
Abstract
As we mark 150 years since the birth of Marie Curie, we reflect on the global advances made in radiation oncology and the current status of radiation therapy (RT) research. Large-scale international RT clinical trials have been fundamental in driving evidence-based change and have served to improve cancer management and to reduce side effects. Radiation therapy trials have also improved practice by increasing quality assurance and consistency in treatment protocols across multiple centres. This review summarises some of the key RT practice-changing clinical trials over the last two decades, in four common cancer sites for which RT is a crucial component of curative treatment: breast, lung, urological and lower gastro-intestinal cancer. We highlight the global inequality in access to RT, and the work of international organisations, such as the International Atomic Energy Agency (IAEA), the European SocieTy for Radiotherapy and Oncology (ESTRO), and the United Kingdom National Cancer Research Institute Clinical and Translational Radiotherapy Research Working Group (CTRad), that aim to improve access to RT and facilitate radiation research. We discuss some emerging RT technologies including proton beam therapy and magnetic resonance linear accelerators and predict likely future directions in clinical RT research.
Similar content being viewed by others


Introduction
Born Maria Salomea Skłodowska on 7 November 1867 in Warsaw, Poland, Marie Curie later went on to discover both polonium and radium, and won two Nobel prizes for her work on radioactive substances. Later, during the First World War, she set up a fleet of mobile X-ray units, popularly called ‘the little Curies’, to enable military doctors to locate and remove shrapnel from soldiers’ wounds at the front line. After the war, she was instrumental in founding the Institut du Radium in Paris, which later became part of the Institut Curie, now a world-leading oncology research centre. To mark the 150th anniversary of her birth, we reflect on the global advances made in radiation oncology, focussing on radiation therapy (RT) practice-changing trials over the last two decades. In addition, we discuss global inequalities in access to RT and highlight possible future directions of clinical RT research.
RT is a crucial and cost-effective cancer treatment
Systemic therapy may mistakenly be considered the mainstay of curative oncological treatment, perhaps due to its high profile in the media. In fact, 40% of patients who are cured of cancer will receive RT as part of their management, and around 50% of cancer patients will require RT at some point during their treatment in high as well as low and middle-income countries.1,2,3,4 Despite representing a large proportion of cancer treatment, RT accounts for only 5% of the national cancer budget in both the UK and Sweden.3,5 By contrast, the European Union average proportion of total oncology expenditure spent on cancer drugs has increased from 12% in 2005 to 23% in 2014.6 In addition to its curative potential, RT also has a key role in the palliation of symptoms including pain, bleeding and nerve compression, as well as in curative intent treatments.
RT comprises multiple different treatment modalities, including external beam therapy (encompassing photons, electrons, protons and other particles) and internal/surface treatment (brachytherapy and radiopharmaceuticals). The most widely used modality is megavoltage photon therapy, which is a form of high-energy electromagnetic radiation produced by a linear accelerator. Megavoltage photons have a range of tissue penetration, which allows treatment of deeper internal body structures, such as pelvic organs and lung tumours. Other forms of external beam therapy are orthovoltage photons, which have shallower tissue penetration and are useful for treating skin and soft tissue; and electrons, which also have a short range of tissue penetration but a different dose distribution to orthovoltage photons, and are used mainly for treating skin and superficial tumours. Proton beam therapy is an emerging form of external beam therapy, which has a peak of dose deposition at a sharply defined point (the ‘Bragg peak’) and as such has potential for a much lower dose to nearby critical organs. Internal RT uses very short-range radiation from radioactive sources delivered inside the body. This can be solid sources placed during a surgical procedure or on the body surface, as in brachytherapy for prostate or cervical cancer. Alternatively, unsealed sources may be used, for example radiopharmaceutical injections, which are preferentially taken up by cancer tissues.
RT has dramatically improved both technologically and in terms of clinical outcomes; less than two decades ago, RT was mostly given as simple ‘fields’, which are square/rectangular beams, with minimal imaging guidance. Now, it is increasingly common to deliver highly targeted image-guided treatment with intensity modulated RT (IMRT). This enables dose reduction to the surrounding normal structures, thereby minimising toxicity, and facilitates dose escalation to the tumour, thereby maximising cancer control.7,8 Another new technique is stereotactic body RT (SBRT), which allows the administration of very high doses of precision radiation in a small number of treatments (fractions).9 This is currently used for some primary lung and brain tumours, but also raises the tantalising question of whether patients with a limited number of metastases (‘oligometastatic disease’) could also be cured using this new technology, in combination with systemic therapy. Finally, the mechanistic understanding of how RT interacts with cancerous and normal tissue at a cellular and molecular level is moving at a rapid pace; as a result, exciting opportunities are now arising for investigating RT in combination with novel drugs, such as immunotherapy and DNA damage response inhibitors10,11 (Fig. 1).

RT has great potential to be combined with multiple classes of novel drugs. Reprinted from Nature Reviews Clinical Oncology.11
RT practice has historically varied greatly across international and national institutions, and even within individual centres. Over recent years, a growing focus on evidence-based medicine has led to an increasing number of RT clinical trials that aim to improve patient outcomes by improving overall survival and local tumour control, and/or reducing (often permanent) side effects. Secondary but important benefits of these practice-changing clinical trials include improvements in RT quality and consistency across multiple centres. This manuscript aims to highlight to a non-specialist audience the results from a number of key clinical trials in RT research. An international range of expert authors selected trials for inclusion that have changed clinical practice by influencing national or international guidelines. Selected trials were published in the last 20 years in four common cancer types where RT is a key component of curative intent treatment: breast, lung, urological and lower gastrointestinal. The majority of the included trials were large randomised phase 3 trials. Explanation of some technical terms is included in Box 1 to assist the non-specialist reader.
The collective effect of these clinical trials is that much of the treatment of patients with RT is now based on prospective clinical trial data of efficacy and toxicity rather than historical and empirical practice. There remains, however, considerable progress to be made in further improving outcomes for patients, by ensuring that existing clinical trial evidence is translated into global clinical practice, and by instigating further research into novel technologies and drug–RT combinations.
Breast RT practice-changing trials
The Early Breast Cancer Trialists’ Collaborative group has clearly demonstrated, through their individual patient-data meta-analyses from randomised clinical trials (RCTs), that RT improves local control and survival following breast-conserving surgery, or following mastectomy for node-positive tumours.12,13 The RCTs included in this meta-analysis generally span several decades, with the earliest commencing in 1964 and all trials starting before 2000. More recent practice-changing trials (Table 1) have investigated the use of fewer treatments (hypofractionation), the role of tumour bed boost, partial breast irradiation, and nodal irradiation.
Hypofractionation, boost and partial breast RT
Evidence from more than 7000 women treated and followed up for 10 years within the UK START and Canadian RCTs demonstrated that shorter, hypofractionated courses of RT are non-inferior to 5 weeks of ‘conventionally’ fractionated therapy (25 fractions) for local tumour control. Furthermore, these hypofractionated treatments cause not more (Canadian fractionation schedule: 16 fractions of 2.66 Gy) or even fewer (UK fractionation schedule: 15 fractions of 2.67 Gy) late side effects14,15,16 than the conventional regimens. This confers important benefits, since late RT toxicity tends to be permanent.17 In addition, fewer RT visits are more convenient for patients and more cost-effective for healthcare providers.18,19,20 These results led to hypofractionation being adopted within international guidelines from the American Society for Radiation Oncology (ASTRO) and the UK National Institute for Health and Care Excellence (NICE).21,22 While hypofractionation is now standard practice in the UK and widely adopted in Canada, uptake in the United States and Europe is patchy, despite the convincing evidence. This is perceived to be a consequence of professional and societal barriers to optimal care, together with variations in treatment economics across different healthcare systems and specifically reimbursement, which is still calculated per fraction in many countries.23,24
The EORTC 22881-10882 study randomised patients to receive either a boost dose to the tumour bed following whole-breast irradiation, or whole-breast irradiation alone. This trial showed improved local control in patients receiving the boost, although this was at the cost of increased late side effects.25,26 After long-term updates, which confirmed the results and enabled better subgroup analyses, this trial led to international guidelines widely recommending a boost for patients ‘at high risk of recurrence’ following breast conserving surgery, but advising that the boost could be safely avoided for those at low/intermediate risk.21,22
The aim of partial irradiation is to focus RT on the region at highest risk of recurrence, to maintain high rates of local tumour control while minimising toxicity by virtue of a smaller irradiated volume. Very promising results were demonstrated by the Budapest and Florence partial breast RT trials, but the relatively small numbers in these studies have been insufficient to change practice internationally.27,28 Intra-operative partial breast RT has also been investigated and is potentially very attractive to patients if it means post-operative RT can be avoided. However, the ELIOT trial using intra-operative electrons failed to show non-inferiority with whole-breast RT; this may have been at least in part due to patient selection due to inclusion of patients with higher risk of recurrence.29 The TARGIT trial using photon intra-operative RT reported non-inferiority with whole-breast RT, but non-standard statistical analysis was used and median follow up was very short at only 2 years 5 months.30,31 Two large randomised partial breast RT trials have recently reported: IMPORT LOW and GEC-ESTRO.32,33 IMPORT LOW reported that partial breast RT, delivered over an identical 3-week period to the control group, yielded non-inferiority in local relapse rates while also reducing side effects. These results have been published too recently to be labelled ‘practice changing’; however, the study marked an important step in reducing late toxicity for a large population of low-risk patients. IMPORT LOW also used a simple RT technique leveraging existing radiotherapy equipment and standard RT techniques, with the only difference being the reduced treatment volume. The GEC-ESTRO trial, which used a brachytherapy approach for accelerated partial breast irradiation, confirmed non-inferiority with whole-breast RT. The results of four further phase 3 RCTs investigating partial breast RT using different techniques will be published in the next few years (NCT00103181, NCT00282035, NCT01247233, NCT01803958).
Nodal irradiation
Some breast cancer recurrences occur locoregionally and therefore the local management of local lymph node groups is an important consideration, especially in patients at higher risk of recurrence. The AMAROS trial randomised patients to either surgical dissection or axillary node RT, following positive sentinel lymph node biopsy, and reported reduced rates of lymphoedema in the RT arm with comparable loco-regional tumour control rates. This important study provides patients with more options after a positive sentinel lymph node biopsy, and has led to a dramatic fall in axillary surgery in many centres.34 More recently, there has been increasing interest in the addition of internal mammary chain (IMC) nodal irradiation to standard RT. Two large RCTs were published in 2015, both of which showed an improvement in disease-free survival with the addition of IMC irradiation.35,36 This was confirmed in a population-based Danish study where patients with right-sided breast cancer received IMC-RT, whereas left-sided patients did not and received normal standard of care at the time.37 These studies led to IMC irradiation being re-introduced in the 2016 ASCO post-mastectomy RT guidelines.38
Taken together, these practice-changing trials have facilitated ‘risk-adapted RT’, whereby breast RT approaches are offered based on the individual’s broad risk of recurrence. These range from partial breast RT in lower risk patients to IMC RT in high-risk patients in order to optimise local tumour control while minimising side effects. This demonstrates that RT for breast cancer is no longer a ‘one size fits all’ strategy, although we are still some way from delivering truly personalised breast RT. Further research is needed to: reliably identify which group of patients can avoid breast RT completely39; determine optimal timing of RT with mastectomy and reconstruction40; determine whether there is an advantage to deliver breast RT pre-operatively and how to best combine RT with novel drugs in higher risk patients.41
Lung RT practice-changing trials
In recent years we have seen many technological advances in the field of lung radiotherapy. These include the integration of 4-dimensional computed tomography (CT) and positron emission tomography (PET) for planning; the improved target conformality with the delivery of IMRT; SBRT; and the optimisation of image guidance (Table 2).
Early-stage non-small cell lung cancer
A key change in lung RT has been the introduction of SBRT for early-stage non-small cell lung cancers (NSCLC). This development came after multiple studies investigated this highly targeted and high-dose RT, which is delivered in just a few fractions. Treatment outcomes are comparable with surgery, especially for patients with medical co-morbidities.42,43,44,45,46,47,48,49,50,51 Evidence-based guidelines, mostly based on non-randomised phase II trials, distinguish patients who can be treated safely with SBRT from those at risk of excessive toxicity (especially those with centrally located tumours). Patients at higher risk of toxicity should be treated with a dose-adapted SBRT regimen, preferably within further clinical trials to allow collection of high-quality prospective toxicity data.52 Population-based studies have also demonstrated the effectiveness of this technique for improving overall survival in a non-selected elderly patient population.53,54
Locally advanced NSCLC
One of the main strategies for improving outcomes in patients with locally advanced NSCLC is dose escalation, which has shown encouraging results in phase I–II trials over the last two decades.55,56,57,58 However, the outcome of the phase III Radiation Therapy Oncology Group (RTOG) 0617 trial was surprisingly disappointing;59 dose escalation with concurrent chemoradiotherapy to 74 Gy in 37 fractions led to worse survival, compared with the standard of care (60 Gy in 30 fractions). The results of RTOG 0617 had a profound impact on usual clinical practice and future clinical trials, establishing 60 Gy in 30 fractions as the new benchmark for chemoradiotherapy in locally advanced NSCLC. Importantly, it also provided prospective evidence supporting IMRT for NSCLC, as a secondary analysis showed IMRT produced lower rates of severe pneumonitis and resulted in lower cardiac doses, compared with conventional RT.60
NSCLC and brain metastases
Avoidance of unnecessary treatment is important, especially for patients requiring palliation. The QUARTZ trial examined the role of whole-brain RT (WBRT) plus optimal supportive care in patients with NSCLC and brain metastases. The trial found no improvement in survival or quality adjusted life years with the addition of WBRT.61 As a result, WBRT is usually not recommended for the majority of patients; however, it may still be beneficial for some patients with better prognosis, such as those with driver mutations.
Small cell lung cancer
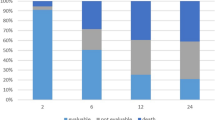
Very little progress was made for several decades in the systemic treatment of both limited- and extensive-stage small cell lung cancer (SCLC). Recently, advances in RT techniques, use of prophylactic cranial irradiation for all stages of SCLC, and improved combination of chemotherapy with RT have led to major improvements in survival. The current standard of care for patients with limited-stage SCLC is based on an RCT that compared once daily with twice-daily RT delivered concurrently with chemotherapy, which demonstrated superiority of twice-daily RT in terms of survival.62 However, since the publication of this study in 1999, there has been a lack of consensus regarding routine use of twice-daily RT, despite its superiority, due to logistical issues and concerns regarding toxicity (for example, one-third of the patients developed ≥grade 3 radiation oesophagitis). To help resolve this, the CONVERT trial compared twice-daily RT (45 Gy in 30 fractions) to a higher RT dose delivered once daily (66 Gy in 33 fractions), both given concurrently with chemotherapy.63 Overall survival outcomes did not differ between the two groups; however, the survival achieved in both groups was higher and toxicity much lower (>50% reduction) than previously reported.62 As this trial was designed to show superiority of once-daily RT and was not powered to show equivalence, the implication is that twice-daily RT should be considered the standard of care.
In the extensive-stage setting, an EORTC trial demonstrated that prophylactic cranial irradiation in patients who had responded to chemotherapy reduced the incidence of brain metastases and improved survival, compared with no subsequent treatment.64 Later, the CREST trial randomised extensive-stage SCLC patients to receive either thoracic RT (30 Gy in ten fractions) and prophylactic cranial irradiation, or to receive prophylactic cranial irradiation alone. Although there was no difference in overall survival at 1 year, a pre-planned analysis revealed a significant improvement in overall survival at 2 years, with a low rate of severe toxicities.65 Both of these trials were practice changing, and have led to new recommendations in international guidelines.66
The studies discussed have demonstrated significant survival improvements in both NSCLC and SCLC patients. Areas of unmet research need include the evaluation of modern RT technologies (such as SBRT and protons) in a wider population, and the development of individualised treatment strategies.
Urological RT practice-changing trials
Radiation-based therapy is used as an alternative to radical prostatectomy for localised disease, producing equivalent survival to surgery.67 It is also used as the key treatment modality for locally advanced disease. The development of RT as a curative treatment has been supported by technical refinement of RT, including treatment delivery with reduced toxicity, dose escalation and use of concomitant androgen deprivation therapy (ADT) (Table 3).
Localised prostate cancer
RCTs have led to a significant improvement in the evidence base supporting RT for localised prostate cancer over the last two decades. Prior to this, clinical practice was largely based on non-randomised studies. Recognition of the benefit for local control, even in high-risk/locally advanced patients, has been of key importance. The PR07 trial in locally advanced or ‘high risk’ localised node-negative prostate cancer provided evidence for a clear survival benefit of RT in addition to ADT, and similar results were reported by a Scandinavian trial.68,69 Non-randomised data from the STAMPEDE RCT also showed significantly improved survival with combined RT and ADT, compared with ADT alone, in patients with both high-risk and node-positive prostate cancer.70 Furthermore, several randomised dose-escalation studies have provided evidence to support an increased RT dose from 64–68 Gy to 74–78 Gy.71,72,73 These dose escalation trials showed improvements in biochemical progression-free survival, but not overall survival. The addition of RT to ADT, and use of a higher dose range 74–78 Gy, are now routine practice in the UK. Recent data suggest that additional benefit could be accrued through further dose escalation using a brachytherapy boost in high-risk patients, at the cost of increased toxicity.74
Based on the principle that prostate cancer may be more sensitive to increases in daily dose per fraction than previously thought, the CHHiP trial compared two hypofractionated regimens (60 Gy in 20 fractions vs. 57 Gy in 19 fractions) to the standard UK regimen at the time (74 Gy in 37 fractions), in men with T1b–T3aN0M0 prostate cancer. The 5-year results demonstrated that 60 Gy in 20 fractions was non-inferior to the standard regimen in terms of biochemical or clinical failure, and was associated with similar toxicity.75,76 As a result, this trial has already changed practice in the majority of UK centres.77,78 The RTOG 0415, HYPRO and PROFIT trials have also recently published data supporting the use of moderate hypofractionation; it seems likely that these trials together will lead to wider international use of hypofractionation in low-intermediate-risk prostate cancer.79,80,81
Metastatic prostate cancer
The most common metastatic site in prostate cancer is bone. Delivery of RT to multiple sites of bone disease can be achieved by using bone-seeking radiopharmaceuticals. Beta-emitting radioisotopes such as strontium-89 have been used in the palliation of bone pain for many years. More recently the alpha-emitting radioisotope radium-223, given as a course of 6-monthly injections, has been shown to be a key addition to the treatment options for men with castration-resistant prostate cancer with bone metastases. The ALSYMPCA trial clearly demonstrated an improvement in overall survival, quality of life scores, and time to first symptomatic skeletal-related event for radium-223, when compared with placebo.82,83 This treatment has been rapidly included in international guidelines and clinical practice, and provides another important addition to treatment options for men with castration-resistant prostate cancer.84,85
Muscle-invasive bladder cancer
RT has been used as an alternative bladder-preserving modality to radical cystectomy for muscle-invasive bladder cancer, but has been limited by the lower rate of complete response. To address this issue, over the last two decades the addition of either chemotherapy or radiation sensitisers to RT has been explored to improve local control. The evidence for these two treatment options has been has been provided by two randomised trials: the BC2001 trial showed an improvement in locoregional disease-free survival with the addition of 5-fluorouracil (5FU) and mitomycin C to RT,86 and the BCON trial showed improved overall survival with the addition of nicotinamide and carbogen (a gas mixture of 2% carbon dioxide and 98% oxygen).87 The low recurrence rates observed in these trials have led to growing acceptance that RT with concomitant chemotherapy or radiation sensitisers is a valid alternative to cystectomy for many patients, and led to NICE recommending that either RT or surgery should be offered to patients being treated with curative intent.88
Lower gastrointestinal RT practice-changing trials
Radical surgical resection is the cornerstone of treatment for localised rectal cancer; however, in the 1980s, radical surgery alone resulted in unacceptably high rates of local recurrence.89 Significant improvements in surgical techniques, such as total mesorectal excision (TME), resulted in lower local recurrence rates and led to a range of phase III trials that tested the additional benefit of pre-operative RT (Table 4).
Pre-operative RT in rectal cancer
Two phase III international trials demonstrated statistically significant reductions in local recurrence when 25 Gy in five fractions was given prior to TME, compared with TME alone.90,91 There was no difference in overall survival. These trials changed the standard of care for patients with resectable rectal cancer, with clinical adoption initially occurring in Northern Europe; however, this approach is now globally supported by international guidelines.92
Investigating a different strategy, four phase III trials established pre-operative concurrent chemoradiation as a standard of care for locally advanced rectal cancer. Two of these trials demonstrated that addition of concurrent 5FU and leucovorin to RT (45 Gy in 25 fractions) significantly reduced local recurrence, with no difference in overall survival.93,94 Two additional phase III trials demonstrated reduced local recurrence and toxicity when pre-operative chemoradiation was used, compared with post-operative chemoradiation95,96 and this approach is supported in both resectable and locally advanced rectal cancer. The use of pre-operative chemoradiation is now supported by international guidelines.97,98
With these two overlapping standards of care, two further phase III trials were performed that directly compared the two approaches.99,100 These trials reported no significant difference in local recurrence and survival, and as a result, both approaches are supported by international guidelines. Chemoradiation is recommended as the preferred option when the patient has locoregional disease with very close margins of surgical excision.
Anal cancer RT practice-changing trials
Three phase III trials performed in the 1980s resulted in a major change in clinical practice.101,102,103 Prior to this, radical surgery was performed that resulted in permanent colostomy. The trials determined concurrent mitomycin C, fluorouracil and RT as the standard of care, resulting in the avoidance of major surgery in the majority of patients. Subsequently the UK ACT2 trial introduced a continuous shrinking-field RT technique, using a lower total dose (50.4 Gy) where initial wide field irradiation was immediately followed by boost radiotherapy targeting areas of visible cancer. This approach was adopted into European practice and supported in European guidelines.104 Three phase III trials (ACT2, RTOG 9811 and ACCORD 03) demonstrated that additional chemotherapy either before or after concurrent chemoradiation did not improve cancer outcomes.105,106,107 Furthermore, in the RTOG 9811 trial, pre-operative and concurrent cisplatin-5FU led to higher colostomy rates and inferior disease-free survival rates. In addition, two small phase II trials had a significant effect on clinical practice. The UK EXTRA trial reported acceptable local control and toxicity using concurrent capecitabine rather than 5FU,108 and the use of concurrent capecitabine is now supported in international guidelines. The RTOG 0529 phase II trial109 reported an improvement in acute toxicity and acceptable outcomes with IMRT, compared with the RTOG 9811 trial, and IMRT is now widely used in anal cancer. It is clear that practice-changing and practice-defining clinical trials are feasible in this rare cancer.
There is substantial inequality in access to evidence-based RT
Clinical trials have some perceived disadvantages. One such shortcoming is the length of time taken to produce mature results, which is often many years; aspects of management potentially become out-dated by the time the trial is able to report results. Another disadvantage concerns the selective populations that are often treated within trials, which may not represent ‘real life’ patients; patients in trials are typically younger and fitter, have less co-morbidities and are submitted to stricter follow-up schemes than the general patient population.110 Both of these aspects can limit uptake of trial results into clinical practice,111 and this may be hampered further by infrastructural, organisational or financial barriers, such as those observed for twice-daily RT in treating limited-stage SCLC.
The European SocieTy for Radiotherapy and Oncology-Health Economics in Radiation Oncology (ESTRO-HERO) project surveyed European countries regarding the availability of RT facilities and personnel, which are key issues for RT access (Fig. 2). The study reported large variation across Europe in resource availability, and showed a clear correlation with national income. It also highlighted serious gaps in RT provision and staffing that was more pronounced in, although not limited to, countries in Southern and Eastern Europe.112,113 Across 40 European countries, RT utilisation was much lower than estimated; just under half were treating less than 70% of patients requiring RT.114 Similarly, the Global Task Force on Radiotherapy in Cancer Care and Control (GTFRCC) published a model of worldwide RT supply and demand based on cancer incidence, number of RT machines available and evidence-based guidelines for RT. At least 36 countries had no RT machines at all, and there was a distinct correlation between national income and availability of RT machines. Using available evidence from world-wide clinical trials and guidelines, this report also provided compelling evidence that investment in RT would save many millions of life-years and also create positive economic benefits4,115; even if a patient is no longer able to contribute to the workforce, the intrinsic personal or societal value of a life-saving intervention has been estimated to be 2.3 times the gross domestic product per person in a given year.116 In order to achieve the ultimate goal of equal access to radiotherapy worldwide, the GTFRCC has set forward a number of ‘Calls to Action’, including measurable targets for expansion of human resources and RT capacity (both requiring sustainable financing), aligning RT access with universal healthcare coverage and, last but not least, systematically including radiotherapy expansion in national cancer control planning.

Megavoltage RT equipment and personnel per million inhabitants across Europe. Countries coloured grey indicate no available data. Reprinted from ref. 130. Copyright (2015), with permission from Elsevier
How can the RT community tackle these issues?
Large-scale clinical trials have provided a solid rationale for making changes in clinical practice to improve patient care; adequate infrastructure and human resources are now needed to enable the implementation of these changes globally. International organisations are working to improve access to RT and to encourage research. The International Atomic Energy Agency (IAEA) has highlighted inequity in access to RT, and it promotes the setting up and maintaining of RT services in low- and middle-income countries through partnerships with centres in high-income countries. ESTRO promotes evidence-based RT and addresses the inequity of access to high-quality RT across Europe. The newly established ESTRO Cancer Foundation aims to raise awareness of RT benefits and to create a community of supporters. Its first initiative is the Marie Curie Legacy Campaign (www.150yearsmariecurie.org), which will educate the general public about the life and work of this iconic scientist, and highlight RT as a key component of cancer treatment (Fig. 3). In addition, the UK Clinical and Translational Radiotherapy Research Working Group (CTRad) facilitates the development of new RT trials and raises awareness of the importance of RT research to funding bodies. A particular success has been through engagement with pharmaceutical companies to drive forward research into RT and novel drug combinations.11 Both ESTRO and CTRad are committed to tackling major challenges for future RT trials and assisting stakeholders in developing solutions (Table 5).

Celebrating 150 years since the birth of Marie Curie. Reproduced with permission from ACJC-Musée Curie
What is the future of RT research?
Future RT research will focus on reducing treatment toxicity and on further improving survival rates and management of locoregional relapse. This is likely to be increasingly driven by biomarkers to assist in individualising RT treatment. There now exist validated biomarkers for some cancer types, for example p16 positivity predicts better prognosis and response to chemoRT treatment in head and neck cancer. However, for most cancer types, biomarkers for response to RT treatment and toxicity are not yet established, and this will be an important area of future translational RT research. In this section, we discuss selected areas of predicted future clinical RT research. As we look to further refine RT, our trial designs will also need to evolve accordingly.
Reducing the toxicity of RT
RT-related toxicity may be reduced by avoiding unnecessary treatment and by continued improvements in tumour targeting, to reduce the ‘safety margin’ of normal tissue around the cancer. Technological developments such as proton beam therapy and the integration of magnetic resonance imaging (MRI) technology into RT are likely to be important areas of future research aiming to improve tumour targeting.
Proton beam therapy has the potential to dramatically reduce doses to nearby critical structures, because the physical properties of the proton radiation beam are very different to photons. This is especially important, for example, near the eye and parts of the central nervous system. It also reduces the risks of ionising radiation in paediatric patients, which can have devastating effects on growth and development.117 Until now, proton beam therapy has mainly been introduced in privately funded centres rather than through comparative clinical trials, and thus the evidence base for some tumour types is very limited. Small-scale clinical trials and patient registries are now being established, and it is hoped that the wider introduction of proton beam therapy on a global scale will provide opportunities for larger international clinical trials to demonstrate clinical benefit and assess the cost-effectiveness of this new therapy for a broad range of tumour types.
MRI allows for greater resolution of soft tissue than CT, which means many tumours, such as abdominopelvic cancers, can be identified more accurately, meaning smaller normal tissue margins are needed. MRI is currently widely used to improve the accuracy of radiological tumour staging and to guide the contouring of structures for RT planning, prior to treatment. The current challenge concerns how to accurately identify and monitor these tumours online during treatment. Many centres have the capability to perform daily image guidance with repeat CT scanning before each RT treatment, using the linear accelerator itself; however, this is of limited use for accurately imaging soft tissue, especially where there is considerable organ motion. Recently, hybrid RT machines have been developed that combine a linear accelerator with an MRI scanner (MR-linac) that is able to perform a new generation of imaging before and during RT delivery. This allows accurate localisation of the tumour pre-treatment and supports the ability to adapt treatment daily if required and to monitor the tumour and critical organ movement during treatment.118,119 This, in the future, will allow ‘gating’; the automatic switching on and off of the treatment beam according to pre-set parameters, for example to allow for respiratory and bowel motion. This may facilitate greatly improved image guidance of RT delivery, minimising the dose to normal tissues and enabling dose escalation to the tumour.
Assessment of these new technologies will be facilitated by the recently published framework for evaluation of RT technology, R-IDEAL,120 and by international clinical and research networks, for example the European Particle Therapy Network (an ESTRO taskforce) and the ATLANTIC MRL research consortium. Recently funded clinical trials are increasingly including imaging, blood or tissue biomarkers, and we expect this will support a move towards the increased personalisation of RT, for example identifying which patients are likely to benefit from RT and tailoring the dose or fractionation. Trial designs that encompass biomarker discovery or prospective validation of predictive biomarkers will maximise value for trial funders and research opportunities for patients.121,122
Improving survival rates with RT
Improved survival rates are likely to occur through employing/adopting RT in novel situations. There is growing interest in using SBRT to deliver a much higher dose than traditionally given for oligometastatic or oligoprogressive disease123; early trials have shown improvements in progression-free survival for this approach.124 Larger trials aiming to evaluate the role and benefit of ‘radical’ high-dose RT in oligometastatic disease across disease sites are currently underway in the UK (CORE) or in development (ESTRO/EORTC OligoCare studies). SBRT and/or MR-guided RT may also prove beneficial in cancers not traditionally amenable to RT, such as renal and pancreatic cancers, due to the previous inability to irradiate without including large normal tissue margins that precluded the delivery of a tumouricidal dose.
Survival may also be improved through dose escalation via improved image guidance (as previously discussed), and novel drug combinations with RT. There is currently particular interest in combining RT with DNA damage response inhibitors and immunotherapy. RT induces direct cell death by causing single- and double-stranded DNA breaks. Double-stranded DNA breaks are much more lethal to cells than single-strand breaks; however, single-stranded DNA breaks are a more frequent consequence of ionising radiation. DNA damage response inhibitors may therefore act in a ‘synthetically lethal’ manner to selectively increase the number of double-stranded DNA breaks in irradiated cells, with minimal effects on nearby non-irradiated cells.125 RT also promotes immune-mediated cell death through the increased release of tumour antigens, the induction of inflammatory cytokines, and the transient overexpression of cell surface receptors.126 Together, these mechanisms facilitate effector T cell killing of irradiated tumour cells and priming of antigen-presenting cells to increase the adaptive immune response against tumour cells elsewhere in the body, in non-irradiated areas. There are multiple ongoing clinical trials of DNA damage response inhibitors with RT127 and immunotherapy with RT.128,129 Efficient trial design in this field, through use of adaptive model-based phase I dose-finding strategies, risk stratification, biomarkers and/or appropriate intermediate endpoints, and multi-arm multi-stage studies will support more rapid evaluation of the most promising drug–RT combinations.
Conclusion
Major steps have been made in developing new RT techniques and regimens to optimise cancer outcomes, whilst simultaneously minimising toxicity. These have been achieved through high-quality clinical trials, involving collaboration across countries.
Particular successes have been the introduction of SBRT for early-stage NSCLC especially for medically inoperable patients, and the increasing use of hypofractionation in breast and prostate cancer as this improves convenience for patients and cost-effectiveness for healthcare providers, whilst maintaining excellent cancer outcomes. Despite these achievements, and together with the high cost-effectiveness of RT, access to evidence-based RT is not available to everyone. Organisations such as the IAEA, ESTRO and CTRad are making great progress in raising awareness of this inequity and educating both health professionals and policy makers. As we mark the 150th anniversary of Marie Curie’s birth, we hope that international co-operation of the RT community will facilitate high-quality evidenced-based RT for the millions of people who require it, regardless of where they live.
References
Ringborg, U. et al. The Swedish Council on Technology Assessment in Health Care (SBU) Systematic Overview of Radiotherapy for Cancer including a Prospective Survey of Radiotherapy Practice in Sweden 2001*/ Summary and Conclusions. Acta Oncol. 426, 357–365 (2003).
International Atomic Energy Agency. Planning National Radiotherapy Services: a Practical Tool. (Vienna: IAEA Human Health Series Publications, 2010)
Parker, T. Radiotherapy Services in England 2012 (London: Department of Health, 2012).
Atun, R. et al. Expanding global access to radiotherapy. Lancet Oncol. 16, 1153–1186 (2015).
Norlund, A., SBU Survey Group. Costs of radiotherapy. Acta Oncol. 42, 411–415 (2003).
Jönsson, B., Hofmarcher, T., Lindgren, P. & Wilking, N. The cost and burden of cancer in the European Union 1995-2014. Eur. J. Cancer 66, 162–170 (2016).
Williams, M. V., Jamesy, N. D., Summersz, E. T., Barrettx, A. & Ashk, D. V. National Survey of Radiotherapy Fractionation Practice in 2003. Clin. Oncol. 18, 3–14 (2006).
Society and College of Radiographers; Institute of Physics and Engineering in Medicine; Royal College of Radiologists. Intensity Modulated Radiotherapy (IMRT) in the UK: Current Access and Predictions of Future Access Rates (London/York: Society and College of Radiographers; Institute of Physics and Engineering in Medicine; Royal College of Radiologists, 2014).
Ahmad, S. S., Duke, S., Jena, R., Williams, M. V. & Burnet, N. G. Advances in radiotherapy. BMJ 345, e7765 (2012).
Giaccia, A. J. Molecular radiobiology: the state of the art. J. Clin. Oncol. 32, 2871–2878 (2014).
Sharma, R. A. et al. Clinical development of new drug–radiotherapy combinations. Nat. Rev. Clin. Oncol. 13, 627–642 (2016).
EBCTCG (Early Breast Cancer Trialists’ Collaborative Group), McGale, P. et al. Effect of radiotherapy after mastectomy and axillary surgery on 10-year recurrence and 20-year breast cancer mortality: meta-analysis of individual patient data for 8135 women in 22 randomised trials. Lancet 383, 2127–2135 (2014).
Early Breast Cancer Trialists’ Collaborative Group (EBCTCG), Darby, S. et al. Effect of radiotherapy after breast-conserving surgery on 10-year recurrence and 15-year breast cancer death: meta-analysis of individual patient data for 10,801 women in 17 randomised trials. Lancet 378, 1707–1716 (2011).
Owen, J. R. et al. Effect of radiotherapy fraction size on tumour control in patients with early-stage breast cancer after local tumour excision: long-term results of a randomised trial. Lancet Oncol. 7, 467–471 (2006).
Whelan, T. J. et al. Long-Term results of hypofractionated radiation therapy for breast cancer. N. Engl. J. Med. 362, 513–520 (2010).
Haviland, J. S. et al. The UK Standardisation of Breast Radiotherapy (START) trials of radiotherapy hypofractionation for treatment of early breast cancer: 10-year follow-up results of two randomised controlled trials. Lancet Oncol. 14, 1086–1094 (2013).
Coles, C. E., Moody, A. M., Wilson, C. B. & Burnet, N. G. Reduction of radiotherapy-induced late complications in early breast cancer: the role of intensity-modulated radiation therapy and partial breast irradiation. Part II--Radiotherapy strategies to reduce radiation-induced late effects. Clin. Oncol. 17, 98–110 (2005).
Suh, W. W., Pierce, L. J., Vicini, F. A. & Hayman, J. A. A cost comparison analysis of partial versus whole-breast irradiation after breast-conserving surgery for early-stage breast cancer. Int. J. Radiat. Oncol. Biol. Phys. 62, 790–796 (2005).
Lievens, Y. Hypofractionated breast radiotherapy: financial and economic consequences. Breast 19, 192–197 (2010).
Monten, C. & Lievens, Y. Adjuvant breast radiotherapy: how to trade-off cost and effectiveness? Radiother. Oncol. 126, 132–138 (2018).
Smith, B. D. et al. Fractionation for whole breast irradiation: an American society for radiation oncology (ASTRO) evidence-based guideline. Int. J. Radiat. Oncol. Biol. Phys. 81, 59–68 (2011).
National Institute for Health and Care Excellence. Early and Locally Advanced Breast Cancer: Diagnosis and Treatment (London: NICE, 2009).
Bekelman, J. E. et al. Uptake and costs of hypofractionated vs. conventional whole breast irradiation after breast conserving surgery in the United States, 2008–2013. JAMA 312, 2542–2550 (2014).
Prades, J. et al. Understanding variations in the use of hypofractionated radiotherapy and its specific indications for breast cancer: a mixed-methods study. Radiother. Oncol. 123, 22–28 (2017).
Bartelink, H. et al. Impact of a higher radiation dose on local control and survival in breast-conserving therapy of early breast cancer: 10-year results of the randomized boost versus no boost EORTC 22881-10882 trial. J. Clin. Oncol. 25, 3259–3265 (2007).
Vrieling, C. et al. Prognostic factors for local control in breast cancer after long-term follow-up in the EORTC boost vs no boost trial. JAMA Oncol. 3, 42 (2017).
Polgár, C. et al. Accelerated partial-breast irradiation using high-dose-rate interstitial brachytherapy: 12-year update of a prospective clinical study. Radiother. Oncol. 94, 274–279 (2010).
Livi, L. et al. Accelerated partial breast irradiation using intensity-modulated radiotherapy versus whole breast irradiation: 5-year survival analysis of a phase 3 randomised controlled trial. Eur. J. Cancer 51, 451–463 (2015).
Veronesi, U. et al. Intraoperative radiotherapy versus external radiotherapy for early breast cancer (ELIOT): a randomised controlled equivalence trial. Lancet Oncol. 14, 1269–1277 (2013).
Vaidya, J. S. et al. Risk-adapted targeted intraoperative radiotherapy versus whole-breast radiotherapy for breast cancer: 5-year results for local control and overall survival from the TARGIT-A randomised trial. Lancet 383, 603–613 (2014).
Haviland, J. S., A’Hern, R., Bentzen, S. M., Whelan, T. & Bliss, J. M. Radiotherapy for breast cancer, the TARGIT-A trial. Lancet 383, 1716–1717 (2014).
Strnad, V. et al. 5-year results of accelerated partial breast irradiation using sole interstitial multicatheter brachytherapy versus whole-breast irradiation with boost after breast-conserving surgery for low-risk invasive and in-situ carcinoma of the female breast: a randomised, phase 3, non-inferiority trial. Lancet 387, 229–238 (2016).
Coles, C. E. et al. Partial-breast radiotherapy after breast conservation surgery for patients with early breast cancer (UK IMPORT LOW trial): 5-year results from a multicentre, randomised, controlled, phase 3, non-inferiority trial. Lancet 390, 1048–1060 (2017).
Donker, M. et al. Radiotherapy or surgery of the axilla after a positive sentinel node in breast cancer (EORTC 10981-22023 AMAROS): a randomised, multicentre, open-label, phase 3 non-inferiority trial. Lancet Oncol. 15, 1303–1310 (2014).
Poortmans, P. M. et al. Internal mammary and medial supraclavicular irradiation in breast cancer. N. Engl. J. Med. 373, 317–327 (2015).
Whelan, T. J. et al. Regional nodal irradiation in early-stage breast cancer. N. Engl. J. Med. 373, 307–316 (2015).
Thorsen, L. B. J. et al. DBCG-IMN: a population-based cohort study on the effect of internal mammary node irradiation in early node-positive breast cancer. J. Clin. Oncol. 34, 314–320 (2016).
Recht, A. et al. Postmastectomy radiotherapy: an American Society of Clinical Oncology, American Society for Radiation Oncology, and Society of Surgical Oncology Focused Guideline update. J. Clin. Oncol. 34, 4431–4442 (2016).
Bhattacharya, I. S., Kirby, A. M., Bliss, J. M. & Coles, C. E. Can interrogation of tumour characteristics lead us to safely omit adjuvant radiotherapy in patients with early breast cancer? Clin. Oncol. 30, 158–165 (2018).
Aristei, C. et al. The Assisi Think Tank Meeting and Survey of post MAstectomy Radiation Therapy after breast reconstruction: the ATTM-SMART report. Eur. J. Surg. Oncol. https://doi.org/10.1016/j.ejso.2018.01.010 (2018).
Lightowlers, S. V. et al. Preoperative breast radiation therapy: indications and perspectives. Eur. J. Cancer 82, 184–192 (2017).
Baumann, P. et al. Outcome in a prospective phase II trial of medically inoperable stage I non-small-cell lung cancer patients treated with stereotactic body radiotherapy. J. Clin. Oncol. 27, 3290–3296 (2009).
Fakiris, A. J. et al. Stereotactic body radiation therapy for early-stage non-small-cell lung carcinoma: four-year results of a prospective phase II study. Int. J. Radiat. Oncol. Biol. Phys. 75, 677–682 (2009).
Ricardi, U. et al. Stereotactic body radiation therapy for early stage non-small cell lung cancer: results of a prospective trial. Lung Cancer 68, 72–77 (2010).
Timmerman, R. et al. Stereotactic body radiation therapy for inoperable early stage lung cancer. JAMA 303, 1070 (2010).
Timmerman, R. D. et al. Long-term results of RTOG 0236: a Phase II Trial of Stereotactic Body Radiation Therapy (SBRT) in the treatment of patients with medically inoperable stage I non-small cell lung cancer. Int. J. Radiat. Oncol. 90, S30 (2014).
Videtic, G. M. M. et al. Intensity-modulated radiotherapy-based stereotactic body radiotherapy for medically inoperable early-stage lung cancer: excellent local control. Int. J. Radiat. Oncol. Biol. Phys. 77, 344–349 (2010).
Soldà, F. et al. Stereotactic radiotherapy (SABR) for the treatment of primary non-small cell lung cancer; Systematic review and comparison with a surgical cohort. Radiother. Oncol. 109, 1–7 (2013).
Nagata, Y. et al. Prospective trial of stereotactic body radiation therapy for both operable and inoperable T1N0M0 non-small cell lung cancer: Japan Clinical Oncology Group Study JCOG0403. Int. J. Radiat. Oncol. 93, 989–996 (2015).
Cassidy, R. J. et al. Stereotactic body radiotherapy for early-stage non–small-cell lung cancer in patients 80 years and older: a multi-center analysis. Clin. Lung Cancer 18, 551–558.e6 (2017).
Sun, B. et al. 7-year follow-up after stereotactic ablative radiotherapy for patients with stage I non-small cell lung cancer: results of a phase 2 clinical trial. Cancer 123, 3031–3039 (2017).
Postmus, P. E. et al. Early and locally advanced non-small-cell lung cancer (NSCLC): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 28(Suppl. 4), iv1–iv21 (2017).
Palma, D. et al. Impact of introducing stereotactic lung radiotherapy for elderly patients with stage I non–small-cell lung cancer: a population-based time-trend analysis. J. Clin. Oncol. 28, 5153–5159 (2010).
Dalwadi, S. M. et al. Practice patterns and outcomes in elderly stage I non-small-cell lung cancer: a 2004 to 2012 SEER analysis. Clin. Lung Cancer 19, e269–e276 (2018).
Socinski, M. A. et al. Dose-escalating conformal thoracic radiation therapy with induction and concurrent carboplatin/paclitaxel in unresectable stage IIIA/B nonsmall cell lung carcinoma: a modified phase I/II trial. Cancer 92, 1213–1223 (2001).
Socinski, M. A. et al. Randomized phase II trial of Induction chemotherapy followed by concurrent chemotherapy and dose-escalated thoracic conformal radiotherapy (74 Gy) in stage III non–small-cell lung cancer: CALGB 30105. J. Clin. Oncol. 26, 2457–2463 (2008).
Schild, S. E. et al. Results of a phase I trial of concurrent chemotherapy and escalating doses of radiation for unresectable non–small-cell lung cancer. Int. J. Radiat. Oncol. 65, 1106–1111 (2006).
Bradley, J. D. et al. Primary analysis of the phase II component of a phase I/II dose intensification study using three-dimensional conformal radiation therapy and concurrent chemotherapy for patients with inoperable non–small-cell lung cancer: RTOG 0117. J. Clin. Oncol. 28, 2475–2480 (2010).
Bradley, J. D. et al. Standard-dose versus high-dose conformal radiotherapy with concurrent and consolidation carboplatin plus paclitaxel with or without cetuximab for patients with stage IIIA or IIIB non-small-cell lung cancer (RTOG 0617): a randomised, two-by-two factorial phase 3 study. Lancet Oncol. 16, 187–199 (2015).
Chun, S. G. et al. Impact of intensity-modulated radiation therapy technique for locally advanced non–small-cell lung cancer: a secondary analysis of the NRG Oncology RTOG 0617 Randomized Clinical Trial. J. Clin. Oncol. 35, 56–62 (2017).
Mulvenna, P. et al. Dexamethasone and supportive care with or without whole brain radiotherapy in treating patients with non-small cell lung cancer with brain metastases unsuitable for resection or stereotactic radiotherapy (QUARTZ): results from a phase 3, non-inferiority, randomised trial. Lancet 388, 2004–2014 (2016).
Turrisi, A. T. et al. Twice-daily compared with once-daily thoracic radiotherapy in limited small-cell lung cancer treated concurrently with cisplatin and etoposide. N. Engl. J. Med. 340, 265–271 (1999).
Faivre-Finn, C. et al. Concurrent once-daily versus twice-daily chemoradiotherapy in patients with limited-stage small-cell lung cancer (CONVERT): an open-label, phase 3, randomised, superiority trial. Lancet Oncol. 18, 1116–1125 (2017).
Slotman, B. et al. Prophylactic cranial irradiation in extensive small-cell lung cancer. N. Engl. J. Med. 357, 664–672 (2007).
Slotman, B. J. et al. Use of thoracic radiotherapy for extensive stage small-cell lung cancer: a phase 3 randomised controlled trial. Lancet 385, 36–42 (2015).
Früh, M. et al. Small-cell lung cancer (SCLC): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 24(S6), vi99–vi105 (2013).
Hamdy, F. C. et al. 10-Year outcomes after monitoring, surgery, or radiotherapy for localized prostate cancer. N. Engl. J. Med. 375, 1415–1424 (2016).
Widmark, A. et al. Endocrine treatment, with or without radiotherapy, in locally advanced prostate cancer (SPCG-7/SFUO-3): an open randomised phase III trial. Lancet 373, 301–308 (2009).
Mason, M. D. et al. Final report of the intergroup randomized study of combined androgen-deprivation therapy plus radiotherapy versus androgen-deprivation therapy alone in locally advanced prostate cancer. J. Clin. Oncol. 33, 2143–2150 (2015).
James, N. D. et al. Failure-free survival and radiotherapy in patients with newly diagnosed nonmetastatic prostate cancer: data from patients in the control arm of the STAMPEDE Trial. JAMA Oncol. 2, 348–357 (2016).
Peeters, S. T. H. et al. Dose-response in radiotherapy for localized prostate cancer: results of the Dutch multicenter randomized phase III trial comparing 68 Gy of radiotherapy with 78 Gy. J. Clin. Oncol. 24, 1990–1996 (2006).
Dearnaley, D. P. et al. Escalated-dose versus standard-dose conformal radiotherapy in prostate cancer: first results from the MRC RT01 randomised controlled trial. Lancet Oncol. 8, 475–487 (2007).
Dearnaley, D. P. et al. Escalated-dose versus control-dose conformal radiotherapy for prostate cancer: long-term results from the MRC RT01 randomised controlled trial. Lancet Oncol. 15, 464–473 (2014).
Morris, W. J. et al. Androgen Suppression Combined with Elective Nodal and Dose Escalated Radiation Therapy (the ASCENDE-RT Trial): an analysis of survival endpoints for a randomized trial comparing a low-dose-rate brachytherapy boost to a dose-escalated external beam boost for high- and intermediate-risk prostate cancer. Int. J. Radiat. Oncol. 98, 275–285 (2017).
Wilkins, A. et al. Hypofractionated radiotherapy versus conventionally fractionated radiotherapy for patients with intermediate-risk localised prostate cancer: 2-year patient-reported outcomes of the randomised, non-inferiority, phase 3 CHHiP trial. Lancet Oncol. 16, 1605–1616 (2015).
Dearnaley, D. et al. Conventional versus hypofractionated high-dose intensity-modulated radiotherapy for prostate cancer: 5-year outcomes of the randomised, non-inferiority, phase 3 CHHiP trial. Lancet Oncol. 17, 1047–1060 (2016).
The Royal College of Radiologists. Radiotherapy Dose- Fractionation (London: Royal College of Radiologists, 2016).
NHS England Specialised Services Clinical Reference Group Radiotherapy. Clinical Commissioning Policy: Hypofractionated External Beam Radiotherapy In The Treatment Of Localised Prostate Cancer (Adults) (electronic format only: NHS England, 2017).
Incrocci, L. et al. Hypofractionated versus conventionally fractionated radiotherapy for patients with localised prostate cancer (HYPRO): final efficacy results from a randomised, multicentre, open-label, phase 3 trial. Lancet Oncol. 17, 1061–1069 (2016).
Lee, W. R. et al. Randomized phase III noninferiority study comparing two radiotherapy fractionation schedules in patients with low-risk prostate cancer. J. Clin. Oncol. 34, 2325–2332 (2016).
Catton, C. N. et al. Randomized trial of a hypofractionated radiation regimen for the treatment of localized prostate cancer. J. Clin. Oncol. 35, 1884–1890 (2017).
Parker, C. et al. Alpha emitter radium-223 and survival in metastatic prostate cancer. N. Engl. J. Med. 369, 213–223 (2013).
Nilsson, S. et al. Patient-reported quality-of-life analysis of radium-223 dichloride from the phase III ALSYMPCA study. Ann. Oncol. 27, 868–874 (2016).
Parker, C., Gillessen, S., Heidenreich, A. & Horwich, A. Cancer of the prostate: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 26, v69–v77 (2015).
National Institute for Health and Care Excellence. Radium-223 Dichloride For Treating Hormone-relapsed Prostate Cancer With Bone Metastases (TA412) (London: NICE, 2016).
James, N. D. et al. Radiotherapy with or without chemotherapy in muscle-invasive bladder cancer. N. Engl. J. Med. 366, 1477–1488 (2012).
Hoskin, P. J., Rojas, A. M., Bentzen, S. M., & Saunders, M. I. Radiotherapy with concurrent carbogen and nicotinamide in bladder carcinoma. J. Clin. Oncol. 28, 4912–4918 (2010).
National Institute for Health and Care Excellence. Bladder Cancer: Diagnosis And Management (London: NICE, 2015).
MacFarlane, J. K., Ryall, R. D. H. & Heald, R. J. Mesorectal excision for rectal cancer. Lancet 341, 457–460 (1993).
Kapiteijn, E. et al. Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer. N. Engl. J. Med. 345, 638–646 (2001).
Sebag-Montefiore, D. et al. Preoperative radiotherapy versus selective postoperative chemoradiotherapy in patients with rectal cancer (MRC CR07 and NCIC-CTG C016): a multicentre, randomised trial. Lancet 373, 811–820 (2009).
Glynne-Jones, R. et al. Rectal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 28(s4), iv22–iv40 (2017).
Bosset, J.-F. et al. Chemotherapy with preoperative radiotherapy in rectal cancer. N. Engl. J. Med. 355, 1114–1123 (2006).
Gérard, J.-P. et al. Preoperative radiotherapy with or without concurrent fluorouracil and leucovorin in T3-4 rectal cancers: results of FFCD 9203. J. Clin. Oncol. 24, 4620–4625 (2006).
Sauer, R. et al. Preoperative versus postoperative chemoradiotherapy for rectal cancer. N. Engl. J. Med. 351, 1731–1740 (2004).
Roh, M. S. et al. Preoperative multimodality therapy improves disease-free survival in patients with carcinoma of the rectum: NSABP R-03. J. Clin. Oncol. 27, 5124–5130 (2009).
National Institute for Health and Care Excellence. Colorectal Cancer: The Diagnosis And Management Of Colorectal Cancer (London: NICE, 2011).
Glimelius, B., Tiret, E., Cervantes, A. & Arnold, D. Rectal cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 24(S6), vi81–vi88 (2013).
Bujko, K. et al. Long-term results of a randomized trial comparing preoperative short-course radiotherapy with preoperative conventionally fractionated chemoradiation for rectal cancer. Br. J. Surg. 93, 1215–1223 (2006).
Ngan, S. Y. et al. Randomized trial of short-course radiotherapy versus long-course chemoradiation comparing rates of local recurrence in patients with T3 rectal cancer: Trans-Tasman Radiation Oncology Group trial 01.04. J. Clin. Oncol. 30, 3827–3833 (2012).
Flam, M. et al. Role of mitomycin in combination with fluorouracil and radiotherapy, and of salvage chemoradiation in the definitive nonsurgical treatment of epidermoid carcinoma of the anal canal: results of a phase III randomized intergroup study. J. Clin. Oncol. 14, 2527–2539 (1996).
Bartelink, H. et al. Concomitant radiotherapy and chemotherapy is superior to radiotherapy alone in the treatment of locally advanced anal cancer: results of a phase III randomized trial of the European Organization for Research and Treatment of Cancer Radiotherapy and Gastrointestinal Cooperative Groups. J. Clin. Oncol. 15, 2040–2049 (1997).
Northover, J. M. A. et al. Epidermoid anal cancer: results from the UKCCCR randomised trial of radiotherapy alone versus radiotherapy, 5-fluorouracil, and mitomycin. Lancet 348, 1049–1054 (1996).
Glynne-Jones, R. et al. Anal cancer: ESMO-ESSO-ESTRO clinical practice guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 25, 10–20 (2014).
Ajani, J. A. et al. Fluorouracil, mitomycin, and radiotherapy vs fluorouracil, cisplatin, and radiotherapy for carcinoma of the anal canal: a randomized controlled trial. JAMA 299, 1914–1921 (2008).
Peiffert, D. et al. Induction chemotherapy and dose intensification of the radiation boost in locally advanced anal canal carcinoma: final analysis of the randomized UNICANCER ACCORD 03 trial. J. Clin. Oncol. 30, 1941–1948 (2012).
James, R. D. et al. Mitomycin or cisplatin chemoradiation with or without maintenance chemotherapy for treatment of squamous-cell carcinoma of the anus (ACT II): a randomised, phase 3, open-label, 2 × 2 factorial trial. Lancet Oncol. 14, 516–524 (2013).
Glynne-Jones, R. et al. EXTRA--a multicenter phase II study of chemoradiation using a 5 day per week oral regimen of capecitabine and intravenous mitomycin C in anal cancer. Int. J. Radiat. Oncol. Biol. Phys. 72, 119–126 (2008).
Kachnic, L. A. et al. RTOG 0529: a phase 2 evaluation of dose-painted intensity modulated radiation therapy in combination with 5-fluorouracil and mitomycin-C for the reduction of acute morbidity in carcinoma of the anal canal. Int. J. Radiat. Oncol. Biol. Phys. 86, 27–33 (2013).
De Ruysscher, D. et al. Eligibility for concurrent chemotherapy and radiotherapy of locally advanced lung cancer patients: a prospective, population-based study. Ann. Oncol. 20, 98–102 (2009).
Lievens, Y. Access to innovative radiotherapy: how to make it happen from an economic perspective? Acta Oncol. 56, 1353–1358 (2017).
Grau, C. et al. Radiotherapy equipment and departments in the European countries: final results from the ESTRO-HERO survey. Radiother. Oncol. 112, 155–164 (2014).
Lievens, Y. et al. Radiotherapy staffing in the European countries: final results from the ESTRO-HERO survey. Radiother. Oncol. 112, 178–186 (2014).
Borras, J. M. et al. The optimal utilization proportion of external beam radiotherapy in European countries: an ESTRO-HERO analysis. Radiother. Oncol. 116, 38–44 (2015).
Yap, M. L., Zubizarreta, E., Bray, F., Ferlay, J. & Barton, M. Global access to radiotherapy services: have we made progress during the past decade? J. Glob. Oncol. 2, 207–215 (2016).
Jamison, D. T. et al. Global health 2035: a world converging within a generation. Lancet 382, 1898–1955 (2013).
Schwartz, C. L. Long-term survivors of childhood cancer: the late effects of therapy. Oncologist 4, 45–54 (1999).
McPartlin, A. J. et al. MRI-guided prostate adaptive radiotherapy - a systematic review. Radiother. Oncol. 119, 371–380 (2016).
Henke, L. et al. Phase I trial of stereotactic MR-guided online adaptive radiation therapy (SMART) for the treatment of oligometastatic or unresectable primary malignancies of the abdomen. Radiother. Oncol. https://doi.org/10.1016/j.radonc.2017.11.032 (2017).
Verkooijen, H. M. et al. R-IDEAL: a framework for systematic clinical evaluation of technical innovations in radiation oncology. Front Oncol. 7, 59 (2017).
Bibault, J.-E. et al. Personalized radiation therapy and biomarker-driven treatment strategies: a systematic review. Cancer Metastasis Rev. 32, 479–492 (2013).
Forker, L. J., Choudhury, A. & Kiltie, A. E. Biomarkers of tumour radiosensitivity and predicting benefit from radiotherapy. Clin. Oncol. 27, 561–569 (2015).
Tree, A. C. et al. Stereotactic body radiotherapy for oligometastases. Lancet Oncol. 14, 28–37 (2013).
Ost, P. et al. Surveillance or metastasis-directed therapy for oligometastatic prostate cancer recurrence: a prospective, randomized, multicenter phase II trial. J. Clin. Oncol. 36, 446–453 (2018).
Goldstein, M. & Kastan, M. B. The DNA damage response: implications for tumor responses to radiation and chemotherapy. Annu. Rev. Med. 66, 129–143 (2015).
Van Limbergen, E. J. et al. Combining radiotherapy with immunotherapy: the past, the present and the future. Br. J. Radiol. 90, 20170157 (2017).
Chalmers, A. J. Science in focus: combining radiotherapy with inhibitors of the DNA damage response. Clin. Oncol. 28, 279–282 (2016).
Kang, J., Demaria, S. & Formenti, S. Current clinical trials testing the combination of immunotherapy with radiotherapy. J. Immunother. Cancer 4, 51 (2016).
Marshall, R. et al. Immune checkpoint inhibitors in lung cancer - an unheralded opportunity? Clin. Oncol. 29, 207–217 (2017).
Lievens, Y. et al. HERO (Health Economics in Radiation Oncology): a pan-European project on radiotherapy resources and needs. Clin. Oncol. 27, 115–124 (2015).
Whelan, T. et al. Randomized trial of breast irradiation schedules after lumpectomy for women with lymph node-negative breast cancer. J. Natl. Cancer Inst. 94, 1143–1150 (2002).
Agrawal, R. K. et al. The UK Standardisation of Breast Radiotherapy (START) Trial B of radiotherapy hypofractionation for treatment of early breast cancer: a randomised trial. Lancet 371, 1098–1107 (2008).
Venables, K., Winfield, E., Deighton, A., Aird, E. & Hoskin, P., START Trial Management Group STM. Breast radiotherapy phantom design for the START trial. Br. J. Radiol. 73, 1313–1316 (2000).
Venables, K., Winfield, E., Deighton, A., Aird, E. & Hoskin, P., START Trial Management Group. The START trial-measurements in semi-anatomical breast and chest wall phantoms. Phys. Med. Biol. 46, 1937–1948 (2001).
Venables, K., Winfield, E., Deighton, A., Aird, E. & Hoskin, P. A survey of radiotherapy quality control practice in the United Kingdom for the START trial. Radiother. Oncol. 60, 311–318 (2001).
Winfield, E., Deighton, A., Venables, K., Hoskin, P. J., & Aird, E. G. A. Survey of UK breast radiotherapy techniques: background prior to the introduction of the quality assurance programme for the START (standardisation of radiotherapy) trial in breast cancer. Clin. Oncol. 14, 267–271 (2002).
Winfield, E. A., Deighton, A., Venables, K., Hoskin, P. J. & Aird, E. G. A. Survey of tangential field planning and dose distribution in the UK: background to the introduction of the quality assurance programme for the START trial in early breast cancer. Br. J. Radiol. 76, 254–259 (2003).
Venables, K., Winfield, E. A., Aird, E. G. & Hoskin, P. J. Three-dimensional distribution of radiation within the breast: an intercomparison of departments participating in the START trial of breast radiotherapy fractionation. Int. J. Radiat. Oncol. 55, 271–279 (2003).
Venables, K., Miles, E. A., Deighton, A., Aird, E. G. A. & Hoskin, P. J. Irradiation of the heart during tangential breast treatment: a study within the START trial. Br. J. Radiol. 77, 137–142 (2004).
Venables, K., Miles, E. A., Aird, E. G., & Hoskin, P. J. The use of in vivo thermoluminescent dosimeters in the quality assurance programme for the START breast fractionation trial. Radiother. Oncol. 71, 303–310 (2004).
Venables, K., Miles, E. A., Hoskin, P. J. & Aird, E. G. A., START. Verification films: a study of the daily and weekly reproducibility of breast patient set-up in the START trial. Clin. Oncol. 17, 337–342 (2005).
Venables, K., Miles, E. A., Aird, E. G. A. & Hoskin, P. J. What is the optimum breast plan: a study based on the START trial plans. Br. J. Radiol. 79, 734–739 (2006).
START Trialists’ Group, Bentzen, S. M. et al. The UK Standardisation of Breast Radiotherapy (START) Trial A of radiotherapy hypofractionation for treatment of early breast cancer: a randomised trial. Lancet Oncol. 9, 331–341 (2008).
Hopwood, P. et al. Comparison of patient-reported breast, arm, and shoulder symptoms and body image after radiotherapy for early breast cancer: 5-year follow-up in the randomised Standardisation of Breast Radiotherapy (START) trials. Lancet Oncol. 11, 231–240 (2010).
Royal College of Radiologists. Postoperative Radiotherapy For Breast Cancer: UK Consensus Statements (London: Royal College of Radiologists, 2016).
Poortmans, P. et al. The influence of the boost technique on local control in breast conserving treatment in the EORTC “boost versus no boost” randomised trial. Radiother. Oncol. 72, 25–33 (2004).
van Tienhoven, G., van Bree, N. A., Mijnheer, B. J. & Bartelink, H. Quality assurance of the EORTC trial 22881/10882: “assessment of the role of the booster dose in breast conserving therapy”: the Dummy Run. EORTC Radiotherapy Cooperative Group. Radiother. Oncol. 22, 290–298 (1991).
van Tienhoven, G., Mijnheer, B. J., Bartelink, H. & González, D. G. Quality assurance of the EORTC Trial 22881/10882: boost versus no boost in breast conserving therapy. An overview. Strahlenther. Onkol. 173, 201–207 (1997).
Vrieling, C. et al. The influence of the boost in breast-conserving therapy on cosmetic outcome in the EORTC boost versus no boost trial. EORTC Radiotherapy and Breast Cancer Cooperative Groups. European Organization for Research and Treatment of Cancer. Int. J. Radiat. Oncol. Biol. Phys. 45, 677–685 (1999).
Vrieling, C. et al. Validation of the methods of cosmetic assessment after breast-conserving therapy in the EORTC “boost versus no boost” trial. EORTC Radiotherapy and Breast Cancer Cooperative Groups. European Organization for Research and Treatment of Cancer. Int. J. Radiat. Oncol. Biol. Phys. 45, 667–676 (1999).
Poortmans, P. M. P. et al. Quality assurance in the EORTC phase III randomised “boost vs. no boost” trial for breast conserving therapy: comparison of the results of two individual case reviews performed early and late during the accrual period. Radiother. Oncol. 76, 278–284 (2005).
Senkus, E. et al. Primary breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 26, v8–v30 (2015).
Coles, C. & Yarnold, J., IMPORT Trials Management Group. The IMPORT trials are launched (September 2006). Clin. Oncol. 18, 587–590 (2006).
Coles, C. E. et al. Titanium clip placement to allow accurate tumour bed localisation following breast conserving surgery – audit on behalf of the IMPORT Trial Management Group. Eur. J. Surg. Oncol. 35, 578–582 (2009).
Harris, E. J., Donovan, E. M., Yarnold, J. R., Coles, C. E. & Evans, P. M. Characterization of target volume changes during breast radiotherapy using implanted fiducial markers and portal imaging. Int. J. Radiat. Oncol. 73, 958–966 (2009).
Coles, C. E. et al. Evaluation of implanted gold seeds for breast radiotherapy planning and on treatment verification: a feasibility study on behalf of the IMPORT trialists. Radiother. Oncol. 100, 276–281 (2011).
Harris, E. J. et al. A multicentre observational study evaluating image-guided radiotherapy for more accurate partial-breast intensity-modulated radiotherapy: comparison with standard imaging technique. Effic. Mech. Eval. 1, 1–74 (2014).
Bourez, R. L. & Rutgers, E. J. The European Organization for Research and Treatment of Cancer (EORTC) Breast Cancer Group: quality control of surgical trials. Surg. Oncol. Clin. N. Am. 10, 807–819 (2001).
Hurkmans, C. W., Borger, J. H., Rutgers, E. J. T. & van Tienhoven, G., EORTC Breast Cancer Cooperative Group, Radiotherapy Cooperative Group. Quality assurance of axillary radiotherapy in the EORTC AMAROS trial 10981/22023: the dummy run. Radiother. Oncol. 68, 233–240 (2003).
Association of Breast Surgery Trustees. Association of Breast Surgery Consensus Statement Management of the Malignant Axilla in Early Breast Cancer (London: Association of Breast Surgery, 2015).
Poortmans, P. M. et al. The potential impact of treatment variations on the results of radiotherapy of the internal mammary lymph node chain: a quality-assurance report on the dummy run of EORTC Phase III randomized trial 22922/10925 in Stage I--III breast cancer(1). Int. J. Radiat. Oncol. Biol. Phys. 49, 1399–1408 (2001).
Lievens, Y., Poortmans, P., Van & den Bogaert, W. A glance on quality assurance in EORTC study 22922 evaluating techniques for internal mammary and medial supraclavicular lymph node chain irradiation in breast cancer. Radiother. Oncol. 60, 257–265 (2001).
Poortmans, P. et al. Quality assurance of EORTC trial 22922/10925 investigating the role of internal mammary--medial supraclavicular irradiation in stage I-III breast cancer: the individual case review. Eur. J. Cancer 39, 2035–2042 (2003).
Poortmans, P. et al. Quality assurance in the EORTC randomized trial 22922/10925 investigating the role of irradiation of the internal mammary and medial supraclavicular lymph node chain works. Strahlenther. Onkol. 182, 576–582 (2006).
Musat, E. et al. Quality assurance in breast cancer: EORTC experiences in the phase III trial on irradiation of the internal mammary nodes. Eur. J. Cancer 43, 718–724 (2007).
Thorsen, L. B. J., Thomsen, M. S., Overgaard, M., Overgaard, J. & Offersen, B. V., Danish Breast Cancer Cooperative Group Radiotherapy Committee. Quality assurance of conventional non-CT-based internal mammary lymph node irradiation in a prospective Danish Breast Cancer Cooperative Group trial: The DBCG-IMN study. Acta Oncol. 52, 1526–1534 (2013).
Timmerman, R. et al. Excessive toxicity when treating central tumors in a phase II study of stereotactic body radiation therapy for medically inoperable early-stage lung cancer. J. Clin. Oncol. 24, 4833–4839 (2006).
National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology Non-Small Cell Lung Cancer (electronic format only: National Comprehensive Cancer Network, 2017).
Nyman, J. et al. SPACE – a randomized study of SBRT vs conventional fractionated radiotherapy in medically inoperable stage I NSCLC. Radiother. Oncol. 121, 1–8 (2016).
National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology Small Cell Lung Cancer (electronic format only: National Comprehensive Cancer Network, 2018).
Le Péchoux, C. et al. Standard-dose versus higher-dose prophylactic cranial irradiation (PCI) in patients with limited-stage small-cell lung cancer in complete remission after chemotherapy and thoracic radiotherapy (PCI 99-01, EORTC 22003-08004, RTOG 0212, and IFCT 99-01): a randomised clinical trial. Lancet Oncol. 10, 467–474 (2009).
Groom, N., Wilson, E., Lyn, E. & Faivre-Finn, C. Is pre-trial quality assurance necessary? Experiences of the CONVERT Phase III randomized trial for good performance status patients with limited-stage small-cell lung cancer. Br. J. Radiol. 87, 20130653 (2014).
Groom, N., Wilson, E. & Faivre-Finn, C. Effect of accurate heart delineation on cardiac dose during the CONVERT trial. Br. J. Radiol. 90, 20170036 (2017).
Faivre-Finn, C. et al. Protocol for the CONVERT trial-Concurrent ONce-daily VErsus twice-daily RadioTherapy: an international 2-arm randomised controlled trial of concurrent chemoradiotherapy comparing twice-daily and once-daily radiotherapy schedules in patients with limited stage small cell lung cancer (LS-SCLC) and good performance status. BMJ Open. 6, e009849 (2016).
Slotman, B. J. et al. Prophylactic cranial irradiation in extensive disease small-cell lung cancer: short-term health-related quality of life and patient reported symptoms: results of an international Phase III randomized controlled trial by the EORTC Radiation Oncology and Lung Cancer Groups. J. Clin. Oncol. 27, 78–84 (2009).
Slotman, B. What is the optimal radiotherapy schedule for limited stage small cell lung cancer? Lung Cancer 105, 52–53 (2017).
Haslett, K. et al. Management of patients with extensive-stage small-cell lung cancer: a European survey of practice. Radiother. Oncol. 119, S63–S64 (2016).
Patrice, G. I. et al. Cost-effectiveness of thoracic radiation therapy for extensive-stage small cell lung cancer using evidence from the chest radiotherapy extensive-stage small cell lung cancer trial (CREST). Int. J. Radiat. Oncol. 100, 97–106 (2018).
National Institute for Health and Care Excellence. Prostate Cancer: Diagnosis And Management. (London: NICE, 2014).
Seddon, B., Bidmead, M., Wilson, J., Khoo, V. & Dearnaley, D. Target volume definition in conformal radiotherapy for prostate cancer: quality assurance in the MRC RT-01 trial. Radiother. Oncol. 56, 73–83 (2000).
National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology Prostate Cancer (electronic format only: National Comprehensive Cancer Network, 2017).
Peeters, S. T. H. et al. Acute and late complications after radiotherapy for prostate cancer: results of a multicenter randomized trial comparing 68 Gy to 78 Gy. Int. J. Radiat. Oncol. 61, 1019–1034 (2005).
Aluwini, S. et al. Hypofractionated versus conventionally fractionated radiotherapy for patients with prostate cancer (HYPRO): acute toxicity results from a randomised non-inferiority phase 3 trial. Lancet Oncol. 16, 274–283 (2015).
Aluwini, S. et al. Hypofractionated versus conventionally fractionated radiotherapy for patients with prostate cancer (HYPRO): late toxicity results from a randomised, non-inferiority, phase 3 trial. Lancet Oncol. 17, 464–474 (2016).
American Urological Association. Clinically Localized Prostate Cancer: AUA/ASTRO/SUO Guideline. http://www.auanet.org/guidelines/clinically-localized-prostate-cancer-new-(aua/astro/suo-guideline-2017)#x6909. Accessed 3 Nov 2017.
Höcht, S. et al. Hypofractionated radiotherapy for localized prostate cancer. Strahlenther. Onkol. 193, 1–12 (2017).
Sartor, O. et al. Effect of radium-223 dichloride on symptomatic skeletal events in patients with castration-resistant prostate cancer and bone metastases: results from a phase 3, double-blind, randomised trial. Lancet Oncol. 15, 738–746 (2014).
Huddart, R. A. et al. Randomized noninferiority trial of reduced high-dose volume versus standard volume radiation therapy for muscle-invasive bladder cancer: results of the BC2001 trial (CRUK/01/004). Int. J. Radiat. Oncol. Biol. Phys. 87, 261–269 (2013).
McDonald, F. et al. Defining bowel dose volume constraints for bladder radiotherapy treatment planning. Clin. Oncol. 27, 22–29 (2015).
van Gijn, W. et al. Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer: 12-year follow-up of the multicentre, randomised controlled TME trial. Lancet Oncol. 12, 575–582 (2011).
Marijnen, C. A. M. et al. Acute side effects and complications after short-term preoperative radiotherapy combined with total mesorectal excision in primary rectal cancer: report of a multicenter randomized trial. J. Clin. Oncol. 20, 817–825 (2002).
Marijnen, C. A. M. et al. Impact of short-term preoperative radiotherapy on health-related quality of life and sexual functioning in primary rectal cancer: report of a multicenter randomized trial. J. Clin. Oncol. 23, 1847–1858 (2005).
Lange, M. M. et al. Urinary dysfunction after rectal cancer treatment is mainly caused by surgery. Br. J. Surg. 95, 1020–1028 (2008).
Lange, M. M. et al. Risk factors for sexual dysfunction after rectal cancer treatment. Eur. J. Cancer 45, 1578–1588 (2009).
Kusters, M. et al. Patterns of local recurrence in rectal cancer; a study of the Dutch TME trial. Eur. J. Surg. Oncol. 36, 470–476 (2010).
Wiltink, L. M. et al. Health-related quality of life 14years after preoperative short-term radiotherapy and total mesorectal excision for rectal cancer: report of a multicenter randomised trial. Eur. J. Cancer 50, 2390–2398 (2014).
Wiltink, L. M. et al. No increased risk of second cancer after radiotherapy in patients treated for rectal or endometrial cancer in the randomized TME, PORTEC-1, and PORTEC-2 trials. J. Clin. Oncol. 33, 1640–1646 (2015).
Chen, T. Y.-T. et al. Bowel function 14 years after preoperative short-course radiotherapy and total mesorectal excision for rectal cancer: report of a multicenter randomized trial. Clin. Colorectal Cancer 14, 106–114 (2015).
Wiltink, L. M. et al. Long-term health-related quality of life in patients with rectal cancer after preoperative short-course and long-course (chemo) radiotherapy. Clin. Colorectal Cancer 15, e93–e99 (2016).
National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology Rectal Cancer (electronic format only: National Comprehensive Cancer Network, 2016).
Quirke, P. et al. Effect of the plane of surgery achieved on local recurrence in patients with operable rectal cancer: a prospective study using data from the MRC CR07 and NCIC-CTG CO16 randomised clinical trial. Lancet 373, 821–828 (2009).
Stephens, R. J. et al. Impact of short-course preoperative radiotherapy for rectal cancer on patients’ quality of life: data from the Medical Research Council CR07/National Cancer Institute of Canada Clinical Trials Group C016 randomized clinical trial. J. Clin. Oncol. 28, 4233–4239 (2010).
Glynne-Jones, R. et al. Best time to assess complete clinical response after chemoradiotherapy in squamous cell carcinoma of the anus (ACT II): a post-hoc analysis of randomised controlled phase 3 trial. Lancet Oncol. 18, 347–356 (2017).
Glynne-Jones, R. et al. Tumour- and treatment-related colostomy rates following mitomycin C or cisplatin chemoradiation with or without maintenance chemotherapy in squamous cell carcinoma of the anus in the ACT II trial. Ann. Oncol. 25, 1616–1622 (2014).
Glynne-Jones, R., Adams, R., Lopes, A. & Meadows, H. Clinical endpoints in trials of chemoradiation for patients with anal cancer. Lancet Oncol. 18, e218–e227 (2017).
National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology Anal Carcinoma (electronic format only: National Comprehensive Cancer Network, 2017).
Gunderson, L. L. et al. Long-term update of US GI intergroup RTOG 98-11 Phase III trial for anal carcinoma: Survival, relapse, and colostomy failure with concurrent chemoradiation involving fluorouracil/mitomycin versus fluorouracil/cisplatin. J. Clin. Oncol. 30, 4344–4351 (2012).
Gunderson, L. L. et al. Anal carcinoma: impact of tn category of disease on survival, disease relapse, and colostomy failure in US Gastrointestinal Intergroup RTOG 98-11 Phase 3 Trial. Int. J. Radiat. Oncol. 87, 638–645 (2013).
Ben-Josef, E. et al. Impact of overall treatment time on survival and local control in patients with anal cancer: a pooled data analysis of radiation therapy oncology group trials 87-04 and 98-11. J. Clin. Oncol. 28, 5061–5066 (2010).
Acknowledgements
The authors acknowledge the UK National Cancer Research Institute Clinical and Translational Radiotherapy Research Working Group (CTRad) who initiated and coordinated the development of this manuscript. Institut Curie made an agreement with Paris Sciences and Lettres, research university, to install professorships entitled ‘Marie Curie’. The first ‘Marie Curie professor’ that will be installed is Philip Poortmans, at the occasion of the 150th anniversary of her birth. The authors acknowledge the contribution of Arta Leci, Project Manager, ESTRO Cancer Foundation, in providing information on the Marie Curie Legacy Campaign. The authors acknowledge the contribution of the association Curie et Joliot-Curie - Musée Curie for providing Fig. 3.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Research support: CEC is supported by the Cambridge National Institute of Health Research Biomedical Research Centre. RH and EH are supported by the Royal Marsden/Institute of Cancer Research NIHR Biomedical Research Centre.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Thompson, M.K., Poortmans, P., Chalmers, A.J. et al. Practice-changing radiation therapy trials for the treatment of cancer: where are we 150 years after the birth of Marie Curie?. Br J Cancer 119, 389–407 (2018). https://doi.org/10.1038/s41416-018-0201-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41416-018-0201-z
This article is cited by
-
Localized nuclear reaction breaks boron drug capsules loaded with immune adjuvants for cancer immunotherapy
Nature Communications (2023)
-
Human Cancer Cell Radiation Response Investigated through Topological Analysis of 2D Cell Networks
Annals of Biomedical Engineering (2023)
-
Human lung-cancer-cell radioresistance investigated through 2D network topology
Scientific Reports (2022)
-
Differential molecular response in mice and human thymocytes exposed to a combined-dose radiation regime
Scientific Reports (2022)
-
RENORT: a project to analyze patterns of care in radiation oncology in Spain
Clinical and Translational Oncology (2022)
