
Abstract
Psychosis is associated with a high risk of relapse, with 67% of clients relapsing within one year following a first episode. In light of the high personal, social, and healthcare costs of the illness, it is paramount to understand the risk factors associated with psychosis relapse. The current systematic review aims to critically review the role of psychosocial stress in psychosis relapse in individuals with an established psychotic disorder. This review systematically searched Ovid (PsycINFO, EMBASE, MEDLINE) literature databases from inception until 28th February 2022. Sixteen studies were eligible for inclusion. Most studies found that individuals with psychosis demonstrate high levels of psychosocial stress and are more likely to be socially withdrawn compared to healthy controls or other clinical presentations. Most studies reported a statistically significant association between psychosocial stress and psychosis relapse, as well as between social withdrawal and psychosis relapse. However, no studies examined the association between high levels of interpersonal sensitivity and psychosis relapse. Individuals with psychosis tend to experience high levels of psychosocial stress and social withdrawal, and these appear to increase the risk of psychosis relapse. Due to high levels of heterogeneity within the literature, we could only conduct a narrative synthesis of the findings. Future studies would benefit from employing a meta-analytic approach.
Similar content being viewed by others


Introduction
Psychosis is a reality distortion experience characterized by delusions, hallucinations, and disorganized thinking1. It is associated with a high risk of relapse, with ~67% of clients relapsing within one year following a first episode2. In addition to causing distress to patients and their families, psychosis relapse has been posited to exert adverse effects on underlying neurobiological processes, which in turn can negatively affect the long-term course of the illness3. Relapse has also been associated with increased risk of harm to self and others, which causes disruption to ones occupational, educational, and relationship roles4. Relapse can also increase perceptions of stigma, leading to increased isolation3. In addition to the distress and disability caused by psychosis, there is an economic burden associated with the illness as treating individuals with psychosis after a symptom relapse costs four times more than treating individuals with a stable course of the disorder1. These neurobiological, psychosocial, and healthcare consequences highlight the importance of understanding the risk factors associated with psychosis relapse.
Gene-environment interactions have been found to play a significant role in psychosis relapse5,6. Indeed, there is considerable evidence that a combination of genetic and environmental/psychosocial factors lead to the dysregulation of the mesolimbic dopamine pathway and of the hypothalamic-pituitary-adrenal axis. This subsequently results in an elevated sensitivity to psychosocial stressors and an increased risk of psychosis relapse5,6,7,8,9. While several studies have examined the impact of genetic risk factors8,10, research examining the impact of psychosocial risk factors on psychosis relapse is limited5.
Psychosocial stress is a potential social risk factor for psychosis relapse that is gaining interest. It has been defined as an emotional, physical, and psychological reaction to social stressors11. Social stressors can be grouped into three categories: chronic stressors (e.g., long-term unemployment), life events (e.g., homelessness), and minor daily hassles (e.g., offensive comments)12. Social stressors have been frequently reported prior to an episode of psychosis13,14, and a high number of stressful events tend to precede the onset of frank psychosis15,16. These findings are consistent with the stress-vulnerability model, which states that cumulative exposure to psychosocial stressors interacts with ones bio-psychosocial vulnerability to gives rise to mental health difficulties17. Furthermore, individuals with psychosis have been found to report a high level of psychosocial stress compared to healthy individuals18,19,20. These findings indicate that social stressors are common in individuals with psychosis.
The role of psychosocial stress in psychosis relapse has been suggested by previous studies21,22. Indeed, an association between high levels of psychosocial stress and psychosis relapse has been consistently reported23,24,25. This finding is also in line with recent retrospective cross-sectional studies reporting that relapse appears to be related to psychosocial stressors, such as moving home and ethnic minority status21,22. Nevertheless, this association’s direction is unclear, as many studies have found that individuals with psychosis tend to show heightened sensitivity to stress6,26. In other words, patients with psychosis may present with heightened stress sensitivity and/or might be exposed to a higher number of stressful events compared to the healthy population. These are distinct yet related aspects which can be individual targets of psychological interventions27,28. In addition, a few earlier studies have reported negative findings, suggesting that there is no association between psychosocial stress and psychosis relapse29,30.
Some of the above inconsistencies might be explained by individual characteristics such as interpersonal sensitivity—a personality trait, referring to the excessive awareness of the emotions and behaviour of others31, which has been implicated in the onset and maintenance of psychosis32,33. It has also been found that interpersonal sensitivity is prominent in the prodromal stages of the illness, among individuals at clinical high risk of psychosis (CHR)34,35 and that this trait was more prominent in CHR individuals compared to healthy controls31,36. Taken together, these studies suggest that individuals at risk of, and with established psychosis report a high level of interpersonal sensitivity, and that this may be associated with onset of psychosis and psychosis relapse. However, the association between interpersonal sensitivity and psychosis relapse has not been fully explored yet.
Alongside personality traits, social behaviours such as social withdrawal, have been studied in association with psychosis relapse. Social withdrawal refers to one’s withdrawal from interpersonal/social relationships accompanied by detachment and an apathetic attitude37. Social withdrawal is one of the negative symptoms of psychosis that, at least in part, explains the small social network observed in individuals suffering from psychosis38. Social withdrawal also appears to be positively linked with psychosis relapse39,40. This finding is in line with the bio ecosystem theory of negative symptoms that explains the impact of several environmental factors (i.e., socio-cultural factors) on negative symptoms (i.e., social withdrawal) and psychosis relapse41. It is still unclear whether social withdrawal progressively precedes psychosis relapse (and can therefore be potentially used as a predictor of relapse), is a negative symptom frequently observed in individuals who are experiencing an episode of psychosis, or a consequence of the illness due to self-stigma or avoidant coping. Social withdrawal, in all its manifestations, could therefore be an intervention target after an FEP to break vicious cycles of avoidance and potentially prevent reoccurrence of symptoms.
Several systematic reviews have examined the association between psychosocial stress and psychosis relapse in individuals with psychosis, however these reviews have several limitations. For example, as some were conducted before the millennium23,25 they did not include more reliable and accurate measurement tools (e.g., ecological momentary assessment) that could improve the ecological validity of findings. Other reviews have been found to be inconclusive42, or only included observational studies43. This did not allow to clarify the relationship between psychosocial stress and psychosis relapse. Previous reviews have also used different definitions of relapse. For example, Petros and colleagues have defined relapse as hospitalization44 and have excluded alternative definitions (e.g., exacerbation/return of symptoms without hospitalization). Other reviews have examined psychosocial stress focusing on a specific stressor, (e.g., childhood trauma)44, which limits the generalizability of the findings as the term psychosocial stress might refer to a wide range of different stressors (e.g., significant life events and minor daily hassles). It is also important to note that childhood trauma cannot be equated or treated similarly to arguments, moving home, or the experience of uncontrollable daily hassles.
Finally, only one review has examined psychosocial stress focusing on different stressors45. However, it included studies that induced psychosocial stress experimentally, which limits the findings’ generalizability as it excluded naturally occurring stressors within one’s daily environment.
The current systematic review aims to overcome some of the above limitations by critically considering different social risk factors, specifically, psychosocial stress, interpersonal sensitivity, and social withdrawal, and their associations with psychosis relapse in individuals with established psychotic disorder (Fig. 1). A better understanding of psychosis’ psychosocial risk factors might allow mental health professionals to intervene early and to apply available preventative strategies before the re-emergence of symptoms.

We propose the following Psychosis Relapse Model. This model suggests that a combination of psychosocial stress, social withdrawal, and interpersonal sensitivity increase risk for psychosis relapse and could be targets of preventive strategies.
Results
Search results
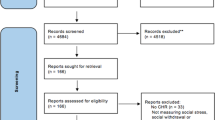
The PRISMA flow diagram of the search results is presented in Fig. 2, where 460 eligible studies were identified for the initial screening. Of these, 119 were duplicates and thus removed, leaving 341 studies for the initial screening. Out of these, 268 were excluded due to being irrelevant to the research questions, leaving 73 studies for full-text retrieval. During the full-text retrieval, 15 studies were excluded due to being qualitative, reviews, validity studies, or being inaccessible in English. The remaining 58 studies were thoroughly reviewed, and of those, 40 were excluded due to not meeting the inclusion criteria. Further, two additional studies were excluded due to insufficient data. A final number of 16 studies matched the inclusion criteria for this review.

PRISMA Flow Diagram.
Study characteristics
The characteristics of the 16 included studies are presented in Table 1. These studies were published between 1971 and 2021 and conducted in eight countries. These studies adopted different research designs: 11 were cohort studies, 5 were cross-sectional studies.
Sample characteristics
The sample characteristics of the 16 included studies are presented in Table 1. These studies included 2248 participants with psychosis. Of these 2248 individuals, 1463 had schizophrenia, 76 had schizoaffective disorder, 24 has psychosis not otherwise specified, 31 had schizophrenia or schizoaffective disorder and 51 were at risk of postpartum psychosis. The participants’ age ranged from 18 to 65 years old, and the majority were male. Furthermore, the measurement of socioeconomic status was only reported in 7 studies.
Risk of bias assessment scores
The risk of bias assessment scores for all the included studies is shown in Tables 2 and 3. The risk of bias for the 11 cohort studies was also conducted using the NOS. The overall risk of bias score suggests a moderate risk of bias, indicating that these are moderate-quality studies. For the 5 cross-sectional studies, the risk of bias was conducted using the modified NOS. The overall risk of bias score suggests a low risk of bias, indicating these are high-quality studies.
Psychosis relapse
The studies identified by this review employed different definitions of psychosis relapse. Nine studies defined relapse as re-hospitalization21,23,29,30,46,47,48,49,50, whereas 3 studies defined relapse as re-hospitalization and symptom exacerbation5,51,52. Furthermore, 2 studies defined psychosis relapse as symptom exacerbation24,25, and 2 studies defined psychosis relapse using a specific scale (i.e, the 8-point criterion)22,53.
Social stressors
Sixteen studies examined the impact of social stress on psychosis relapse and were eligible for inclusion. Seven studies investigated conflict within social groups (Including racism, criticism, or illness/death)21,22,24,46,47,50,52. Three studies investigated general psychosocial stress including lack of social support and social adjustment29,30,49. One study examined minor stressful events25, while 2 studies investigated a wide range of social stressors (e.g., finances, social environment, and employment/education issues)25,48, two studies investigated housing-related stressors (e.g., change of address)22,23, and 1 study investigated childhood adverse events and stress sensitivity5.
Social stress and relapse
Out of the 16 studies, 10 investigated whether individuals with psychosis report a high level of psychosocial stress. Whereas one study reported that individuals with psychosis (i.e., FEP, bipolar disorder, schizophrenia, and schizoaffective) have higher levels of perceived and psychosocial stress than healthy controls or other psychiatric conditions5.
Out of the 16 studies, 13 investigated the association between psychosocial stress and psychosis relapse in individuals with psychosis. Of these 13 studies, three reported no significant association between psychosocial stress (i.e., life stress and childhood adverse events) and psychosis relapse in individuals with schizophrenia29,30,50. In contrast, 10 studies supported the association between psychosocial stress (e.g., childhood maltreatment, address changes, illness/death in family, employment/education changes or redundancies, property damage, racism, interpersonal conflicts, and divorce) and psychosis relapse in individuals with different psychotic disorders (e.g. schizophrenia)5,21,22,23,24,25,46,48,49,52.
Social withdrawal and psychosis relapse
Out of the 16 studies, 6 investigated whether there is an association between social withdrawal and psychosis relapse in individuals with psychosis. These six studies reported that social withdrawal and similar behaviours were evident in individuals with psychosis (e.g., schizophrenia) before their psychosis relapse30,47,48,51,52,53. For example, individuals with chronic schizophrenia were more likely to relapse due to community social adjustment issues30 In contrast, individuals with acute schizophrenia were more likely to relapse due to close relationship conflicts30. Another study reported reduced social support during hospitalization but not before re-hospitalization (ref. 54. Furthermore, Hultman and Wieselgren52 reported that socially isolated individuals who were satisfied with their social life were more likely to relapse than socially isolated individuals keen to increase their social contact.
Interpersonal sensitivity and psychosis relapse
None of the eligible studies assessed interpersonal sensitivity nor its association with psychosis relapse.
Discussion
The current systematic review examined the association between psychosocial stress and risk of psychosis relapse in individuals with a psychotic disorder. Most studies reported an association between psychosocial stress and psychosis relapse, as well as social withdrawal and psychosis relapse. However, there was no evidence to establish whether individuals with psychosis have a higher level of interpersonal sensitivity and whether this is associated with psychosis relapse. In addition, the reviewed literature showed that individuals with psychosis experience a higher level of psychosocial stress and social withdrawal compared to healthy controls.
Psychosocial stress and relapse
Thirteen studies provided information regarding the association between psychosocial stress and psychosis relapse in individuals with psychosis. Of these 13 studies, 10 support an association between psychosocial stress (including different types of minor and major social stressors) and psychosis relapse5,21,22,23,24,25,46,48,49,52. Two social stressors (i.e., interpersonal conflict and moving home) were found to increase psychosis relapse22,23,24,25. However, these studies did not document living conditions (e.g., homelessness) preceding psychosis relapse nor the reasons behind address changes, which would have allowed a better understanding of the impact of this form of psychosocial stresses on relapse. Camacho and colleagues reported a contrasting finding indicating that interpersonal conflict has a low impact on hospitalization21. A possible explanation for this finding could be the lack of a validated measurement tool to assess social stressors, as individual chart reviews were employed to assess stressors.
Although most studies support the association between psychosocial stress and psychosis relapse, three studies reported contradictory findings29,30,50. This could be explained in part by at least two factors: the relatively small sample size (N = 51), and the retrospective nature of these studies, which increases the chance of recall bias55. In addition, some of these studies used subjective measurement tools (e.g., clinical notes) to assess psychosis relapse. For example, Vallejos et al.50 used a self-report questionnaire to assess psychosis relapse. This type of instrument increases the chances of recall bias, as well as under or over-reporting. Finally, Lahniers & White29 recruited individuals with acute schizophrenia and did not include individuals in remission or chronic stages of psychosis, which further limits the generalizability of the findings.
Social withdrawal and relapse
All the included six studies suggest that social withdrawal is associated with psychosis relapse30,47,48,51,52,53. Hultman et al.52 reported that socially isolated individuals who were satisfied with their social life were more likely to relapse than socially isolated individuals keen to increase their social contact. A possible explanation is that isolated individuals dissatisfied with their social life may be more vulnerable to relapse because they have lower stress thresholds couples with increased stress-sensitivity, which is consistent with the vulnerability-stress model17.
Interpersonal sensitivity and relapse
The current review search was conducted systematically in three of the most comprehensive databases. Nevertheless, we did not find studies investigating interpersonal sensitivity or its association with psychosis relapse that met our inclusion criteria. Numerous studies examined interpersonal sensitivity among CHR individuals; however, there is a dearth of studies examining interpersonal sensitivity among individuals with a psychotic disorder34,35.
Strengths and limitations
The current review has some limitations. Firstly, due to the findings’ heterogeneity, it was not possible to conduct a meta-analysis alongside the present review. Once more evidence become available, future studies would benefit from employing a meta-analytic approach to quantify the magnitude of associations between variables. Secondly, as variable definitions of relapse were presented across studies, it was difficult to compare findings. Nevertheless, this review helps to address previous reviews’ limitations, as they only used one definition to define relapse, limiting the generalizability of their findings. Thirdly, many included studies were cross-sectional. While this allows the association between these review variables to be examined, longitudinal studies examining the prospective impact of social stress on psychotic relapse would be better suited to clarify this association.
Despite these limitations, this review has a number of strengths. Firstly, this review attempted to address limitations of previous reviews by including studies with a wide range of different stressors and relapse definitions. Secondly, this review included 16 modest-quality studies that have been published recently (from inception until 28th February 2022) in 8 countries, with relatively large sample sizes (N = 21–641). The relatively large samples and the geographical distribution contribute to increase the generalizability of findings.
Clinical implications and future directions
The current review’s findings provide a rationale for mental health professionals to apply preventative interventions to enhance psychosocial stress management skills in individuals with psychosis, and potentially reducing the likelihood of psychosis relapse. Surprisingly, however, none of the established psychological interventions for psychosis, including those which are recommended by NICE, specifically target psychosocial stress. Interestingly, this review included a study that employed a smartphone app to monitor social stress in real time53. The use of smartphone apps to track psychosocial stressors in real time might be a possible way of assisting clinicians in the prediction of psychosis relapse56. Furthermore, this review highlighted the substantial impact of address change on psychosis relapse, which should be further investigated, collecting detailed information about living conditions before, during, and after the onset of symptoms.
Conclusions
This systematic review supports the idea of an association between psychosocial stress and risk of psychosis relapse in individuals with a psychotic disorder. Individuals with psychosis tend to experience a high level of psychosocial stress and social withdrawal, and they both appear to increase the risk of psychosis relapse. The role of interpersonal sensitivity in psychosis relapse remains to be explored. Due to the high heterogeneity within the existing literature, only a narrative synthesis of the findings was conducted. Future studies would benefit from employing a meta-analytic approach.
Methods
Protocol and registration
This review followed the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines57. The review protocol was registered in the prospective international register of systematic reviews (PROSPERO: CRD42021264478), and it documented and specified the methods and exclusion/inclusion criteria in advance.
Search strategy and selection criteria
We systematically searched Ovid (PsycINFO, EMBASE, MEDLINE) literature databases from inception until 28th February 2022. We employed the following search strings: (psychosis OR psychotic OR schizophreni*) AND (interpersonal sensitiv* OR interpersonal awareness OR relational sensitiv* OR social withdrawal OR social avoidance OR social network OR social stress* OR social advers* OR psychosocial stress*) AND (relapse OR hospitalisation OR readmission OR hospital admission). Hand-searching was also conducted while reviewing the articles’ full text to find new references.
We applied no restrictions regarding ethnicity, gender, socioeconomic status, publication’ date, language, and psychiatric treatment settings (inpatients or outpatients). We applied the following inclusion criteria: (1) randomized controlled trials (RCTs), cohort, case-control, and cross-sectional studies; (2) that assess (Psycho)social stress and psychosis relapse, with psychosis relapse defined as return/exacerbation of psychosis symptoms or re-hospitalization (3); with participants who suffer from a psychosis disorder as indicated by the DSM or ICD, who are between 14 and 65 years old. We excluded (1) qualitative studies, systematic reviews, meta-analyses, and case reports; (2) studies that included participants diagnosed with psychosis due to organic causes or who had a comorbid learning disability; and (3) papers that were unrelated to our variables of interest, namely interpersonal sensitivity, social withdrawal, and psychosocial stress with relapse of psychosis.
Data extraction process
The study screening was completed independently by one reviewer (KM) and was subsequently cross-checked by a second reviewer (PR). Disagreements were settled by consensus. Furthermore, one reviewer (KM) independently extracted the following data from the included studies: country of origin, author, publication date, study design, sample size, data analysis, key results, participant information, and antipsychotic adherence status. In addition, information about the independent variables (i.e., psychosocial stress, social withdrawal, interpersonal sensitivity) and the dependent variables (i.e., relapse) and how they were measured was extracted.
Risk of bias assessment
The risk of bias and certainty assessment was conducted by co-authors (KM). The risk of bias for cohort studies was conducted using the modified version of the Newcastle-Ottawa Quality Assessment Scale (NOS) to ascertain the reliability and validity of these studies’ results58. The risk of bias for the cross-sectional studies was also conducted using an adapted version of the NOS59. In contrast, the risk of bias for RCTs was conducted using a critical appraisal tool60.
Data availability
Data sharing is not applicable to this article as no new data were collected or analysed as part of this study.
References
Nova, S. P. I. The abandoned illness. A report by the Schizophrenia Commission. Executive summary. (2012).
Di Capite, S., Upthegrove, R. & Mallikarjun, P. The relapse rate and predictors of relapse in patients with first-episode psychosis following discontinuation of antipsychotic medication. Early Interv. Psychiatry 12, 893–899 (2018).
Emsley, R., Chiliza, B., Asmal, L. & Harvey, B. H. The nature of relapse in schizophrenia. BMC Psychiatry 13, 50 (2013).
Emsley, R. Antipsychotic maintenance treatment in schizophrenia and the importance of preventing relapse. World Psychiatry 17, 168–169 (2018).
Hazelgrove, K. et al. Risk factors for postpartum relapse in women at risk of postpartum psychosis: the role of psychosocial stress and the biological stress system. Psychoneuroendocrinology 128, 105218 (2021).
Mizrahi, R. Social stress and psychosis risk: common neurochemical substrates? Neuropsychopharmacology 41, 666–674 (2016).
Heinz, A., Deserno, L. & Reininghaus, U. Urbanicity, social adversity and psychosis. World Psychiatry 12, 187–197 (2013).
Howes, O. D. & Murray, R. M. Schizophrenia: an integrated sociodevelopmental-cognitive model. Lancet 383, 1677–1687 (2014).
Van Os, J., Kenis, G. & Rutten, B. P. F. The environment and schizophrenia. Nature 468, 203–212 (2010).
Gassó, P. et al. A longitudinal study of gene expression in first-episode schizophrenia; exploring relapse mechanisms by co-expression analysis in peripheral blood. Transl Psychiatry 11, 539 (2021).
Wheaton, B., Young, M., Montazer, S. & Stuart-Lahman, K. Social Stress in the Twenty-First Century. in Handbooks of Sociology and Social Research 299–323 (Springer Science and Business Media B.V., 2013).
Levine, S. & Scotch, N. A. Social Stress (Routledge, 2017).
Bendall, S., Jackson, H. J., Hulbert, C. A. & McGorry, P. D. Childhood trauma and psychotic disorders: a systematic, critical review of the evidence. Schizophr. Bull. 34, 568–579 (2008).
Cutajar, M. C. et al. Schizophrenia and other psychotic disorders in a cohort of sexually abused children. Arch. Gen. Psychiatry 67, 1114–1119 (2010).
Brown, G. W. & Birley, J. L. T. Crises and life changes and the onset of schizophrenia. J Health Soc. Behav. 9, 203–214 (1968).
Day, R. et al. Stressful life events preceding the acute onset of schizophrenia: a cross-national study from the World Health Organization. Cult. Med. Psychiatry 11, 123–205 (1987).
Zubin, J. & Spring, B. Vulnerability: a new view of schizophrenia. J. Abnorm. Psychol. 86, 103–126 (1977).
Lataster, T., Valmaggia, L., Lardinois, M., Van Os, J. & Myin-Germeys, I. Increased stress reactivity: a mechanism specifically associated with the positive symptoms of psychotic disorder. Psychol. Med. 43, 1389–1400 (2013).
Myin‐Germeys, I. et al. Emotional reactivity to daily life stress in psychosis and affective disorder: an experience sampling study. Acta Psychiatr. Scand. 107, 124–131 (2003).
Veling, W., Pot-Kolder, R., Counotte, J., Van Os, J. & Van Der Gaag, M. Environmental social stress, paranoia and psychosis liability: a virtual reality study. Schizophr. Bull. 42, 1363–1371 (2016).
Camacho, A., Ng, B., Bejarano, A., Simmons, A. & Chavira, D. Crisis visits and psychiatric hospitalizations among patients attending a community clinic in rural Southern California. Community Mental Health J. 48, 133–137 (2012).
Ünal, B., Akgül, Ö., Binbay, T., Alptekin, K. & Kivircik Akdede, B. B. Association of wider social environment with relapse in schizophrenia: registry based six-year follow-up study. Noropsikiyatri Arsivi 56, 235–242 (2019).
Caton, C. L. M. & Goldstein, J. Housing change of chronic Schizophrenic patients: a consequence of the revolving door. Sm. Sci. Med 19, 759–764 (1984).
Docherty, N. M. et al. Anxiety interacts with expressed emotion criticism in the prediction of psychotic symptom exacerbation. Schizophr. Bull. 37, 611–618 (2011).
Malla, A. K., Cortese, L., Shaw, T. S. & Ginsberg, B. Psychiatric epidemiology life events and relapse in schizophrenia A one year prospective study. Soc. Psychiatry Psychiatr. Epidemiol. 25, 221–224 (1990).
DeVylder, J. E. et al. Stress sensitivity and psychotic experiences in 39 low- and middle-income countries. Schizophr. Bull. 42, 1353–1362 (2016).
Fowler, D., Hodgekins, J. & French, P. Social recovery therapy in improving activity and social outcomes in early psychosis: current evidence and longer term outcomes. Schizophr. Res. 203, 99–104 (2019).
Lutgens, D., Gariepy, G. & Malla, A. Psychological and psychosocial interventions for negative symptoms in psychosis: systematic review and meta-analysis. Br. J. Psychiatry 210, 324–332 (2017).
Lahniers, C. & Edward White, K. Changes in environmental life events and their relationship to psychiatric hospital admissions. J. Nerv. Ment. Dis. 163, 154–158 (1976).
Serban, G. Relationship of mental status, functioning and stress to readmission of schizophrenics. Br. J. Soc. Clin. Psychol. 14, 291–299 (1975).
Mushtaq, A., Fatima, B., Fatema, A. A., Syed, H. & Sohail, H. Interpersonal sensitivity in the at-risk mental state for psychosis in Karachi, Pakistan. Eur. Psychiatry 41, S563–S563 (2017).
Bogren, M. et al. Predictors of psychosis: a 50-year follow-up of the Lundby population. Eur. Arch. Psychiatry Clin. Neurosci. 260, 113–125 (2010).
Meisel, S. F., Garety, P. A., Stahl, D. & Valmaggia, L. R. Interpersonal processes in paranoia: a systematic review. Psychol. Med. 48, 2299–2312 (2018).
Masillo, A. et al. Interpersonal sensitivity and persistent attenuated psychotic symptoms in adolescence. Eur. Child Adolesc. Psychiatry 27, 309–318 (2018).
McDonnell, J., Stahl, D., Day, F., McGuire, P. & Valmaggia, L. R. Interpersonal sensitivity in those at clinical high risk for psychosis mediates the association between childhood bullying victimisation and paranoid ideation: a virtual reality study. Schizophr. Res. 192, 89–95 (2018).
Masillo, A. et al. Interpersonal sensitivity in the at-risk mental state for psychosis. Psychol. Med. 42, 1835–1845 (2012).
Morese, R., Palermo, S., Torello, C. & Torello, C. Social Withdrawal and Mental Health: An Interdisciplinary Approach (IntechOpen, 2020).
Bjornestad, J. et al. “With a little help from my friends” social predictors of clinical recovery in first-episode psychosis. Schizophr. Bull. 43, S57–S57 (2017).
Fikreyesus, M., Soboka, M. & Feyissa, G. T. Psychotic relapse and associated factors among patients attending health services in Southwest Ethiopia: a cross-sectional study. BMC Psychiatry 16, 354 (2016).
Simone, C., Carolin, L., Max, S. & Reinhold, K. Associations between community characteristics and psychiatric admissions in an urban area. Soc. Psychiatry Psychiatr. Epidemiol. 48, 1797–1808 (2013).
Strauss, G. P. A bioecosystem theory of negative symptoms in schizophrenia. Front. Psychiatry 12, 655471 (2021).
Fallon, P. Life events; their role in onset and relapse in psychosis, research utilizing semi-structured interview methods: a literature review. J. Psychiatr. Ment. Health Nurs. 15, 386–392 (2008).
Martland, N., Martland, R., Cullen, A. E. & Bhattacharyya, S. Are adult stressful life events associated with psychotic relapse? A systematic review of 23 studies. Psychol. Med. 50, 2302–2316 (2020).
Petros, N. et al. Impact of childhood trauma on risk of relapse requiring psychiatric hospital admission for psychosis. Br. J. Psychiatry 209, 169–170 (2016).
Lange, C. et al. Experimentally induced psychosocial stress in schizophrenia spectrum disorders: a systematic review. Schizophr. Res. 182, 4–12 (2017).
Chakraborty, A., King, M., Leavey, G. & McKenzie, K. Perceived racism, medication adherence, and hospital admission in African-Caribbean patients with psychosis in the United Kingdom. Soc. Psychiatry Psychiatr. Epidemiol. 46, 915–923 (2011).
Chu, C.-C., Klein, H. E., Omaha, D. & Louis, S. Psychosocial and environmental variables in outcome of black schizophrenics. J. Natl Med. Assoc. 77, 793–6 (1985).
Krupinski, J., Stoller, D. A. & Eva, D. P. M. Sociopsychiatric study of schizophrenia: the follow-up. Aust. N.Z. J. Psychiatry 5, 146–155 (1971). vol.
Megna, J. L., Gupta, S., Ursino, A. & Dewan, M. Variable effects of psychosocial factors on the clinical course of schizophrenia. Ann. Clin. Psychiatry 17, 19–21 (2005).
Vallejos, M., Cesoni, O. M., Farinola, R., Bertone, M. S. & Prokopez, C. R. Adverse childhood experiences among men with schizophrenia. Psychiatr. Q. 88, 665–673 (2017).
Cechnicki, A. & Wojciechowska, A. Correlations between features of social network and outcomes in those suffering from schizophrenia seven years from the first hospitalisation. Psychiatr. Pol. 41, 513–525 (2007).
Hultman, C. M. & Wieselgren, I. Relationships between social support, social coping and life events in the relapse of schizophrenic patients. Scand. J. Psychol. 38, 3–13 (1997).
Buck, B. et al. Relationships between smartphone social behavior and relapse in schizophrenia: a preliminary report. Schizophr. Res. 208, 167–172 (2019).
Müller, B., Nordt, C., Lauber, C. & Rössler, W. Changes in social network diversity and perceived social support after psychiatric hospitalization: Results from a longitudinal study. Int. J. Soc. Psychiatry 53, 564–575 (2007).
Shiffman, S., Stone, A. A. & Hufford, M. R. Ecological momentary assessment. Annu. Rev. Clin. Psychol. 4, 1–32 (2008).
Eisner, E. et al. Feasibility of using a smartphone app to assess early signs, basic symptoms and psychotic symptoms over six months: a preliminary report. Schizophr. Res. 208, 105–113 (2019).
Page, M. et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372, n71 (2021).
Wells, G. A. et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses (Ottawa Hospital Research Institute, 2008).
Modesti, P. A. et al. Panethnic differences in blood pressure in europe: a systematic review and meta-analysis. PLoS ONE 11, e0147601 (2016).
Joanna Briggs Institute. Checklist for systematic reviews and research syntheses. (2017).
Acknowledgements
This study is funded by a project grant from the Medical Research Council (MR/S026428/1).
Author information
Authors and Affiliations
Contributions
All authors have made substantial contributions to the conception or design of the work or the acquisition, analysis or interpretation of the data; have substantially contributed to the drafting the work or to the critical revision of important intellectual content; have given final approval of the completed version, and are taking accountability for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Almuqrin, A., Georgiades, A., Mouhitzadeh, K. et al. The association between psychosocial stress, interpersonal sensitivity, social withdrawal and psychosis relapse: a systematic review. Schizophr 9, 22 (2023). https://doi.org/10.1038/s41537-023-00349-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41537-023-00349-w
This article is cited by
-
Depicted simulation model for removal of second-generation antipsychotic drugs adsorbed on Zn-MOF: adsorption locator assessment
Journal of Molecular Modeling (2024)
