomic factors, nor livestock farming, was associated with higher incidence rates. The steep upward time trend and the spatial clustering of MM suggest interactions between genetic and environmental determinants that might be more efficiently investigated in the areas at risk.
Similar content being viewed by others

Introduction
Multiple myeloma (MM) is a mature B cell lymphoma, which worldwide standardized rate is 2.1 × 10–5 (95% CI 1.8–2.3)1, ranging from 0.1 to 4.5 among the male population of Asian countries to 10.2–13.1 × 10–5 among the male Afro-American population of Texas and Wisconsin2. MM incidence is more elevated among men; increases sharply with age3; and it occurs more frequently among several occupations, including farmers, cleaners, printers, painters, food processors, and teachers, in several industry jobs, and following exposure to ionizing radiation, certain pesticides, and solvents4,5,6,7,8,9,10. However, its aetiology is still unclear.
As it concerns its time and space variability, an increasing time trend of MM has been described in the Czech Republic11, South America12, Taiwan13, and in Canada14. Three studies described an excess risk in metropolitan and urban areas12,14,15, while no spatial clustering of MM cases was observed in a UK study16.
The Sardinian population is well known for its peculiar genetic features17, which have provided the ideal setting for studies on the genes associated with the local high prevalence of male centenarians18, multiple sclerosis19, or type I childhood diabetes. The study of spatial distribution of MM incidence over the island might provide clues for future more in-depth studies on genetic susceptibility and gene-environment interactions in MM aetiology.
Based on the data reported in the 11th Edition of the International Agency for Research on Cancer (IARC) Cancer Incidence in the Five Continents (CI5-11), the incidence rate ranges 2.6–5.4 × 10–5 across the 33 Italian Cancer Registries2. The history of cancer registration in Sardinia is relatively recent, fragmented, and discontinuing: the Sassari Cancer Registry, covering the northern part of the island and about 30% of the resident population, started in 1993 and ceased operating in 2013; the Nuoro Cancer Registry, covering the central-eastern part of the island and 13% of the total population, started in 2003 and it keeps functioning. After several decades of unsuccessful attempts, a Cancer Registry has been planned for southern Sardinia, but it might take an unpredictable length of time to start operating regularly. The standardized incidence (world population, all ages) reported in the CI5-11 is 2.9 among males and 2.8 × 10–5 among females in northern Sardinia, and 4.0 among males and 2.1 among females in its central-eastern part2.
To get around the lack of an official system of regular surveillance of cancer incidence, in 1974, the chief haematologist of the Cagliari Oncology Hospital (BG) initiated a database of incident cases of haemolymphatic malignancies over the whole region, with the collaboration of all the clinical, surgical and pathology departments, social security agencies, and health authorities, and he kept updating it up to 2003, as described elsewhere20. To explore the time trend and the geographical distribution of multiple myeloma over the territory of the island, we used such database, which was previously validated by comparison with mortality and hospitalization data21.
Results
Time trend in MM incidence
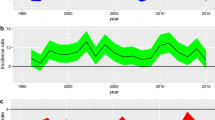
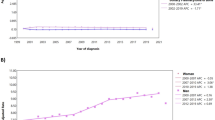
In 1974–2003, 1606 MM cases occurred among the Sardinian population. Based on the standard World population, the incidence rate over these three decades was 2.17 × 10–5 (95% CI 2.01–2.34) for the total population (all ages), 2.29 (95% CI 2.06–2.52) among males, and 2.06 (95% CI 1.83–2.28) among females, with a male/female ratio of 0.95. The crude rate over the study period was 2.73 × 10–5 (95% CI 2.57–2.89) among the total population, 3.17 (95% CI 2.94–3.40) among males, and 2.30 (95% CI 2.07–2.53) among females. With Poisson regression analysis, the average annual increase in MM incidence was 2.19% (95% CI 1.60 – 2.78, p < 0.001). Graphs in Fig. 1 show the trend of MM incidence from linear regression analysis, by gender: the upward trend was similar among the female (0.189 × 10–5 per year, p = 0.007) and the male population (0.113 × 10–5 per year, p < 0.001), with a slope 10 times steeper above the age of 65 (0.479 × 10–5 per year, p < 0.001) than below 65 (0.049 × 10–5 per year, p < 0.001) (analysis of covariance: F = 307.37, DF = 58; p < 0.001). Results from the univariate regression analysis were confirmed with Poisson regression analysis. The upward time trend was observed in the areas with incidence rate below the median (0.110 × 10–5 per year, p < 0.001), as well as in the areas where incidence rate was above the median (0.207 × 10–5 per year, p < 0.001), but its slope was twice as steep in the high incidence areas (analysis of covariance: F = 61.5, DF = 58; p < 0.001). To further validate our data base with cancer registry data, we contrasted the 1993–2002 data from the Sassari Cancer Registry to the same figures in our data base for the same area. In 1993–1997, the Sassari Cancer Registry data reported a MM incidence, based on the world standard population, of 2.7 × 10–5 among men and 2.1 among women22, which increased up to 3.5 among men and 2.9 in 1998–200223. The corresponding figures for the same area in our data base were 2.4 for men and 1.7 for women in 1993–1997, and 2.8 for men and 2.1 for women in 1998–2002. In 2008–2012, MM incidence (world standard population) was stable for both genders in the northern part of the region (Sassari Cancer Registry: men 2.9 × 10–5; women 2.8 × 10–5), while it was 4.0 × 10–5 among men, more than double the 1974–2003 figure from the clinical database (1.8 × 10–5), and 2.1 × 10–5 among women, substantially similar to the 1974–2003 incidence (2.3 × 10–5), in the Nuoro Cancer Registry2.

1974–2003 annual incidence rate of multiple myeloma in Sardinia, Italy, by gender (a males, b females) and overall (c).
Geographic map of MM incidence
Figure 2 shows the map of the posterior probability (P) of a MM incidence rate above the critical rate in each of the 356 Sardinian communes, overall and by gender. Seven communes stand out exceeding the 95th percentile distribution of the likelihood ratio. These are: Arborea (9 cases, likelihood ratio 20.2, P = 0.953), Padria (5 cases, likelihood ratio 20.2, P = 0.953), Benetutti (8 cases, likelihood ratio 46.8, P = 0.979), Bitti (11 cases, likelihood ratio 59.2, P = 0.983), Oschiri (11 cases, likelihood ratio 70.0, P = 0.986), Perfugas (10 cases, likelihood ratio 75.2, P = 0.987), and Seneghe (9 cases, likelihood ratio 177.9, P = 0.994). Another 25 communes have a posterior probability ranging 80–94%, based on 3 or more cases. The map shows a tendency of communes with a high posterior probability of an increased MM incidence to concentrate in the north-eastern area of the island, with the low probability areas located in the southern areas and in the two major urban areas, one, Cagliari, in the south, and the second, Sassari, in northwest Sardinia. Supplementary Table 2 shows the age and gender standardized incidence rates aggregated by health district.

Map of multiple myeloma incidence in Sardinia, Italy. Likelihood ratios are presented by commune with the following colour scales: white < 0.165, pale grey 0.166–0.335, pale-medium grey 0.336–0.50, medium-dark grey 0.501–0.80, dark grey 0.801–0.95, black > 0.951. (a) males; (b) females; (c) total population. Maps of the administrative borders of the Italian communes were created by Spataro C and Piersoft Paolicelli F (https:\\umap.geonue.com/ en/map/confini-e-dati-statistici-dei-comuni-ditalia_297#8/40.102/8.973), using open access software by ANCITEL, a company providing services to the Association of the Italian Communes, under an ODBL (Open Database License) license. An ODBL license requires users to extend such license to the products created using it.
Analysis of MM risk factors
We explored with weighted multivariate regression analysis whether socioeconomic conditions, or size of livestock, or an aging population might have generated the wide geographic variability in MM incidence we observed. As an indicator of socioeconomic conditions, we used the Italian National Institute of Statistics (ISTAT) deprivation index, which combines the following: proportion of the resident population who attained elementary education at most; proportion of the resident population aged 15 years or older searching for an occupation; proportion of the active population engaged in manual work; proportion of rentals over the total residences; persons per room in the household24. Independent covariates were male/female ratio of the resident population, deprivation index, presence and size of livestock farms (cattle, sheep, and goats)25, and proportion of the population aged ≥ 65 years. We used the commune population sizes relative to the overall regional population as the weights. None of the covariates showed a significant association with MM incidence (Supplementary Table 3).
Discussion
Our results show that in 1974–2003 MM incidence increased in both genders among the Sardinian population. Cancer Registry data confirmed such finding limited to the northern area of the region and the last decade covered by the database we used. There was no further increase in the subsequent years. The steeper slope of the regression line among the elderly suggests that the increasing aging of the Sardinian population and the increasing access of the elderly to specialized medical care over the study period might have contributed to a more frequent diagnosis of the disease along the years. However, the same upward time trend was also observed among the population aged < 65, indicating that other factors might have played a role, possibly interacting with genetic susceptibility to generate the steeper upward time trend we observed in high-risk areas.
Seven communes stand out with the highest probability of their rate exceeding that of the overall population of the region, four located in the north-eastern area (Benetutti, Bitti, Oschiri, and Perfugas) and three scattered in the north-west and central areas. These are mainly agricultural areas, six with archaeological remains indicating their origin dating back to prehistory, and one, Arborea, built in 1928 over a reclaiming land, previously covered by marshes in a malaria endemic area. Most of the population hosted in this new city came in the early years of its foundation from Veneto and Friuli, two regions in north-east Italy, and created a flourishing livestock and agricultural crop economy. This town is also known for the large size of its livestock, with two thirds of Sardinian cattle raised in its land. Although we are unaware of publications exploring the association between zoonoses and risk of multiple myeloma among livestock breeders, several papers investigated the association between risk of lymphoma and contact with livestock26. However, we did not find a relationship between presence of large cattle farms and MM incidence over the whole region. The analysis of cancer mortality and hospitalisation in areas at risk because of industrial or military settlements, reported an isolated excess of mortality from MM in an urban area in north-eastern Sardinia, and no excess in any of eight areas including major industrial settlements27. Our results confirm no excess of MM incidence in the communes surrounding the industrial areas in the Sardinian territory.
The finding of an excess risk associated with having a first-degree relative affected by MM, particularly among men, and African Americans, supports a role of genetic factors28. On the other hand, about 17% of MM heritability seems explained by the known gene variants29. Besides, based on results from molecular biology studies, aberrant class switch recombination occurring early in the natural history of MM suggests that environmental factors, such as high doses of ionizing radiation, and occupational exposure in the farming and petrochemical industries, might also contribute to increase risk30. The DNA damage resulting from environmental exposures would interact with the class switch recombination process to increase the risk of chromosomal translocations, oncogene deregulation, and malignant transformation30. In an analysis of MM risk related to occupation, a moderate increase in risk was reported in association with contact with livestock31. Also, gardeners and nursery workers combined, but not other farming jobs, metal processors, female cleaners, and occupations with high level exposure to organic solvents showed a moderate increase in risk32. Among lifestyle factors, a moderate alcohol intake might would reportedly convey protection33. We could not detect a role of deprivation index, an indicator of socioeconomic level, nor did the prevalence of elderly or the male/female ratio or the presence and size of livestock farming affect MM incidence. However, in our ecological analysis, the population of each commune was the unit, and not the individual. Unless the exposed represent a large proportion of the resident population and a strong association exists between the environmental exposure and the disease, the so-called ecological fallacy is likely to occur and to mask possible associations or to generate spurious increases in risk34.
We are not aware of genetic investigations aiming to identify the varying prevalence of gene polymorphisms implicated in MM among the Sardinian population. The small town of Arborea, with his peculiar modernist architecture, is home for about 4000 inhabitants, a large fraction of whom preserved their original language, diet, and habits. This population has a different ethnic origin than the rest of the Sardinian population, but it is unclear whether this might be related to the excess incidence of MM therein observed. Nonetheless, the incidence for the resident population (both genders), standardized based on the world population, was 4.6 × 10–5, 5.05 among men, and 4.2 among women. The corresponding rates in the Veneto region cancer registry were 4.5 for men and 3.7 for women in the IARC CI5 10th Edition35, and 4.1 for men and 2.7 for women in its 11th Edition2. The corresponding figures in the Friuli Cancer Registry were 3.8 for men and 2.9 for women26, and 3.3 for men and 2.5 for women2, consistent with what observed in the town of Arborea in 1974–2003.
The imprecise correspondence with Cancer Registry data might be due to the fact that the database we used includes the cases resulting from an exhaustive active search of the MM diagnoses in the registers of all clinical departments, followed by a double check of the clinical records of each case for the Durie and Salmon diagnostic criteria36 to come up with the diagnostic certainty of MM. These might not include all the incident cases reported to the Cancer Registries; besides, underdiagnosis of MM might have occurred among the elderly, particularly in the early years of creating the database we used. However, this would affect mostly small villages far apart from the specialized haematology units, located in the major urban centres; still, the elevated risk was mainly observed exactly in small towns, which would contrast this hypothesis.
For the same reason, post-diagnosis relocation of the families seems unlikely to have occurred. The exact address at the time of diagnosis was missing for 58/1606 patients (3.6%); it seems also unlikely that this might have affected the overall pattern.
An advantage of our study is that the diagnoses were all reviewed by the same expert haematologist (GB), thus preventing bias due to the varying diagnostic ability by time and geographic area and minimizing and spreading equally the probability of misdiagnosis over the whole region and along the study period. Although not exactly matching the Cancer Registry data limited to the overlapping period and to the northern part of the island for the reasons explained above, the similar figures calculated from our database confirm the completeness of its records.
Conclusion
Our results describe for the first time increasing time trends of multiple myeloma over several decades among the population of the island of Sardinia. Multiple myeloma incidence increased in both genders, and particularly among the elderly and in high-risk areas. We also observed a clustering of high MM incidence in the north-eastern area, which might be of interest for future gene-environment interaction studies, with special focus on agricultural factors, such as use of pesticides, exposure to endotoxin, and contact with livestock and zoonotic agents. We could not identify a role of socioeconomic status, as indicated by the deprivation index, nor of livestock farming. Finally, our results might support the extension of the Cancer Registry coverage to the whole Sardinian population, which would be of paramount importance not only for fostering further research, but also for early detection of risk areas, so to promote effective preventive intervention, and for a rational planning of cancer treatment resources.
Material and methods
A detailed description of the database of haemolymphatic malignancies we used in this study can be found elsewhere20. Briefly, it includes 14,744 incident cases of any haematological cancer, in both genders, and at any age diagnosed in the Italian region of Sardinia in 1974–2003. For the purposes of this analysis, we selected the 1606 MM cases, 781 males and 825 females.
For each commune (the smallest administrative unit in Italy), we calculated the total person-years for each gender and age group (0–24, 25–34, 35–44, 45–54, 55–64, 65–74, and 75 +) over the study period, from January 1974 through December 2003. The standardized incidence rate, annual and over the whole study period, of MM was calculated using the 1971, 1981, 1991, and 2001 census data of the regional population as the standard. Census figures were extended four years onwards and five years backwards to estimate the resident population in the intercensal years. The time trend along the study period was explored with the linear regression equation, and with Poisson regression, adjusting by age and gender. To compare results with those from the IARC CI5 volumes, we also standardized the regional, gender specific incidence rates using the standard world population. We used analysis of covariance to test the chance probability associated with the different slope of regression coefficients by gender, by age at diagnosis (below or above 65 years old), and by residence in an area with low vs high probability of MM occurrence, using the median as the cut point37.
The statistics to explore the spatial distribution of the probability of MM occurrence have been previously described in detail38. Briefly, we used a Bayesian approach, which allowed us to combine information on MM incidence over the island with that from the individual communes with the following equation:
where P(η|d,I) is the posterior probability distribution of MM incidence rate η for a given commune, after combining the data d for that commune with those from the whole region. \(P\left(\eta |I\right)\) is the prior MM standardized incidence rate, η, from the background regional information; \(P\left(d|\eta ,I\right)\) is the probability of getting \(d\) for the commune assuming \(\eta\) is true, and \(P(d|I)\) sets to one the integral of the posterior probability P(η|d,I) over all possible values of \(\eta\), so to obtain a probability density function.
To detect communes at high risk, we set the critical value of p = 0.001 in the prior probability distribution of MM incidence over the 356 Sardinian communes, and, for each commune and each gender and age subgroup, we calculated the likelihood ratio between the probability of a MM incidence rate higher than the critical probability level and that of a MM incidence rate consistent with what observed at the regional level.
Finally, we plotted on the regional map the probability associated with the likelihood ratio for each commune, using the following colour scale for the area of each commune, based on the quintiles of the probability distribution: white < 0.165, light grey 0.166–0.335, medium-light grey 0.336–0.50, medium-dark grey 0.501–0.80, dark grey 0.801–0.95. The few communes associated with a probability higher than 95% had the darkest black shade.
The methods used in this study do comply with the requirements for ecological studies, including the acknowledgement of the limitations of such study design, as highlighted by Rezaeian’s call for a still missing STROBE statement on ecological studies39. Our ecological study was based on the analysis of aggregated data; no humans were involved. Therefore, the informed consent requirement for participation does not apply. The use of these aggregated data for the purposes of scientific publication was approved by the Ethics Committee of the University Hospital of Cagliari (protocol N. PG 2019/18070, 18 December 2019).
Data availability
Data are preserved in the archives of the Department of Medical Sciences and Public Health of the Cagliari University in aggregated form, and they are publicly available as such. Please contact Prof. Pierluigi Cocco (http://pcocco@unica.it) for any request.
Change history
02 March 2022
A Correction to this paper has been published: https://doi.org/10.1038/s41598-022-07811-2
References
Cowan, A. J. et al. Global burden of multiple myeloma: A systematic analysis for the global burden of disease study 2016. JAMA Oncol. 4, 1221–1227. https://doi.org/10.1001/jamaoncol.2018.2128 (2018).
International Agency for Research on Cancer In Cancer Incidence in Five Continents (eds Bray, F. et al.) 25–1543 (IARC, 2021).
Munshi, N. C. & Anderson, K. C. Plasma cell neoplasms. In DeVita, Hellman, and Rosenberg’s Cancer: Principles & Practice of Oncology 10th edn (eds DeVita, V. T. et al.) 1682–1719 (Wolters Kluwer Health Adis (ESP), 2015).
De Roos, A. J., Baris, D., Weiss, N. S. & Herrinton, L. Epidemiology of Multiple Myeloma. In Multiple Myeloma (eds Malpas, J. S. et al.) 117–148 (Elsevier, 2004).
Perrotta, C. et al. Multiple Myeloma and lifetime occupation: Results from the EPILYMPH study. J. Occup. Med. Toxicol. 7, 25. https://doi.org/10.1186/1745-6673-7-25 (2012).
Lope, V. et al. Occupation, exposure to chemicals, sensitizing agents, and risk of multiple myeloma in Sweden. Cancer Epidemiol. Biomarkers Prev. 17, 3123–3127. https://doi.org/10.1158/1055-9965.EPI-08-0343 (2008).
Figgs, L. W., Dosemeci, M. & Blair, A. Risk of multiple myeloma by occupation and industry among men and women: A 24-state death certificate study. J. Occup. Med. 36, 1210–1221. https://doi.org/10.1097/00043764-199411000-00007 (1994).
Gold, L. S. et al. Occupation and multiple myeloma: An occupation and industry analysis. Am. J. Ind. Med. 53, 768–779. https://doi.org/10.1002/ajim.20857 (2010).
De Roos, A. J. et al. Pooled study of occupational exposure to aromatic hydrocarbon solvents and risk of multiple myeloma. Occup. Environ. Med. 75, 798–806. https://doi.org/10.1136/oemed-2018-105154 (2018).
Lerro, C. C. et al. Cancer incidence in the agricultural health study after 20 years of follow-up. Cancer Causes Control. 30, 311–322. https://doi.org/10.1007/s10552-019-01140-y (2019).
Maluskova, D. et al. Epidemiology of multiple myeloma in the Czech Republic. Klin. Onkol. 30(2), 35–42. https://doi.org/10.14735/amko20172S35 (2017).
Curado, M. P., Oliveira, M. M., Silva, D. R. M. & Souza, D. L. B. Epidemiology of multiple myeloma in 17 Latin American countries: An update. Cancer Med. 7, 2101–2108. https://doi.org/10.1002/cam4.1347 (2018).
Tang, C. H. et al. Epidemiology of multiple myeloma in Taiwan, a population-based study. Cancer Epidemiol. 55, 136–141. https://doi.org/10.1016/j.canep.2018.06.003 (2018).
Tsang, M. et al. Multiple myeloma epidemiology and patient geographic distribution in Canada: A population study. Cancer 125, 2435–2444. https://doi.org/10.1002/cncr.32128 (2019).
Rajabli, N. et al. Epidemiology of leukemia and multiple myeloma in Golestan, Iran. Asian Pac. J. Cancer Prev. 14, 2333–2336. https://doi.org/10.7314/apjcp.2013.14.4.2333 (2013).
Cartwright, R. A., Gilman, E. A., Nicholson, P. & Allon, D. Epidemiology of multiple myeloma in parts of England, 1984–1993. Hematol. Oncol. 17, 31–38. https://doi.org/10.1002/(sici)1099-1069(199903)17:1%3c31::aid-hon636%3e3.0.co;2-f (1999).
Cavalli-Sforza, L. L., Menozzi, P. & Piazza, A. The history and geography of human gene. J. R. Anthropol. Inst. 2, 413. https://doi.org/10.2307/3034645 (1996).
Francalacci, P. et al. Low-pass DNA sequencing of 1200 Sardinians reconstructs European Y-chromosome phylogeny. Science 341, 565–569. https://doi.org/10.1126/science.1237947 (2013).
Fazia, T. et al. Investigating multiple sclerosis genetic susceptibility on the founder population of east-central Sardinia via association and linkage analysis of immune-related loci. Mult. Scler. 24, 1815–1824. https://doi.org/10.1177/1352458517732841 (2018).
Broccia, G. et al. Hematological malignancies in the island of Sardinia, 1974–1993: Age and sex distributions and temporal changes in incidence. Hematol. Oncol. 22, 91–109. https://doi.org/10.1002/hon.733 (2004).
Cocco, P. Lessons learned from the ‘Quirra syndrome’ epidemiology? No, thanks. Epidemiol. Prev. 36, 41–44 (2012).
International Agency for Research on Cancer In Cancer Incidence in Five Continents (eds Parkin, D. M. et al.) 93–771 (IARC, 2002).
International Agency for Research on Cancer In Cancer Incidence in The Five Continents (eds Curado, M. P. et al.) 417–893 (IARC, 2007).
Minerba, L. & Vacca, D. [Deprivation indexes for the analysis of inequality across the communes of Sardinia]. In: https://istat.it/it/archivio/6727 (2006).
LAORE - Agenzia Regionale per lo Sviluppo in Agricoltura [Data on cattle, sheep, and goat farms in Sardinia – 2019]. http://sardegnaagricoltura.it/documenti (2020).
Cocco, P. et al. Lymphoma risk in livestock farmers: Results of the Epilymph study. Int. J. Cancer. 132, 2613–2618. https://doi.org/10.1002/ijc.27908 (2013).
Biggeri, A. et al. Report on health status of residents in areas with industrial, mining, or military sites in Sardinia, Italy. Epidemiol. Prev. 30(1 Suppl 1), 5–95 (2006) ([In Italian]).
Schinasi, L. H. et al. Multiple myeloma and family history of lymphohaematopoietic cancers: Results from the International Multiple Myeloma Consortium. Br. J. Haematol. 175, 87–101. https://doi.org/10.1111/bjh.14199 (2016).
Chattopadhyay, S. et al. Genome-wide interaction and pathway-based identification of key regulators in multiple myeloma. Commun. Biol. 2, 89. https://doi.org/10.1038/s42003-019-0329-2 (2019).
Morgan, G. J., Davies, F. E. & Linet, M. Myeloma aetiology and epidemiology. Biomed. Pharmacother. 56, 223–234. https://doi.org/10.1016/s0753-3322(02)00194-4 (2002).
Svec, M. A., Ward, M. H., Dosemeci, M., Checkoway, H. & De Roos, A. J. Risk of lymphatic or haematopoietic cancer mortality with occupational exposure to animals or the public. Occup. Environ. Med. 62, 726–735. https://doi.org/10.1136/oem.2005.021550 (2005).
Perrotta, C. et al. Multiple myeloma and occupation: A pooled analysis by the International Multiple Myeloma Consortium. Cancer Epidemiol. 37, 300–305. https://doi.org/10.1016/j.canep.2013.01.008 (2013).
Andreotti, G. et al. A pooled analysis of alcohol consumption and risk of multiple myeloma in the international multiple myeloma consortium. Cancer Epidemiol. Biomarkers Prev. 22, 1620–1627. https://doi.org/10.1158/1055-9965.EPI-14-1145 (2013).
International Agency for Research on Cancer In Cancer Incidence in Five Continents (eds Forman, D. et al.) 126–1363 (IARC, 2013).
Greenland, S. & Robins, J. Ecologic studies-biases, misconceptions, and counterexamples. Am. J. Epidemiol. 139, 747–760. https://doi.org/10.1093/oxfordjournals.aje.a117069 (1994).
Durie, B. G. & Salmon, S. E. A clinical staging system for multiple myeloma. Correlation of measured myeloma cell mass with presenting clinical features, response to treatment, and survival. Cancer 36, 842–854 (1975).
Snedecor, G. W. & Cochran, W. G. Statistical Methods 6th edn. (The Iowa State University Press, 1967).
Broccia, G. et al. Haemolymphatic cancer among children in Sardinia, Italy: 1974–2003 incidence. BMJ Open 10, e037163. https://doi.org/10.1136/bmjopen-2020-037163 (2020).
Rezaeian, M. A call for revising the strengthening the reporting of observational studies in epidemiology statement to include ecologic studies. J. Clin. Epidemiol. 67, 836. https://doi.org/10.1016/j.jclinepi.2014.02.010 (2014).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
G.B.: Conceptualization, Data curation, Validation, Project administration, Writing—review & editing. J.C.: Conceptualization, Methodology, Formal analysis, Roles/Writing—original draft, Writing—review & editing. C.O.-O.: Visualization, Writing—review & editing. F.M.: Formal analysis, Visualization, Writing—review & editing. I. P.: Formal analysis, Visualization, Writing—review & editing. S.D.M.: Supervision, Writing—review & editing. P.C.: Conceptualization, Methodology, Supervision, Roles/Writing—original draft, Writing—review & editing.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this Article was revised: The original version of this Article contained an error in the Results section, under subheading “Geographic map of MM incidence”. Full information regarding the corrections made can be found in the correction for this Article.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Broccia, G., Carter, J., Ozsin-Ozler, C. et al. Time trend and Bayesian mapping of multiple myeloma incidence in Sardinia, Italy. Sci Rep 12, 2736 (2022). https://doi.org/10.1038/s41598-022-06745-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-06745-z
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
