
Abstract
The persistent increase of multidrug-resistant (MDR) Mycobacterium tuberculosis (Mtb) infections negatively impacts Tuberculosis treatment outcomes. Host-directed therapies (HDT) pose an complementing strategy, particularly since Mtb is highly successful in evading host-defense by manipulating host-signaling pathways. Here, we screened a library containing autophagy-modulating compounds for their ability to inhibit intracellular Mtb-bacteria. Several active compounds were identified, including two drugs of the diphenylbutylpiperidine-class, Fluspirilene and Pimozide, commonly used as antipsychotics. Both molecules inhibited intracellular Mtb in pro- as well as anti-inflammatory primary human macrophages in a host-directed manner and synergized with conventional anti-bacterials. Importantly, these inhibitory effects extended to MDR-Mtb strains and the unrelated intracellular pathogen, Salmonella enterica serovar Typhimurium (Stm). Mechanistically Fluspirilene and Pimozide were shown to regulate autophagy and alter the lysosomal response, partly correlating with increased bacterial localization to autophago(lyso)somes. Pimozide’s and Fluspirilene’s efficacy was inhibited by antioxidants, suggesting involvement of the oxidative-stress response in Mtb growth control. Furthermore, Fluspirilene and especially Pimozide counteracted Mtb-induced STAT5 phosphorylation, thereby reducing Mtb phagosome-localized CISH that promotes phagosomal acidification. In conclusion, two approved antipsychotic drugs, Pimozide and Fluspirilene, constitute highly promising and rapidly translatable candidates for HDT against Mtb and Stm and act by modulating the autophagic/lysosomal response by multiple mechanisms.
Similar content being viewed by others
Introduction
Tuberculosis (TB), an infectious disease caused by the pathogen Mycobacterium tuberculosis (Mtb), generally manifests as pulmonary disease, although any other organ can be affected. Infection is transmitted by aerosol borne Mtb which is phagocytosed by alveolar macrophages1. Currently, 23% of the world’s population is estimated to be latently infected with the bacillus, from which around 5–10% will progress towards developing active disease during their lifetime2. In 2019, this led to around 10 million new TB cases, and an unacceptable number of over 1.4 million deaths2. Major efforts addressing new TB vaccine candidates are in progress3, mainly because the only TB vaccine currently available, Bacillus Calmette-Guérin (BCG) can protect infants against severe forms of TB, but is clearly insufficient in preventing pulmonary TB in adults4.
Another major class of human pathogens is the genus of Salmonella, which contains several serovars that cause significant global morbidity and mortality. Typhoid and paratyphoid fever are caused by the Salmonella enterica serotype Typhi and Paratyphi, respectively, while nontyphoidal salmonellosis (gastroenteritis) is related to other serovars, such as Salmonella enterica serovar Typhimurium (Stm)5. More than a billion people are affected annually by these infections, leading to several hundreds of thousands of deaths5,6.
A major difficulty in TB control is the increase in infections with MDR- and extensive-drug resistant TB (XDR-TB), with only 39% being treated successfully in case of the latter2. Also, the emergence of drug-resistant Salmonella is a major concern, urging the development of new therapeutics7. Although numerous antibiotics against TB are currently in clinical trials and a few new antibiotics for the treatment of MDR-TB and XDR-TB, Bedaquilin, Linezolid and Pretomanid8,9, have recently been approved, several reasons encourage the search for alternative treatment strategies10. Barriers such as toxicity, long treatment duration, high costs and social stigma are hampering treatment adherence, thus contributing to the emergence of antibiotic resistance11. Additionally, the inevitable emergence of future resistance against new antibiotics will negatively impact the global goal of eradicating TB, prompting the need for complementary strategies. Host-directed therapy (HDT) might prove a successful contributor towards this goal since it is expected to shorten treatment duration, has the potential to synergize with anti-bacterial therapy, could eradicate dormant bacteria which often escape conventional antibiotic treatment, and should be equally effective against drug-susceptible and drug-resistant Mtb12. An additional advantage is that bacterial resistance against HDT is unlikely to be a problem because single bacterial mutations will be insufficient to counteract multiple host mechanisms simultaneously13. As a first step towards HDT, drug repurposing is an attractive strategy because it could rapidly create a pipeline for new treatment modalities14.
The reason for Mtb’s persistence in human host cells is thought to primarily be due to its ability to modify host signaling and effector pathways to its own advantage. Upon the first contact with phagocytic cells, host cell manipulation is initiated by using extracellular receptors, for example the induction of anti-inflammatory IL-10 via TLR2 and the reduction of pro-inflammatory cytokine production via a pathway initiated by the binding of mycobacterial mannose-capped lipoarabinomannan to the mannose receptor15,16. Following phagocytosis, Mtb halts the process of phagosome maturation by preventing fusion with lysosomes17. Additionally, the bacterium induces the depletion of the vacuolar ATPase (v-ATPase) from the Mtb phagosome, which results in decreased lysosomal acidification and bacterial degradation and therefore decreased antigen processing and antigen presentation, impairing both innate and adaptive immune responses18. Furthermore, the mycobacterial secretion machinery, such as the ESAT-6 secretion system-1 (ESX-1) encoded by the region of difference 1 (RD1) that is present in virulent Mtb strains but absent from BCG, is of vital importance in manipulating host defense mechanisms targeting the bacterium, exemplified by the inhibition of autophagy by ESX-1 secretion-associated protein B (EspB)19,20. Salmonellae also possess numerous mechanisms through which it manipulates infected host cells, including the activation of the host kinase Akt1 to inhibit phagosomal maturation via the Akt1/AS160 pathway21. Thus, numerous bacterial effector molecules, including constituents of the bacterial cell wall, can impair the host cell response and promote the bacteria’s survival.
Various studies, including our own, have aimed to identify druggable host target molecules for HDT22,23,24,25. Many of these studies underscored the importance of autophagy in controlling the intracellular Mtb lifecycle25,26,27. Autophagy regulates cellular homeostasis through recycling intracellular cargo, including protein aggregates, damaged organelles and intracellular pathogens, and delivering these to lysosomes for destruction28. Autophagy selectively targeting intracellular pathogens, also termed xenophagy, has been shown to restrict replication and survival of both Mtb and Salmonellae29, and is activated by various host molecules, such as IFN-γ30, TNF-α31, and extracellular DNA sensor stimulator of interferon genes (STING)32, for which we showed the DNA damage-regulated autophagy modulator 1 (DRAM1) to play an important role27. Several small molecule activators of autophagy have been reported to lower intracellular Mtb burden, including metformin, statins, nitazoxanide, gefitinib and imatinib14.
Although metformin treatment of patients suffering from diabetes mellitus (DM) lowered the prevalence of latent tuberculosis infection (LTBI)33, it failed to show an anti-TB effect in DM patients with pulmonary active TB34,35. Statins have similarly been shown to lower LTBI prevalence33, but in addition have pleiotropic effects on the host response, which can both positively and negatively impact treatment outcome36. Nitazoxanide has been shown to have host-directed activity against Mtb by inducing autophagy, although it also has direct antimicrobial activity37. Tyrosine kinases, including those sensitive to Imatinib such as ABL1, have been found to play a role in Mtb infection by several groups including ours22,38,39. Corroborating these findings, Imatinib has been shown to display anti-mycobacterial activity in vivo in mice40 and is currently being evaluated in a phase 2 trial.
Drugs with efficacy towards controlling intracellular infections with low toxicity are still in short supply. Here, we screened a library of compounds with defined autophagy-inducing or -inhibitory activity using our previously described, human cell based (Mtb-MelJuSo) intracellular infection model22. Several promising candidates were identified, among which two antipsychotic drugs of the diphenylbutylpiperidine-class41, Fluspirilene and Pimozide, were found as particularly interesting hits.
We found that Fluspirilene and Pimozide employ multiple mechanisms converging mostly on the autophagosomal/lysosomal response pathway to control different species of intracellular bacteria. Pimozide was particularly able to induce reactive oxygen species (ROS) which are of vital importance in the host defense response. Furthermore, Fluspirilene and particularly Pimozide inhibited STAT5-dependent Mtb-induced CISH-mediated degradation of phagosomal v-ATPase, underscoring the feasibility of targeting this recently uncovered mechanism. In conclusion we have uncovered potent HDT activity of two antipsychotics against (drug resistant) intracellular Mtb and Stm in human cells.
Materials and methods
Chemicals
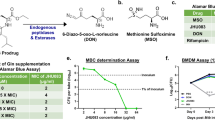
The Screen-Well Autophagy Library version 1.2 (http://www.enzolifesciences.com/BML-2837/screen-well-autophagy-library/) was purchased from Enzo Life Sciences, Brussels, Belgium. H-89 diHCl (H-89), Fluspirilene, Pimozide, Ebselen, NG-Methyl-L-arginine acetate salt (L-NMMA), MitoTEMPO, Phorbol 12-myristate 13-acetate (PMA), N-acetyl cysteine (NAC), tert-butylhydroperoxide (TBHP) and Rifampicin were purchased from Sigma-Aldrich, Zwijndrecht, The Netherlands. Torin-1 and Isoniazid were purchased from SelleckChem, Munich, Germany. Hygromycin B was acquired from Life Technologies-Invitrogen, Bleiswijk, The Netherlands and Gentamicin sulfate was bought from Lonza BioWhittaker, Basel, Switzerland.
Antibodies
Rabbit anti-phospho-STAT5 (RRID:AB_823649), rabbit anti-CISH (RRID:AB_11178524) and rabbit polyclonal anti-TFEB (RRID:AB_11220225) were all bought from Cell Signaling Technology, Leiden, The Netherlands. Phalloidin-iFluor 647 and Phalloidin-iFluor 405 were obtained from Abcam, Cambridge, United Kingdom. Goat anti-rabbit IgG (H + L) AlexaFluor647 conjugate (RRID:AB_2536101) was purchased from ThermoFisher Scientific, Breda, The Netherlands.. Anti-human CD11b-PE (RRID:AB_395789) and anti-human CD1a-BV605 (RRID:AB_2741933) were acquired from BD BioSciences, Vianen, The Netherlands and anti-human CD14-FITC (RRID:AB_830677) and anti-human CD163-AF647 (RRID:AB_2563475) from BioLegend, San Diego, CA, USA.
Cell culture
HeLa and MelJuSo cell lines were maintained at 37 °C/5% CO2 in Gibco Iscove’s Modified Dulbecco’s Medium (IMDM, Life Technologies-Invitrogen) supplemented with 10% fetal bovine serum (FBS; Greiner Bio-One, Alphen a/d Rijn, The Netherlands), 100 units/ml Penicillin and 100 µg/ml Streptomycin (both Life Technologies-Invitrogen) (complete IMDM) as described previously22,23.
Buffy coats were obtained from healthy donors after written informed consent (Sanquin Blood Bank, Amsterdam, The Netherlands). Peripheral blood mononuclear cells (PBMCs) were purified using density gradient centrifugation over Ficoll-Paque and monocytes isolated with subsequent CD14 MACS sorting (Miltenyi Biotec, Bergisch Gladsbach, Germany) as described previously22,23. Monocytes were differentiated into pro-inflammatory (Mφ1) or anti-inflammatory (Mφ2) macrophages with 5 ng/ml of granulocyte‐macrophage colony‐stimulating factor (GM‐CSF; Life Technologies-Invitrogen) or 50 ng/ml macrophage colony‐stimulating factor (M‐CSF; R&D Systems, Abingdon, UK), respectively, for 6 days with a cytokine boost at 3 days, as previously reported42. Cells were cultured at 37 °C/5% CO2 in Gibco Roswell Park Memorial Institute (RPMI) 1640 medium or RPMI 1640 (Dutch modified) (Life Technologies-Invitrogen) supplemented with 10% FBS and 2 mM L-alanyl-L-glutamine (GlutaMAX) (PAA, Linz, Austria), 100 U/ml penicillin and 100 µg/ml streptomycin (complete RPMI) at a density of 1 × 106 cells per ml in T75 flasks (Sigma-Aldrich). Macrophages were harvested using Trypsin–EDTA 0.05% (ThermoFisher Scientific) and scraping and macrophage differentiation was evaluated by cell surface marker expression of CD11b, CD1a, CD14 and CD163 implementing flow cytometry and by quantification of IL-10 and IL-12p40 secretion using ELISA following 24-h stimulation in the presence or absence of 100 ng/ml of lipopolysaccharide (LPS; InvivoGen, San Diego, United States).
Bronchoalveolar lavage (BAL) samples from purpose-bred, Indian-type rhesus macaques in the present study, were used as they were available occasionally, when an animal happened to be indicated for ketamine-sedation and euthanasia for veterinary and animal welfare reason. Thus, the availability of sample was exploited as it occurred, beyond any legal requirement for prior approval of protocol as there was no pre-existing study plan nor any discomfort afflicted to animals for the sake of a research objective. Using a bronchoscope for instillation and recovery, cells were harvested by flushing with 3 consecutive volumes of 20 mL of sterile, pre-warmed, isotonic saline solution. Samples were immediately put on ice and kept cold until further processing. To isolate the cellular fraction, the BAL was filtered over a 100 μm filter and spun down at 400 g for 10 min at 4 °C. To enrich BAL cells for alveolar macrophages (AMφ), BAL cells were resuspended in complete RPMI and incubated for 4 h at 37 °C/5% CO2 in a T75 flask after which non-adherent cells were discarded. Adherent cells were washed with PBS and harvested using Trypsin–EDTA 0.05% and scraping. Cells were counted using Türk solution, spun down by centrifugation at 400 g for 10 min, resuspended in complete RPMI and seeded at 300,000 per ml for downstream application. NHP samples were obtained at the Biomedical Primate Research Centre (BPRC), Rijswijk, the Netherlands. BPRC is licensed by the Dutch authority to breed non-human primates and to use them for research in areas of life-threatening and disabling diseases without suitable alternatives. BPRC complies to all relevant legislation with regard to the use of animals in research; the Dutch 'Wet op de Dierproeven' and the European guideline 2010/63/EU. BPRC is AAALAC accredited since 2012.
Bacterial infection of cells
Mtb (wild-type H37Rv or DsRed-expressing H37Rv)22 was cultured in Difco Middlebrook 7H9 broth (Becton Dickinson, Breda, the Netherlands) supplemented with 10% ADC (Becton Dickinson), 0.05% Tween 80 (Sigma-Aldrich), and with the addition of 50 µg/ml Hygromycin B in the case of DsRed-expressing H37Rv. Mtb suspensions were prepared from a running Mtb culture, which was one day prior to infection diluted to a density corresponding with early log-phase growth (OD600 of 0.25). Stm strain SL1344 was cultured in Difco lysogeny broth (LB) (Becton Dickinson). Stm was grown overnight in LB, subsequently diluted 1:33 in fresh LB and used after approximately 3 h of incubation, when log-phase growth was achieved (OD600 of 0.5). Bacteria (or liquid broth at equal v/v for mock-infection) were diluted in complete IMDM or complete RPMI without antibiotics for infecting cell lines or primary cells, respectively. We consistently used a multiplicity of infection (MOI) of 10 for both strains. Cell lines and primary cells, which had been seeded at a density of 10,000 or 30,000 cells per well, respectively, in 96-well flat-bottom plates 1 day prior to infection, were inoculated with 100 μl of the bacterial suspension. Cells were subsequently centrifuged for 3 min at 800 rpm and incubated at 37 °C/5% CO2 for 20 min in case of Stm infection or 60 min in case of Mtb infection. Extracellular bacteria were then washed away with culture medium containing 30 μg/ml Gentamicin sulfate, incubated for 10 min at 37 °C/5% CO2, followed by replacement with medium containing 5 μg/ml Gentamicin sulfate and, if indicated, chemical compounds until readout. MOI of the bacterial inoculum was confirmed by a standard colony-forming unit (CFU) assay.
Chemical compound treatment
Cells were treated for 24 h, unless indicated otherwise, with chemical compound at a concentration of 10 µM, unless indicated otherwise, or DMSO at equal v/v in medium containing 5 μg/ml Gentamicin sulfate. Treatment regimens were designed not to exceed DMSO solvent end concentrations of 0.2%.
Rifampicin and Isoniazid were used at a concentration of 0.05 µg/mL and 0.4 µg/mL, respectively. Higher concentrations of antibiotics showed almost complete eradication of Mtb growth which thus completely abrogates the window of detection for any additive/synergistic host-directed drug effects, while in contrast lower antibiotic concentrations showed a larger donor variability in the effect on Mtb outgrowth.
Colony-forming unit (CFU) assay
Cells were lysed in H2O containing 0.05% SDS (ThermoFisher Scientific). Lysates of Mtb-infected cells were serially diluted in steps of fivefold in 7H9 broth and 10 μl droplets were spotted onto square Middlebrook 7H10 agar plates. Plates were incubated at 37 °C for 12–14 days and bacterial colonies quantified using a microscope with a magnification of 2.5 times to enhance early detection of bacterial growth. Lysates of Stm-infected cells were serially diluted in LB broth, thereafter 10 μl droplets were spotted onto square LB agar plates and incubated overnight at 37 °C.
Liquid bacterial growth inhibition assay
Stm or Mtb cultures in logarithmic growth phase were diluted to an OD600 of 0.1 in LB broth or 7H9 broth respectively, of which 200 μl per flat-bottom 96-well was incubated with chemical compound, antibiotic or DMSO at equal v/v at indicated concentrations. Stm growth was measured after overnight incubation at 37 °C, while Mtb growth was evaluated for 10 days of incubation at 37 °C. Absorbance was measured by optical density at 550 nm on a Mithras LB 940 plate reader (Berthold Technologies, Bad Wildbad, Germany) while shaking between measurements.
Flow cytometry
Infected cells were at experimental endpoint washed with 100 µl of PBS and detached by incubation in 50 µl of Trypsin–EDTA 0.05% for five minutes. Single cell suspensions were fixed by adding 100 µl of 1.5% paraformaldehyde and incubated for 60 min at 4 °C. Acquisition was performed using a BD FACSLyric™ Flow Cytometer equipped with BD FACSuite software (BD Biosciences). Data was analyzed using FlowJo software v10.
Cell viability assay
Cells seeded at a density of 30,000 cells/well in 96-well flat-bottom plates were stained in 50 μl RPMI without phenol red (Life Technologies-Invitrogen) containing propidium iodide (PI) (1:500, Sigma-Aldrich) and 100 μg/ml of Hoechst 33,342 (Sigma-Aldrich). Cells were incubated at room temperature (RT) for 5 min. Per well 3 images were taken using a Leica AF6000 LC fluorescence microscope combined with a 20 × dry objective. The number of dead cells (positive for PI) versus total number of adherent cells (positive for Hoechst) was quantified using CellProlifer version 3.0.043.
Immunostaining
Cells were seeded on poly-d-lysine coated glass-bottom (no. 1.5) 96-well plates (MatTek, Ashland, Massachusetts, United States), pre-washed with PBS, at a density of 30,000 per well. After overnight incubation, cells were infected with DsRed-expressing Mtb at a MOI of 10 as previously described. At the indicated experimental endpoint, cells were washed three times with PBS and fixed for 60 min at RT using 1% methanol-free EM-grade formaldehyde (ThermoFisher Scientific) diluted in PBS. Cells were washed with PBS and remaining reactive formaldehyde was quenched using 100 μl of Glycine solution (1.5 mg/ml in PBS) for 10 min at RT. Cells were permeabilized in 0.1% Triton-X (Sigma-Aldrich) diluted in PBS for 10 min at RT and Fc-receptors were subsequently blocked using 5% human serum (HS; Sanquin Blood bank, Amsterdam, The Netherlands) for 45 min at RT. After removal of the 5% HS, cells were stained with primary antibody diluted in 5% HS for 30 min at RT, washed three times with 5% HS and incubated with secondary antibody in 5% HS for 30 min at RT in the dark. After washing three times with 5% HS, cells were counterstained with 50 ul of 2 μg/ml Hoechst 33,342 and Phalloidin for 30 min at RT in the dark. Images, at least 3 per well, were acquired using a Leica TCS SP8 X WLL confocal system and 63X oil immersion objective. Hybrid detectors were used with a time gate to switch off data collection during the pulse. The fluorescent dyes LysoTracker Deep Red (ThermoFisher Scientific) (75 nM) and CYTO-ID 2.0 (Enzo LifeSciences) (1:500) were added to the cells 30 min prior to treatment endpoint. Cells were fixed at the experimental endpoint and counterstained with Hoechst and Phalloidin as described above except for permeabilization.
Colocalization analysis was performed as follows. Image background was subtracted using the rolling ball (20-pixel radius) algorithm with Fiji software44. CellProlifer 3.0.0 was used to first correct for non-homogenous illumination if necessary, then for the segmentation of both the fluorescent bacteria and marker of interest using global thresholding with intensity-based de-clumping45. For every experiment, segmentation was performed independently with both a range of thresholds and adaptive three-class Otsu thresholding to confirm segmentation results. Then per image the overlap of Mtb with marker of interest was calculated as percentage of object overlap (colocalization) or the integrated intensity of the marker of interest per single nucleus or bacterium was determined. Data in Figs. 3C and 4C are shown for 4 individuals, while two donors could not be analyzed due to high background levels.
Reactive oxygen species (ROS)/reactive nitrogen species (RNS) assay
Cells were seeded in complete RPMI in Corning 96-well Special Optics Flat Clear Bottom Black Polystyrene TC-Treated Microplates (Sigma-Aldrich) at a density of 40,000 per well. After overnight incubation at 37 °C/5% CO2, cells were washed once with PBS and incubated with 5 μM CM-H2DCFDA (Life Technologies-Invitrogen), a general oxidative stress indicator, for 30 min at 37 °C/5% CO2 in phenol red free RPMI. Cells were washed twice with PBS followed by treatment with chemical compounds (10 µM) in 100 μl of complete RPMI without phenol red. 50 µM of TBHP was used as technical assay control. Oxidation of the probe yields a fluorescent adduct which presence was quantified every 5 min for 2 h by measuring fluorescence using the SpectraMax i3x at 37 °C. Specific settings used were 10 flashes per read with an 493/9 excitation and a 522/15 emission filter pair and a high PMT gain.
Total RNA isolation and cDNA synthesis
Total RNA isolation was performed using TRIzol Reagent (Life Technologies-Invitrogen) according to the manufacturer's instructions and described previously23. RNA yield was quantified using a DeNovix DS-11 Spectrophotometer (ThermoFisher Scientific). Total RNA (0.5 μg) was reverse transcribed using SuperScript IV Reverse Transcriptase (Life Technologies-Invitrogen). Briefly, RNA samples were first incubated at 65 °C for 5 min in the presence of 0.5 mM dNTPs and 2.5 µM oligo(dT)20 (Life Technologies-Invitrogen). Subsequently, cDNA synthesis was initiated by adding a master mix containing 1 × first strand buffer, 5 mM DTT, 40 U RNaseOUT (ThermoFisher Scientific) and 200 U SuperScript IV and incubating at 50–55 °C for 10 min followed by inactivation of the reverse transcriptase at 80 °C for 10 min.
TaqMan qPCR
Multiplex quantitative polymerase chain reaction (qPCR) was carried out using a QuantStudio 6 Flex Real-Time PCR System (ThermoFisher Scientific) as described previously23. qPCR reactions were performed in a final volume of 25 µl containing 1 × TaqMan Universal PCR Master Mix, No AmpErase UNG, 0.5 × CISH-FAM TaqMan primers (Hs00367082_g1, ThermoFisher Scientific), 0.5 × GAPDH-VIC TaqMan primers ((Hs02758991_g1, ThermoFisher Scientific), and 5 µl cDNA. Thermal cycling conditions were 1 cycle of 2 min/50 °C and 10 min/95 °C, followed by 40 cycles of 15 s/95 °C and 1 min/60 °C. The threshold cycle (Ct) values of CISH transcripts were normalized to GAPDH by the 2-ΔΔCT algorithm method46. Relative expression levels were calculated by applying the formula ((2−ΔCT(Target gene))/(2−ΔCT(GAPDH))).
Statistics
Statistics were performed as described previously23. Normal distribution of the data was tested using the Shapiro–Wilk test. If the data was normally distributed, unpaired t-test with Welch’s correction or one-way ANOVA with Dunnett’s multiple comparison test were applied when assessing differences between 2 and 3 or more groups of unpaired data, respectively. Normally distributed paired samples were analyzed using repeated measure (RM) one-way ANOVA with Dunnett’s multiple comparison test and Geisser Greenhouse correction. Two-way ANOVA with Tukey’s multiple comparison test was used when the effect of two independent variables was tested simultaneously. Assessing differences between 2 or more groups of unpaired observations from not normally distributed data was performed using Kruskal–Wallis test, while paired observations were tested using the Wilcoxon matched-pairs signed rank test with post-hoc Benjamini–Hochberg correction. Analyses were performed using GraphPad Prism 8.
Results
Compounds were identified that contain autophagy-regulating activity and repurposing potential for HDT against Mtb and Stm
By employing our previously described flow-cytometry-based assay using Mtb-infected human MelJuSo cells22, we screened the Screen-Well Autophagy library that includes clinically approved molecules, to find new drugs with HDT activity against intracellular Mtb. Mtb-infected human cells were treated during 24 h with compounds. The PKA/PKB-Akt1 inhibitor H-89 was included as a positive control based on our earlier work21,22. We identified 25 compounds that strongly reduced bacterial burden (< 35% infected cells compared to control DMSO). From these 25 molecules we discontinued 15 because of undesirable significant host cell toxicity (cell-yield < 85% after 24 h treatment compared to control DMSO), and 2 because of a current lack of clinical approval (SB-216763 and Licochalcone A). Two additional compounds were not pursued further since their in vivo adjunct therapy potential had already been shown previously, independently validating our discovery approach (Chloroquine and its metabolite Hydroxychloroquine)47 (Fig. 1A, and Table S1).

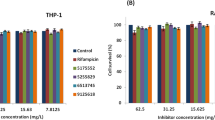
Identification of compounds with autophagy-regulating activity and repurposing potential for HDT against Mtb and Stm. (A) MelJuSo-Mtb model-based screening results of the Screen-Well Autophagy library at 10 µM concentration after 24 h of treatment sorted by effect size on the percentage of infected cells (DsRed-Mtb positive cells) compared to DMSO. Data points display the mean ± standard deviation of 3 replicates. The positive control H-89 and two structural analogues Fluspirilene and Pimozide are annotated. (B) MelJuSo-Mtb model-based screening results of H-89, Fluspirilene and Pimozide at 10 µM concentration after 24 h of treatment on the percentage of cells compared to DMSO. Data points display the mean of 3 replicates and represent two independent experiments. Dotted lines indicate DMSO set at 100% and median is shown for each condition. Statistical significance was tested using a RM one-way ANOVA with Dunnett’s multiple comparison test (* = p-value < 0.05). (C) CFU assay of Mφ1 (upper panel) and Mφ2 (lower panel) infected with Mtb and treated with 10 µM of Fluspirilene, Pimozide, H-89 as positive control or DMSO at equal v/v for 24 h. Effect of compound treatments are shown separate since donors tested were not always identical. Each dot represents a single donor (7 and 8 for H-89, 8 and 9 for Fluspirilene and 9 and 10 donors for Pimozide were tested in Mφ1 and Mφ2, respectively) and depicts the mean of 3 or 4 replicates. Dotted lines indicate DMSO set at 100% and median + 95% confidence intervals are shown for every condition. Statistical significance was tested using Wilcoxon matched-pairs signed rank test with post-hoc Benjamini–Hochberg correction (right panel) (* = q-value < 0.1). (D) CFU assay of Mφ1 (upper panel) and Mφ2 (lower panel) infected with Stm and treated with 10 µM of Fluspirilene, Pimozide, H-89 as positive control or DMSO at equal v/v for 24 h. Each dot represents a single donor (6 donors in total) and depicts the mean of 3 or 4 replicates. Dotted lines indicate DMSO set at 100% and median + 95% confidence intervals are shown for every condition. Statistical significance was tested using Wilcoxon matched-pairs signed rank test with post-hoc Benjamini–Hochberg correction (right panel) (* = q-value < 0.1). (E) Mtb growth in liquid culture during treatment with 10 μM of Fluspirilene, Pimozide or DMSO at equal v/v at assay endpoint, day 10. Rifampicin (20 μg/ml) was used as positive control for Mtb growth inhibition. Bars depict mean ± standard deviation of 3 replicates. Experiment shown is a representative of 4 independent experiments. Statistical significance of treatment versus DMSO was tested using a one-way ANOVA with Dunnett’s multiple comparisons test (**** = p-value < 0.0001). (F) Stm growth in liquid culture during treatment with 10 μM of Fluspirilene, Pimozide or DMSO at equal v/v. Gentamicin (50 μg/ml) was used as positive control for Stm growth inhibition. Bars depict mean ± standard deviation of 3 replicates. Experiment shown is a representative of 2 independent experiments. Statistical significance of treatment versus DMSO was tested using a one-way ANOVA with Dunnett’s multiple comparisons test (**** = p-value < 0.0001).
In our effort to focus on new candidates it was of interest that 2 of the 6 remaining compounds, notably Fluspirilene and Pimozide, are structural analogues of the diphenylbutylpiperidine-class of antipsychotic drugs. Both drugs have an extensive clinical safety profile and are already for several decades used to treat multiple disorders. To explore and compare mechanistics of the analogues, we decided to focus on these two drugs only in this study, while detailed work on the other hit compounds will be described elsewhere.
We observed no cellular toxicity following treatment with Fluspirilene and Pimozide, while H-89 treatment affected cell numbers slightly (Fig. 1B). To validate these initial screening results further in a physiologically more relevant in vitro model, we generated primary GM-CSF-derived pro-inflammatory macrophages (Mφ1) and M-CSF-derived anti-inflammatory macrophages (Mφ2)22,42,48, and tested the potential of the two diphenylbutylpiperidines to inhibit outgrowth of intracellular Mtb (using a classical colony forming unit (CFU) assay as read-out (Fig. 1C). Both Fluspirilene and Pimozide induced a significant decrease of Mtb outgrowth in Mφ1 and particularly Mφ2 (median reduction of bacterial outgrowth of 22% and 36% for Fluspirilene and 35% and 32% for Pimozide, respectively) (Fig. 1C and Table S2).
To investigate potential broader-range applicability of Fluspirilene and Pimozide, we investigated their intracellular bacterial growth inhibitory activity against a different class of intracellular bacteria, using Stm-infected human Mφ (Fig. 1D and Table S2). H-89 was again included as a positive control (it displays greater activity against Stm than Mtb)21,22. Interestingly, both drugs vastly reduced Stm outgrowth (median reduction of bacterial outgrowth > 96% and > 98% in Mφ1 and Mφ2, respectively), suggesting these HDT drugs could be more broadly applicable.
To exclude that Fluspirilene and Pimozide acted in a direct anti-bacterial manner, extracellular Stm and Mtb were treated with Fluspirilene and Pimozide in liquid broth, in equal concentrations (10 µM) as used in the cell-based infection models. Fluspirilene and Pimozide did not affect Mtb or Stm growth, whereas control antibiotics Rifampicin (Mtb) and Gentamicin (Stm) inhibited bacterial growth (Fig. 1E, F and Table S2).
Taken together, we identified two clinically approved structural analogues displaying reported autophagy-inducing capacities as novel safe candidate molecules for HDT, that inhibited intracellular Mtb as well as Stm in both pro- and anti-inflammatory human primary macrophages.
Fluspirilene and Pimozide HDT activity against intracellular Mtb was confirmed cross-species of host and mycobacterium
Since HDT drugs act on host rather than bacterial targets, they should inhibit outgrowth of drug-susceptible and multi-drug resistant (MDR)-Mtb strains similarly. To verify this, we measured the effect of the two diphenylbutylpiperidines on CFU outgrowth in human Mφ2 (we focused on Mφ2 since we found similar efficacy in both Mφ1 and Mφ2). The cells were infected with either Mtb Dutch outbreak strain 2003–1128 or Mtb Beijing strain 16,319, both MDR-Mtb-strains. Indeed, treatment with Fluspirilene and Pimozide significantly inhibited bacterial outgrowth of both MDR-Mtb strains highly efficiently (Fig. 2A and Table S2), thereby emphasizing their clinical relevance.

Further in depth and translational validation of Fluspirilene and Pimozide HDT activity against intracellular Mtb. (A) CFU assay of Mφ2 infected with MDR-Mtb strain Dutch outbreak 2003–1128 (left panel) or MDR-Mtb strain Beijing 16,319 (right panel) and treated with 10 µM of Fluspirilene, Pimozide or DMSO at equal v/v for 24 h. Each dot represents a single donor (5 donors in total) and depicts the mean of 3 replicates. Dotted lines indicate DMSO set at 100% and median + 95% confidence intervals are shown for every condition. Statistical significance was tested using RM one-way ANOVA with Dunnett’s multiple comparison test (left panel) (** = p-value < 0.01 and *** = p-value < 0.001) or Wilcoxon matched-pairs signed rank test with post-hoc Benjamini–Hochberg correction (right panel) (* = q-value < 0.1). (B) CFU assay of Mφ2 infected with Mtb and treated with a combination of a suboptimal dose of Rifampicin (0.05 µg/ml) and 10 μM of Fluspirilene, Pimozide or DMSO at equal v/v for 24 h. Bars depict mean ± standard deviation of 3 replicates from a representative donor (out of 4 donors tested), expressed as a percentage of the DMSO control in the absence of Rifampicin. Black bars represent Fluspirilene, Pimozide or DMSO only, red bars represent the combination with Rifampicin. Statistical significance was tested using a two-way ANOVA with Tukey’s multiple comparisons test comparing Fluspirilene or Pimozide treatment (in the absence or presence of Rifampicin) to the corresponding DMSO control (* = p-value < 0.05, ** = p-value < 0.01, *** = p-value < 0.001 and **** = p-value < 0.0001). (C) CFU assay of Mφ2 infected with Mtb as in (B), but a suboptimal dose of Isoniazid (0.4 µg/ml) was used. Bars depict mean ± standard deviation of 3 replicates from a representative donor (out of 3 donors tested), expressed as a percentage of the DMSO control in the absence of Isoniazid. (D) Flow cytometry assay measuring the percentage of Mtb-infected cells (left panel), CFU assay (middle panel) and cell viability assay measuring the percentage of live cells (right panel) of ex vivo non-human primate bronchoalveolar lavage cells enriched for alveolar macrophages (NHP AMφ) infected with DsRed-expressing Mtb and treated with 10 µM of Fluspirilene, Pimozide or DMSO at equal v/v for 24 h. Each dot represents a single NHP donor (3 donors in total) and depicts the mean of 1 to 2 replicates (left panel), 6 replicates (middle panel) or 3 replicates (right panel), expressed as a percentage of the DMSO control. Statistical significance was tested using a RM one-way ANOVA with Dunnett’s multiple comparison test (* = p-value < 0.05).
Clinical application of HDT will most likely be considered as adjunct to standard antibiotic therapy for TB14. Since HDT and antibiotics have different targets, we investigated whether synergistic/additive effects between these treatments could be detected. Combining either Fluspirilene or Pimozide with a suboptimal dose of Rifampicin (0.05 µg/ml) inhibited Mtb outgrowth to a significantly larger extent compared to Fluspirilene, Pimozide, or Rifampicin treatment alone (Fig. 2B and Table S2). Unexpectedly, this effect was not observed when Fluspirilene and Pimozide were combined with a suboptimal dose of Isoniazid (0.4 µg/ml) (Fig. 2C and Table S2). While not further investigated here, a possible explanation for this could be that the diphenylbutylpiperidines alter host cell processes required for Isoniazid’s conversion into its active form49.
To further strengthen the potential utility of Fluspirilene and Pimozide, we next tested their efficacy on Mtb-infected ex vivo non-human primate (NHP) bronchoalveolar lavage (BAL) cells which are a rich source of alveolar macrophages (AMφ), the primary target cells for Mtb. Cross-species efficacy of the drugs would suggest functional conservation of their host targets as well as translate and validate our above findings in human cells. Importantly, 24-h treatment with either one of the drugs decreased outgrowth of intracellular Mtb. This was reflected in the reduced percentage of infected cells (Fig. 2D, left panel), and especially in the reduced number of colony forming bacteria (Fig. 2D, middle panel, and Table S2). Notably, Fluspirilene and Pimozide treatment showed noy toxicity towards the ex vivo NHP AMφ (Fig. 2D, right panel).
Taken together, these results significantly strengthen the potential value of Fluspirilene and Pimozide in HDT approaches against intracellular infections, including MDR-Mtb bacteria, and demonstrate their activity also in (NHP) infected alveolar macrophages.
Fluspirilene and Pimozide regulate autophagy, induce a lysosomal response and enhance bacterial presence in autophago(lyso)somes
Because Fluspirilene and Pimozide are known to modulate and induce autophagy50, we investigated this as a potential mode of action against intracellular Mtb. Mφ2 were infected with Mtb, treated for 4 h with Fluspirilene and Pimozide, stained with CYTO-ID (a tracer that stains all autophagy-related vesicles) and visualized using confocal microscopy (Fig. 3A, left panel). Importantly, both Fluspirilene and Pimozide, although not statistically significant, tended to increase the CYTO-ID vesicle area and the bacterial localization in these vesicles (Fig. 3A, middle and right panel, and Table S2), lending support to the involvement of autophagy in Fluspirilene and Pimozide’s mode of action against intracellular Mtb in infected human cells.

Fluspirilene and Pimozide regulate autophagy, induce a lysosomal response and enhance bacterial presence in autophago(lyso)somes. (A) Confocal microscopy of DsRed-expressing Mtb-infected Mφ2 treated with 10 µM of Fluspirilene, Pimozide, 1 µM Torin-1 or DMSO at equal v/v for 4 h. 30 min prior to the experimental endpoint cells were incubated with CYTO-ID to stain for autophagy-related vesicles, fixed and counterstained for the nucleus using Hoechst 33,342. Shown in the left panel are representative images of Mφ2, while the middle panel displays the quantification of CYTO-ID positive areas (log2FC CYTO-ID area to DMSO) and the right panel the quantification of Mtb colocalization with CYTO-ID positive vesicles. Scale bar annotates 5 µm. Each dot represents a single donor (4 donors in total) and depicts the mean (middle panel) or mean ± standard deviation (right panel) of 3 replicates and with median and 95% confidence intervals shown (middle panel) or median shown by gray bars (right panel). Statistical significance was tested using a RM one-way ANOVA with Dunnett’s multiple comparison test. (B) Confocal microscopy of DsRed-expressing Mtb-infected Mφ2 treated with 10 µM of Fluspirilene, Pimozide, 1 µM Torin-1 as positive control or DMSO at equal v/v for 4 h. Cells were fixed at the experimental endpoint, permeabilized using 0.1% Triton-X, stained for TFEB and counterstained for the nucleus and F-actin using Hoechst 33,342 and Phalloidin, respectively. Shown in the left panel are representative images of Mφ2, while the middle panel shows violin plots representing all nuclei quantified (n = 79, n = 64 n = 71 and n = 56 for DMSO, Torin-1, Fluspirilene and Pimozide, respectively) of a representative donor with median and interquartile range indicated and the right panel displays the log2FC of median nuclear TFEB intensity per donor normalized to DMSO (5 donors in total) with median and 95% confidence intervals indicated. Scale bar annotates 5 µm. Dotted line indicates median of DMSO. Statistical significance was tested using Kruskal–Wallis test with Dunn’s multiple comparison test (middle panel) (* = p-value < 0.05 and **** = p-value < 0.0001) or RM one-way ANOVA with Dunnett’s multiple comparison test (right panel). (C) Confocal microscopy of DsRed-expressing Mtb-infected Mφ2 treated with 10 µM of Fluspirilene, Pimozide, 1 µM Torin-1 or DMSO at equal v/v for 4 h. 30 min prior to the experimental endpoint cells were incubated with Lysotracker Deep Red to stain for acidic vesicles, fixed and counterstained for the nucleus using Hoechst 33,342. Shown in the left panel are representative images of Mφ2, while the middle panel displays the quantification of Lysotracker positive areas (log2FC Lysotracker area to DMSO) and the right panel the quantification of Mtb colocalization with Lysotracker positive vesicles. Scale bar annotates 5 µm. Each dot represents a single donor (4 donors in total) and depicts the mean ± standard deviation of 3 replicates. Shown are median and 95% confidence intervals (middle panel) or median by gray bars (right panel). Statistical significance was tested using a RM one-way ANOVA with Dunnett’s multiple comparison test.
To assess whether the reduction in Mtb outgrowth induced by Fluspirilene and Pimozide could also be associated with an increase in lysosomal activity we first examined the nuclear accumulation of transcription factor EB (TFEB), a master regulator of the coordinated lysosomal expression and regulation (CLEAR) gene network, as well as autophagy51,52. Nuclear intensity of TFEB was quantified in Mtb-infected Mφ2 after 4 h of treatment with Fluspirilene, Pimozide or Torin-1 as positive control53, using confocal microscopy (Fig. 3B, left panel). A highly significant increase in nuclear TFEB was observed for both Fluspirilene and Pimozide, even to a similar extent as the positive control Torin-1 (Fig. 3B, right panel, and Table S2). To investigate the lysosomal response in more detail we employed the lysosomal tracer Lysotracker. DsRed-Mtb-infected Mφ2 were treated with Fluspirilene and Pimozide for 4 h and the lysosomal area and localization of bacteria in lysosomes was quantified (Fig. 3C, left panel). Pimozide tended to induce an increase in lysosomal area, in contrast to Fluspirilene (Fig. 3C, middle panel). Additionally, Fluspirilene and Pimozide induced a mild, though statistically not significant average increase in colocalization of bacteria and lysosomes compared to DMSO (Fig. 3C, right panel, and Table S2).
Collectively, these results suggest that the lysosomal response key regulator TFEB and likely also the autophagic response are involved in enhancing host defense induced by diphenylbutylpiperidines, which restricts outgrowth of intracellular Mtb. Notwithstanding, the observed limited effect sizes for some of these processes suggested to us that these mechanisms likely do not fully account for the potent HDT activity of Fluspirilene and Pimozide against intracellular Mtb. We therefore postulated that other mechanisms of action are likely involved in the control of intracellular bacteria upon treatment with Fluspirilene and Pimozide.
Fluspirilene and Pimozide inhibit STAT5 function and Pimozide additionally reduces the presence of cytokine-inducible SH2-containing protein (CISH) on Mtb phagosomes
Because Pimozide has been reported to inhibit STAT5 function by dephosphorylation54, and work by Queval, Song55 recently uncovered a STAT5-mediated control of phagosomal acidification induced by Mtb, we explored functional inhibition of STAT5 by diphenylbutylpiperidines as a potential mode of action to control intracellular Mtb. First, the effect of 4-h treatment with diphenylbutylpiperidines on nuclear presence of phosphorylated STAT5 (P-STAT5) was investigated in Mtb-infected Mφ2 using confocal microscopy (Fig. 4A, left panel). Both Fluspirilene and Pimozide significantly decreased the nuclear presence of P-STAT5 Fig. 4A, middle and right panel, and Table S2). To further corroborate our finding that Fluspirilene and Pimozide lowered nuclear P-STAT5 quantity and hence its transcriptional activity, we analyzed the expression levels of cytokine-inducible SH2-containing protein (CISH), a transcriptional target of STAT543. We confirmed the observation by Queval, Song25 that Mtb infection increases CISH transcript levels in our Mtb-Mφ2 model after 4 h (Fig. 4B). Unexpectedly, Fluspirilene increased CISH transcript levels, even to a higher extent than the positive control GM-CSF56, while Pimozide did not affect CISH transcript expression levels, despite the compound's’ effects on P-STAT5 (Fig. 4B). We therefore quantified colocalization of CISH protein with Mtb, since the presence of CISH on the Mtb phagosome has been associated with bacterial survival55. Pimozide treatment caused a significant decrease of CISH fluorescence intensity per bacterium within the 4 h time-period, but Fluspirilene did not clearly show a difference compared to DMSO (Fig. 4C and Table S2).

Fluspirilene and Pimozide inhibit STAT5 function and Pimozide additionally reduces the presence of cytokine-inducible SH2-containing protein (CISH) on Mtb phagosomes. (A) Confocal microscopy of DsRed-expressing Mtb-infected Mφ2 treated with 10 µM of Fluspirilene, Pimozide or DMSO at equal v/v for 4 h. Cells were fixed at the experimental endpoint, permeabilized using 0.1% Triton-X, stained for P-STAT5 and counterstained for the nucleus and F-actin using Hoechst 33,342 and Phalloidin, respectively. Shown in the left panel are representative images of Mφ2, while the middle panel shows violin plots representing all nuclei quantified (n = 73, n = 77 and n = 75 for DMSO, Fluspirilene and Pimozide, respectively) of a representative donor with median and interquartile range indicated and the right panel displays the log2FC of median nuclear P-STAT5 intensity per donor normalized to DMSO (5 donors in total) with median and 95% confidence intervals indicated. Scale bar annotates 5 µm. Dotted line indicates median of DMSO. Statistical significance was tested using Kruskal–Wallis test with Dunn’s multiple comparison test (middle panel) (** = p-value < 0.01, *** = p-value < 0.001 and **** = p-value < 0.0001) or RM one-way ANOVA with Dunnett’s multiple comparison test (* = p-value < 0.05). (B) Mφ2 derived from 2 donors were mock- or Mtb-infected and Mtb-infected Mφ2 were subsequently treated with 10 µM of Fluspirilene, Pimozide, GM-CSF (50 ng/ml) as positive control or DMSO at equal v/v for 4 h. Transcript levels of Cytokine-inducible SH2-containing protein (CISH) were determined in duplicate using qRT-PCR before (0 h baseline) and 4-h post-infection. Data was normalized to GAPDH (ΔCt). Each dot represents a single donor and displays the log2FC expression levels of CISH in response to treatment compared to their respective baseline control (T0) (ΔΔCt). Horizontal lines indicate median expression levels and dotted line indicates the median of Mtb-infected Mφ2 treated with DMSO. (C) Confocal microscopy of DsRed-expressing Mtb-infected Mφ2 treated with 10 µM of Fluspirilene, Pimozide or DMSO at equal v/v for 4 h. Cells were fixed at the experimental endpoint, permeabilized using 0.1% Triton-X, stained for CISH and counterstained for the nucleus and F-actin using Hoechst 33,342 and Phalloidin, respectively. Shown in the left panel are representative images of Mφ2, while the middle panel shows violin plots representing all bacteria quantified (n = 182, n = 179 and n = 217 for DMSO, Fluspirilene and Pimozide, respectively) of a representative donor with median and interquartile range indicated and the right panel displays the log2FC of median CISH integrated intensity per bacterium per donor normalized to DMSO (5 donors in total) with median and 95% confidence intervals indicated. Scale bar annotates 5 µm. Dotted line indicates median of DMSO. Statistical significance was tested using Kruskal–Wallis test with Dunn’s multiple comparison test (middle panel) (**** = p-value < 0.0001) or RM one-way ANOVA with Dunnett’s multiple comparison test (* = p-value < 0.05).
Taken together, these data suggest that Fluspirilene and Pimozide both decrease P-STAT5 protein levels in the nucleus. In addition, although the effects on intracellular Mtb bacteria did not correlate with differential expression of the STAT5 target CISH at the transcript level, Pimozide lowered CISH protein presence on the Mtb phagosome. Thus, both Fluspirilene and Pimozide likely target intracellular Mtb by a mechanism involving P-STAT5, which for Pimozide, but not Fluspirilene, includes routing through the CISH effector pathway. These results suggest that structurally highly related HDT compounds can nevertheless subtly differ in their mode of actions against intracellular infection.
Pimozide induces ROS/RNS production and antioxidants impair bacterial killing by Pimozide as well as Fluspirilene
Next to autophagy and lysosomal degradation, reactive oxygen species (ROS) and reactive nitrogen species (RNS) represent additional mechanisms that could play a key role in controlling intracellular Mtb. Of note, Pimozide has been reported to induce ROS production in various cell types57,58,59, prompting us to explore the role of radical species in the mode of action of both Fluspirilene and Pimozide. Using a general oxidative stress indicator (CM-H2DCFDA), we measured ROS/RNS production in uninfected Mφ2 (due to biosafety level 3-restrictions) during treatment with Fluspirilene and Pimozide. Pimozide but not Fluspirilene treatment clearly increased ROS/RNS production (Fig. 5A and B, left panel). To confirm that probe conversion was caused by cellular produced radical species, the probe was incubated with Pimozide in a cell-free system, which showed no significant effect (Fig. 5C). To examine whether we could confirm the induction of ROS/RNS production by Pimozide, we added the antioxidant N-acetylcysteine (NAC) to the Pimozide treatment regimen (Fig. 5B, right panel). In 7 out of 9 donors Pimozide-induced ROS/RNS production was impaired by the addition of NAC, indicating that the probe conversion indeed reflects elevated ROS/RNS production.

Pimozide induces ROS/RNS production and antioxidants impair bacterial killing by Pimozide as well as Fluspirilene. (A) Mφ2 were pulsed for 30 min with 5 µM of probe CM-H2DCFDA followed by exposure to 10 µM Fluspirilene or Pimozide, 50 µM TBHP as positive control, or DMSO at equal v/v. Production of reactive oxygen species (ROS) was monitored by measuring Fluorescence intensity (522 nm) over a time course of two hours. Each dot depicts the mean of 3 replicates of a representative donor (7 donors in total). (B) Mφ2 were pulsed for 30 min with 5 µM of probe CM-H2DCFDA followed by exposure to 10 µM Fluspirilene or Pimozide, 50 µM TBHP as positive control or DMSO at equal v/v for the duration of the experiment (left panel). Pimozide and DMSO were additionally combined with 5 mM of the antioxidant N-acetyl cysteine (NAC) (right panel). Each dot represents the area under the curve (AUC) of a single donor (7 donors in left panel and 9 donors in right panel) and depicts the mean of 3 to 6 replicates. Median with 95% confidence intervals are shown. Statistical significance was tested using a Wilcoxon matched-pairs signed rank test with post-hoc Benjamini–Hochberg correction (left panel) (* = q-value < 0.1) or Wilcoxon matched-pairs signed rank test (right panel) (** = p-value < 0.01). (C) Probe CM-H2DCFDA (5 µM) fluorescence measured in the presence of 10 µM of Pimozide or DMSO at equal v/v in the absence of cells. Bars display the mean ± standard deviation of 3 replicates and represent the fluorescence intensity measured after 60 min of incubation in one single experiment. Statistical significance was tested using an unpaired t test with Welch’s correction. (D) CFU assay of Mtb-infected Mφ2 and treated with 10 µM of Fluspirilene (left panel) or Pimozide (right panel) combined with anti-oxidants (5 mM of NAC, 10 µM of MitoTempo, 25 µM of Ebselen or 1 mM of L-NMMA) or DMSO at equal v/v for 24 h. Each dot represents a single donor (7 donors in total) and depicts the mean of 3 to 6 replicates. Dotted lines indicate DMSO set at 100% with median indicated by gray bars. Statistical significance was tested using a RM one-way ANOVA with Dunnett’s multiple comparison test (* = p-value < 0.05).
To study the importance of Pimozide-induced ROS/RNS production in its control of intracellular bacterial infection, Mtb-infected Mφ2 were treated with either Pimozide or Fluspirilene in combination with various ROS/RNS inhibitors, namely: NAC, Ebselen (a NOX inhibitor and glutathione peroxidase mimic60), MitoTEMPO (a mitochondria-targeted radical scavenger61), and L-NMMA (a nitric oxide synthase (NOS) inhibitor62) (Fig. 5D and Table S2). NAC, and L-NMMA, but not Ebselen and MitoTEMPO, significantly inhibited the HDT effects of Pimozide (Fig. 5D, right panel). Interestingly, we also observed a significant effect of MitoTEMPO but not NAC, L-NMMA or Ebselen, on Fluspirilene (Fig. 5D, left panel), indicating a -possibly differential- role for ROS/RNS in the mode of action of both Fluspirilene and Pimozide. NAC, MitoTEMPO, L-NMMA and Ebselen treated Mtb-infected Mφ2 all showed some reduced bacterial outgrowth, which was significant for NAC and Ebselen (Supplementary Fig. 1 and Table S2), further emphasizing the role of ROS/RNS in intracellular bacterial control, which is supported by their antagonistic effect on Pimozide and Fluspirilene induced infection control.
In conclusion, we have identified two clinically approved drugs, Fluspirilene and Pimozide, which we show to have novel and significant potential as host-directed therapeutics for the treatment of intracellular bacterial pathogens such as Mtb and Stm, mechanistically operating by multiple mechanisms of action. We show that both Fluspirilene and Pimozide significantly alter the lysosomal response and tend to increase autophagic targeting of Mtb, likely via nuclear translocation of TFEB. Furthermore, our findings support two additional modes of action, particularly associated with Pimozide-mediated activity. Firstly, Fluspirilene and Pimozide counteract Mtb-induced STAT5 phosphorylation, but only Pimozide thereby reduced the presence of CISH on the Mtb phagosome, thus probably regulating its acidification55. Secondly, Pimozide induced measurable ROS/RNS production and its efficacy was impacted by ROS/RNS inhibitors. Together these mechanisms likely work in concert (Fig. 6) to reduce intracellular bacterial outgrowth and thus could be targeted by adjunct HDT in difficult to treat intracellular infections such as Mtb and Stm and likely also related pathogens.

Model of the modes of action of Fluspirilene and Pimozide. Both Fluspirilene and Pimozide increased the localization of Mtb in autophagy-related vesicles implying they induce selective autophagy, i.e. xenophagy (I). Although increased ROS/RNS production was significantly induced by Pimozide only, antioxidants impaired the efficacy of Pimozide and to a lesser extent also Fluspirilene (II). Fluspirilene and Pimozide both inhibited STAT5 activity and Pimozide consequently reduced CISH localization on the Mtb containing vesicle (III). Lastly, Fluspirilene and to a larger extent Pimozide, increased nuclear TFEB localization concomitant with an increased lysosomal response (IV). Black arrows indicate the general process of Mtb phagocytosis and subsequent events, white arrows show compound mediated activation or inhibition of targets and green and red lines depict signaling pathways and protein interactions with reduced or increased bacterial outgrowth as outcome, respectively.
Discussion
In this study, we aimed to find new host-directed therapy (HDT) candidate drugs for the treatment of (drug resistant) TB and other difficult to treat intracellular bacterial infections, and identified two structural analogues of the diphenylbutylpiperidine-class, Fluspirilene and Pimozide, with strong efficacy against intracellular Mtb and Stm. We next validated their HDT potential in Mtb and Stm primary human macrophages with either pro- or anti-inflammatory phenotypes. Importantly, we corroborated their activity against intracellular Mtb in a cross-species non-human model using bronchoalveolar lavage fluid macrophages, which are a rich source of alveolar macrophages (AMφ), the primary target cells for Mtb. This cross-species efficacy underscored functional conservation of host target molecules and independently validated their effects in human Mtb infected cells. Additionally, the strong HDT activity of Fluspirilene and Pimozide was confirmed also against clinical isolates of multi-drug resistant (MDR)-Mtb strains, and moreover acted in a synergistic and/or additive mode with a suboptimal dose of Rifampicin. Extracellular bacterial proliferation itself was unaffected by these compounds, indicating that their targeting of host mechanisms is responsible for their activity. Furthermore, the high efficacy shown against Stm, indicates that these drugs could be repurposed as treatment against a wider range of intracellular pathogens as already shown for other HDTs and pathogens63.
Interestingly, we propose to have found several modes of action employed by Fluspirilene and Pimozide, including modulation of the lysosomal response, autophagy, induction of ROS/RNS production and finally the inhibition of STAT5 with consequently decreased localization of CISH protein on the Mtb phagosome. We postulate that these mechanisms cooperate in concert via multiple pathways to reduce intracellular bacterial outgrowth. Drugs acting via multiple effector mechanisms might be desirable over single mechanism of action (MOA), because developing bacterial resistance against multiple host effector mechanisms simultaneously will be extremely hard to achieve (summarized in Fig. 6).
Fluspirilene and Pimozide are potent inhibitors of several dopamine receptors and calcium channels and are used clinically to treat psychotic disorders, like schizophrenia, psychosis and Tourette syndrome41,64. Some antipsychotic drugs have already been shown to exert (host directed) antimicrobial activity. For example, phenothiazine-derived drugs, which include Trifluorperazine, as well as butyrophenone derivatives, with Haloperidol as a well-known example, have therapeutic potential against several pathogens as we and others have shown previously22,26,65,66. The diphenylbutylpiperidine-class of drugs has also been studied, revealing host-directed effects of Pimozide against both facultative and obligate intracellular pathogens, Listeria monocytogenes and Toxoplasma gondii respectively67,68. Also, Fluspirilene has been shown to potentiate antimicrobial activity against several bacteria, but only in a direct antibiotic manner69,70. Despite these observations, we found no direct antimicrobial effect of Fluspirilene (or Pimozide) on either Mtb or Stm. This is likely reconciled by the fact that Fluspirilene displayed minimum inhibitory concentrations (MICs) of > 80 µM for E. coli and K. pneumoniae which both belong to the same order as Stm, namely Enterobacterales, whereas in our work we employed significantly lower (10 µM) concentrations at which strong HDT but no direct anti-bacterial effects were observed69.
Our work suggests that four different host effector mechanisms are likely to play a role in the treatment-efficacy of Fluspirilene and Pimozide. A first mechanism we demonstrated was that Fluspirilene and Pimozide activated autophagy in Mtb-infected Mφ and increased the localization of Mtb in autophagic vesicles (Fig. 3A). Although this was not investigated in further detail, we hypothesize that Ca2+ signaling could be important to this effector mechanism. Both Fluspirilene and Pimozide antagonize calcium channel activity and can lower intracellular Ca2+ levels, thereby inactivating Calpain that leads to the induction of autophagy41,64,71,72. In support of this, a screen of Fluspirilene analogues showed that Ca2+ channel inhibition was necessary for their ability to induce autophagy in a neuroglioma cell line, since analogues that lacked the ability to block Ca2+ channels lacked autophagy-inducing activity71. Importantly, the host Ca2+ signaling pathway is also manipulated directly by Mtb to inhibit autophagy73. Whether Ca2+-related effects also play a role in HDT activity of Fluspirilene and Pimozide against intracellular Mtb and Stm, however, remains currently unknown and will require future studies. Recently, new diphenylbutylpiperidine analogues with stronger autophagy-inducing capabilities were developed that represent interesting novel HDT for future studies74.
The second mechanism that Fluspirilene and Pimozide are likely to employ is the lysosomal response (Fig. 3). An additional new finding with mechanistic implications was that treatment with Fluspirilene and Pimozide strongly increased the intranuclear presence of TFEB (Fig. 3B). This transcriptional regulator controls a coordinated lysosomal response75, as well as autophagy76. This ability of Fluspirilene and Pimozide was, to the best of our knowledge, hitherto unknown. TFEB translocation has been observed for drugs of the phenothiazine-class including Trifluorperazine77, suggesting this might represent common functionality of several different antipsychotic drugs.
The third mechanism we uncovered was phagosomal acidification, a process vital in the host response against intracellular bacteria, which is inhibited by the protein CISH that is under transcriptional control of STAT555. This pathway is exploited by Mtb which induces GM-CSF to activate STAT5, leading to enhanced CISH expression and consequent V-ATPase degradation55. Although treatment with both Fluspirilene and Pimozide led to a reduction of nuclear STAT5, we could experimentally confirm the decrease in CISH protein on Mtb containing vesicles only for Pimozide (Fig. 4A and C). Further research will be needed to further unravel the subtle differences in precise MOAs between Pimozide and Fluspirilene, but this is beyond the scope of the current work.
As a fourth effector mechanism, we found that Pimozide strongly induced ROS/RNS production. Mechanistically, the efficacy of both Pimozide and Fluspirilene towards intracellular Mtb was inhibited by ROS/RNS inhibitors. Of these two diphenylbutylpiperidines, only Pimozide is known to induce ROS/RNS production and to inhibit the expression of antioxidant genes, like catalase, in vitro as well as in vivo57,78. Interestingly, similar to the results from Cai, Zhou57, addition of n-acetyl-cysteine (NAC), a general ROS scavenger, partly inhibited the Pimozide induced increase in ROS/RNS levels by human macrophages, and reduced bacterial survival (Fig. 5B and D). Since multiple signaling pathways could contribute to the ROS/RNS production caused by Pimozide, we investigated this in more detail. The respiratory burst induced upon phagocytosis did not seem to be involved since Ebselen, a NADPH oxidase (NOX) inhibitor79, did not restore bacterial survival. Because L-NMMA, selective for nitric oxide synthase (NOS) affected Pimozide’s efficacy, a role for nitric oxide (NO) seems likely. It has become evident that the functions of ROS and NO are intertwined and that inhibition of one leads to cross-inhibition of the other, supporting this possibility80,81.
Taken together, we have identified four potential mechanistic effector pathways each of which is regulated by Fluspirilene and/or Pimozide, and which likely act in concert to reduce intracellular bacterial outgrowth. Combinatorial treatment regimens using multiple approaches including HDT as well as anti-bacterial molecules are considered indispensable to eradicating TB82. An interesting finding was that although Fluspirilene and Pimozide displayed additive effects with a low dose regimen of Rifampicin, this was not observed with Isoniazid. Isoniazid is a prodrug and requires conversion by the Mtb catalase-peroxidase (KatG) enzyme to its active form, resulting in the production of bacteria-derived reactive species49,83. These radicals have both direct and indirect antimicrobial properties and in the latter case host ROS/RNS production can lead to the induction of autophagy, which is capable of targeting Mtb49.
The repurposing of drugs with known safety profiles presents attractive and significant advantages in terms of drug development, including safety and toxicity testing and clinical evaluation. One important consideration is the feasibility of using these drugs at an effective yet safe dose for new indications. To our knowledge, data on Fluspirilene is sparse, but information regarding dosing and toxicity for Pimozide is available. The FDA recommends a maximum dose of 10 mg/day84, and doses in the range of 1 to 12 mg/day reach a serum level of Pimozide in the nanomolar range85. Oral delivery might not be optimally effective as treatment for pulmonary TB, and inhalation therapy, e.g., by aerosolic nebulizers, would be one way to achieve an optimally effective local concentration, while circumventing the systemic toxicity often associated with orally administered drugs86. As a proof of concept, Gupta et al. have shown that inhalable particles consisting of Rapamycin (a HDT drug) and two antibiotics cleared Mtb in mice in which case the Rapamycin concentration achieved in the lungs was 100 times higher compared to intravenous injection87.
Since the continuing rise of global drug resistance will affect the treatment of many bacterial infections, approaches complementary to bacterial-directed strategies can offer important supplemental approaches. We have demonstrated the novel HDT potential of two approved antipsychotic drugs, Fluspirilene and Pimozide, against Mtb and Stm, two important but unrelated intracellular pathogens. Our results provide new insights into the molecular and functional effects of these two diphenylbutylpiperidines on key mechanisms of host defense, particularly: autophagy, lysosomal acidification, ROS/RNS generation and phagosome maturation via STAT5/CISH inhibition. We show that Fluspirilene and Pimozide target these host responses, by similar but subtly different MOAs, which is accompanied by reduced intracellular outgrowth of Mtb and Stm in human cells. Based on these findings, we propose that the class of diphenylbutylpiperidines could be repurposed as novel HDT drugs for both TB and salmonellosis and further explored as host-directed compounds against other intracellular pathogens.
Data availability
The datasets generated and analyzed during the current study are not deposited in external repositories but are included as supplementary file or available from the corresponding author on reasonable request.
References
Turner, R. D. & Bothamley, G. H. Cough and the transmission of tuberculosis. J. Infect. Dis. 211(9), 1367–1372 (2015).
WHO. Global Tuberculosis Report 2020 2020 (World Health Organization, 2020).
Coppola, M. & Ottenhoff, T. H. Genome wide approaches discover novel Mycobacterium tuberculosis antigens as correlates of infection, disease, immunity and targets for vaccination. Semin. Immunol. 39, 88–101 (2018).
Andersen, P. & Doherty, T. M. The success and failure of BCG - implications for a novel tuberculosis vaccine. Nat. Rev. Microbiol. 3(8), 656–662 (2005).
Gilchrist, J. J., MacLennan, C. A. & Hill, A. V. Genetic susceptibility to invasive Salmonella disease. Nat. Rev. Immunol. 15(7), 452–463 (2015).
Majowicz, S. E. et al. The global burden of nontyphoidal Salmonella gastroenteritis. Clin. Infect. Dis. 50(6), 882–889 (2010).
Klemm, E. J. et al. Emergence of host-adapted Salmonella Enteritidis through rapid evolution in an immunocompromised host. Nat. Microbiol. 1, 15023 (2016).
TB Alliance Pipeline. https://www.tballiance.org/portfolio.
Conradie, F. et al. Treatment of highly drug-resistant pulmonary tuberculosis. N. Engl. J. Med. 382(10), 893–902 (2020).
Alliance, T. Pretomanid and BPaL Regimen for Treatment of Highly Resistant Tuberculosis. Oral presentation at Antimicrobial Drugs Advisory Committee (2019).
Charyeva, Z. et al. What works best for ensuring treatment adherence. Lessons from a social support program for people treated for tuberculosis in Ukraine. PLoS ONE 14(8), e0221688 (2019).
Machelart, A. et al. Host-directed therapies offer novel opportunities for the fight against tuberculosis. Drug Discov. Today 22(8), 1250–1257 (2017).
Kaufmann, S. H. E. et al. Host-directed therapies for bacterial and viral infections. Nat. Rev. Drug. Discov. 17(1), 35–56 (2018).
Kilinc, G. et al. Host-directed therapy to combat mycobacterial infections*. Immunol. Rev. 301, 62–83 (2021).
Nair, S. et al. The PPE18 of Mycobacterium tuberculosis interacts with TLR2 and activates IL-10 induction in macrophage. J. Immunol. 183(10), 6269–6281 (2009).
Zhou, K. L. et al. Mycobacterial mannose-capped lipoarabinomannan: A modulator bridging innate and adaptive immunity. Emerg. Microbes. Infect. 8(1), 1168–1177 (2019).
Carranza, C. & Chavez-Galan, L. Several routes to the same destination: Inhibition of phagosome-lysosome fusion by Mycobacterium tuberculosis. Am. J. Med. Sci. 357(3), 184–194 (2019).
Hmama, Z. et al. Immunoevasion and immunosuppression of the macrophage by Mycobacterium tuberculosis. Immunol. Rev. 264(1), 220–232 (2015).
Ly, A. & Liu, J. Mycobacterial virulence factors: Surface-exposed lipids and secreted proteins. Int. J. Mol. Sci. 21(11), 3985 (2020).
Huang, D. & Bao, L. Mycobacterium tuberculosis EspB protein suppresses interferon-gamma-induced autophagy in murine macrophages. J. Microbiol. Immunol. Infect. 49(6), 859–865 (2016).
Kuijl, C. et al. Intracellular bacterial growth is controlled by a kinase network around PKB/AKT1. Nature 450(7170), 725 (2007).
Korbee, C. J. et al. Combined chemical genetics and data-driven bioinformatics approach identifies receptor tyrosine kinase inhibitors as host-directed antimicrobials. Nat. Commun. 9(1), 358 (2018).
Moreira, J. D. et al. Functional inhibition of host histone deacetylases (HDACs) enhances in vitro and in vivo anti-mycobacterial activity in human macrophages and in Zebrafish. Front. Immunol. 11, 36 (2020).
Jayaswal, S. et al. Identification of host-dependent survival factors for intracellular Mycobacterium tuberculosis through an siRNA screen. PLoS Pathog. 6(4), e1000839 (2010).
Kumar, D. et al. Genome-wide analysis of the host intracellular network that regulates survival of Mycobacterium tuberculosis. Cell 140(5), 731–743 (2010).
Sundaramurthy, V. et al. Integration of chemical and RNAi multiparametric profiles identifies triggers of intracellular mycobacterial killing. Cell Host Microbe. 13(2), 129–142 (2013).
van der Vaart, M. et al. The DNA damage-regulated autophagy modulator DRAM1 links mycobacterial recognition via TLR-MYD88 to autophagic defense [corrected]. Cell Host Microbe. 15(6), 753–767 (2014).
Gutierrez, M. G. et al. Autophagy is a defense mechanism inhibiting BCG and Mycobacterium tuberculosis survival in infected macrophages. Cell 119(6), 753–766 (2004).
Gomes, L. C. & Dikic, I. Autophagy in antimicrobial immunity. Mol. Cell 54(2), 224–233 (2014).
Singh, S. B. et al. Human IRGM induces autophagy to eliminate intracellular mycobacteria. Science 313(5792), 1438–1441 (2006).
Harris, J. & Keane, J. How tumour necrosis factor blockers interfere with tuberculosis immunity. Clin. Exp. Immunol. 161(1), 1–9 (2010).
Watson, R. O., Manzanillo, P. S. & Cox, J. S. Extracellular M. tuberculosis DNA targets bacteria for autophagy by activating the host DNA-sensing pathway. Cell 150(4), 803–815 (2012).
Magee, M. J. et al. Reduced prevalence of latent tuberculosis infection in diabetes patients using metformin and statins. Eur. Respir. J. 53(3), 1801695 (2019).
Lee, Y. J. et al. The effect of metformin on culture conversion in tuberculosis patients with diabetes mellitus. Korean J. Int. Med. 33(5), 933–940 (2018).
Naicker, N., Sigal, A. & Naidoo, K. Metformin as host-directed therapy for TB treatment: Scoping review. Front. Microbiol. 11, 435 (2020).
Guerra-De-Blas, P. D. et al. Potential effect of statins on Mycobacterium tuberculosis infection. J. Immunol. Res. 2018, 1–14 (2018).
Shakya, A., Bhat, H. R. & Ghosh, S. K. Update on nitazoxanide: A multifunctional chemotherapeutic agent. Curr. Drug Discov. Technol. 15(3), 201–213 (2018).
Napier, R. J. et al. Imatinib-sensitive tyrosine kinases regulate mycobacterial pathogenesis and represent therapeutic targets against tuberculosis. Cell Host Microbe. 10(5), 475–485 (2011).
Bruns, H. et al. Abelson tyrosine kinase controls phagosomal acidification required for killing of Mycobacterium tuberculosis in human macrophages. J. Immunol. 189(8), 4069–4078 (2012).
Napier, R. J. et al. Low doses of imatinib induce myelopoiesis and enhance host anti-microbial immunity. PLoS Pathog. 11(3), e1004770 (2015).
Gould, R. J. et al. Antischizophrenic drugs of the diphenylbutylpiperidine type act as calcium channel antagonists. Proc. Natl. Acad. Sci. U. S. A. 80(16), 5122–5125 (1983).
Verreck, F. A. et al. Phenotypic and functional profiling of human proinflammatory type-1 and anti-inflammatory type-2 macrophages in response to microbial antigens and IFN-gamma- and CD40L-mediated costimulation. J. Leukoc. Biol. 79(2), 285–293 (2006).
Gillinder, K. R. et al. Direct targets of pSTAT5 signalling in erythropoiesis. PLoS ONE 12(7), e0180922 (2017).
Schindelin, J. et al. Fiji: an open-source platform for biological-image analysis. Nat. Methods 9(7), 676–682 (2012).
McQuin, C. et al. Cell profiler 3.0: Next-generation image processing for biology. PLoS Biol. 16(7), e2005970 (2018).
Livak, K. J. & Schmittgen, T. D. Analysis of relative gene expression data using real-time quantitative PCR and the 2−ΔΔCT method. Methods 25(4), 402–408 (2001).
Mishra, R. et al. Targeting redox heterogeneity to counteract drug tolerance in replicating Mycobacterium tuberculosis. Sci. Transl. Med. 11(518), eaaw6635 (2019).
Verreck, F. A. et al. Human IL-23-producing type 1 macrophages promote but IL-10-producing type 2 macrophages subvert immunity to (myco)bacteria. Proc. Natl. Acad. Sci. U. S. A. 101(13), 4560–4565 (2004).
Kim, J. J. et al. Host cell autophagy activated by antibiotics is required for their effective antimycobacterial drug action. Cell Host Microbe. 11(5), 457–468 (2012).
Zhang, L. et al. Small molecule regulators of autophagy identified by an image-based high-throughput screen. Proc. Natl. Acad. Sci. U. S. A. 104(48), 19023–19028 (2007).
Settembre, C. et al. TFEB controls cellular lipid metabolism through a starvation-induced autoregulatory loop. Nat. Cell Biol. 15(6), 647–658 (2013).
Di Malta, C., Cinque, L. & Settembre, C. Transcriptional regulation of autophagy: Mechanisms and diseases. Front. Cell Dev. Biol. 7, 114 (2019).
Zhitomirsky, B. et al. Lysosomotropic drugs activate TFEB via lysosomal membrane fluidization and consequent inhibition of mTORC1 activity. Cell Death Dis. 9(12), 1191 (2018).
Nelson, E. A. et al. The STAT5 inhibitor pimozide decreases survival of chronic myelogenous leukemia cells resistant to kinase inhibitors. Blood 117(12), 3421–3429 (2011).
Queval, C. J. et al. Mycobacterium tuberculosis controls phagosomal acidification by targeting CISH-mediated signaling. Cell Rep. 20(13), 3188–3198 (2017).
Lehtonen, A. et al. Granulocyte-macrophage colony-stimulating factor (GM-CSF)-induced STAT5 activation and target-gene expression during human monocyte/macrophage differentiation. J. Leukoc. Biol. 71(3), 511–519 (2002).
Cai, N. et al. The STAT3 inhibitor pimozide impedes cell proliferation and induces ROS generation in human osteosarcoma by suppressing catalase expression. Am. J. Transl. Res. 9(8), 3853–3866 (2017).
Chen, J. J. et al. Antipsychotic agent pimozide promotes reversible proliferative suppression by inducing cellular quiescence in liver cancer. Oncol. Rep. 42(3), 1101–1109 (2019).
Zielke, S. et al. Loperamide, pimozide, and STF-62247 trigger autophagy-dependent cell death in glioblastoma cells. Cell Death Dis. 9(10), 994 (2018).
Azad, G. K. & Tomar, R. S. Ebselen, a promising antioxidant drug: mechanisms of action and targets of biological pathways. Mol. Biol. Rep. 41(8), 4865–4879 (2014).
Dikalova, A. E. et al. Therapeutic targeting of mitochondrial superoxide in hypertension. Circ. Res. 107(1), 106–116 (2010).
Hibbs, J. B. Jr., Taintor, R. R. & Vavrin, Z. Macrophage cytotoxicity: Role for L-arginine deiminase and imino nitrogen oxidation to nitrite. Science 235(4787), 473–476 (1987).
Czyz, D. M. et al. Host-directed antimicrobial drugs with broad-spectrum efficacy against intracellular bacterial pathogens. MBio 5(4), e015344-14 (2014).
Shi, Q. et al. Mechanisms of action of autophagy modulators dissected by quantitative systems pharmacology analysis. Int. J. Mol. Sci. 21(8), 2855 (2020).
Andersson, J. A. et al. Combating multidrug-resistant pathogens with host-directed nonantibiotic therapeutics. Antimicrob. Agents Chemother. 62(1), e01943-17 (2018).
Nehme, H. et al. Antibacterial activity of antipsychotic agents, their association with lipid nanocapsules and its impact on the properties of the nanocarriers and on antibacterial activity. PLoS ONE 13(1), e0189950 (2018).
Lieberman, L. A. & Higgins, D. E. A small-molecule screen identifies the antipsychotic drug pimozide as an inhibitor of Listeria monocytogenes infection. Antimicrob. Agents Chemother. 53(2), 756–764 (2009).
Dittmar, A. J., Drozda, A. A. & Blader, I. J. Drug repurposing screening identifies novel compounds that effectively inhibit Toxoplasma gondii growth. Msphere 1(2), e00042-15 (2016).
Hind, C. K. et al. Evaluation of a library of FDA-approved drugs for their ability to potentiate antibiotics against multidrug-resistant gram-negative pathogens. Antimicrob. Agents Chemother. 63(8), e00769-19 (2019).
Cheng, Y. S. et al. Repurposing screen identifies unconventional drugs with activity against multidrug resistant Acinetobacter baumannii. Front. Cell. Infect. Microb. 8, 438 (2019).
Xia, H. G. et al. Control of basal autophagy by calpain1 mediated cleavage of ATG5. Autophagy 6(1), 61–66 (2010).
Vucicevic, L. et al. Mechanisms and therapeutic significance of autophagy modulation by antipsychotic drugs. Cell Stress 2(11), 282–291 (2018).
Garg, R. et al. Mycobacterium tuberculosis calcium pump CtpF modulates the autophagosome in an mTOR-dependent manner. Front. Cell. Infect. Microbiol. 10, 461 (2020).
Chen, G. et al. Synthesis and SAR study of diphenylbutylpiperidines as cell autophagy inducers. Bioorg. Med. Chem. Lett. 21(1), 234–239 (2011).
Sardiello, M. et al. A gene network regulating lysosomal biogenesis and function. Science 325(5939), 473–477 (2009).
Singh, N. et al. Antimycobacterial effect of IFNG (interferon gamma)-induced autophagy depends on HMOX1 (heme oxygenase 1)-mediated increase in intracellular calcium levels and modulation of PPP3/calcineurin-TFEB (transcription factor EB) axis. Autophagy 14(6), 972–991 (2018).
Zhang, Y. et al. Rescue of pink1 deficiency by stress-dependent activation of autophagy. Cell Chem. Biol. 24(4), 471–480 (2017).
Kim, U. et al. Pimozide inhibits the human prostate cancer cells through the generation of reactive oxygen species. Front. Pharmacol. 10, 1517 (2020).
Smith, S. M. et al. Ebselen and congeners inhibit NADPH oxidase 2-dependent superoxide generation by interrupting the binding of regulatory subunits. Chem. Biol. 19(6), 752–763 (2012).
Mullebner, A. et al. Interaction between mitochondrial reactive oxygen species, heme oxygenase, and nitric oxide synthase stimulates phagocytosis in macrophages. Front. Med. 4, 452 (2018).
West, A. P. et al. TLR signalling augments macrophage bactericidal activity through mitochondrial ROS. Nature 472(7344), 476-U543 (2011).
Young, C., Walzl, G. & Du Plessis, N. Therapeutic host-directed strategies to improve outcome in tuberculosis. Mucosal. Immunol. 13(2), 190–204 (2020).
Vilcheze, C. & Jacobs, W. R. The mechanism of isoniazid killing: Clarity through the scope of genetics. Annu. Rev. Microbiol. 61, 35–50 (2007).
(FDA), F.a.D.A. ORAP (Pimozide) (2011).
van der Weide, K. & van der Weide, J. The influence of the CYP3A4*22 polymorphism and CYP2D6 polymorphisms on serum concentrations of aripiprazole, haloperidol, pimozide, and risperidone in psychiatric patients. J. Clin. Psychopharmacol. 35(3), 228–236 (2015).
Brunaugh, A. D., Sharma, S. & Smyth, H. Inhaled fixed-dose combination powders for the treatment of respiratory infections. Expert Opin. Drug Deliv. 18(8), 1101–1115 (2021).
Gupta, A. et al. Preparation and preclinical evaluation of inhalable particles containing rapamycin and anti-tuberculosis agents for induction of autophagy. Pharm. Res. 33(8), 1899–1912 (2016).
Acknowledgements
We gratefully acknowledge Dr J. Bestebroer (VUMC, Amsterdam, The Netherlands) for mycobacterial reporter constructs and Dick van Soolingen and Kirsten Kremer (RIVM, Bilthoven, The Netherlands) for providing the MDR-Mtb strains. This project was funded by the European Union’s Seventh Programme for research, technological development and demonstration under Grant Agreement No. PhagoSys HEALTH-F4-2008-223451, grants from the Netherlands Organization for Health Research and Development (ZonMw-TOP Grant 91214038) and NWO Domain Applied and Engineering Sciences (NWO-TTW grant 13259). We acknowledge the support from FAPESP (Grant: 2017/03332-5) to CS fellowship. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
M.T.H., C.J.K., J.E., T.H.M.O. and M.C.H. designed the experiments. M.T.H., C.J.K., J.E., C.S., I.G., F.V., S.V., K.V.W., C.G.E., K.D., L.W. performed the experiments. M.T.H., C.J.K. and S.V. processed the experimental data and M.T.H., C.J.K., T.H.M.O. and M.C.H. contributed to the interpretation of the results. M.T.H., T.H.M.O. and M.C.H. wrote the manuscript and designed the figures. F.A.W.V. contributed to the interpretation of the results and reviewed the manuscript. T.H.M.O. and M.C.H. supervised the project. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Heemskerk, M.T., Korbee, C.J., Esselink, J.J. et al. Repurposing diphenylbutylpiperidine-class antipsychotic drugs for host-directed therapy of Mycobacterium tuberculosis and Salmonella enterica infections. Sci Rep 11, 19634 (2021). https://doi.org/10.1038/s41598-021-98980-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-98980-z
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
