
Abstract
Augmenting the body with artificial limbs controlled concurrently to one’s natural limbs has long appeared in science fiction, but recent technological and neuroscientific advances have begun to make this possible. By allowing individuals to achieve otherwise impossible actions, movement augmentation could revolutionize medical and industrial applications and profoundly change the way humans interact with the environment. Here, we construct a movement augmentation taxonomy through what is augmented and how it is achieved. With this framework, we analyze augmentation that extends the number of degrees-of-freedom, discuss critical features of effective augmentation such as physiological control signals, sensory feedback and learning as well as application scenarios, and propose a vision for the field.
Similar content being viewed by others


Introduction
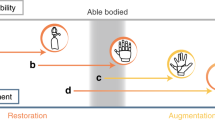
The goal of human movement augmentation is to extend a person’s movement abilities. When this augmentation increases the number of movement degrees-of-freedom (DoF augmentation), it can enable a person to perform tasks that are impossible to achieve with their natural limbs alone. An example would be the third arm that a person can control simultaneously to their natural arms in trimanual tasks (Fig. 1a). In this emerging paradigm, a user is endowed with a supernumerary effector (SE) in the form of a wearable limb (Fig. 1a), an external robot (Fig. 1c, e), or an effector in virtual reality (Fig. 1f). While human movement augmentation is often considered for unimpaired individuals, it uses technologies that originate from developments to restore functions in impaired individuals, such as prosthetics for amputees or exoskeletons for stroke patients. However, it is free from the typical constraints of restoration neurotechnology: it does not need to substitute a lost ability with the same function, and it is not bound to a natural appearance. Such freedom to implement out-of-the-box solutions could in turn be used to apply SEs for rehabilitation/restoration or to develop new technologies for aiding impaired individuals (Fig. 1c, d).

a Extra hand for assembly tasks. b Polydactyly hand with six fingers providing superior manipulation abilities4. c Third arm to facilitate activities of daily living in hemiplegics. d Centaur robot for stability and walking assistance. e Surgery with three tools controlled by the hands and a neural interface. f Augmented interaction with a mobile device can free one hand to e.g. operate a map. Panel a by Tobias Pistohl; b modified from ref. 4. Panels c, e, and f by Nathanael Jarrassé. Panel d by Camille Blondin.
Despite the recent growth in interest in DoF augmentation1,2,3, the realization of SEs that can be controlled independently from the natural limbs and in coordination with them has remained elusive. A fundamental open question is whether human users can control additional DoFs without limiting natural movement. In this regard, a recent study demonstrated that subjects born with an extra finger on each hand can control multiple extra DoFs, giving them superior manipulation abilities without any apparent movement deficits (Fig. 1b and ref. 4). However, it is unclear whether subjects can learn to control artificial supernumerary DoFs (sDoFs) that they are not born with, and whether this could enhance functional abilities. If so, where would such augmentation capabilities come from and what are their limits? How can the nervous system represent the extra limb and its relation to other limbs? These questions will impact the future of movement augmentation and determine which approaches are most suited.
This paper analyzes the potential and constraints for different DoF augmentation strategies by considering these questions. Compared to recent supernumerary robotic limb reviews1,2,3, particular emphasis is placed on the neuroscientific and technical factors that can enable the control of sDoFs, rather than on the specific device design and fabrication. In the first section we develop a taxonomy of movement augmentation, which yields the first classification of different types of augmentation. The components needed for augmentation are identified in the subsequent section. We then review and analyze the current implementations of DoF augmentation based on the proposed taxonomy, considering the potential features for each augmentation type. After we examine how the critical factors of feedback and learning affect these different augmentation types. Finally, we investigate the applications scenarios of DoF augmentation, and identify the impediments and open issues to make DoF augmentation a reality.
In this manuscript, relevant literature was identified using the following steps: (i) papers on supernumerary robotic limbs were first identified using the keywords “supernumerary robot” and “wearable robotic arm” as search terms in the IEEE explore, Web of Science, and Google Scholar search databases, over a period from 2000 to 2021. (ii) The 1340 papers found in this way were filtered to remove duplicate works and to ensure that the selected papers had a scope encompassing “experiments considering movement augmentation” or “the development or validation of a human augmentation control scheme”. This resulted in 95 manuscripts. (iii) Papers describing works on the same topic with similar device and/or applications were identified, and representative papers are discussed in the present manuscript. (iv) This review was complemented by author-specific knowledge with regards to the fields of “brain–computer interfaces”, “artificial proprioception” and “motor learning” which were included due to their relevance to topics discussed in later sections.
A taxonomy of movement augmentation
Movement augmentation can be classified based on the specific aspects of motor action that are enhanced (Fig. 2). Existing forms of augmentation include:
-
Power augmentation which increases the user’s forces or speed. Examples are exoskeletons5 and suits6 reducing physical load7 as well as cars increasing speed.
-
Workspace augmentation which extends the spatial reach of natural limbs, with tools such as a rake or an endoscope8, or through teleoperation or outer space manipulation9.
-
Command augmentation which addresses the limitations of the motor system by processing the user’s command signal. Examples include switching control between different tools in robot-aided surgery using a dedicated handle with a clutch10, or tremor attenuation to improve eye surgery through active noise cancellation with a robotic interface11.
These augmentation forms improve already existing movement abilities. In contrast, DoF augmentation endows subjects with extra abilities to interact with their environment. While it has only emerged in the last decades12,13,14, DoF augmentation could potentially reshape human-environment interaction as the examples of Fig. 1 illustrate.

The logos for each form of augmentation (figures by Camille Blondin) illustrate example applications. The five histograms correspond to whether or not the form of augmentation grants the user more DoFs than their body and provides them with explicit control, as well as the level of how ready each device is for widespread usage, and how much feedback and learning would be required.
DoF augmentation ideally provides independent and coordinated control of sDoFs with respect to one’s own natural DoFs. Hence, a mere increase in the number of mechanical DoFs is not sufficient for DoF augmentation as the additional DoFs also need to be controlled at least to some degree independently from the natural DoFs. This can be realized in three different ways (Fig. 2):
-
Autonomous DoF augmentation extends the number of DoFs involved in one or more tasks using autonomously controlled devices. For instance, a robot may help carry an object with its human user.
-
DoF augmentation by transfer, in contrast, lets the user control the sDoFs. However, it only extends the number of movement DoFs involved in a task by re-purposing other existing body DoFs that are task-irrelevant. An example would be a third arm controlled by foot movements for three-tool surgery.
-
Augmentation by DoF extension lets the user control the sDoFs by extending the body’s total number of movement DoFs. An example would be a third arm driven by neural activity that can be controlled independently from and concurrently with the natural limbs while preserving the full repertoire of natural movement abilities.
The different ways to achieve DoF augmentation are analyzed in Fig. 2. While all forms of DoF augmentation may provide sDoFs, only augmentation by extension grants the user both an increased number of movement DoFs and their direct control. The figure also illustrates the differences between these augmentation schemes in terms of their readiness to be used, their potential requirement for additional feedback devices, and the learning required for their use.
The assumption of both augmentation by transfer and extension is that the human user is able to voluntarily manipulate body signals that do not interfere with natural motion behaviors. Limbs not involved in a task, such as the foot while seated in bimanual manipulation, could be used to enlarge the range of possible actions, enabling augmentation by transfer. In addition, as the number of muscles is higher than the body’s mechanical DoFs, there is muscle redundancy that could potentially be used for augmentation by transfer and extension. Moreover, the number of neurons used for musculoskeletal control is much higher than the number of muscles, suggesting further potential DoF augmentation capability. Such areas in the space of possible signals which do not correlate with differences in movements, have been coined a “null space”15,16,17 in analogy to the null space of linear algebra.
Features of movement augmentation
DoF augmentation typically includes three components (Fig. 3): The supernumerary effector (SE) that provides the sDoFs, the command interface that converts user intention into commands for the SE; and the feedback devices, which give the user SE status knowledge. The SE can be a robotic limb or an effector in virtual reality. It can be wearable and move with the body (Fig. 1a, d), or can be separated, e.g., a robotic arm fixed to its user’s wheelchair (Fig. 1c). In addition, the technological design can be optimized to its functional task and, thus, may vary across applications. For instance, a surgical device can be controlled by the surgeon (Fig. 1e), while a mobile phone application (Fig. 1f) may be controlled while subjects can simultaneously use their hands.

An individual is augmented using a body, muscle or neural interface to control the supernumerary effector. Sensory information may be provided through feedback devices. The interfaces, supernumerary effector and feedback devices are shown at representative locations. While muscle interfaces are generally noninvasive, neural interfaces can be both invasive or noninvasive.
Existing SE research has mainly focused on developing supernumerary limbs, which typically comprise robotic arms18,19,20,21,22,23,24,25, fingers26,27,28,29,30,31 and legs32,33,34,35,36. Supernumerary arms are fixed to the user’s torso20,23,24, shoulders18, or elbow22. Applications include aircraft fuselage assembly19, construction37, and surgery38, while the complexity of their control has to date limited their usage. In contrast, supernumerary fingers and legs typically possess fewer sDoFs and have applications focused on aiding impaired individuals39 or gait support36. Supernumerary fingers have taken the form of either an extra thumb27,30 or additional stabilizing fingers26. Virtual SEs have been applied for studying a subject’s ability to use an SE40,41,42,43, or to better understand how subjects perceive augmentation through additional limbs13,44 or fingers45,46. However, to date, applications such as those in Fig. 1f have not been realized.
A command interface for SE control is required in many DoF augmentation applications. Three forms of the interface are considered (Fig. 3):
-
Body interfaces use the measured movement or force of a body segment. Body interfaces are in general noninvasive and may use limb movement, or information coming from the head such as gaze, facial expression, or the tongue.
-
Muscle interfaces pick up muscle activity to command the SE. Noninvasive interfaces can use surface electromyography (EMG), magnetomyography, ultrasound, or intramuscular EMG as an invasive alternative.
-
Neural interfaces extract signals from the nervous system. Noninvasive interfaces may use electroencephalography/magnetoencephalography (EEG/MEG), functional magnetic resonance imaging (fMRI), functional near-infrared spectroscopy (fNIRS), or the spiking activity of motor units. Invasive interfaces measuring signals inside the brain, spinal cord, or muscles may also be used.
The key terminology of human movement augmentation used throughout this manuscript is listed in Table 1.
Autonomous augmentation
In autonomous augmentation, the sDoFs are not directly controlled by the user. Autonomous augmentation can hence be considered as a special form of human–robot collaboration with two constraints: (i) the robotic agent does not share the control of the body DoF (in contrast to robotic exoskeletons) and instead is responsible for controlling additional DoFs to those of the human user; and (ii) the augmentation device is either worn or at least operated within the same workspace and used for the purpose of augmenting the human user. Autonomous augmentation may promote precise and quick movement while minimizing additional mental effort. However, it lacks continuous knowledge of the user’s desired behavior and therefore has been mainly used in specialized applications where SEs have very constrained behaviors, such as overhead assembly18, aircraft manufacturing19, or grasping support47.
Autonomous augmentation’s critical problems are user intent estimation and its transformation into SE action. For simple objectives such as bracing48 or gait support34, these two problems are typically translated into control problems. In this manner, the unknown user intent is often assumed to match the defined task. For example, the intent of a system such as that in Fig. 1d may be to maintain its posture and then its action to be executed is that of a stabilizing controller48. Such strategies provide safe and/or optimal action, but they give no flexibility to the user, and therefore can only be applied to specialized activities.
For more complex behaviors, autonomous augmentation relies on predictive schemes requiring the current state, task knowledge, and potentially the user’s physiological measurements. Dimensionality reduction or other machine-learning algorithms47,49,50 have been applied to control supernumerary fingers for which the action of the limb can be well imagined, however, this approach is limited to work under a small set of desired actions. Recently, an alternative of considering the autonomous SE as the follower within a redundant leader-follower system was proposed51 using an observer to estimate the user’s intent. While the method does not depend on previous data, it needs a task model meaning that it is limited to known actions.
Partial autonomy, which splits the sDoF allowing for those with a well-defined function to be autonomous while other sDoF are user-controlled, represents a means to benefit from autonomous augmentation while minimizing its disadvantages52,53. When and how to use it is an open research topic. For example, in ref. 53 principal component analysis and the predictability of the natural limb motion were used to split between autonomous and directly controlled sDoFs. Nature may also show us a way to select useful automatic behaviors. In humans, reflexes complement slower voluntary actions, where for instance, long-delay reflexes compensate for dynamic coupling54 and contribute to controlling standing55. The forces exerted by a wearable SE during use are not negligible and demand the user to compensate for them24. When using one or more SEs in dynamic scenarios21,24,56, the control could implement low-level automatic compensation for dynamic coupling between the natural limbs and SEs such as to ensure the body stability, so that the user could neglect them and focus on task control.
Augmentation by transfer
In augmentation by transfer, the human operator uses body DoFs not involved in a task to control the sDoFs and coordinate them with the natural DoFs. An example is given by excavator control, where successful excavation requires the simultaneous movement of the platform and bucket, which is achieved through simultaneous commands from the feet and hands. Compared to teleoperation that relocates DoFs, augmentation by transfer increases a task’s DoFs by redirecting DoFs not normally used in performing the intended task.
Augmentation by transfer typically uses a command input of movements21,30,57,58 or muscle activations20,59 that do not directly interfere with the task-specific motions so that the sDoFs are in the task’s null space (see the section “A taxonomy of movement augmentation”). Using volitional sDoF control with a suitable interface, augmentation by transfer enables the control of complex supernumerary limbs as has been demonstrated in enhancing dexterity30,60, advanced industrial settings61, or through the control of a 13 DoF robotic endoscope and tool system58,62.
A simple implementation of augmentation by transfer is to use DoFs from direct kinematic or force recordings, for instance from a 3D camera system57 or mechanical sliders63. The mental effort associated with augmentation by transfer may limit the possible movement speed and accuracy40,42. Pressure and bending sensors at the foot have commonly acted as an input source for seated tasks21 and a supernumerary thumb30,64. Additional sources of input have included pressure sensors in the mouth through tongue control65. The simultaneous use of position and force measurements demonstrates the potential of using body interfaces to control SEs with multiple DoFs21.
SEs can also be commanded using an actuated exoskeleton or endpoint robotic interface. Here, the interface measures position to control SEs and also provides force feedback that can facilitate control. For instance, a seated operator can use a passive foot interface placed on the ground to control four sDoF58. Active interfaces have been used with both feet25, a hand and a foot29, and an elbow66.
As augmentation by transfer requires an interface, good performance and user comfort demand that this interface fits the user’s anatomy and neuromechanics. Therefore, the interface should be adapted to the user’s characteristics such as size or movement patterns, and typical user features can inform the design52,58. Moreover, the mapping from user movement to SE command can be identified from an individual’s movement patterns using machine-learning techniques58.
Activation of muscles independent of the task can also be used, although this may result in large-signal variability. For example, EMG signals from the torso have been used to control simple supernumerary arms20, and the frontalis and auricularis facial muscles have been considered to control a one DoF supernumerary finger28,67. Despite muscles such as the Auricularis being independent of most motion, since they have an inherent function, we consider measurement of only their activation to be augmentation by transfer, since that function is impaired while they are used as an input.
sDoFs control may also be achieved using signals from the null space of the limbs used in the task52,68. For instance, it has been shown that the user’s arms can both generate natural motion and simultaneously control sDoFs68. However, such systems depend on interference between the natural DoFs and sDoFs, which has not yet been experimentally evaluated.
Some commercial surgical robots mimic augmentation by transfer, by using a clutch system to switch the control between DoFs and sDoFs10. While this allows a user to control sDoFs, it does not allow for simultaneous sDoF control, and was thus classified under “command augmentation”. This engineering solution, which has been found to result in inferior performance in surgical inspired tasks62,63, likely has a limited potential relative to augmentation by transfer.
Finally, autonomous augmentation and augmentation by transfer can also be combined using automatic motion sequences initiated by actions in the task’s null space. Here, the user provides direct commands of intent to trigger predefined sequences for controlling the sDoFs, by using signals including voice commands22, facial expressions69 or eye movements70. Hand gestures have also been used to trigger the movement of an artificial actuator attached to the user’s wrist59,60. While such systems can use more actions than is possible in typical autonomous augmentation, the control of the DoFs is still limited to activating predefined motions.
Augmentation by extension
In augmentation by extension, the body’s DoF are extended independently from all-natural DoFs, thereby preserving the natural movement repertoire. Autonomous augmentation uses an external operator for sDOF control, while augmentation by transfer uses task-irrelevant movements. Augmentation by extension instead uses physiological signals that can be modulated without interfering with natural limb control. Studies on augmentation by extension have only recently been conducted. A fundamental question is whether humans have the neural resources to control additional DoFs without limiting other functions71.
Several studies have investigated the applicability of using different muscular or neural signals to control sDoFs concurrently to and independently from natural movement. Muscular activity not associated with overt movement (“muscular null space”), for example, co-contraction of muscle groups, has been used for sDoF control concurrent to isometric force generation72. Neural control has been considered for instance in nonhuman primates who were encouraged to perform brain–computer interfaces (BCIs) tasks by modulating the firing rates of cortical neurons simultaneously to natural limb movements73,74. Control could be established with motor cortical neurons that were not tuned but also with neurons that were tuned to the natural movements at similar performance as the BCI only task74.
In humans, 2D cursor control was achieved where one DoF was controlled by finger movements and the other by high-gamma band (70–90 Hz) electrocorticographic (ECoG) activity emerging from a motor cortical site41. Subjects could dissociate their ECoG signals from the originally correlated finger movements and could modulate their signals largely independently from the ongoing finger movements despite the pre-experimental association between both.
During EEG-based BCI control, human subjects could simultaneously perform overt movements75,76. As EEG control signals were produced by movement imagination of limbs not involved in the performed overt movements, these studies, however, follow the approach of augmentation by transfer. In a more recent study, EEG signals evoked by grasping imagination have been used to trigger pre-programmed grasping movements of a third robotic arm while subjects balanced a ball on a board with their two hands77. However, the sources of the EEG control signals and the simultaneity of both tasks in this study are unclear78.
For spinal motor neuron activity obtained from high-density surface EMG79, human subjects could partially modulate the beta band (13–30 Hz) activity without altering the force produced by the innervated muscle43. Moreover, subjects could control a 2D cursor using the low-frequency (<7 Hz) activity that is directly related to the force and the beta-band activity from the motor neurons of the same muscle (see Fig. 4h). Even though the beta band control remained weak, this study provides some support for using motor neuron populations in human movement augmentation. Recent results indicate that subjects could also perform 2D cursor control with three motor units from the same muscle80. However, subjects were instructed to perform multiple natural DoF movements which is a known way to alter motor recruitment81. Despite the potential existence of a neural substrate allowing for selective motor unit control81, a recent study, using more constrained movements, questioned whether independent recruitment of motor units could be learnt82.

a An artistic vision of a third hand in 198212. Examples of autonomous augmentation with (b) arm to hold a part while working on it120 and c coordinated legs to help stable walking36. Augmentation by transfer (d) with EMG control of supernumerary arms20 and e for three hand surgery with flexible endoscope58. Haptic feedback (f) for extra finger96 and (g) to control grasping with supernumerary arms commanded by the feet21. Towards augmentation by extension with (h) noninvasive interface for 2D cursor control by motor neurons from the tibialis anterior muscles43. Low-frequency <7Hz and 20Hz sub-band of beta activity control the horizontal and vertical cursor movements. i Concurrent control of high-gamma band ECoG activity and finger movement41 to control a 2D cursor. Time-resolved spectrograms show ECoG activity during movements to the upper and lower left targets. ECoG activity in the 70–90 Hz band, which controls movements along the vertical axis, can be modulated independently from concurrent finger movements that control movements along the horizontal axis. Panel b by Alexis Poignet and Mahdi Khoramshahi, h by Simone Tanzarella. Panel i modified from ref. 41.
Note that in all aforementioned studies, the overall number of controlled DoF was low, movements were simple and natural limb movement was highly restricted, not reflecting its full repertoire. Moreover, in some studies different DoFs were controlled by signals associated with different body parts, and hence the approach was effectively augmentation by transfer. Thus, no study yet has demonstrated augmentation by extension and it remains an open question whether it can be realized.
A crucial consideration for the development of augmentation by extension is the choice of the physiological control signal. Besides being independent of natural limb movement and information-rich, the accessibility of the control signal is critical as augmentation by extension aims to provide general applications. EEG and MEG offer noninvasive brain signals, however, both recordings are prone to artifacts and have limited resolution and bandwidth. Moreover, current MEG is not portable and EEG and MEG’s usability may therefore be very limited, allowing only for a small number of sDoF controlled at rather low precision and reliability. Also, fMRI and fNIRS signals may be of limited use for augmentation given their relatively low temporal resolution and in the case of fMRI their non-portability. Recordings of single units or local field potentials in the brain may offer more information-rich and movement-independent signals, yet, these signals can only be recorded invasively and may not be appropriate for many applications. An emerging technique which may allow for wearable and noninvasive control of an SE is based on the spiking activities of multiple motor units obtained from high-density surface EMG recordings83. Future studies will have to investigate the amount of independent control that subjects can acquire, which features of spinal motor neuron firing can be controlled, and how this can be used for movement augmentation. Besides neural signals, muscular null space signals are an interesting alternative for movement augmentation that can also be recorded in a portable and noninvasive way and should be further investigated as a candidate signal for augmentation.
Sensory feedback
Representative existing systems illustrating the different categories of DoF augmentation are shown in Fig. 4. Current systems rely mainly on vision to control SE performance. This may limit the user’s task focus, can require significant mental effort, and is susceptible to occlusion. Studies on sensory feedback for prostheses have suggested that feedback plays a key role in enriching an artificial limb user’s experience and control84. Sensory feedback for sDoFs should not substitute natural limb feedback, but extend and complement it. Furthermore, this information is fundamental to achieve tentative SE embodiment, i.e., a combined internal representation together with the natural limbs which may reduce the mental effort of SE control85.
An often overlooked specificity of wearable SEs is that haptic feedback is intrinsically provided through the connection to the user’s body as well from the motors’ acoustic noise and vibration52. This may be used by the brain to model and embody the SE86, to acquire information on the environment87 or augment sensory information about the task by physical interaction with the natural limbs or collaborators88. In turn, this suggests that sensory feedback is more critical for a detached robot arm used as a SE or a virtual SE (Fig. 1c, e, f).
In natural limb proprioception, the sense of presence and kinematics/dynamics of body segments are known to play a central role in movement planning and execution89. Possible noninvasive feedback modalities to create similar artificial SE proprioception include vibrotactile motors90,91, electrotactile arrays92,93, or direct mechanical stimulation through pressure or skin stretch94,95. Tactile feedback has been provided for several supernumerary hands using a direct mapping of force to haptic sensation21,96,97. These systems have considered one or two DoF force feedback and only a few studies have considered the effect of sensory feedback to the augmentation91,93,96.
A number of questions need to be investigated to develop tactile and proprioceptive feedback for DoF augmentation: Would such feedback really represent added value compared to vision? Should the feedback translate position, velocity, torque or a mixture of them? Where should such feedback be relayed? And how does the feedback affect the user’s performance and SE embodiment? The answer for each of these questions will typically differ for each form of augmentation.
Augmentation by transfer uses the natural limbs not involved in a task to command a SE. Therefore, the user can rely on these limbs’ proprioception and forward model and may not need additional sensory feedback conveyed to other body parts. To enable the association of the feedback received on the natural limbs with the interaction of the SE with the environment, haptic feedback is required e.g., through a robotic interface25,38,58.
In autonomous augmentation, safety of operation requires that feedback be provided if or before the SE comes in contact with the body or with the environment. However, autonomous behaviors of the SE are implemented so as to discharge the SE user from controlling it in routine tasks. Therefore, continuous artificial feedback may not be required in addition to the naturally available feedback such as from vision or haptic feedback from the connection of the SE with the body. For example, the automatic compensation for dynamic coupling with the body should not be fed back as its role is to free the user from the corresponding mental effort and enable them to focus on the task.
Augmentation by extension can benefit most from a rich multimodal sensory feedback and is at the same time the most challenging class of augmentation to implement, as the motor system has no intrinsically associated sensory feedback system. Augmentation by extension allows the use of SEs in parallel to their limbs, thus noninvasive interfaces should exploit part of the body others than limbs, such as the back or the side of the trunk, the tongue, or the head. Minimally invasive interfaces could also offer a solution, such as neural interfaces implanted percutaneously98. For subjects with neurological impairments, other more invasive channels could be considered in the future, such as intraneural, dorsal root ganglion or epidural implants99. Due to their invasiveness, these solutions are likely limited in their potential application.
Learning
The achievable performance and skill with a SE depend on its design, the control interface, and the sensory feedback it provides. However, the performance of augmentation will also critically depend on the learning carried out with the SE in order to improve task performance.
Autonomous augmentation typically requires that the user comprehends the relationship between natural limb movement and autonomous behavior. As the SE’s behavior is designed to support human action, the user should normally learn to ignore the SE’s actions and focus on their relevant subtask. However, the sDoF available may result in the user selecting new strategies to perform the task, in analogy to possible behavioral changes that drivers make in adapting to an automatic gearbox. Finally, for complex autonomous sequences, the human user may learn to predict the SE’s behavior, both for safety and coordination, similar to learning predictive models in movement interaction88.
Augmentation by transfer uses the natural activation of certain body segments to control the sDoFs. As humans control and coordinate their body segments from before birth, we expect that the learning requirements can be reduced by exploiting existing coordination patterns. In such cases, it is mainly the mapping of the additional limbs’ signals to the sDoF control that needs to be learned. The underlying learning process may correspond to the learning of modified visuomotor coordination100 and force fields101, which can be learned quickly87. Indeed, learning a simple trimanual coordination task appears to require a duration in the range of an hour40,42. If instead new coordination patterns, which do not belong to the subject’s natural movement repertoire, are used to control the primary DoFs and the sDoFs, extended practice may be required. The level of coordination between the primary DoFs and sDoFs achievable in augmentation by transfer will also depend on the natural coordination between the associated natural limbs. For example, the coordination between one foot and hand may not be as efficient as between the two hands42,64. Several works have investigated the learning of skilled actions such as the coordination of two SEs20 or complex manipulation with a hand equipped with a supernumerary sixth finger28,64. This process requires significantly more time than simple monitor tasks40,42.
While the learning of augmentation by extension arguably depends on the way it is implemented, it requires that subjects can learn to modulate a control signal independently from natural movement. Several studies have demonstrated a high degree of flexibility and adaptability of cortical neurons: firing rates of individual motor cortical neurons can be conditioned102,103 and as a result controlled independently of muscle activity104 and neighboring neurons105. New mappings from firing rates of populations of motor cortical neuron to BCI-controlled cursor movement can be learned within sessions as long as the co-modulation of neurons is maintained as in natural movement106. Even mappings with altered co-modulation of neurons can be learned with training spanning several days107. These findings demonstrate a high level of cortical neuron adaptability. They were, however, not obtained during a movement augmentation paradigm combining neural control with natural limb movements. Moreover, the reported studies were based on intracortical recordings. It remains an open question whether noninvasive recordings exhibit similar flexibility.
How does the brain adapt and reorganize during the acquisition of SE control? There is little data on this question to date, yet we expect that reorganization of the brain may occur in multiple areas, and may depend on the type of augmentation as well as on the specific sensory feedback and methodology used for augmentation. In general, augmentation by transfer may induce changes similar to those seen in learning new motor skills or learning new inter-joint and inter-limb coordination patterns. Recently, a slight shift in fMRI correlates of single digits in primary sensorimotor areas was observed when subjects learned to use a supernumerary thumb commanded by their foot64, as was previously observed in piano players108. At the same time, no changes in the hand-foot association in primary sensorimotor areas were observed in64 after practicing with the foot-controlled supernumerary thumb. The use of a sixth finger has also been suggested to induce changes in the corticospinal output during imagined grasping with the supernumerary finger as compared to imagined pinch and whole-hand grasping109. For augmentation by extension, there are currently no studies that have examined reorganization in the brain while subjects learned to use the SE. A polydactyly individual with fully functional natural supernumerary digits (six per hand) exhibited dedicated neural resources to control the extra finger, as evidenced by fMRI correlates in ref. 4. However, this subject was born with supernumerary limbs and therefore their brain organization is the result of genetics and a long-term developmental process. The possibly different brain reorganization in adults using SE needs to be investigated in future studies.
A possible concern about learning to use a SE is that it may deteriorate the normal natural limb control. Could learn to control a SE overload the overall repertoire of brain function? The amount of training and the level of proficiency achieved by professional athletes or musicians would suggest that the brain is able to learn an almost unlimited number of skills. However, there are reports describing how hyper-trained function can impair others, such as London taxi drivers with exceptional navigation ability at the cost of limited new spatial memory110. In addition to plasticity, this concern is also linked with the overall mental effort that can be handled by the brain, the ability to process information which is limited111.
Application scenarios
DoF augmentation has been suggested for a range of medical, industrial and commercial applications, particularly in areas where multi-person collaboration would otherwise be required. Within laboratory settings, fields of application include aircraft fuselage assembly48, construction37, and surgery38,62. Wearable SEs for restorative purposes, including balance assistance20 and supernumerary finger’s for aiding hemiplegic stroke patients28,59 have also been tested on patients. However, there is currently no clear evidence to suggest that (i) subjects would have improved performance with the supernumerary limb, and (ii) the SE could be used in a practical setting given safety and regulatory constraints.
Within the different types of DoF augmentation, augmentation by transfer is likely the closest to being suitable for real-life applications, as it is based on direct user control obtained from DoFs that the user is already familiar with controlling. In particular, body interfaces such as that of27,30,62 exploit well-established technologies, such as pressure sensors and pedals, that users have a high familiarity with using for giving commands and therefore appear suited for potential broader trials. In contrast, autonomous augmentation is currently limited by the capabilities of intent estimation algorithms, which also adds safety/liability challenges. Augmentation by extension has yet to be demonstrated in laboratory experiments and therefore appears to be further from practical application than the other two types of DoF augmentation.
It is not yet clear which tasks are most suited for DoF augmentation due to a lack of understanding of the capability of human user’s to exploit it. In particular, the limits of the user’s ability to simultaneously coordinate their natural limbs with the SE needs to be better understood as this ability is a requirement of many of the proposed applications including robotic surgery and industrial assembly. To study the effect of the coordination between the SEs and natural limbs, we propose to identify tasks based upon (i) whether or not the dynamics of the hands are coupled (coupling); and (ii) whether or not the desired output of each hand depends on the others (dependence). Table 2 summarizes the coordination types in the case of manipulation with three limbs with examples of typical tasks. This involves typical three-handed tasks such as holding an elastic membrane, opening a door while holding a box with both hands and manoeuvring both the camera and tools in surgery. Using these coordination types, different tasks, and the relative augmentation performance may be evaluated.
Within this context, existing research has shown that without the presence of physical constraints (all uncoupled) superior performance is possible using three hands in place of two40,63. This is observed both when all hands are independent40, and when the sDoFs need to be coordinated with the natural DoF for operating a camera for position control (all dependent)63, as would be the case for surgery with a camera. In40 subjects also felt no additional mental effort for control, and in fact expressed a preference for using the sDoF in the task. When considering tasks that can only be performed with three hands, it was observed that subjects felt little change in mental effort irrespective of the condition when going from a bimanual reaching task to a trimanual task42. However, such coupling does result in reduced performance and when continuously tracking additionally leads to increased mental effort42. Finally, when comparing subject performance to that of dyads, the dyad has to date outperformed the single user controlling an SE who had the higher mental effort in all tested cases112,113. However, the relative difference between results appears to reduce in coupled motion (all coupled and all dependent)112, and may disappear when haptic feedback and some learning is provided113, although users still reported increased mental effort.
Towards effective human movement augmentation
The field of DoF augmentation has exhibited a steady increase in research activity over the last decade1,2. In this regard, a series of pioneering studies14,20,26,32,47 have explored various robotic SEs and their autonomous or movement/muscle based control as well as their application to augment movement. Basic related neuroscience aspects such as natural SE4, multitasking, independence and coordination of SE and natural limbs40,57, learning64,113, SE embodiment13,46, and the feasibility of true DoF augmentation41, have also been investigated, providing foundational knowledge of user capability for augmentation. In this section, we analyze the limitations of current systems and propose several areas where we think future work should focus to make DoF augmentation a reality. Key open questions for DoF augmentation are also highlighted in Table 3.
Autonomous augmentation
Autonomous augmentation represents a form of human–robot interaction that has been little investigated, in particular, in terms of the possible interactions and control strategies. Current systems have been restricted to simple and well-constrained applications. Partial autonomy represents one solution to expand the set of possible actions e.g., through partitioning sDoF between autonomous and manual control53. More complex interaction behaviors are also possible. To understand what kinds of SE behaviors could be implemented, we consider the interaction framework of114. A strategy that has been used to implement autonomous augmentation consists of dividing the task in independent subtasks for the human and the SE. For instance, a surgeon is in charge of the whole operation but for automatic knot tying the robot takes over. Another relatively simple autonomous augmentation strategy consists of the “assistance behavior” of114, where the SE control is strictly subordinate to natural limb motion. For instance, to manipulate a large object with three hands, the SE would coordinate its movements to maintain shape or a constant force with respect to the natural hands. However, more complex interaction control strategies could be used where the SE is considered as an autonomous agent. For instance, a third arm may be used for robot-assisted physical rehabilitation according to an egalitarian control scheme115. Rich interactive behaviors of an autonomous SE with the natural limbs may be implemented using differential game theory114,115.
Given that most applications of movement augmentation will require contact between a human and an artificial mechanism, the safety of that interaction must be considered before future applications are possible. While this is an issue to be considered in all forms of augmentation, its impact is likely greatest in autonomous augmentation for which the user lacks direct control of the SE. For instance, computer-controlled reflex mechanisms should be developed to prevent the SE from harming the user or a nearby person.
Augmentation by transfer
Augmentation by transfer requires that users possess the capacity to simultaneously and independently control multiple limbs or muscles. Volitional modulation of control signals needs to be carried out together with ongoing movement. While the body can simultaneously control multiple DoFs, for instance coordinated motion of the hands and feet, movement augmentation may increase task complexity and require multitasking. The brain may have limits on the total number of DoFs it can control as well as on the complexity and number of subtasks it can carry out simultaneously. These limits will need to be experimentally investigated to determine the possible performance.
Some applications will require augmented sensory feedback, for which basic questions need to be investigated. This includes the questions of what, where and how exactly it should be? Ideally, since sensory feedback closes the loop from the user’s action to the SE’s reaction, its placement and modality should parallel the actuation and usage of the SE. The level of knowledge given by inherent feedback also needs further investigation to identify when and in which cases additional feedback modules are best suited.
Both multitasking and the exploitation of sensory feedback may improve with increased user experience. If learning to control sDoFs corresponds to skill learning, what can be achieved will also depend on the amount of training time required, e.g., months or years of training may be necessary for good performance as in sports. However, such extended training periods may not be available or desirable for all applications. Systematic research is therefore required to develop and optimize learning paradigms for the acquisition of skilled SE control.
Augmentation by extension
The major current limiting factor in augmentation by extension lies with determining where the resources for controlling the sDoFs could come from. Two fundamental questions need to be addressed in this regard: (i) do users have sufficient independent physiological control signals? and (ii) can such signals be reliably and robustly sourced? Given the high degree of redundancy present from the neural to kinematic levels of the musculoskeletal system, we believe that in principle, the nervous system is able to learn to generate signals that can be modulated independently from movement. However, this is currently unknown, and even if the brain can generate such a signal, its reliability and dimensionality may limit the functionality of augmentation by extension.
Motor unit activities may offer a noninvasive and portable solution to provide multidimensional signals to control an SE, however it remains to be shown they can be used for augmentation. Moreover, current decomposition algorithms extracting spiking activity from surface EMG recordings in isometric conditions need to be extended to movements in order to be used for many applications.
Muscular null space signals are another noninvasive and portable alternative signal type for augmentation with initial results focusing on the use of co-contraction showing promise52. However, co-contraction, which could be used by both motor units and muscle signals for augmentation, is also used by the nervous system to regulate the interaction with the environment through impedance control116. Hence, it is important to examine whether alternative redundant muscle patterns exists that can be used to control supernumerary DoFs.
While many of these issues may be overcome in the future, the same issues on multitasking, sensory feedback, and learning as described in the previous section for augmentation by transfer need to be considered for augmentation by extension. To maximize the performance of augmented movement, future research should thus determine and document the limits of human capability and user-specific algorithms to translate physiological control signals into augmented movement. Similarly, greater understanding of learning and plasticity specifically associated with DoF augmentation is needed since most current research can only be speculatively extended to DoF augmentation. There will likely be hard limits to the complexity and number of tasks the brain can perform simultaneously, thus restricting the functional capabilities that can be achieved with augmentation by transfer and extension.
Ethical aspects
The augmentation of human movement abilities raises important ethical questions. This includes potential concerns that movement augmentation technology may negatively affect natural motor function, change subjects’ body identity and image, reinforce inequalities or pose problems in responsibility assignment as the boundary between humans and technology becomes increasingly blurred117. As a result of these questions, and the potentially “unnatural” nature of the augmentation, users may reject their augmentation device as has been observed for prostheses118. The user’s acceptance of augmentation is an essential issue for which the determining factors have started to be studied119, although there are currently no established guidelines. We believe that these and further important ethical issues of movement augmentation must therefore be addressed in a multidisciplinary approach that combines neuroscience and technology with philosophical, legal, and safety aspects.
Experiments and applications
Common to all forms of augmentation is a need for greater understanding of the underlying computational and neural mechanisms. Progress in these basic aspects of movement augmentation will require extensive experiments with human subjects to analyze: (i) the coordination and learning behaviors, (ii) the subject’s evaluation on augmentation systems (e.g., on the aspects of comfort, sense of agency, utility, and on how their use modify actions experience), (iii) restorative devices for impaired individuals that will require patient-specific protocols.
Limitations in the precision and control capabilities of the SE’s movements and in the accuracy of user’s control signal, may limit the usability of augmentation in certain applications, such as in surgery requiring precise control. These system and human limitations should be considered to design new protocols specifically for multimanual operation.
Finally, virtual SEs e.g., on computers or mobile devices are yet unexplored and may offer new and interesting possibilities for future studies as applications in augmented and virtual reality become more common.
References
Tong, Y. & Liu, J. Review of research and development of supernumerary robotic limbs. IEEE/CAA J. Autom. Sin. 8, 929–952 (2021).
Yang, B., Huang, J., Chen, X., Xiong, C. & Hasegawa, Y. Supernumerary robotic limbs: a review and future outlook. IEEE Transact. Med. Robot. Bionics. 3, 623–639 (2021).
Prattichizzo, D. et al. Human augmentation by wearable supernumerary robotic limbs: review and perspectives. Prog. Biomed. Eng. 3, 042005 (2021).
Mehring, C. et al. Augmented manipulation ability in humans with six-fingered hands. Nat. Commun. 10, 1–9 (2019).
Dollar, A. M. & Herr, H. Lower extremity exoskeletons and active orthoses: challenges and state-of-the-art. IEEE Trans. Robot. 24, 144–158 (2008).
Zhang, J. et al. Human-in-the-loop optimization of exoskeleton assistance during walking. Science 356, 1280–1284 (2017).
De Looze, M. P., Bosch, T., Krause, F., Stadler, K. S. & O’Sullivan, L. W. Exoskeletons for industrial application and their potential effects on physical work load. Ergonomics 59, 671–681 (2016).
Sung, G. T. & Gill, I. S. Robotic laparoscopic surgery: a comparison of the Da Vinci and Zeus systems. Urology 58, 893–898 (2001).
Gu, Y.-L. & Xu, Y. A normal form augmentation approach to adaptive control of space robot systems. Dyn. Control 5, 275–294 (1995).
Ballantyne, G. H. & Moll, F. The Da Vinci telerobotic surgical system: the virtual operative field and telepresence surgery. Surgical Clin. North Am. 83, 1293–1304 (2003).
Riviere, C. N., Ang, W. T. & Khosla, P. K. Toward active tremor canceling in handheld microsurgical instruments. IEEE Trans. Robot. Autom. 19, 793–800 (2003).
Stelarc. Writing one word with three hands simultaneously. http://stelarc.org/?catID=20265 (1982).
Guterstam, A., Petkova, V. I. & Ehrsson, H. H. The illusion of owning a third arm. PLoS ONE 6, e17208 (2011).
Davenport, C., Parietti, F. & Asada, H. H. Design and biomechanical analysis of supernumerary robotic limbs. In Dynamic Systems and Control Conference, Vol. 45295, 787–793 (ASME, Fort Lauderdale, Florida, USA, 2012).
Kaufman, M. T., Churchland, M. M., Ryu, S. I. & Shenoy, K. V. Cortical activity in the null space: permitting preparation without movement. Nat. Neurosci. 17, 440–448 (2014).
Law, A. J., Rivlis, G. & Schieber, M. H. Rapid acquisition of novel interface control by small ensembles of arbitrarily selected primary motor cortex neurons. J. Neurophysiol. 112, 1528–1548 (2014).
Dominijanni, G. et al. The neural resource allocation problem when enhancing human bodies with extra robotic limbs. Nat. Mach. Intell. 3, 850–860 (2021).
Llorens-Bonilla, B. & Asada, H. H. A robot on the shoulder: Coordinated human-wearable robot control using coloured Petri nets and partial least squares predictions. In IEEE International Conference on Robotics and Automation, 119–125 (IEEE, Hong Kong, China, 2014).
Parietti, F. & Asada, H. H. Supernumerary robotic limbs for aircraft fuselage assembly: body stabilization and guidance by bracing. In IEEE International Conference on Robotics and Automation, 1176–1183 (IEEE, Hong Kong, China, 2014).
Parietti, F. & Asada, H. H. Independent, voluntary control of extra robotic limbs. In IEEE International Conference on Robotics and Automation, (ed. Okamura, A.) 5954–5961 (IEEE, Singapore, 2017).
Sasaki, T., Saraiji, M. Y., Fernando, C. L., Minamizawa, K. & Inami, M. Metalimbs: multiple arms interaction metamorphism. In ACM SIGGRAPH Emerging Technologies, 1–2 (ACM, Los Angeles, California, USA, 2017).
Vatsal, V. & Hoffman, G. Design and analysis of a wearable robotic forearm. In IEEE International Conference on Robotics and Automation, (ed. Lynch, K.) 5489–5496 (IEEE, Brisbane, Queensland, Australia, 2018).
Nguyen, P. H., Sparks, C., Nuthi, S. G., Vale, N. M. & Polygerinos, P. Soft poly-limbs: toward a new paradigm of mobile manipulation for daily living tasks. Soft Robot. 6, 38–53 (2019).
Véronneau, C. et al. Multifunctional remotely actuated 3-dof supernumerary robotic arm based on magnetorheological clutches and hydrostatic transmission lines. IEEE Robot. Autom. Lett. 5, 2546–2553 (2020).
Amanhoud, W., Hernandez Sanchez, J., Bouri, M. & Billard, A. Contact-initiated shared control strategies for four-arm supernumerary manipulation with foot interfaces. Int. J. Robot. Res. 40, 986–1014 (2021).
Wu, F. & Asada, H. Supernumerary robotic fingers: an alternative upper-limb prosthesis. In Dynamic Systems and Control Conference, Vol. 46193, V002T16A009 (ASME, San Antonio, Texas, USA, 2014).
Prattichizzo, D., Malvezzi, M., Hussain, I. & Salvietti, G. The sixth-finger: a modular extra-finger to enhance human hand capabilities. In The IEEE International Symposium on Robot and Human Interactive Communication, 993–998 (IEEE, Edinburgh, Scotland, UK, 2014).
Hussain, I. et al. A soft supernumerary robotic finger and mobile arm support for grasping compensation and hemiparetic upper limb rehabilitation. Robot. Autonomous Syst. 93, 1–12 (2017).
Cunningham, J., Hapsari, A., Guilleminot, P., Shafti, A. & Faisal, A. A. The supernumerary robotic 3rd thumb for skilled music tasks. In IEEE International Conference on Biomedical Robotics and Biomechatronics, 665–670 (IEEE, Enschede, Netherlands, 2018).
Clode, D. The third thumb. https://www.daniclodedesign.com/thethirdthumb (2018).
Malvezzi, M. et al. Design of multiple wearable robotic extra fingers for human hand augmentation. Robotics 8, 102 (2019).
Parietti, F., Chan, K. C., Hunter, B. & Asada, H. H. Design and control of supernumerary robotic limbs for balance augmentation. In IEEE International Conference on Robotics and Automation, 5010–5017 (IEEE, Seattle, Washington, USA, 2015).
Treers, L. et al. Design and control of lightweight supernumerary robotic limbs for sitting/standing assistance. In International Symposium on Experimental Robotics, (eds Kulić, D., Nakamura, Y., Khatib, O. & Venture, G.) 299–308 (Springer, Nagasaki, Japan, 2016).
Kurek, D. A. & Asada, H. H. The mantisbot: Design and impedance control of supernumerary robotic limbs for near-ground work. In IEEE International Conference on Robotics and Automation, (ed. Okamura, A.) 5942–5947 (IEEE, Singapore, 2017).
Khazoom, C., Caillouette, P., Girard, A. & Plante, J.-S. A supernumerary robotic leg powered by magnetorheological actuators to assist human locomotion. IEEE Robot. Autom. Lett. 5, 5143–5150 (2020).
Hao, M., Zhang, J., Chen, K., Asada, H. & Fu, C. Supernumerary robotic limbs to assist human walking with load carriage. J. Mechanisms Robotics 12, 6 (2020).
Seo, W., Shin, C.-Y., Choi, J., Hong, D. & Han, C. S. Applications of supernumerary robotic limbs to construction works: case studies. In International Symposium on Automation and Robotics in Construction, Vol. 33, 1 (IAARC Publications, Auburn, Alambama, USA, 2016).
Abdi, E., Bouri, M., Himidan, S., Burdet, E. & Bleuler, H. Third arm manipulation for surgical applications: an experimental study. In New Trends in Medical and Service Robots, (eds Bleuler, H. et al.) 153–163 (Springer, 2016).
Hussain, I., Spagnoletti, G., Salvietti, G. & Prattichizzo, D. Toward wearable supernumerary robotic fingers to compensate missing grasping abilities in hemiparetic upper limb. Int. J. Robot. Res. 36, 1414–1436 (2017).
Abdi, E., Burdet, E., Bouri, M., Himidan, S. & Bleuler, H. In a demanding task, three-handed manipulation is preferred to two-handed manipulation. Sci. Rep. 6, 1–11 (2016).
Bashford, L. et al. Concurrent control of a brain–computer interface and natural overt movements. J. Neural Eng. 15, 066021 (2018).
Huang, Y., Eden, J., Cao, L., Burdet, E. & Phee, S. J. Tri-manipulation: an evaluation of human performance in 3-handed teleoperation. IEEE Trans. Med. Robot. Bionics 2, 545–548 (2020).
Bräcklein, M., Ibanez, J., Barsakcioglu, D. Y. & Farina, D. Towards human motor augmentation by voluntary decoupling beta activity in the neural drive to muscle and force production. J. Neural Eng. 18, 016001 (2021).
Sasaki, T., Saraiji, M. Y., Minamizawa, K., Kitazaki, M. & Inami, M. Changing body ownership using visual metamorphosis. In Virtual Reality International Conference, 1–2 (ACM, Laval, France, 2016).
Hoyet, L., Argelaguet, F., Nicole, C. & Lécuyer, A. "wow! i have six fingers!": would you accept structural changes of your hand in VR? Front. Robot. AI. 3, 27 (2016).
Cadete, D. & Longo, M. R. A continuous illusion of having a sixth finger. Perception 49, 807–821 (2020).
Wu, F. Y. & Asada, H. Bio-artificial synergies for grasp posture control of supernumerary robotic fingers. In Robotics, Sci. Syst. (MIT Press, Berkeley, California, USA, 2014).
Parietti, F., Chan, K. & Asada, H. H. Bracing the human body with supernumerary robotic limbs for physical assistance and load reduction. In IEEE International Conference on Robotics and Automation, 141–148 (IEEE, Hong Kong, China, 2014).
Wu, F. Y. & Asada, H. H. Implicit and intuitive grasp posture control for wearable robotic fingers: a data-driven method using partial least squares. IEEE Trans. Robot. 32, 176–186 (2016).
Setiawan, J. D. et al. Grasp posture control of wearable extra robotic fingers with flex sensors based on neural network. Electronics 9, 905 (2020).
Khoramshahi, M., Morel, G. & Jarrassé, N. Intent-aware control in kinematically redundant systems: towards collaborative wearable robots. In IEEE International Conference on Robotics and Automation (IEEE, Xi’an, China, 2021).
Guggenheim, J., Hoffman, R., Song, H. & Asada, H. H. Leveraging the human operator in the design and control of supernumerary robotic limbs. IEEE Robot. Autom. Lett. 5, 2177–2184 (2020).
Song, H. & Asada, H. H. Integrated voluntary-reactive control of a human-superlimb hybrid system for hemiplegic patient support. IEEE Robot. Autom. Lett. 6, 1646–1653 (2021).
Kurtzer, I. L., Pruszynski, J. A. & Scott, S. H. Long-latency reflexes of the human arm reflect an internal model of limb dynamics. Curr. Biol. 18, 449–453 (2008).
Asai, Y. et al. A model of postural control in quiet standing: robust compensation of delay-induced instability using intermittent activation of feedback control. PLoS ONE 4, e6169 (2009).
Guggenheim, J. W., Parietti, F., Flash, T. & Asada, H. H. Laying the groundwork for intra-robotic-natural limb coordination: Is fully manual control viable? ACM Trans. Hum.-Robot Interact. 9, 1–12 (2020).
Abdi, E., Burdet, E., Bouri, M. & Bleuler, H. Control of a supernumerary robotic hand by foot: an experimental study in virtual reality. PLoS ONE 10, e0134501 (2015).
Huang, Y. et al. A subject-specific four-degree-of-freedom foot interface to control a surgical robot. IEEE/ASME Trans. Mechatron. 25, 951–963 (2020).
Hussain, I., Spagnoletti, G., Salvietti, G. & Prattichizzo, D. An EMG interface for the control of motion and compliance of a supernumerary robotic finger. Front. Neurorobotics 10, 18 (2016).
Leigh, S. W. & Maes, P. Body integrated programmable joints interface. In Conference on Human Factors in Computing Systems, 6053–6057 (ACM, San Jose, California, USA, 2016).
Srinivas, S., Virk, G. S. & Haider, U. Multipurpose supernumerary robotic limbs for industrial and domestic applications. In International Conference on Methods and Models in Automation and Robotics, 289–293 (IEEEE, Miedzyzdroje, Poland, 2015).
Huang, Y. et al. A three-limb teleoperated robotic system with foot control for flexible endoscopic surgery. Annals Biomed. Eng. 49, 2282–2296 (2021).
Dougherty, Z. & Winck, R. C. Evaluating the performance of foot control of a supernumerary robotic limb. In Dynamic Systems and Control Conference, Vol. 59162, V003T16A003 (ASME, Park City, Utah, USA, 2019).
Kieliba, P., Clode, D., Maimon-Mor, R. O. & Makin, T. R. Robotic hand augmentation drives changes in neural body representation. Sci. Robot. 6, eabd7935 (2021).
Koike, U. et al. Development of an intraoral interface for human-ability extension robots. J. Robot. Mechatron. 28, 819–829 (2016).
Wu, F. Y. & Asada, H. H. “hold-and-manipulate” with a single hand being assisted by wearable extra fingers. In IEEE International Conference on Robotics and Automation, 6205–6212 (IEEE, Seattle, Washington, USA, 2015).
Meraz, N. S., Shikida, H. & Hasegawa, Y. Auricularis muscles based control interface for robotic extra thumb. In IEEE International Symposium on Micro-NanoMechatronics and Human Science, 1–3 (IEEE, Nagoya, Japan, 2017).
Baldi, T. L. et al. Exploiting implicit kinematic kernel for controlling a wearable robotic extra-finger. Preprint at https://arxiv.org/abs/2012.03600 (2020).
Fukuoka, M. et al. Facedrive: facial expression driven operation to control virtual supernumerary robotic arms. In SIGGRAPH Asia, 9–10 (ACM, Brisbane, Queensland, Australia, 2019).
Maimon-Mor, R. O. et al. Towards free 3D end-point control for robotic-assisted human reaching using binocular eye tracking. In IEEE International Conference on Rehabilitation Robotics, (eds Amirabdollahian, F., Burdet, E. & Masia, L.) 1049–1054 (IEEE, London, England, UK, 2017).
Di Pino, G., Maravita, A., Zollo, L., Guglielmelli, E. & Di Lazzaro, V. Augmentation-related brain plasticity. Front. Syst. Neurosci. 8, 109 (2014).
Gurgone, S. et al. Muscular null space control for human motor augmentation. Simultaneous control of natural and extra degrees of freedom by isometric force and electromyographic activity in the muscle-to-force null space. J Neural Eng. 19, https://doi.org/10.1088/1741-2552/ac47db (2022).
Orsborn, A. L. et al. Closed-loop decoder adaptation shapes neural plasticity for skillful neuroprosthetic control. Neuron 82, 1380–1393 (2014).
Milovanovic, I., Robinson, R., Fetz, E. E. & Moritz, C. T. Simultaneous and independent control of a brain-computer interface and contralateral limb movement. Brain-Computer Interfaces 2, 174–185 (2015).
Cheung, W., Sarma, D., Scherer, R. & Rao, R. P. Simultaneous brain-computer interfacing and motor control: expanding the reach of non-invasive BCIs. In International Conference of the IEEE Engineering in Medicine and Biology Society, (ed. Lovell, N.) 6715–6718 (IEEE, San Diego, California, USA, 2012).
Leeb, R., Lancelle, M., Kaiser, V., Fellner, D. W. & Pfurtscheller, G. Thinking penguin: multimodal brain–computer interface control of a VR game. IEEE Trans. Computational Intell. AI Games 5, 117–128 (2013).
Penaloza, C. I. & Nishio, S. BMI control of a third arm for multitasking. Sci. Robot. 3, eaat1228 (2018).
Burdet, E. & Mehring, C. e-letter to Penaloza and Nishio “BMI control of a third arm for multitasking’. Sci. Robot. 3 (2018).
Barsakcioglu, D. Y., Bräcklein, M., Holobar, A. & Farina, D. Control of spinal motoneurons by feedback from a non-invasive real-time interface. IEEE Transac. Biomed. Eng. 68, 926–935 (2020).
Formento, E., Botros, P. & Carmena, J. Skilled independent control of individual motor units via a non-invasive neuromuscular-machine interface. J. Neural Eng. 18, 066019 (2021).
Marshall, N. J. et al. Flexible neural control of motor units. Preprint at https://www.biorxiv.org/content/10.1101/2021.05.05.442653v1 (2021).
Bräcklein, M. et al. The control and training of single motor units in isometric tasks are constrained by a common synaptic input signal. Preprint at https://www.biorxiv.org/content/10.1101/2021.08.03.454908v1 (2021).
Farina, D., Negro, F., Muceli, S. & Enoka, R. M. Principles of motor unit physiology evolve with advances in technology. Physiology 31, 83–94 (2016).
Zollo, L. et al. Restoring tactile sensations via neural interfaces for real-time force-and-slippage closed-loop control of bionic hands. Sci. Robot. 4, eaau9924 (2019).
Pynn, L. K. & DeSouza, J. F. The function of efference copy signals: implications for symptoms of schizophrenia. Vis. Res. 76, 124–133 (2013).
Miller, L. E. et al. Sensing with tools extends somatosensory processing beyond the body. Nature 561, 239–242 (2018).
Franklin, D. W. et al. CNS learns stable, accurate, and efficient movements using a simple algorithm. J. Neurosci. 28, 11165–11173 (2008).
Takagi, A., Ganesh, G., Yoshioka, T., Kawato, M. & Burdet, E. Physically interacting individuals estimate the partner’s goal to enhance their movements. Nat. Hum. Behav. 1, 1–6 (2017).
Dadarlat, M. C., O’doherty, J. E. & Sabes, P. N. A learning-based approach to artificial sensory feedback leads to optimal integration. Nat. Neurosci. 18, 138–144 (2015).
Alva, P. G. S., Muceli, S., Atashzar, S. F., William, L. & Farina, D. Wearable multichannel haptic device for encoding proprioception in the upper limb. J. Neural Eng. 17, 056035 (2020).
Noccaro, A., Raiano, L., Pinardi, M., Formica, D. & Di Pino, G. A novel proprioceptive feedback system for supernumerary robotic limb. In IEEE RAS/EMBS International Conference for Biomedical Robotics and Biomechatronics, 1024–1029 (IEEE, New York, New York, USA, 2020).
D’Alonzo, M., Dosen, S., Cipriani, C. & Farina, D. HyVE: hybrid vibro-electrotactile stimulation for sensory feedback and substitution in rehabilitation. IEEE Trans. Neural Syst. Rehabilitation Eng. 22, 290–301 (2013).
Wang, W. et al. Building multi-modal sensory feedback pathways for SRL with the aim of sensory enhancement via BCI. In IEEE International Conference on Robotics and Biomimetics, 2439–2444 (IEEE, Dali, China, 2019).
Wheeler, J., Bark, K., Savall, J. & Cutkosky, M. Investigation of rotational skin stretch for proprioceptive feedback with application to myoelectric systems. IEEE Trans. Neural Syst. Rehabilitation Eng. 18, 58–66 (2010).
Akhtar, A. et al. Passive mechanical skin stretch for multiple degree-of-freedom proprioception in a hand prosthesis. In International Conference on Human Haptic Sensing and Touch Enabled Computer Applications, (eds Auvray, M. & Duriez, C.) 120–128 (Springer, Versailles, France, 2014).
Hussain, I., Meli, L., Pacchierotti, C., Salvietti, G. & Prattichizzo, D. Vibrotactile haptic feedback for intuitive control of robotic extra fingers. In IEEE WorldHaptics, 394–399 (IEEE, Chicago, Illinois, USA, 2015).
Hussain, I. et al. Using the robotic sixth finger and vibrotactile feedback for grasp compensation in chronic stroke patients. In IEEE International Conference on Rehabilitation Robotics, 67–72 (IEEE, Singapore, 2015).
Oddo, C. M. et al. Intraneural stimulation elicits discrimination of textural features by artificial fingertip in intact and amputee humans. eLife 5, e09148 (2016).
Chandrasekaran, S. et al. Sensory restoration by epidural stimulation of the lateral spinal cord in upper-limb amputees. eLife 9, e54349 (2020).
Mazzoni, P. & Krakauer, J. W. An implicit plan overrides an explicit strategy during visuomotor adaptation. J. Neurosci. 26, 3642–3645 (2006).
Conditt, M. A., Gandolfo, F. & Mussa-Ivaldi, F. A. The motor system does not learn the dynamics of the arm by rote memorization of past experience. J. Neurophysiol. 78, 554–560 (1997).
Fetz, E. E. Operant conditioning of cortical unit activity. Science 163, 955–958 (1969).
Moritz, C. T., Perlmutter, S. I. & Fetz, E. E. Direct control of paralysed muscles by cortical neurons. Nature 456, 639–642 (2008).
Fetz, E. E. & Finocchio, D. V. Operant conditioning of specific patterns of neural and muscular activity. Science 174, 431–435 (1971).
Fetz, E. E. & Baker, M. A. Operantly conditioned patterns on precentral unit activity and correlated responses in adjacent cells and contralateral muscles. J. Neurophysiol. 36, 179–204 (1973).
Sadtler, P. T. et al. Neural constraints on learning. Nature 512, 423–426 (2014).
Oby, E. R. et al. New neural activity patterns emerge with long-term learning. Proc. Natl Acad. Sci. USA 116, 15210–15215 (2019).
Ogawa, K., Mitsui, K., Imai, F. & Nishida, S. Long-term training-dependent representation of individual finger movements in the primary motor cortex. Neuroimage 202, 116051 (2019).
Rossi, S. et al. Emerging of new bioartificial corticospinal motor synergies using a robotic additional thumb. Sci. Rep. 11, 1–11 (2021).
Maguire, E. A., Woollett, K. & Spiers, H. J. London taxi drivers and bus drivers: a structural MRI and neuropsychological analysis. Hippocampus 16, 1091–1101 (2006).
Townsend, J. T. & Eidels, A. Workload capacity spaces: a unified methodology for response time measures of efficiency as workload is varied. Psychonomic Bull. Rev. 18, 659–681 (2011).
Noccaro, A., Eden, J., Di Pino, G., Formica, D. & Burdet, E. Human performance in three-hands tasks. Sci. Rep. 11, 1–8 (2021).
Huang, Y., Eden, J., Ivanova, E., Phee, S. J. & Burdet, E. Trimanipulation: evaluation of human performance in a 3-handed coordination task. In IEEE International Conference on Systems, Man, and Cybernetics, 882–887 (IEEE, 2021).
Jarrassé, N., Charalambous, T. & Burdet, E. A framework to describe, analyze and generate interactive motor behaviors. PLoS ONE 7, e49945 (2012).
Li, Y., Carboni, G., Gonzalez, F., Campolo, D. & Burdet, E. Differential game theory for versatile physical human–robot interaction. Nat. Mach. Intell. 1, 36–43 (2019).
Franklin, D. W. et al. Endpoint stiffness of the arm is directionally tuned to instability in the environment. J. Neurosci. 27, 7705–7716 (2007).
Blanke, O. & Aspell, J. E. Brain technologies raise unprecedented ethical challenges. Nature 458, 703–703 (2009).
Biddiss, E. & Chau, T. Upper-limb prosthetics: critical factors in device abandonment. Am. J. Phys. Med. Rehabilitation 86, 977–987 (2007).
Meyer, J. T., Gassert, R. & Lambercy, O. An analysis of usability evaluation practices and contexts of use in wearable robotics. J. NeuroEng. Rehabilitation 18, 1–15 (2021).
Nima project—Sorbonne arm. https://nima-project.eu (2022).
Acknowledgements
This research was supported in part by the European Commission grants H2020 NIMA (FETOPEN 899626), TRIMANUAL (MSCA 843408), the UK EPSRC Centre for Doctoral Training in Neurotechnology and Health, the Italian Ministry of Education, University and Research grant ENABLE (FARE R16ZBLF9E3), and from la Caixa Foundation (ID 100010434, fellowship code LCF/BQ/PI21/11830018).
Author information
Authors and Affiliations
Contributions
The concepts and taxonomy were developed by J.E., M.B., J.I., D.Y.B., D.F., E.B., C.M. The paper was prepared by J.E., M.B., G.d.P., E.B., C.M. It was revised by all authors.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Peer review
Peer review information
Nature Communications thanks H. Harry Asada, Gionata Salvietti and the other, anonymous, reviewer(s) for their contribution to the peer review of this work.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Eden, J., Bräcklein, M., Ibáñez, J. et al. Principles of human movement augmentation and the challenges in making it a reality. Nat Commun 13, 1345 (2022). https://doi.org/10.1038/s41467-022-28725-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41467-022-28725-7
This article is cited by
-
Impact of supplementary sensory feedback on the control and embodiment in human movement augmentation
Communications Engineering (2023)
-
Wearable Extra Robotic Limbs: A Systematic Review of Current Progress and Future Prospects
Journal of Intelligent & Robotic Systems (2023)
-
Congruence-based contextual plausibility modulates cortical activity during vibrotactile perception in virtual multisensory environments
Communications Biology (2022)
-
Knowing the intention behind limb movements of a partner increases embodiment towards the limb of joint avatar
Scientific Reports (2022)
-
The Ethics of Supernumerary Robotic Limbs. An Enactivist Approach
Science and Engineering Ethics (2022)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
