
Abstract
The aim of this study was to clarify risk factors for esophageal candidiasis (EC) in immunocompetent patients in a community hospital. 7736 patients who underwent esophagogastroduodenoscopy at our hospital from April 2012 to July 2018 were enrolled. The relationships between EC and the following factors: age, gender, body mass index, lifestyle, lifestyle-related diseases, medication, and endoscopic findings were analyzed. EC was observed in 184 of 7736 cases (2.4% morbidity rate). Multivariate analysis revealed that significant risk factors for the development of EC were: diabetes mellitus {odds ratio (OR): 1.52}, proton pump inhibitor (PPI) use (OR: 1.69), atrophic gastritis (AG) (OR: 1.60), advanced gastric cancer (OR: 4.66), and gastrectomy (OR: 2.32). When severe EC (Kodsi grade ≥ II) was compared to mild EC (grade I), the most significant risk factors were advanced gastric cancer (OR: 17.6) and gastrectomy (OR: 23.4). When considering the risk of AG and PPI use with EC development, the risk increased as follows: AG (OR: 1.59), PPI use (OR: 2.25), and both (OR: 3.13). PPI use, AG, advanced gastric cancer and post-gastrectomy are critical risk factors for the development of EC. We suggest close monitoring for EC development when PPIs are administered to patients with these factors.
Similar content being viewed by others
Introduction
Esophageal candidiasis (EC) is the most common esophageal infection. It is caused by candida fungi that are normally present in the oral cavity and digestive tract1. Candida albicans (C. albicans), the most important fungal pathogen in humans, is a gastrointestinal commensal that forms colonies on the esophagus in up to 20% of people2. The incidence of EC is 0.3–5.2% in the general population3, but is much higher in patients with severe immunodeficiency, such as human immunodeficiency virus (HIV)-infected patients4. A study by Takahashi et al.5 found that the prevalence of EC among patients who underwent esophagogastroduodenoscopy in their cohort was 1.7% overall, but was 9.8% in patients with HIV infection. Although most EC cases are asymptomatic and discovered by chance during endoscopic examinations, some cases can cause symptoms such as painful swallowing, chest discomfort, bleeding ulcers, and stenosis with passage disorders.
Various co-morbidities are associated with EC including: diabetes mellitus, steroid or immunosuppressant use, malignant tumors, and acquired immune deficiency syndrome (AIDS) caused by HIV infection6. Proton pump inhibitors (PPIs), which are widely used for peptic ulcers, gastroesophageal reflux disease (GERD), and eradication therapy against Helicobacter pylori (H. pylori), have been reported to increase the risk of developing EC7,8,9. Importantly, EC is observed after PPI administration even in patients without underlying diseases that cause immunosuppression10. PPI can reduce gastric acid secretion, resulting in a state of achlorhydria in the stomach11 and the low-acid environment created by PPIs may affect the body’s antifungal activity against Candida.
Gastric and esophageal pathologies are often associated with the secretion dynamics of gastric acid. Esophageal hiatal hernia and GERD cause the backflow of gastric acid into the esophagus, increasing the acidity. Conversely, gastrectomy and atrophic gastritis caused by H. pylori infection reduces gastric acid secretion decreasing the acidity in the esophagus. Therefore, any pathology that affects the acid level in the esophagus may greatly influence the development of EC. However, the correlations between endoscopic findings regarding gastric and esophageal pathologies and EC have not been fully characterized.
The purpose of this study was to examine risk factors for the development of EC among immunocompetent patients in a community hospital, focusing on associations with gastric and esophageal pathologies. In addition, predictors for the development and severity of EC in these patients were also evaluated using medical records.
Methods
Study design
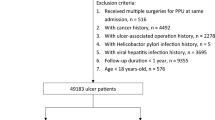
Patients who underwent esophagogastroduodenoscopy at Gihoku Kosei Hospital between April 2012 and July 2018 were retrospectively analyzed. They included both of inpatients and outpatients. Among the 18,153 procedures, 7736 patients were retained, after excluding duplications, and were included in this study. In the 7736 patients, 4271 had abdominal symptoms such as upper abdominal pain and 3465 were screened for gastric cancer. Patient histories (age, gender, lifestyles, comorbidities, and medication) prior to examination were recorded. This study protocol was approved by the Institutional Review Board of the Gihoku Kosei Hospital, Gifu, Japan (Reference No. 20200801). Informed consent was obtained from all patients before total colonoscopy examination for clinical research. The study was carried out in accordance with the Declaration of Helsinki.
EC was diagnosed based on typical endoscopic findings or pathological findings. Biopsy was conducted to distinguish EC from other diseases, such as cytomegalovirus infection, herpes simplex virus infection, and eosinophilic or inflammatory lesions. The Kodsi classification was used to categorize EC severity12. To assess gastric atrophy, the Kimura-Takemoto classification was applied13.
Statistical methods
Statistical analysis was performed using EZR14. The Pearson χ2 test was used for categorical data to compare the proportions of each candidate risk factor. Fisher’s exact test was applied to the categorical data when one of the categorical numbers was less than 10. Multivariate logistic regression analysis was used to analyze the independent risk factors for the development and severity of EC. Values of P < 0.05 were considered statistically significant.
Ethics
All subjects provided written informed consent before enrollment. The study protocol was approved by the Ethics Committee of Gihoku Kosei Hospital (Reference No. 20200801) and adhered to the tenets of the Declaration of Helsinki.
Results
Characteristics of patients
The characteristics of the 7736 patients were as follows: median age: 61.3 years (range, 15–105 years), gender: 3929 men (50.8%), and median body mass index (BMI): 23.0 kg/m2 (range, 10.7–37.3). Diabetes mellitus was found in 860 patients (11.1%). PPIs were taken by 1253 patients (16.2%). EC was observed in 184 of 7736 patients (2.4% incidence); this rate was similar to a previous report of regional general hospitals10. Moreover, 3161 patients had atrophic gastritis (40.9%) (Table 1).
Predictors for the development of EC
Univariate analysis showed that age over 65 years {odds ratio (OR): 1.95; P < 0.001), diabetes mellitus (OR: 1.85; P = 0.003), PPI use (OR: 2.2; P < 0.001), oral steroid use (OR: 2.96; P = 0.021), inhaled steroid use (OR: 3.62; P = 0.031), atrophic gastritis (OR: 1.63; P = 0.001), advanced gastric cancer (OR: 5.04; P < 0.001), and gastrectomy (OR: 2.48; P = 0.010) were significant risk factors for EC. BMI over 25 kg/m2 (OR: 0.51; P = 0.002) was independently associated with a decreased risk of EC. In contrast, GERD (OR: 0.83; P = 0.737) and esophageal hiatal hernia (OR: 0.55; P = 0.081) were not significant risk factors in this study (Table 2).
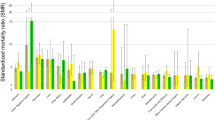
Multivariate analysis also revealed that diabetes mellitus {OR: 1.52; 95% confidence interval (CI), 1.01–2.29, P = 0.043}, PPI use (OR: 1.69; 95% CI, 1.19–2.41, P = 0.003), atrophic gastritis (OR: 1.60; 95% CI, 1.17–2.18, P = 0.003), advanced gastric cancer (OR: 4.66; 95% CI, 2.40–9.05, P < 0.001), and gastrectomy (OR: 2.32; 95% CI, 1.18–4.57, P = 0.015) were independent risk factors for developing EC. In contrast, obesity (BMI ≥ 25) reduced EC risk (OR: 0.53; 95% CI, 0.34–0.84, P = 0.006). There were no significant differences between the two groups with regard to steroid use (inhaled: P = 0.069, oral: P = 0.201, respectively) (Fig. 1).

Predictors of esophageal candidiasis by a multiple logistic regression analysis. The plot shows the odds ratios (black squares) and 95% confidence intervals (CIs). PPI proton pump inhibitor.
Predictors of EC severity
EC severity was evaluated using the Kodsi classification12. The severity of EC in the 184 patients examined in our cohort were: 146 patients with Kodsi grade I (79.3%), 20 with grade II (10.9%), 16 with grade III (8.7%), and 2 with grade IV (1.1%). EC patients were stratified as mild (grade I) or moderate/severe (grade II and higher). Patients with moderate/severe EC were more likely to have advanced gastric cancer (P = 0.003) and gastrectomy (P = 0.006) than patients with mild EC (Table 3). In multivariate analysis, advanced gastric cancer (OR: 17.6; 95% CI, 3.54–87.9, P < 0.001) and gastrectomy (OR: 23.4; 95% CI, 4.24–129, P < 0.001) were also identified as significant risk factors for developing sever EC. Atrophic gastritis (P = 0.078) and PPI use (P = 0.072) were not associated with EC severity in the present study (Fig. 2).

Predictors of disease severity of esophageal candidiasis by a multiple logistic regression analysis. The plot shows the odds ratios (black squares) and 95% confidence intervals (CIs) (horizontal lines). PPI proton pump inhibitor, GERD gastroesophageal reflux disease.
Impact of PPI use on the risk of EC in patients with atrophic gastritis
As both PPIs and atrophic gastritis cause reduced acidity, their combination may have a much greater impact on EC development than either alone. Therefore, we next examined whether PPI use may increase the risk for developing EC in patients with atrophic gastritis. The enrolled patients were stratified into the following 4 groups: patients without atrophic gastritis who did not receive PPI (control group, n = 3967), patients with atrophic gastritis who did not receive PPI (gastritis group, n = 2516), patients without atrophic gastritis who received PPI (PPI group, n = 608), and patients with atrophic gastritis who did receive PPI (gastritis plus PPI group, n = 645). The incidence of EC in each group was 1.6% (control group), 2.6% (gastritis group), 3.6% (PPI group), and 5.0% (gastritis plus PPI group). The OR with respect to the control was 1.59 (95% CI, 1.12–2.25), 2.25 (95% CI, 1.38–2.25), and 3.13 (95% CI, 2.03–4.83) for the gastritis group, PPI group, and gastritis plus PPI group, respectively (Table 4).
Discussion
The results of the present study clearly showed that diabetes mellitus, advanced gastric cancer, and PPI use are risk factors for developing EC among immunocompetent patients in our community hospital. This was consistent with results of previous studies6,7,8,9,10. In addition, we have demonstrated the first evidence that atrophic gastritis and gastrectomy are significant risk factors for the development of EC in immunocompetent patients. Importantly, the risk of developing EC increased when patients with atrophic gastritis were treated with PPI.
PPI use, atrophic gastritis, and gastrectomy are strongly associated with the creation of low-acid environments in the stomach (or remaining stomach in the case of gastrectomy). Atrophic mucosa does not produce normal amounts of acid. Stomach acidity is neutralized to a pH level of approximately 7.0 with increasing degree of mucosal atrophy15. Gastric pH is also reported to increase to a pH of 4.0–6.0 after PPI administration16. Therefore, PPI use and atrophic gastritis both contribute to a low-acid environment in the stomach and esophagus, which may increase the pathogenicity of Candida fungi. C. albicans can switch to its infectious pathogenic hyphal form in low-acid environments17. Elevation of pH by vagotomy is also associated with overgrowth of C. albicans in the gastric lumen18.
In addition to suppressing the secretion of gastric acid, PPI administration may also reduce host antifungal immunological responses. Natural killer cell activity against C. albicans in the spleen was shown to be inhibited by the PPI omeprazole19. Macrophages use intracellular proton pumps to maintain the acidic environments of endosomes and lysosomes, essential for fungal killing20,21. These results suggest that PPI administration could directly decrease the ability of the immune system to protect against Candida infection.
In the present study, EC patients were less likely to have a high BMI (≥ 25); however, the precise mechanism for this finding is unclear. In other diseases, obesity is a risk factor for infection22. Certainly, obesity is associated with diabetes mellitus, which we have shown to be an independent risk factor for EC6. However, lower BMI is reported to be an independent risk factor of Candida colonization in the oropharynx23. At least in elderly patients with many complications, malnutrition that causes immune dysfunction may increase the risk for Candida colonization. Future studies clarifying the impact of BMI or malnutrition on the development of EC should be conducted.
Esophageal hiatal hernia and GERD, both of which are often observed in obese patients, create an acidic environment in the esophagus. Therefore, we presumed that these pathologies increase antifungal activity in the esophageal mucosa and reduced the risk of EC; however, neither factor was reduced the risk of EC development in the present study. Therefore, it is likely that the absolute amount of gastric acid secretion in the stomach may be more critical for developing EC than the backflow of acid into the esophagus. To examine the impact of acid levels on the development of EC, the pH levels in both the stomach and esophagus should be evaluated in future studies.
Our study has several limitations. First, this was a retrospective study and we could not exclude bias that affects the development of EC. Second, the immune status of the enrolled patients was not fully assessed. The patients were assessed at a community hospital and none presented with readily identifiable immunodeficiency; however, immune activity and the presence of HIV infection were not examined. Finally, we did not evaluate the degree of atrophic mucosa in patients with atrophic gastritis and the status of H. pylori infection (naïve, present infection, or post eradication) has not been considered. Further investigation regarding these concerns could help us to identify the risk factors for EC in more detail.
In conclusion, atrophic gastritis was found to be an independent risk factor for the development of EC among immunocompetent patients in a community hospital. The risk in these patients was further increased when combined with PPI use. We hypothesize that this is due to the synergistic decrease in acid production that occurs in atrophic gastritis and is induced by PPIs. Immune inhibition by PPIs may also play a role in allowing Candida to flourish in this environment. PPIs, which strongly inhibit gastric acid secretion, are used extensively worldwide to treat acid-related disorders such as peptic ulcer and GERD. However, 25–75% of PPI use has been reported to be inappropriate24. Especially, it might be required caution when we use PPI for patients with atrophic gastritis, advanced gastric cancer or post-gastrectomy.
Conclusion
PPI use, atrophic gastritis, advanced gastric cancer and post-gastrectomy are critical risk factors for the development of EC. We suggest close monitoring for EC development when PPIs are administered to patients with these factors.
Abbreviations
- AIDS:
-
Acquired immune deficiency syndrome
- BMI:
-
Body mass index
- C. albicans :
-
Candida albicans
- CI:
-
Confidence interval
- EC:
-
Esophageal candidiasis
- GERD:
-
Gastroesophageal reflux disease
- HIV:
-
Human immunodeficiency virus
- H. pylori :
-
Helicobacter pylori
- OR:
-
Odds ratio
- PPI:
-
Proton pump inhibitors
References
Robertson, K. D. & Mehta, D. Esophageal Candidiasis. in StatPearls (StatPearls Publishing, 2019).
Pappas, P. G. et al. Clinical practice guideline for the management of candidiasis: 2016 update by the infectious diseases society of America. Clin. Infect. Dis. 62, e1–e50 (2016).
Mohamed, A. A., Lu, X. & Mounmin, F. A. Diagnosis and treatment of esophageal candidiasis: Current updates. Can. J. Gastroenterol. Hepatol 2019, 3585136 (2019).
Vazquez, J. A. Optimal management of oropharyngeal and esophageal candidiasis in patients living with HIV infection. HIV AIDS (Auckl) 2, 89–101 (2010).
Takahashi, Y. et al. Long-term trends in esophageal candidiasis prevalence and associated risk factors with or without HIV infection: Lessons from an endoscopic study of 80,219 patients. PLoS ONE 10, e0133589 (2015).
O’Rourke, A. Infective oesophagitis: Epidemiology, cause, diagnosis and treatment options. Curr. Opin. Otolaryngol. Head Neck Surg. 23, 459–463 (2015).
Larner, A. J. & Lendrum, R. Oesophageal candidiasis after omeprazole therapy. Gut 33, 860–861 (1992).
Chocarro Martínez, A. et al. Risk factors for esophageal candidiasis. Eur. J. Clin. Microbiol. Infect. Dis. 19, 96–100 (2000).
Daniell, H. W. Acid suppressing therapy as a risk factor for Candida esophagitis. Dis. Esophagus 29, 479–483 (2016).
Nassar, Y., Eljabbour, T., Lee, H. & Batool, A. Possible risk factors for Candida esophagitis in immunocompetent individuals. Gastroenterol. Res. 11, 195–199 (2018).
Corleto, V. D., Festa, S., Di Giulio, E. & Annibale, B. Proton pump inhibitor therapy and potential long-term harm. Curr. Opin. Endocrinol. Diabetes Obes. 21, 3–8 (2014).
Kodsi, B. E., Wickremesinghe, C., Kozinn, P. J., Iswara, K. & Goldberg, P. K. Candida esophagitis: A prospective study of 27 cases. Gastroenterology 71, 715–719 (1976).
Ohno, A. et al. Endoscopic severe mucosal atrophy indicates the presence of gastric cancer after Helicobacter pylori eradication -analysis based on the Kyoto classification. BMC Gastroenterol. 20, 1–7 (2020).
Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 48, 452–458 (2013).
Taguchi, Y. et al. Helicobacter pylori inhibits the secretory activity of gastric parietal cells in patients with chronic gastritis: An ultrastructural study. Scand. J. Gastroenterol. 32, 656–663 (1997).
Katz, P. et al. Daytime intragastric acid control: Post hoc analyses of esomeprazole 20 mg and over-the-counter proton-pump inhibitors. Ther. Adv. Gastroenterol. 8, 322–330 (2015).
Vylkova, S. et al. The fungal pathogen Candida albicans autoinduces hyphal morphogenesis by raising extracellular pH. MBio 2, e00055-11 (2011).
Brooks, J. R., Smith, H. F. & Pease, F. B. Bacteriology of the stomach immediately following vagotomy: The growth of Candida albicans. Ann. Surg. 179, 859–862 (1974).
Scaringi, L. et al. Activity inhibition of cytolytic lymphocytes by omeprazole. Scand. J. Immunol. 44, 204–214 (1996).
Lukacs, G. L., Rotstein, O. D. & Grinstein, S. Determinants of the phagosomal pH in macrophages. In situ assessment of vacuolar H(+)-ATPase activity, counterion conductance, and H+ ‘leak’. J. Biol. Chem. 266, 24540–24548 (1991).
Nanda, A. et al. Activation of proton pumping in human neutrophils occurs by exocytosis of vesicles bearing vacuolar-type H+-ATPases. J. Biol. Chem. 271, 15963–15970 (1996).
Huttunen, R. & Syrjänen, J. Obesity and the risk and outcome of infection. Int. J. Obes. 37, 333–340 (2013).
Mojazi Amiri, H., Frandah, W., Colmer-Hamood, J., Raj, R. & Nugent, K. Risk factors of Candida colonization in the oropharynx of patients admitted to an intensive care unit. J. Mycol. Médicale 22, 301–307 (2012).
Forgacs, I. & Loganayagam, A. Overprescribing proton pump inhibitors. BMJ 336, 2–3 (2008).
Acknowledgements
We profoundly appreciate Ms. Yukiko Goda for her valuable technical assistance.
Funding
This research received no external funding.
Author information
Authors and Affiliations
Contributions
Conceptualization: H.O., S.A. Formal analysis: H.O., S.A., Y.H., M.S. Investigation: H.O., S.A., M.M., Y.H., T.O., Y.S., O.Y., E.T., T.K, T. Iwashita, T. Ibuka, I.Y. Methodology: I.Y., M.I., K.S., M.S.. Writing original draft: H.O., S.A., M.S.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ogiso, H., Adachi, S., Mabuchi, M. et al. Risk factors for the development of esophageal candidiasis among patients in community hospital. Sci Rep 11, 20663 (2021). https://doi.org/10.1038/s41598-021-00132-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-00132-w
This article is cited by
-
Diabetes in a hospital cohort of persons living with HIV: a descriptive and comparative study in French Guiana
BMC Infectious Diseases (2023)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
