
Abstract
Neuropsychiatric mood and motivation symptoms (depression, anxiety, apathy, impulse control disorders) in Parkinson’s disease (PD) are highly disabling, difficult to treat and exacerbated by current medications and deep brain stimulation therapies. High-resolution intracranial recording techniques have the potential to undercover the network dysfunction and cognitive processes that drive these symptoms, towards a principled re-tuning of circuits. We highlight intracranial recording as a valuable tool for mapping and desegregating neural networks and their contribution to mood, motivation and behavioral symptoms, via the ability to dissect multiplexed overlapping spatial and temporal neural components. This technique can be powerfully combined with behavioral paradigms and emerging computational techniques to model underlying latent behavioral states. We review the literature of intracranial recording studies investigating mood, motivation and behavioral symptomatology with reference to 1) emotional processing, 2) executive control 3) subjective valuation (reward & cost evaluation) 4) motor control and 5) learning and updating. This reveals associations between different frequency specific network activities and underlying cognitive processes of reward decision making and action control. If validated, these signals represent potential computational biomarkers of motivational and behavioural states and could lead to principled therapy development for mood, motivation and behavioral symptoms in PD.
Similar content being viewed by others


Introduction
Parkinson’s disease (PD) is a highly disabling neurodegenerative movement disorder, affecting 1% of the population over the age of 601. To date, motor symptoms of PD have been the main focus of research and therapy development. However, people with PD, which has been described as the quintessential neuropsychiatric disorder, also experience a range of disabling non-motor symptoms including mood, motivation and behaviour such as depression, anxiety, apathy and impulsive compulsive behaviours (ICB)2. The prevalence of mood and motivation disorders in PD is high, reaching 50% for depression and anxiety, 40% for apathy3 and 14–30% for ICB2. Yet, despite their prevalence, the complexity of these symptoms and their interaction with current treatments for motor symptoms, the circuit mechanisms underlying them remain unclear. As a result, there have to date been few successful treatment options for motivation and behavioral symptoms in PD4,5.
Mood and motivation disorders in PD have sometimes been broadly classified into two different extremes of a single spectrum with “hypodopaminergic” symptoms (depression, anxiety, and apathy) at one end and “hyperdopaminergic” symptoms (pathological impulsivity and ICB) at the other6,7,8. This simple distinction does support a significant role for dopamine in the pathophysiology of these symptoms and is based on a number of clinical and experimental observations9,10,11,12. However, a single dimension of behaviour is insufficient to account for the complex and multi-faceted neuropsychiatric symptoms (NPS) that occur in PD. Moreover, it is unlikely that complex mood states or behaviours map accurately onto such a simplistic schema such as a “hypo” or ‘hyper’ dopaminergic state. Rather, mood states arise from the complex interactions between systems in the brain, and likely arise from different computations that might also be reflected in distinct oscillatory processes that are present during specific behaviors. Therefore, different mood and motivational states might map onto different oscillations within the cortico-basal ganglia networks and these may go awry in PD, contributing to non-motor symptoms.
Invasive neurophysiology, and specifically intracranial recordings, provide tools for recording neural network signals that can be combined with behavioural paradigms that index distinct aspects of behaviour. Such recordings offer the potential to tap into neural synchronisation at different frequencies, and thus potentially functionally segregate processing streams that are spatially overlapping in the cortex and basal ganglia13.
Intracranial recordings can be performed using intraoperative microelectrode recordings of single or multiple neurons, or local field potential (LFP) recordings of aggregated neural population signals. Electrophysiological LFP activities are classically analysed with respect to partially physiological distinct power (spectral) bands including: delta (1–3 Hz), theta (4–7 Hz), alpha (8–12 Hz), beta (13–30 Hz) and gamma (35–100 Hz). Together these techniques can help identify the site, spectral signatures and precise temporal windows that are involved in specific cognitive sub-processes.
LFPs, when combined with cortical (magnetoencephalography, electroencephalographic and electrocorticography) recordings, can also disclose inter-regional (cortico-subcortical) networks expressed as rich, multiplexed, spatio-spectral components14. The precision of such recordings have the potential to dissociate the mechanisms underlying different symptoms, particularly when combined with experimental paradigms that can tap into the computational processes that underlie behaviour. In the future, these neurophysiology signals may serve as valuable biomarkers for principled re-tuning of unbalanced systems by targeting the particular frequency domains underlying a specific symptom. Such adaptive neurostimulation approaches are already proving highly fruitful for treating motor system impairments and here we propose a similar approach to non-motor impairments15,16. We focus on particular dimensions of mood, motivation and behaviour that are specifically impacted in PD and have been studied with intracranial neurophysiology. Disturbances in cognition, arousal, circadian and sleep rhythms also make a significant contribution to NPS in PD but have been covered elsewhere and so are not reviewed here17,18,19.
Our framework considers symptoms and behaviour using experimental, behavioural paradigms that assay 1) emotional processing, 2) executive control 3) subjective valuation (reward and cost evaluation) 4) motor control and 5) learning and updating (Fig. 1). Here, we specifically review the mapping of these constructs onto underlying neurophysiology captured through intracranial recordings. For each cognitive process we describe neurophysiological studies that distinguish between patient groups and then focus on studies examining neurophysiological recordings using behavioral paradigms and within-subject approaches. We have included available studies using recordings from targets used in clinical practice - subthalamic nucleus (STN) is represented in a predominance of studies but we also include globus pallidus interna (GPi), ventral thalamus and pedunculopontine nucleus (PPN) in patients with PD undergoing Deep Brain Stimulation (DBS). We included both micro and macro-electrode recordings either during surgery, in the few days immediately following or in chronically implanted patients using new sensing-enabled DBS pacemakers20. Taken together this work suggests there is significant promise in the potential for neurophysiological recordings in patients to identify localised oscillatory signals that distinguish between different mood and motivation impairments.

Schematic indicating central computational processes (top row), neurocognitive dysfunction and symptom presentation (middle row) and behavioral paradigms and frequently occurring spatio-spectral LFP correlates (bottom row). These are shown for different computational stages of processing including affect and primary emotional response, executive control of information, subjective valuation, leading to motor initiation and then motor stopping of prepotent response where required. This leads to an outcome and feedback and learning, which will update all stages of the decision cycle. All stages shown serially, although these are likely implemented in parallel.
Affect and emotional processing
Emotional processing and relationship with depression and anxiety – across subject studies
In healthy and clinical populations it has been demonstrated that deficits in emotional processing are involved in the generation of depression and anxiety21,22. It is now well established that parallel segregated networks subserving limbic, associative and motor functions exist between prefrontal cortex and basal ganglia and that these are partially spatially and functionally dissociable at the level of the STN and basal ganglia23,24.
Single unit micro-electrode recordings have demonstrated that STN (particularly ventral STN) is associated with increased theta-alpha activity (Table 1)25. Further, increased resting state alpha power oscillation in the left ventral STN positively correlates with depressive symptoms in PD, whereas theta correlates negatively with both depression and anxiety26. LFP studies have built on this and compared intracranial neurophysiological (STN) recordings with symptoms of depression, measured with the Beck’s Depression Inventory (BDI-II)27,28. Overall, these studies showed reduced STN alpha reactivity (event related desynchronization) to positively valenced stimuli, and increased alpha desynchronization to negative stimuli in depressed patients with PD, effects that continue up to 3 months post-operatively28. STN alpha reactivity to positive emotional stimuli was also found to be enhanced (and response to negative stimuli reduced) by administration of exogenous dopamine, a relationship that was most pronounced in non-depressed patients27. These studies suggest that a component of the alpha rhythm in the STN may track emotional valence and that this indexes a negative emotional bias in patients with PD and depression and is modulated by dopamine.
Emotional processing—within-subject studies
Seven other studies have investigated changes in intracranial recordings from the STN while performing tasks assessing emotional processing29,30,31,32,33,34,35. These studies also support a modulation of alpha in response to emotional visual stimuli, reporting a greater alpha-ERD and larger evoked response potential (ERP) amplitude in response to pleasant and unpleasant stimuli compared to neutral ones in PD patients ON medication29,30,31,32,33. This work has shown that the relationship between alpha and valence holds when controlling for arousal32, with valence and arousal likely encoded by separate neuronal populations in the STN29. Two further studies specifically investigated hemispheric laterality during emotional acoustic stimuli and demonstrated a regional specialization (ventro-medial) and a hemispheric asymmetry (right dominance)34,35, which generalizes to emotional lateralization research outside of PD36.
Recent investigations have also evaluated emotional processing during stimulation of the STN at different frequencies and provide support that these alpha oscillations may be potentially mechanistic and causal (Fig. 2)37. Stimulating the right-STN demonstrated an interaction between emotional picture ratings and stimulation frequency, with 10 Hz (alpha frequency) stimulation increasing subjective valence ratings of negative pictures compared to no stimulation, an effect that was increased in depressed patients37. The study however did not measure underlying physiology during stimulation in order to demonstrate entrainment of underlying oscillations to stimulation and therefore only provides partial supportive evidence of causality.

A Average event locked spectrogram from 28 patients with PD, recorded from the STN at the time of emotional image (IAPS) presentation (left). Statistical parametric mapping on stimulus locked baseline corrected spectrograms demonstrates two significant clusters; a theta power increase and an alpha/beta de-synchronization (left). Alpha is lower (greater desynchronization) following pleasant vs. unpleasant stimuli in the ON medication state (right). This effect reverses OFF medication, showing that in the absence of dopamine alpha is poorly responsive to pleasant stimuli and shows increased reactivity to negative stimuli. (reproduced with permission from Huebl et al. 2014). B Impact of alpha (10 Hz) stimulation of the STN increases IAPS valence ratings, an effect not seen with 130 Hz stimulation (reproduced with the permission from Mandali et al. 2021).
In summary, LFP studies recording from the STN in PD support that a component of alpha band activity in the STN is correlated with processing of emotional stimuli and degree of depressive symptomatology.
Behaviour—impulsivity and apathy
ICBs comprise impulse control disorders such as pathological gambling, compulsive shopping, compulsive sexual behaviour and eating, and related disorders such as punding/hobbyism and dopamine dysregulation syndrome38. ICB are formally defined as a class of psychiatric disorders characterized by a failure to resist a temptation, urge, or impulse that may harm oneself or others39. An interplay between exposure to dopaminergic medications, deep brain stimulation and personality traits, as well as disease-related characteristics in people with PD, appears to underlie the generation of these behavioural disorders40,41. Many studies have solely assessed motor impulsivity (using motor stopping tasks) and have reported contradictory results with some studies even finding lower motor impulsivity in certain ICB cohorts42,43,44. It is also worth noting that the compulsivity component of ICB in PD has less commonly been taken into account45. Although impulsivity and ICB as clinical constructs encompass many different cognitive subprocesses of decision making, they are likely concentrated specifically in aberrant executive control, reward evaluation and motor control46 (Fig. 1, Tables 2 and 3).
Impulsivity and apathy—across subjects studies
Single unit recordings in people with PD have implicated the STN in patients with ICB47, however, the spectral components of micro-electrode single unit activity have been less consistently linked to ICBs in a single frequency band48. The first study evaluating neural mechanisms of ICB in PD using LFP recordings identified low frequency (4–10 Hz) oscillations as being linked to ICBs, particularly in the ON medication state and in ventral STN49. This study also found greater STN-premotor/prefrontal (EEG contacts F3,F4) cortex theta (4–7 hz) band coherence in patients with ICBs compared to those without. However, other frequencies have also been implicated and recently a correlation has been shown between resting state low frequency activity in the alpha range during the OFF medication condition and trait impulsivity as measured with the Barratt Impulsivity scale irrespective of the presence and severity of ICB50.
Two studies have investigated differences in STN LFPs in PD patients specifically with pathological gambling, using behavioural paradigms involving economic decision-making51,52. Spectral analysis revealed a relationship between pre-cue beta and diagnosis of ICB, but this difference did not predict future choices52. However, all PD patients showed an STN low frequency (2–12 Hz) increase during decision making and PD patients with pathological gambling adopted a risky strategy and showed greater, low-frequency power during high conflict trials51. Clinical impulsivity also predicts subcortical evoked response activity and shows dissociable effects on STN and GPi53.
In summary, these studies demonstrate that STN and GPi recordings can elicit ICB biomarkers at the levels of single cells, ERPs and LFP oscillations. There is a suggestion that low frequency local activity, particularly a component in the theta range, may be particularly associated with ICBs in PD.
Impulsivity and apathy—within-subject studies
Executive control and reflection impulsivity
Appropriate executive control prevents reacting to inappropriate cues, responding when too little information is available or waiting too long to respond. Deficits of this type of information processing can result in reflection impulsivity40,54. There are a number of behavioural paradigms which evaluate action inhibition under conflict which can index higher order executive control, including the Stroop task55, the Flanker task56, the Simon task57 and random dot kinematograms (RDK)58,59.
LFP studies in PD using the Stroop task, in which words are presented in congruent and incongruent colours, demonstrate a relative increase in theta activity on incongruent trials60,61. Event-related STN stimulation during the Stroop task has probed the temporal window of conflict processing and demonstrated that stimulation delivered early post stimulus causally impacts behaviour, relatively speeding up responding on conflict trials and increasing errors61. Generalizing to alternative forms of inhibitory control, other studies have recorded STN LFPs during spatial conflict tasks (Simon task and Flanker tasks) to demonstrate increased theta power during spatially incongruent trials, with rewarded inhibition linked to theta phase resetting (indexed by inter-trial theta phase clustering)62,63,64,65. Cross-site phase locking between motor cortex (M1) and STN has also been shown to regulate the influence of the STN on M1 representations of incorrect response-tendencies, in the beta band during the Simon task65. These results demonstrated that theta activity is linked to conflict processing, through both theta amplitude and phase modulations, likely supported by signal processing in other frequency bands, including the motor cortex - subthalamic beta network.
Recent work has combined the Flanker task with drift diffusion modelling (DDM), a computational framework that models decision making as a process of evidence accumulation towards a threshold. This found that some STN theta activity is linked to dynamic decision processes, rather than being simply a biomarker of conflict, with subthalamic stimulation modulating evidence accumulation rates and theta setting thresholds66. A further seminal study extends this work to other forms of conflict by using a paradigm that presents decisions containing either high or low reward conflict while recording from medial prefrontal cortex (mPFC) and STN (Fig. 3)67. This study again confirmed an increase in mPFC and STN theta activity which, after fitting the DDM, was found to be correlated with decision thresholds.

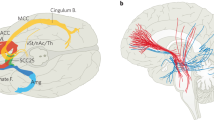
A Theoretical model of medial prefrontal cortex (mPFC)—STN mediation of decision thresholds. mPFC detects conflict which leads to adjustment of decision thresholds in the STN. This process is interrupted by DBS. B Modelling of relationship between mPFC theta and decision threshold (negative regression coefficient—high theta correlates with low decision threshold, positive regression coefficient - high theta correlates with increased decision threshold). This reveals that OFF DBS (blue line)—increased theta was associated with increased decision threshold for high-conflict trials (solid line), but not low-conflict trials (dashed line). ON DBS, increased theta was associated with a decreased decision threshold on high-conflict trials (reproduced with permission from Cavanagh et al. 2011). C Schematic of combined intracranial mPFC—STN intra-operative electrode recordings. D Normalized oscillatory power averaged across all STN (upper) and mPFC (lower) electrodes and across all correct trials in a movement conflict task. Both brain regions showed a pre-response increase in theta power, although this is earlier and greatest averaged to the cue in the case of mPFC. In the beta band, the STN showed a pre-response decrease in power while the mPFC showed a post-response increase in beta power (reproduced with permission from Zavala et al. 2018).
One challenge for behavioral tasks that present abrupt cues is the profound evoked low frequency neural activity that any salient sudden cue can elicit, potentially confounding salience with conflict. A continuous form of conflict paradigm implements an RDK in which clouds of dots continuously move in different directions on the screen to, on average, indicate the correct direction for an upcoming voluntary movement such as a button press68. In addition to investigating conflict (with dots moving in different directions), the paradigm measures reflection impulsivity since subjects control how much information they sample before making a decision. RDK paradigms plus neurophysiology recordings in PD have confirmed increased low frequency activity during motion conflict, activity that was coherent between medial prefrontal cortical (mPFC) theta and STN theta-delta in conflict trials58. Prefrontal cortical - STN theta dynamically tracks evidence accumulation, accounting for variable incoming evidence presentation rates59. Combining RDK paradigms with DDM has again demonstrated that trial-by-trial decision thresholds are also indexed by mPFC-STN low frequency phase alignment69. Using RDK paradigms it has also been shown that mPFC-STN theta appears to again be supported by a spatially and spectrally segregated beta band neural network between motor cortex and STN which also supports decision threshold setting70. This study showed that these two networks were functionally distinct in mediating speed - accuracy tradeoffs. Specifically, an increase in STN low frequency oscillatory power was found to predict increased thresholds only after instructions emphasizing accuracy, while cue-induced reductions of STN beta reflected a decreased threshold, irrespective of whether the subject was prioritising speed or accuracy.
In addition, recent work investigating mPFC-STN theta and beta within a novel conflict paradigm showed that functional roles of these oscillations are regionally specific (Fig. 3)71. The authors here demonstrated that within trial adaptations to conflict are mediated by increased mPFC-STN theta synchrony, causing response inhibition, whereas across trials, beta signals more strongly mediated behavioural adaptations to conflict or errors. Here, beta was modulated within a trial in the STN, whereas more so in PFC post trial. Support for a causal role for a component of beta oscillations in threshold setting comes from a study which combined RDK, DDM and closed-loop DBS in a single paradigm to demonstrate a temporally precise causal impact of DBS and beta oscillations on response threshold setting72. Notably, the component of STN beta activity coupled with the prefrontal cortex (PFC) may have a complementary, more general role to motor initiation threshold setting, as parallel work has demonstrated that this network indexes working memory encoding, even in the absence of motor initiation73. Theta signals have also been linked to higher order conflict resolution including moral reasoning74. These data are anatomically complimented by studies of single units recording, where a change in neural firing activities was described in the STN and in the GPi in response to conflict in a decision-making task75 or to a deviant tone in an oddball task76.
In summary, these studies demonstrate a link between a component of PFC theta activity and PFC-STN synchrony in conflict detection, in addition to complementary effects of a beta motor cortex - STN network. Further work investigating how these two networks collectively set thresholds for action initiation are warranted.
Subjective valuation: reward cost evaluation and choice impulsivity
One of the most studied cognitive functions of the basal ganglia in animal models is reward processing77. In humans, reward processing and apathy have been mapped to distributed prefrontal cortical and basal ganglia networks with ventromedial prefrontal, anterior cingulate cortex, supplementary motor areas and ventral striatum plus connected areas being important nodes5. Electrophysiological studies in PD have further expanded our knowledge on the role of basal ganglia in reward processing in humans using paradigms for reward, loss and effort evaluation during recordings from STN, GPi and PPN (Table 3).
Reward versus effort trade-off paradigms, where participants make decisions about whether to exert different levels of effort for reward, are valuable to understanding healthy motivation and the clinical symptom of apathy, which likely reflects modulation of sensitivity to effort and reward78,79. The first comprehensive study in PD, using a reward (monetary) and effort (grip force) paradigm80, reported an STN spectral response to both reward and effort cues in the 1–10 Hz range with larger responses produced by larger rewards. Moreover, these responses were reflective of the subjective value of reward and predicted patients’ trial-by-trial decisions of whether to exert effort for reward, an effect that weakened OFF levodopa (Fig. 4)80. Low frequency activity also appears linked to other types of reward discounting, as another study analysing LFPs recorded from the STN showed an increase in theta power preceding risk taking decisions81. Further studies of single unit activity and LFP recorded in the STN of patients with PD have used reward paradigms including the Balloon Analogue Risk Task82 (for risk taking behaviour), a rewarded Go/NoGo task83, a modified version of the Monetary Incentive Delay task84,85(reward evaluation) and a task of decision making using a 2-choice preference-based task86. These studies suggested that STN cells show significant modulation by reward and that STN neurons that responded were valence specific (i.e., they responded exclusively to either reward opportunity or threat of loss), moreover they suggest that the STN is modulated more in response to reward than the GPi.

A STN group level neurophysiology related to reward-effort decision making. Cluster-based permutation analysis showing proportion of subjects in which the LFP power increased significantly for each frequency x time combination, demonstrates low frequency reward locked STN activities (top). Low frequency activity scales with reward value and notably the reward effect on LFP correlates with the reward effect on behaviour (reproduced with permission from Zenon et al. 2016). B Action stopping indexed through a stop-signal task during LFP recordings from the STN. Stopping triggers an increase in STN beta activity which starts prior to the stop signal reaction time (reproduced with permission from Wessel et al. 2016).
In summary, single unit recordings and LFP studies in the STN and GPi in PD support that particularly the STN is involved in the processes of reward, risk, and effort evaluation and that this may involve a component of low frequency (particularly theta) activity.
Motor control and motor impulsivity
Information processing and reward evaluation lead to motor preparation and initiation. The computational process of action control involves the appropriate release of prepared movements paired with stopping or switching when required. Behavioural tasks can be used to assess impulsivity defined as impaired inhibitory control over prepotent motor or cognitive responses. Processes of action selection versus action inhibition have been shown to map to dissociable subcortical locations of dorsal and ventral STN respectively87. The GPi, although less studied, also appears to encode motor versus higher order functions topographically88.
In the motor Go/No-Go task89 and the Stop Signal Task (SST)90, participants are presented with a stimulus that requires them either to respond (Go) or withhold a response (NoGo/Stop). Impulsive participants may make more commission errors (Go responses on No-go or Stop trials) and/or anticipation errors (responding too fast). A number of LFP studies have probed the role of STN in modulating action inhibition using these tasks with the majority taking a within-subject approach. It is now increasingly recognized that motor impulsivity is just a single component of impulsive behavior and may not correlate strongly with clinical impulsivity symptoms44.
Three studies have employed simple or modified versions of the Go-NoGo task83,91,92 while six studies have employed the SST65,93,94,95,96,97 with concurrent STN LFP recordings. In the first classical Go-NoGo study, beta oscillations decreased prior to movement and rebounded following post-movement in the Go trials91. However, in the No-Go trials, the beta decrease terminated earlier and before the reaction time in a majority of patients. This was supported in a modified, probabilistic, bimanual version of the Go-NoGo paradigm in which patients had to switch hand movements92. A third, recent Go-NoGo study was more complex, in that there was an additional monetary reward/loss component incorporated into the design83. This was a single unit recording study in both STN and GPi and mainly focused on reward related neural findings, but did report that reward related firing rates were not differentially modulated by motor initiation or inhibition.
The SST paradigm, in which the stop signal comes after the initial go signal at a variable delay, is supported by a computationally described analysis framework—the race model98. The first study to investigate STN LFP signals during the SST showed an increase in beta oscillations after the stop signal which was higher on successful, compared to failed stops92. This has been replicated in other studies, related to both reactive and proactive inhibition and in a vocal stopping task which found that stopping related beta changes are right lateralized (Fig. 4)93,95,96. A further study which did examine for across-subject symptom differences using classical categorical symptom classification, showed a reduction in beta desynchronisation (a relative increase) in successful stopping94. However, this study also showed that in the ON medication state, successful inhibition of the response was associated with a decrease in cortico-subthalamic gamma power and coherence. This gamma related finding was notably only present in the 4 out of 10 subjects with dopamine agonist related ICDs but hasn’t been replicated in other studies which found conflicting results99. Recent work has also shown that beta activity is likely complemented by rapid evoked responses through the hyperdirect pathway from prefrontal areas including the right inferior frontal gyrus for mediating response inhibition100.
Motor inhibition following prepotent action planning and initiation is a final stage of response control. It is here shown to be partly related to motor network beta signals, with an increase in beta, multiplexed with other signals, being found at the time of motor inhibition and associated with successful stopping.
Reward learning and updating
Whilst there have been a number of studies investigating motor learning and outcome related updating101,102,103,104, to date there have been very few studies investigating reward learning, with many reward studies only reporting on the reward decision making epoch rather than post-feedback physiology67. One study directed towards reward feedback and learning investigated whether beta oscillations are specifically modulated by outcomes in a reinforcement learning task105. In the task, subjects made self-directed joystick movements that were then mapped onto dynamic reward probabilities that had to be learnt. This study found that although STN alpha and low beta activity was negatively correlated with previous reinforcement magnitudes, these did not specifically correlate with reward prediction errors (RPEs). This is somewhat surprising given the link between beta oscillations and dopamine, which also signal RPEs77. This might be partially explained by dissociated effects of phasic and tonic dopamine neuronal firing or to specifics of the task and recording / processing techniques. Notably, one recent study evaluated LFP changes during a reward task, but this was in only three PD patients undergoing DBS of the PPN106. They showed that in response to reward outcome (but not to no-reward outcome) there was an increased power in alpha-beta bands (10–20 Hz) in PPN106, supporting further reward and RPE related research in PD.
A fuller account of the neurophysiology and neural signals of reward and outcome learning is needed to fully capture the time varying changes in NPS seen in PD over time, particularly the transition from simple impulsive to compulsive behaviours45.
Discussion
Non-motor symptoms and specifically NPS in PD are common and highly disabling, yet, their pathophysiological basis is unclear and the impact on these symptoms of pharmacological and surgical treatments are still actively debated107,108.
In this review we examine previous studies employing intracranial neurophysiology in patients with PD to explore biomarkers of mechanisms underlying the generation and maintenance of mood, motivation and behavioral symptoms. We highlight behavioural dimensions that are particularly pertinent to PD with specific reference to 1) emotional processing, 2) executive control 3) subjective valuation (reward and cost evaluation) 4) motor control and 5) learning and updating.
The available data suggest that there are segregated spatio-spectral neural networks within the brain that may partially index separable dimensions of cognitive sub-processes underpinning mood, motivation and behaviour. Emotional information appears to involve a component of the alpha oscillations expressed in the STN. Executive control and more specifically conflict detection shows an association with pre-frontal theta activity synchronized to a component of STN theta activity. There is also evidence that subjective valuation (in terms of reward, loss and effort) is also partially mediated through low frequency oscillations - mainly a theta component. Regarding motor control and action inhibition, the evidence supports a link between motor cortical - subcortical beta and motor inhibition, potentially multiplexed with gamma. The presence of different neural networks, indexed by different spatial and spectral patterns, for the different cognitive dimensions suggests that these mechanisms are likely computed through different networks. However, although the evidence suggests associations between different spatio-spectral networks and underlying cognitive subprocesses, we do not expect there to be perfect or simple one-to-one mapping between a neurophysiological signal and a complex computational process.
The research to date has highlighted potential biomarkers for future neuropsychiatric state tracking in PD that could be applied to personalized, adaptive, DBS therapies. The studies also show how different cognitive components of high dimensional clinical constructs, such as impulsivity or apathy, appear to be subserved by spatially overlapping but spectrally segregated networks. This is well illustrated by the medial prefrontal - subthalamic network in the theta range that subserves components of impulsivity and can be mapped to underlying computational processes including decision threshold setting. This can be contrasted with a motor cortical area - subcortical beta network which relates to action control and inhibition. Therefore, although spatially overlapping, these networks can be segregated through spectral features which can be used to identify cortical to subcortical distributed networks related to specific cognitive processes. We propose this approach could be used to further identify other spatio-spectral networks, related to distinct cognitive subprocesses, including for example reward (prefrontal cortex - basal ganglia) or effort (supplementary area - basal ganglia) networks. Furthermore, and more broadly, this supports a model whereby cortical information from segregated regions, subserving different cognitive functions, are funnelled into the basal ganglia, but remain partially segregated via dissociable temporal dynamics, indexed through spectral properties. Interactions between these spatially overlapping, but spectrally distinct networks, may be served by higher order inter-frequency interactions in basal ganglia cortical connections towards integration and action selection109. This spatio-spectral network model can complement and also likely integrate with rate firing circuit models, including for example classical prefrontal-basal ganglia parallel organization models and direct versus indirect within basal ganglia accounts23,110.
Limitations and suggestions for behavioural neurophysiology in PD
Although promising, computational neurophysiology aimed at understanding fundamental mechanisms of motivation and its dysfunction is still at an early stage. A key issue relates to the specificity of identified biomarkers for specific symptoms, NPS and cognitive sub-processes. The data to date supports the hypothesis that there may be meaningful and clinically useful segregation between specific spatio-spectral networks with dissociable cognitive subprocesses. Neurophysiological recordings, with high spatial and temporal resolution, significantly increase the specificity of mapping from neural activity to NPS in PD compared to alternative techniques. However, single site LFP recordings, even in narrow power bands may contain activity from multiplexed underlying neuronal pools linked to different networks. Low frequency activity particularly has more spatial spread which could exacerbate this mixing of signals. Therefore, at a given site, there is not likely a simple one-to-one mapping between an oscillatory frequency band and a symptom or behavioural mechanism. We therefore recommend recording of multi-site (cortical and subcortical) LFPs where possible to investigate spatio-spectral networks rather than simply trying to relate single-site single power bands to individual symptoms of computational processes. Furthermore, many of the underlying dimensions and associated behavioural paradigms are not perfectly orthogonal to each other and therefore will correlate with multiple neural activities.
It is important to stress that future studies should focus on decorrelating the contributions of different dimensions of motivation related cognitive processing (including motor processes such as vigour), given that NPS are highly correlated. This could be achieved by testing multiple different behavioural paradigms together in a single cohort in order to examine for specificity of correlations or through using computational models that can isolate separable latent cognitive variables. Notably a majority of studies have been recorded from the STN, rather than GPi, and yet research to date suggest that these two nodes are functionally dissociable and therefore further interrogation of the GPi (and other targets) will be valuable. Intracranial physiology is also currently restricted to PD patients with relatively long disease duration and severe motor symptoms as inclusion criteria for DBS and caution is warranted before extrapolating these findings to all patients with PD. However, pre-operative neuropsychiatric evaluation of DBS patients selects for patients without extremes of NPS which supports a degree of generalization.
While there is a wealth of behavioural research in PD, there is a relative lack of studies specifically designed to investigate neural biomarkers of NPS based on categorical assessments of clinical severity. Integrating the categorical and dimensional approaches and investigating the role of dopaminergic medications through longitudinal (within-subject) studies will help reveal more about inter-individual and the intra-individual differences. Also, this will clarify whether neural correlates identified are secondary to the symptom themselves (states) or related to predisposing factors that make certain PD patients more prone to develop symptoms (traits). Further, there is a current lack of research investigating the underlying neurocircuitry and neural signals of reward learning in PD, which could be critical to understanding the longitudinal evolution of behavioral symptoms in PD, particularly the progression towards more compulsive, habitual responding111,112. A progression from action, to habits and then compulsions in PD shows parallels to processes that have been mapped out in addiction processes113.
Towards future principled therapies for neuropsychiatric symptoms
Previous research findings using intracranial recordings have been used to guide treatment developments for motor symptoms in PD, including the use of STN beta power as a neural marker to drive adaptive DBS stimulation in PD for bradykinesia and rigidity15,114,115,116. Adopting the same approach for non–motor symptoms and identification of the precise neural markers of NPS could be used in the future for closed-loop therapy for mood, motivation and behavioral symptoms in PD. The recent release of new commercial DBS devices that sense neural signals as well as having the capability to deliver precisely temporally targeted stimulation according to neurophysiological biomarkers opens a direct and potentially rapid translational pipeline to leverage this emerging knowledge base32.
PD has been described as the quintessential neuropsychiatric disorder2. Using neurophysiological approaches combined with dimensional paradigms and categorical classification, we have the potential to uncover fundamental neurophysiological mechanisms of mood, motivation and behavioural symptoms in PD. This understanding could then be used towards the characterization of accurate biomarkers and principled therapy developments in PD, and further applied to a wide range of other neuropsychiatric disorders.
Data availability
All the data presented as part of the manuscript are already available and published in the literature. No datasets were generated or analysed during the current study.
References
de Lau, L. M. L. & Breteler, M. M. B. Epidemiology of Parkinson’s disease. Lancet Neurol. 5, 525–535 (2006).
Weintraub, D. & Burn, D. J. Parkinson’s disease: the quintessential neuropsychiatric disorder. Mov. Disord. 26, 1022–1031 (2011).
den Brok, M. G. H. E. et al. Apathy in Parkinson’s disease: a systematic review and meta-analysis. Mov. Disord. 30, 759–769 (2015).
Husain, M. & Roiser, J. P. Neuroscience of apathy and anhedonia: a transdiagnostic approach. Nat. Rev. Neurosci. 19, 470–484 (2018).
Le Heron, C., Apps, M. A. J. & Husain, M. The anatomy of apathy: A neurocognitive framework for amotivated behaviour. Neuropsychologia 118, 54–67 (2018).
Vriend, C. et al. Depression and impulse control disorders in Parkinson’s disease: two sides of the same coin? Neurosci. Biobehav. Rev. 38, 60–71 (2014).
Ardouin, C. et al. Assessment of hyper-and hypodopaminergic behaviors in Parkinson’s disease. Rev. Neurol. 165, 845–856 (2009).
van der Velden, R. M. J., Broen, M. P. G., Kuijf, M. L. & Leentjens, A. F. G. Frequency of mood and anxiety fluctuations in Parkinson’s disease patients with motor fluctuations: A systematic review. Mov. Disord. 33, 1521–1527 (2018).
Czernecki, V. et al. Apathy following subthalamic stimulation in Parkinson disease: a dopamine responsive symptom. Mov. Disord. 23, 964–969 (2008).
Sierra, M. et al. Apathy and Impulse Control Disorders: Yin & Yang of Dopamine Dependent Behaviors. J. Parkinsons. Dis. 5, 625–636 (2015).
Favier, M. et al. Pramipexole reverses Parkinson’s disease-related motivational deficits in rats. Mov. Disord. 29, 912–920 (2014).
Pontone, G. M. et al. ‘Anxious fluctuators’ a subgroup of Parkinson’s disease with high anxiety and problematic on-off fluctuations. Parkinsonism Relat. Disord. 105, 62–68 (2022).
Fogelson, N. et al. Different functional loops between cerebral cortex and the subthalmic area in Parkinson’s disease. Cereb. Cortex 16, 64–75 (2006).
van Wijk, B. C. M. et al. Functional connectivity maps of theta/alpha and beta coherence within the subthalamic nucleus region. Neuroimage 257, 119320 (2022).
Little, S. et al. Adaptive deep brain stimulation in advanced Parkinson disease. Ann. Neurol. 74, 449–457 (2013).
Gilron, R. ’ee et al. Long-term wireless streaming of neural recordings for circuit discovery and adaptive stimulation in individuals with Parkinson’s disease. Nat. Biotechnol. 39, 1078–1085 (2021).
Zahed, H. et al. The neurophysiology of sleep in Parkinsonas disease. Mov. Disord. 36, 1526–1542 (2021).
Gratwicke, J., Jahanshahi, M. & Foltynie, T. Parkinson’s disease dementia: a neural networks perspective. Brain 138, 1454–1476 (2015).
Carceles-Cordon, M., Weintraub, D. & Chen-Plotkin, A. S. Cognitive heterogeneity in Parkinson’s disease: A mechanistic view. Neuron https://doi.org/10.1016/j.neuron.2023.03.021 (2023).
de Hemptinne, C. et al. Prefrontal physiomarkers of anxiety and depression in Parkinson’s disease. Front. Neurosci. 15, 748165 (2021).
Disner, S. G., Beevers, C. G., Haigh, E. A. P. & Beck, A. T. Neural mechanisms of the cognitive model of depression. Nat. Rev. Neurosci. 12, 467–477 (2011).
Joyal, M. et al. Characterizing emotional Stroop interference in posttraumatic stress disorder, major depression and anxiety disorders: A systematic review and meta-analysis. PLoS One 14, e0214998 (2019).
Alexander, G. E., DeLong, M. R. & Strick, P. L. Parallel organization of functionally segregated circuits linking basal ganglia and cortex. Annu. Rev. Neurosci. 9, 357–381 (1986).
Volkmann, J., Daniels, C. & Witt, K. Neuropsychiatric effects of subthalamic neurostimulation in Parkinson disease. Nat. Rev. Neurol. 6, 487–498 (2010).
Rappel, P. et al. Theta‐alpha oscillations characterize emotional subregion in the human ventral subthalamic nucleus. Mov. Disord. https://doi.org/10.1002/mds.27910 (2019).
Sun, Y. et al. α and θ oscillations in the subthalamic nucleus are potential biomarkers for Parkinson’s disease with depressive symptoms. Parkinsonism Relat. Disord. 90, 98–104 (2021).
Huebl, J. et al. Oscillatory subthalamic nucleus activity is modulated by dopamine during emotional processing in Parkinson’s disease. Cortex 60, 69–81 (2014).
Huebl, J. et al. Modulation of subthalamic alpha activity to emotional stimuli correlates with depressive symptoms in Parkinson’s disease. Mov. Disord. 26, 477–483 (2011).
Sieger, T. et al. Distinct populations of neurons respond to emotional valence and arousal in the human subthalamic nucleus. Proc. Natl Acad. Sci. USA 112, 3116–3121 (2015).
Buot, A. et al. Processing of emotional information in the human subthalamic nucleus. J. Neurol. Neurosurg. Psychiatry 84, 1331–1338 (2013).
Buot, A. et al. Emotions Modulate Subthalamic Nucleus Activity: New Evidence in Obsessive-Compulsive Disorder and Parkinson’s Disease Patients. Biol Psychiatry Cogn Neurosci Neuroimaging https://doi.org/10.1016/j.bpsc.2020.08.002 (2020).
Brücke, C. et al. The subthalamic region is activated during valence-related emotional processing in patients with Parkinson’s disease. Eur. J. Neurosci. 26, 767–774 (2007).
Kühn, A. A. et al. Activation of the subthalamic region during emotional processing in Parkinson disease. Neurology 65, 707–713 (2005).
Eitan, R. et al. Asymmetric right/left encoding of emotions in the human subthalamic nucleus. Front. Syst. Neurosci. 7, 69 (2013).
Péron, J. et al. Vocal emotion decoding in the subthalamic nucleus: An intracranial ERP study in Parkinson’s disease. Brain Lang. 168, 1–11 (2017).
Borod, J. C. et al. Right hemisphere emotional perception: evidence across multiple channels. Neuropsychology 12, 446–458 (1998).
Mandali, A. et al. Acute Time-Locked Alpha Frequency Subthalamic Stimulation Reduces Negative Emotional Bias in Parkinson’s Disease. Biological Psychiatry: Cognitive Neuroscience and Neuroimaging https://doi.org/10.1016/j.bpsc.2020.12.003 (2020).
Gatto, E. M. & Aldinio, V. Impulse Control Disorders in Parkinson’s Disease. A Brief and Comprehensive Review. Front. Neurol. 10, 351 (2019).
Weintraub, D. & Claassen, D. O. Impulse Control and Related Disorders in Parkinson’s Disease. Int. Rev. Neurobiol. 133, 679–717 (2017).
Kelly, M. J., Baig, F., Hu, M. T.-M. & Okai, D. Spectrum of impulse control behaviours in Parkinson’s disease: pathophysiology and management. J. Neurol. Neurosurg. Psychiatry 91, 703–711 (2020).
Voon, V. et al. Impulse control disorders and levodopa-induced dyskinesias in Parkinson’s disease: an update. Lancet Neurol. 16, 238–250 (2017).
Claassen, D. O. et al. Proficient motor impulse control in Parkinson disease patients with impulsive and compulsive behaviors. Pharmacol. Biochem. Behav. 129, 19–25 (2015).
Ricciardi, L. et al. Acting without being in control: Exploring volition in Parkinson’s disease with impulsive compulsive behaviours. Parkinsonism Relat. Disord. 40, 51–57 (2017).
Hannah, R. & Aron, A. R. Towards real-world generalizability of a circuit for action-stopping. Nat. Rev. Neurosci. 22, 538–552 (2021).
Dawson, A. et al. Neurocognitive correlates of medication-induced addictive behaviours in Parkinson’s disease: A systematic review. Eur. Neuropsychopharmacol. 28, 561–578 (2018).
Napier, T. C. et al. Linking neuroscience with modern concepts of impulse control disorders in Parkinson’s disease. Mov. Disord. 30, 141–149 (2015).
Rossi, P. J. et al. Impulsivity in Parkinson’s disease is associated with altered subthalamic but not globus pallidus internus activity. J. Neurol. Neurosurg. Psychiatry 88, 968–970 (2017).
Micheli, F. et al. Impulsivity Markers in Parkinsonian Subthalamic Single-Unit Activity. Mov. Disord. https://doi.org/10.1002/mds.28497 (2021).
Rodriguez-Oroz, M. C. et al. Involvement of the subthalamic nucleus in impulse control disorders associated with Parkinson’s disease. Brain 134, 36–49 (2011).
Ricciardi, L. et al. Neurophysiological Correlates of Trait Impulsivity in Parkinson’s Disease. Mov. Disord. 36, 2126–2135 (2021).
Rosa, M. et al. Pathological gambling in Parkinson’s disease: subthalamic oscillations during economics decisions. Mov. Disord. 28, 1644–1652 (2013).
Mazzoni, A. et al. Subthalamic Neural Activity Patterns Anticipate Economic Risk Decisions in Gambling. eNeuro 5, ENEURO.0366-17.2017 (2018).
Eisinger, R. S. et al. Distinct roles of the human subthalamic nucleus and dorsal pallidum in Parkinson’s disease impulsivity. Biol. Psychiatry https://doi.org/10.1016/j.biopsych.2021.03.002 (2021).
Fineberg, N. A. et al. New developments in human neurocognition: clinical, genetic, and brain imaging correlates of impulsivity and compulsivity. CNS Spectr. 19, 69–89 (2014).
Stroop, J. R. Studies of interference in serial verbal reactions. J. Exp. Psychol. 18, 643 (1935).
Eriksen, B. A. & Eriksen, C. W. Effects of noise letters upon the identification of a target letter in a nonsearch task. Percept. Psychophys. 16, 143–149 (1974).
Simon, J. R. Reactions toward the source of stimulation. J. Exp. Psychol. 81, 174–176 (1969).
Zavala, B. et al. Midline Frontal Cortex Low-Frequency Activity Drives Subthalamic Nucleus Oscillations during Conflict. J. Neurosci. 34, 7322–7333 (2014).
Zavala, B. et al. Decisions Made with Less Evidence Involve Higher Levels of Corticosubthalamic Nucleus Theta Band Synchrony. J. Cogn. Neurosci. 28, 811–825 (2016).
Brittain, J.-S. et al. A role for the subthalamic nucleus in response inhibition during conflict. J. Neurosci. 32, 13396–13401 (2012).
Ghahremani, A. et al. Event-related deep brain stimulation of the subthalamic nucleus affects conflict processing. Ann. Neurol. 84, 515–526 (2018).
Duprez, J. et al. Subthalamic nucleus local field potentials recordings reveal subtle effects of promised reward during conflict resolution in Parkinson’s disease. Neuroimage 197, 232–242 (2019).
Aulická, Š. R. et al. Subthalamic nucleus involvement in executive functions with increased cognitive load: a subthalamic nucleus and anterior cingulate cortex depth recording study. J. Neural Transm. 121, 1287–1296 (2014).
Zavala, B. et al. Subthalamic nucleus local field potential activity during the Eriksen flanker task reveals a novel role for theta phase during conflict monitoring. J. Neurosci. 33, 14758–14766 (2013).
Wessel, J. R., Waller, D. A. & Greenlee, J. D. Non-selective inhibition of inappropriate motor-tendencies during response-conflict by a fronto-subthalamic mechanism. Elife 8, e42959 (2019).
Hell, F., Taylor, P. C. J., Mehrkens, J. H. & Bötzel, K. Subthalamic stimulation, oscillatory activity and connectivity reveal functional role of STN and network mechanisms during decision making under conflict. Neuroimage https://doi.org/10.1016/j.neuroimage.2018.01.001 (2018).
Cavanagh, J. F. et al. Subthalamic nucleus stimulation reverses mediofrontal influence over decision threshold. Nat. Neurosci. https://doi.org/10.1038/nn.2925 (2011).
Gold, J. I. & Shadlen, M. N. The neural basis of decision making. Annu. Rev. Neurosci. 30, 535–574 (2007).
Herz, D. M., Zavala, B. A., Bogacz, R. & Brown, P. Neural Correlates of Decision Thresholds in the Human Subthalamic Nucleus. Curr. Biol. 26, 916–920 (2016).
Herz, D. M. et al. Distinct mechanisms mediate speed-accuracy adjustments in cortico-subthalamic networks. Elife 6, e21481 (2017).
Zavala, B. et al. Cognitive control involves theta power within trials and beta power across trials in the prefrontal-subthalamic network. Brain 141, 3361–3376 (2018).
Herz, D. M. et al. Mechanisms Underlying Decision-Making as Revealed by Deep-Brain Stimulation in Patients with Parkinson’s Disease. Curr. Biol. 28, 1169–1178.e6 (2018).
Zavala, B., Jang, A. I. & Zaghloul, K. A. Human subthalamic nucleus activity during non-motor decision making. Elife 6, e31007 (2017).
Fumagalli, M. et al. Conflict-dependent dynamic of subthalamic nucleus oscillations during moral decisions. Soc. Neurosci. 6, 243–256 (2011).
Zaghloul, K. A. et al. Neuronal activity in the human subthalamic nucleus encodes decision conflict during action selection. J. Neurosci. 32, 2453–2460 (2012).
Alanazi, F. I. et al. Neurophysiological responses of globus pallidus internus during the auditory oddball task in Parkinson’s disease. Neurobiol. Dis. 159, 105490 (2021).
Schultz, W. Reward functions of the basal ganglia. J. Neural Transm. 123, 679–693 (2016).
Chong, T. T. J. et al. Dopamine enhances willingness to exert effort for reward in Parkinson’s disease. Cortex 69, 40–46 (2015).
Muhammed, K. et al. Reward sensitivity deficits modulated by dopamine are associated with apathy in Parkinson’s disease. Brain 139, 2706–2721 (2016).
Zénon, A. et al. The human subthalamic nucleus encodes the subjective value of reward and the cost of effort during decision-making. Brain 139, 1830–1843 (2016).
Pearson, J. M., Hickey, P. T., Lad, S. P., Platt, M. L. & Turner, D. A. Local Fields in Human Subthalamic Nucleus Track the Lead-up to Impulsive Choices. Front. Neurosci. 11, 646 (2017).
Lejuez, C. W. et al. Evaluation of a behavioral measure of risk taking: the Balloon Analogue Risk Task (BART). J. Exp. Psychol. Appl. 8, 75–84 (2002).
Justin Rossi, P. et al. The human subthalamic nucleus and globus pallidus internus differentially encode reward during action control. Hum. Brain Mapp. 38, 1952–1964 (2017).
Knutson, B., Westdorp, A., Kaiser, E. & Hommer, D. FMRI visualization of brain activity during a monetary incentive delay task. Neuroimage 12, 20–27 (2000).
Howell, N. A. et al. Preliminary evidence for human globus pallidus pars interna neurons signaling reward and sensory stimuli. Neuroscience 328, 30–39 (2016).
Al-Ozzi, T. M., Botero-Posada, L. F., Lopez Rios, A. L. & Hutchison, W. D. Single unit and beta oscillatory activities in subthalamic nucleus are modulated during visual choice preference. Eur. J. Neurosci. 53, 2220–2233 (2021).
Mosher, C. P., Mamelak, A. N., Malekmohammadi, M., Pouratian, N. & Rutishauser, U. Distinct roles of dorsal and ventral subthalamic neurons in action selection and cancellation. Neuron 109, 869–881.e6 (2021).
Cacciola, A. et al. Structural connectivity-based topography of the human globus pallidus: Implications for therapeutic targeting in movement disorders. Mov. Disord. 34, 987–996 (2019).
Donders, F. C. On the speed of mental processes. Acta Psychol. 30, 412–431 (1969).
Logan, G. D. & Cowan, W. B. On the ability to inhibit thought and action: A theory of an act of control. Psychol. Rev. 91, 295–327 (1984).
Kühn, A. A. et al. Event-related beta desynchronization in human subthalamic nucleus correlates with motor performance. Brain 127, 735–746 (2004).
Williams, D. et al. Behavioural cues are associated with modulations of synchronous oscillations in the human subthalamic nucleus. Brain 126, 1975–1985 (2003).
Ray, N. J. et al. The role of the subthalamic nucleus in response inhibition: evidence from local field potential recordings in the human subthalamic nucleus. Neuroimage 60, 271–278 (2012).
Alegre, M. et al. The subthalamic nucleus is involved in successful inhibition in the stop-signal task: a local field potential study in Parkinson’s disease. Exp. Neurol. 239, 1–12 (2013).
Benis, D. et al. Subthalamic nucleus activity dissociates proactive and reactive inhibition in patients with Parkinson’s disease. Neuroimage 91, 273–281 (2014).
Ghahremani, A. et al. Stopping and slowing manual and spoken responses: Similar oscillatory signatures recorded from the subthalamic nucleus. Brain Lang. 176, 1–10 (2018).
Wessel, J. R. et al. Stop-related subthalamic beta activity indexes global motor suppression in Parkinson’s disease. Mov. Disord. 31, 1846–1853 (2016).
Verbruggen, F. et al. A consensus guide to capturing the ability to inhibit actions and impulsive behaviors in the stop-signal task. Elife 8, e46323 (2019).
Fischer, P. et al. Subthalamic nucleus gamma activity increases not only during movement but also during movement inhibition. Elife 6, 1–21 (2017).
Chen, W. et al. Prefrontal-Subthalamic Hyperdirect Pathway Modulates Movement Inhibition in Humans. Neuron https://doi.org/10.1016/j.neuron.2020.02.012 (2020).
Tan, H., Jenkinson, N. & Brown, P. Dynamic neural correlates of motor error monitoring and adaptation during trial-to-trial learning. J. Neurosci. 34, 5678–5688 (2014).
Torrecillos, F., Alayrangues, J., Kilavik, B. E. & Malfait, N. Distinct Modulations in Sensorimotor Postmovement and Foreperiod β-Band Activities Related to Error Salience Processing and Sensorimotor Adaptation. J. Neurosci. 35, 12753–12765 (2015).
Tan, H. et al. Human subthalamic nucleus in movement error detection and its evaluation during visuomotor adaptation. J. Neurosci. 34, 16744–16754 (2014).
Alayrangues, J., Torrecillos, F., Jahani, A. & Malfait, N. Error-related modulations of the sensorimotor post-movement and foreperiod beta-band activities arise from distinct neural substrates and do not reflect efferent signal processing. Neuroimage 184, 10–24 (2019).
Schroll, H. et al. Reinforcement magnitudes modulate subthalamic beta band activity in patients with Parkinson’s disease. Sci. Rep. 8, 8621 (2018).
Skvortsova, V. et al. A Causal Role for the Pedunculopontine Nucleus in Human Instrumental Learning. Curr. Biol. 31, 943–954.e5 (2021).
Dafsari, H. S. et al. Nonmotor symptoms evolution during 24 months of bilateral subthalamic stimulation in Parkinson’s disease. Mov. Disord. 33, 421–430 (2018).
Scherrer, S. et al. Impulsivity and Compulsivity After Subthalamic Deep Brain Stimulation for Parkinson’s Disease. Front. Behav. Neurosci. 14, 47 (2020).
de Hemptinne, C. et al. Therapeutic deep brain stimulation reduces cortical phase-amplitude coupling in Parkinson’s disease. Nat. Neurosci. https://doi.org/10.1038/nn.3997 (2015).
Albin, R. L., Young, A. B. & Penney, J. B. The functional anatomy of basal ganglia disorders. Trends Neurosci. 12, 366–375 (1989).
Averbeck, B. & O’Doherty, J. P. Reinforcement-learning in fronto-striatal circuits. Neuropsychopharmacology 47, 147–162 (2022).
Averbeck, B. B., O’Sullivan, S. S. & Djamshidian, A. Impulsive and compulsive behaviors in Parkinson’s disease. Annu. Rev. Clin. Psychol. 10, 553–580 (2014).
Everitt, B. J. & Robbins, T. W. Drug Addiction: Updating Actions to Habits to Compulsions Ten Years On. Annu. Rev. Psychol. 67, 23–50 (2016).
Little, S. et al. Adaptive deep brain stimulation for Parkinson’s disease demonstrates reduced speech side effects compared to conventional stimulation in the acute setting. J. Neurol. Neurosurg. Psychiatry 87, 1388–1389 (2016).
Velisar, A. et al. Dual threshold neural closed loop deep brain stimulation in Parkinson disease patients. Brain Stimul. 12, 868–876 (2019).
Little, S. & Brown, P. Debugging Adaptive Deep Brain Stimulation for Parkinson’s Disease. Mov. Disord. 35, 555–561 (2020).
Chen, W. et al. Altered Prefrontal Theta and Gamma Activity during an Emotional Face Processing Task in Parkinson Disease. J. Cogn. Neurosci. 31, 1768–1776 (2019).
Sauleau, Paul et al. Involvement of the subthalamic nucleus in engagement with behaviourally relevant stimuli. Eur. J. Neurosci. 29, 931–942 (2009).
Acknowledgements
We are grateful to Professor Peter Brown for his input on the manuscript and for his scientific mentorship. LR receives research support from MRC award number MR/T023864/1. M.A. is supported by a Biotechnology and Biological Sciences Research Council David Phillips Fellowship (BB/R010668/2), a Jacobs Foundation Fellowship. S.L. is supported by the National Institute Of Neurological Disorders And Stroke of the National Institutes of Health under Award Number K23NS120037. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Author information
Authors and Affiliations
Contributions
L.R., S.L.: research project—conception, organization, execution; statistical analysis—review and critique; manuscript—writing of the first draft, review and critique. M.A.: manuscript—review and critique.
Corresponding author
Ethics declarations
Competing interests
S.L. provides paid consultancy input to Iota Biosciences and has provided paid educational services to Medtronic. S.L. is an unpaid scientific advisor to RuneLabs. L.R. and M.A. declare no competing interests. The authors declare no Competing Financial or Non-Financial Interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ricciardi, L., Apps, M. & Little, S. Uncovering the neurophysiology of mood, motivation and behavioral symptoms in Parkinson’s disease through intracranial recordings. npj Parkinsons Dis. 9, 136 (2023). https://doi.org/10.1038/s41531-023-00567-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41531-023-00567-0
