
Abstract
Preclinical evidence indicates that the endocannabinoid system is involved in neural responses to reward. This study aimed to investigate associations between basal serum concentrations of the endocannabinoids anandamide (AEA) and 2-arachidonylglycerol (2-AG) with brain functional reward processing. Additionally, a personality measure of reward dependence was obtained. Brain functional data were obtained of 30 right-handed adults by conducting fMRI at 3 Tesla using a reward paradigm. Reward dependence was obtained using the subscale reward dependence of the Tridimensional Personality Questionnaire (TPQ). Basal concentrations of AEA and 2-AG were determined in serum. Analyzing the fMRI data, for AEA and 2-AG ANCOVAs were calculated using a full factorial model, with condition (reward > control, loss > control) and concentrations for AEA and 2-AG as factors. Regression analyses were conducted for AEA and 2-AG on TPQ-RD scores. A whole-brain analysis showed a significant interaction effect of AEA concentration by condition (positive vs. negative) within the putamen (x = 26, y = 16, z = −8, F13.51, TFCE(1, 54) = 771.68, k = 70, PFWE = 0.044) resulting from a positive association of basal AEA concentrations and putamen activity to rewarding stimuli, while this association was absent in the loss condition. AEA concentrations were significantly negatively correlated with TPQ reward dependence scores (rspearman = −0.56, P = 0.001). These results show that circulating AEA may modulate brain activation during reward feedback and that the personality measure reward dependence is correlated with AEA concentrations in healthy human volunteers. Future research is needed to further characterize the nature of the lipids’ influence on reward processing, the impact on reward anticipation and outcome, and on vulnerability for psychiatric disorders.
Similar content being viewed by others

Introduction
The processing of reward is crucial to everyday functioning. Rewarding stimuli are primarily processed by subpopulations of dopaminergic neurons of the ventral tegmental area (VTA) and the substantia nigra. These neurons send their axons to brain structures involved in goal-directed behavior, decision making, and motivation, such as components of the limbic system and the striatum including the nucleus accumbens and the putamen [1, 2]. There is preclinical evidence that the endocannabinoid system (eCB), with its two functionally identified endogenous ligands N-arachidonylethanolamine (AEA) and 2-arachidonoylgycerol (2-AG), modulates the activity of the neural reward circuit also called the mesocorticolimbic system with behavioral and neural responses to reward [3,4,5,6]. eCBs act as retrograde messengers on cannabinoid receptors (CB1R) and are thought to be synthesized “on demand” in response to increased neuronal excitation [7]. Dopamine levels in the nucleus accumbens [5] and midbrain dopamine cell activity are strongly influenced by the eCB system in a CB1R-dependent manner [8]. Through these and other interactions eCBs have a significant influence on the hedonic effects of natural rewards such as social interaction [9] or food [10]. In animal models, CB1 receptor agonists enhance brain reward function lowering the threshold for intracranial self-stimulation, producing rewarding effects in the conditioned place-preference paradigm [11]. Notably, however, higher doses of CB1 receptor agonists appear to have the opposite effect [3].
Reward processing consists of an anticipation phase and a feedback phase, also called receipt or outcome. It is still unknown if anticipation and outcome of a reward recruit different brain regions [12]. Meta-analyses of fMRI studies support evidence that both phases recruit the ventral striatum [13, 14]. However, while reward outcome might activate medial orbitofrontal cortex areas—representing the value of the reward received, reward anticipation in addition recruits the anterior cingulate cortex, the insula, and areas within the brainstem [14].
As no human studies have been performed investigating a possible association between functional brain activity and peripheral endocannabinoid concentrations to date, it is completely unknown whether human peripheral endocannabinoid concentrations are associated with either brain functional reward processing or reward outcome.
Beyond the CNS, eCBs are also present in the serum and plasma [15]. Adipocytes, endothelial cells, immune cells, and visceral organs have the ability to synthesize and release eCBs to the blood and have been proposed to be a source of circulating eCBs in the periphery [16,17,18,19]. It is also possible that the lipophilic eCBs in the circulation reflect overflow from the CNS [20]. Human studies in women with major depression showed that circulating basal concentrations of AEA negatively correlate with cognitive and somatic anxiety, suggesting that AEA content may relate to the anxiety dimension of affective disorders [21]. In healthy volunteers, basal AEA serum concentrations were negatively correlated with subjective ratings of anxiety [22]. Another human study showed increases in subjective indices of sexual arousal to be significantly associated with decreases in peripheral 2-AG [23]. This suggests that peripheral eCBs correlate with emotional variables, but the nature and directionality of this relationship is still unclear.
The current study was primarily designed to investigate the effects of the peripheral endocannabinoids AEA and 2-AG on brain function during reward feedback employing a standardized card-guessing paradigm using monetary rewards [24, 25]. Based on animal studies we hypothesized basal concentrations of AEA and 2-AG would be positively correlated with increased brain function to reward in reward associated brain areas, primary with main components of the ventral striatum.
A subsequent aim of the study was to examine the association between endocannabinoid function and the stable personality marker of reward dependence. Reward dependence was assessed using the “Reward Dependence” scale derived from the Tridimensional Personality Questionnaire (TPQ, [26]). The TPQ is an inventory for personality traits developed on fundamental neurobiological assumptions. Moreover, the TPQ is thought to reflect a biologically based and heritable trait. Reward dependence characterizes the individual’s dependency on signals of mainly social reward, in particular verbal signals of social approval, social support, and present mood state [27]. We hypothesized basal concentrations of AEA and 2-AG to be positively correlated with reward dependence scores. Additionally, the Chapman Scales for Physical and Social anhedonia (SASPAS; German version: Burgdörfer and Hautzinger [28]; original version: Chapman et al. [29]) was included. Although not directly related to reward processing, anhedonia describes a reduced capacity to experience pleasure. Anhedonia represents a deficit in reward-related processes [30] and has been shown to be associated with lower nucleus accumbens activity during monetary reward processing (e.g., [31]). Finally, we exploratively examined the effect of gender on eCB concentrations and reward dependence by performing supplemental analyses.
Materials and methods
Participants
Thirty right-handed subjects were recruited by advertisements. Participant screening included a physical examination with an ECG, a psychiatric interview, a blood draw including electrolytes, inflammation markers, hepatic and renal markers, a small blood count and coagulation values, a health questionnaire, including lifetime history of drug use, a structured clinical interview for DSM-IV [32], and two clinical ratings: the Hamilton Depression Rating Scale (HAM-D, [33]) and the Hamilton Anxiety Rating Scale (HAM-A, [34, 35]). Participants were excluded if they had a body mass index (BMI) outside the range of 18–26 kg/m2, had a pathological blood test, were regular smokers, took any regular medication (excluding hormonal contraceptives), had any serious medical condition such as neurological abnormalities, an Axis I psychiatric disorder, brain injuries, worked the night shift or any other contraindication for undergoing an MRI.
Procedure
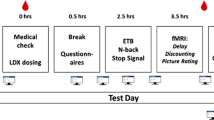
After successful screening, subjects attended an orientation session in which they provided consent and completed the Trier Personality Inventory (TPQ) as well as the Chapman Scales for Physical and Social anhedonia (SASPAS; German version: Burgdörfer and Hautzinger [28]; original version: Chapman et al. [29]). In order to obtain basal endocannabinoid concentrations under reliable, standardized circumstances, the study was splitted in two sessions. Subjects with occurring life events between the sessions were excluded from the study. Subjects were instructed not to consume any drugs 24 h before the sessions. Before session 1 (blood draw), subjects were instructed to have a regular night’s sleep and a small regular breakfast including the usual amount of caffeine at 7.30 a.m. at home. Study sessions started at 9 a.m. in the hospital. In the beginning of each session, breath alcohol and breath CO were monitored. A pregnancy test and a urine drug test were provided. An intravenous catheter was placed in the subjects’ forearm to obtain blood samples during the session. Subjects were informed to be seated in a comfortable chair and to rest. After 60 min, at 10.30 a.m., a blood draw was performed to determine concentrations of AEA and 2-AG. At session 2, the MRI scans were performed using a brain functional reward outcome paradigm. Functional MRI scans were consequently scheduled at 4 p.m. in the afternoon within 7 days after session 1. The cross-sectional study was approved by the local IRB, and all participants provided written informed consent before participation.
Dependent measures
fMRI paradigm
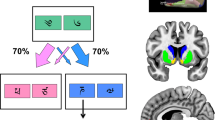
To detect brain activity associated with reward outcome, we employed a card-guessing paradigm [25, 36, 37]. Participants were told that reaction times were irrelevant for the task outcome and the final amount of their monetary reward would depend on their guessing performance on the card game. Participants were unaware that the outcome was actually fixed (10 €). The pseudo-random block design paradigm comprised 9 blocks: 3 “win” blocks (block 1, 4, 7), 3 “loose” blocks (block 2, 5, 8), and 3 control blocks (block 3, 6, 9), with each block consisting of five trials. During each trial, subjects had 3 s to guess whether the value of a visually presented card was lower or higher than 5. After the choice was made, the numerical value of the card was shown for 0.5 s, followed by feedback (red downward-oriented arrow for negative feedback, green upward-oriented arrow for positive feedback) for an additional 0.5 s. When positive feedback was given, subjects were asked to confirm the gain via button press. Finally, a crosshair was presented for 1.5 s after odd-numbered stimuli throughout the whole paradigm (e.g., for the first, third, fifth stimulus, etc.), and for 2.5 s after even-numbered stimuli (e.g., for the second, fourth, sixth stimulus, and so on), resulting in a total trial duration of 5.5 s, respectively, and 6.5 s. During the three “win” blocks, predominantly positive feedback (four trials, 80% correct) was given, whereas during the three “lose” blocks predominantly negative feedback (four trials, 80% false) was given. For each positive feedback, a fictional amount of 1 € was added, while for each negative feedback, a fictional amount of 50 cents was subtracted. The “win” and “lose” blocks were interleaved with three control blocks. During control blocks, subjects were requested to press the button during the presentation of an “x” (3 s), followed by an asterisk (0.5 s), a yellow circle (0.5 s) and a crosshair (again 1.5 s for odd-numbered stimuli; 2.5 s for even-numbered stimuli). All blocks were preceded by an instruction (3 s) resulting in a total block length of 32.5 s for odd-numbered blocks and 33.5 s for even-numbered blocks yielding a total task length of 296.5 s.
Reward dependence
During orientation, subjects completed the TPQ [26] consisting of 100 true–false questions. The TPQ was administered to assess the stable personality trait reward dependency (mean score = 18.41, SD = 4.00), consisting of the four subscales sentimentality, openness to warm communication or social sensitivity, attachment and dependence on approval by others.
Anhedonia
In addition, the Chapman Scales for Physical and Social anhedonia (SASPAS; German version: Burgdörfer and Hautzinger [28]; original version: Chapman et al. [29]) was included, measuring physical and social anhedonia that are associated with a lack of reward.
AEA and 2-AG serum concentrations
Following collection, blood samples were immediately centrifuged. Then, serum was collected and stored at −80 °C until analyses. Lipid extraction from serum was performed as previously described [38]. Contents of AEA and 2-AG were quantified by using atmospheric pressure, chemical ionization liquid chromatography—tandem mass spectrometry (LC-APCI-MS/MS) as described previously [39].
Functional MRI acquisition, preprocessing, and analysis
Acquisition and preprocessing
Our functional MRI acquisition and preprocessing followed standardized published protocols [40, 41]. T2* functional data were acquired with a 3-Tesla scanner (Gyroscan Intera 3 T, Philips Medical Systems, Best, NL) using a single-shot echo planar sequence, with parameters selected to minimize distortion in the region of central interest, while retaining an adequate signal-to-noise ratio (S/N) and T2* sensitivity. Volumes consisting of 34 slices were acquired (matrix 64 × 64, resolution 3.6 mm × 3.6 mm × 3.6 mm; TR = 2.1 s, TE = 30 ms, FA = 90°). The slices were tilted by 25° from the AC/PC line in order to minimize drop-out artifacts in the mediotemporal and orbitofrontal regions. Importantly, the fMRI signal is based on the blood oxygenation level dependent (BOLD) response, reflecting changes in blood flow that follow changes in neural activity. Therefore, fMRI can be seen as indirect measurement of neural activity.
Data were analyzed using statistical parametric mapping software (SPM8, Welcome Department of Cognitive Neurology, London, UK; http://www.fil.ion.ucl.ac.uk/spm). Functional data were preprocessed, including realignment, unwarping, and spatial normalization of each participant’s functional images to the Montreal Neurological Institute International Consortium for Brain Mapping template. Images were smoothed with a Gaussian kernel of 6 mm full-width at half-maximum.
First-level analyses
The onsets and durations of the experimental conditions (reward, loss, control) were modeled by using a canonical hemodynamic response function in the context of a GLM, and the model was corrected for serial correlations. A high-pass filter of 128 s was used to remove low-frequency noise. For each subject, two contrast images were generated in each individual first-level analysis (reward > control, loss > control) in order to investigate our research objective.
Statistical analysis
First-level analyses: fMRI
To investigate the effects of AEA and 2-AG baseline concentrations on brain functional reward outcome processing, separate ANCOVAs were calculated using a full factorial model, with condition (reward > control, loss > control), AEA and 2-AG concentrations as independent variables, and brain function as dependent variable. Gender and age were included in all models as covariates. First, whole-brain analyses were conducted in order to investigate potential interaction effects and main effects. Given the study’s primary focus on the reward system, additional region of interest analyses were performed on the bilateral putamen, substantia nigra, and hippocampus as defined by Tzourio-Mazoyer et al. [42] using an anatomical mask created with the Wake Forest University Pick Atlas [43]. Significance thresholds for multiple testing were obtained at the cluster-level by threshold-free cluster enhancement as a non-parametric approach, which is implemented in the TFCE-toolbox (http://dbm.neuro.uni-jena.de/tfce, Version 164). We consequently established a conservative FWE-corrected threshold of P < 0.05 obtained by 5000 permutations per test. For each subject the mean contrast values (of BOLD signals) of significant clusters were extracted from SPM and further analyzed in SPSS Statistics (version 25; IBM Corporation).
Second-level analyses: associations between AEA, 2-AG, and personality trait reward dependence
In order to investigate associations between endocannabinoid concentrations, reward dependence, and anhedonia, regression analyses were conducted for AEA and 2-AG on TPQ-RD and SASPAS scores for the whole sample. Exploratory analyses were carried out separating the sample by gender (n = 12 females, n = 16 males). All correlation analyses were performed using Spearman’s rho due to non-normality distributions (AEA = Kolmogorov–Smirnov(df = 26) = 0.149, P = 0.14, Shapiro–Wilk(df = 26) = 0.901, P = 0.02, 2-AG = Kolmogorov–Smirnov(df = 26) = 0.246, P < 0.01, Shapiro–Wilk(df = 26) = 0.677, P < 0.01). Additionally, in order to assess the potential influence of subclinical depressiveness and anxiety, the Hamilton Depression Rating Scale (HAM-D, [33]) and Hamilton Anxiety Rating Scale (HAM-A, [34, 35]) were used as clinical rating, and associated with AEA and 2-AG concentrations using partial correlations controlling for gender.
Results
Subjects
The present study comprised 30 right-handed healthy adults (n = 12 females and n = 18 males). Subjects were on average 24.13 years old (SEM + 0.56) and had an average BMI of 21.84 kg/m2 (SEM + 0.31). Subjects consumed 0.9 (SEM + 0.15) cups of coffee per day and 3.29 (SEM + 0.41) alcoholic drinks per week. None of the subjects used nicotine or illegal drugs including THC. On average, subjects had been educated for 16.65 years (SEM + 0.47). AEA concentrations in females were significantly higher than in males (T(df = 27) = 5.21, P < 0.01), whereas 2-AG concentrations were not different in females and males (P = 0.38). Finally, AEA and 2-AG concentrations were not associated with age, education, BMI, caffeine, and alcohol consumption. For technical reasons, 2-AG concentrations of three subjects could not be evaluated. Due to incomplete TPQ questionnaires/missing items 28 subjects were included for TPQ results.
AEA, 2-AG, and brain activation during reward outcome
Behavioral data
The post hoc analysis of the reaction times revealed significantly faster reaction times for the control condition (M = 719.5 ms, SD = 218.6 ms) compared to the reward condition (M = 887.12 ms, SD = 218.82 ms, P < 0.001) and the loss condition (M = 873.77 ms, SD = 139.01 ms, P = 0.004). The reward condition and the loss condition did not significantly differ (P = 0.61). The analysis of reaction times yielded neither an association with 2-AG (P > 0.25), AEA (P > 0.21) nor fMRI BOLD signal during reward outcome (P > 0.11).
Effects of condition
The whole-brain analysis of the AEA by condition model yielded a significant main effect of condition in the three large clusters resulting from an overall increased brain reactivity in the reward condition compared to the loss condition, comprising large parts within the cerebellum including the vermis extending to the middle temporal gyrus and the fusiform gyrus (x = −44, y = −16, z = 58, TFCE(1, 54) = 2253.64, k = 11001, PFWE = 0.006), putamen and caudate nucleus extending to the orbitofrontal gyrus and the hippocampus (x = 12, y = −50, z = −20, TFCE(1, 54) = 2057.08, k = 5540, PFWE = 0.008), and pre- and postcentral gyrus extending to the inferior and superior parietal gyrus, the precuneus and the middle occipital gyrus (x = 12, y = −8, z = −12, TFCE(1, 54) = 1293.13, k = 2415, PFWE = 0.022). In addition, basic activation pattern for the contrasts reward > control and loss > control can be found at Supplementary Table 1 (controlled for age and sex) and Supplementary Table 2 (controlled for age, sex, and AEA concentration).
Effects of AEA
Furthermore, the whole-brain analysis revealed a significant positive main effect of AEA concentrations on brain function in five clusters comprising several areas, namely prefrontal areas comprising the precentral gyrus, the inferior and middle frontal gyrus (cluster 1: x = 30, y = 6, z = 30, TFCE(1, 54) = 1766.90, k = 444, PFWE = 0.004), the middle cingulate gyrus extending to the supramarginal gyrus and thalamus (cluster 2: x = 28, y = −28, z = 24, TFCE(1, 54) = 1663.54, k = 1043, PFWE = 0.004), the bilateral precuneus extending to the paracentral lobuli (cluster 3: x = −18, y = −50, z = 46, TFCE(1, 54)=1565.80, k = 759, PFWE = 0.004), the insula and the putamen (cluster 4: x = 36, y = 8, z = 0, TFCE(1, 54)=1564.59, k = 149, PFWE = .004), and the bilateral thalamus extending to the hippocampus (cluster 5: x = −22, y = −20, z = 6, TFCE(1, 54) = 1538.87, k = 224, PFWE = 0.004; cluster 6: x = 2, y = −34, z = 12, TFCE(1, 54) = 1534.62, k = 185, PFWE = 0.004).
Interaction effects
The region of interest analysis of the interaction revealed a significant interaction effect of AEA concentrations by condition (positive vs. negative) within the putamen (x = 26, y = 16, z = −8, TFCE(1, 54) = 771.68, k = 70, PFWE = 0.044), resulting from an increased putamen activity in reaction to rewarding stimuli in subjects with higher AEA concentrations while this association was absent in the loss condition (Fig. 1).

Right: Scatter plot depicting the association of estimated contrast values (of BOLD signals) of the resulting cluster during the reward condition and AEA concentrations. Error bars (±2 SE). fMRI functional magnetic resonance imaging, AEA anandamide, BOLD blood oxygenation level dependent.
The analyses of the 2-AG full factorial model yielded no significant associations, neither on whole-brain level, nor for the region of interest analyses.
2-AG, AEA, and TPQ reward dependency
The analysis of AEA and 2-AG concentrations and TPQ-RD scores revealed a significant negative correlation between AEA concentrations and TPQ-RD scores (rspearman = −0.56, P = 0.001) (Fig. 2). There was no significant correlation between 2-AG and TPQ-RD scores (rspearman = −0.29, P = 0.073).

The scatter plot shows a significant negative correlation between AEA concentrations and TPQ-RD scores (rspearman = −0.56, P = 0.001).
The exploratory supplementary analyses—separating the sample by gender—revealed a significant negative correlation between AEA concentrations and TPQ-RD scores in females (rspearman = −0.64, P = 0.013) but not in males (rspearman = −0.13, P = 0.315) (Supplementary Fig. 1). Removing the potential outlier (female, TPQ-RD = 12, AEA = 1.84) slightly reduces the significance (rspearman = −0.53, P = 0.046). The 2-AG analysis yielded a significant negative correlation between 2-AG concentrations and TPQ-RD scores in males (rspearman = −0.44, P = 0.049) but not in females (rspearman = −0.39, P = 0.119). The additional analysis of subclinical depressiveness and anxiety yielded show neither a significant associations between HAM-D (r = −0.27, P = 0.098) nor HAM-A (r = −0.11, P = 0.31) with AEA concentrations.
2-AG, AEA, and anhedonia
The analysis of the SASPAS scales for social and physical anhedonia additionally revealed a positive association of AEA concentrations and social anhedonia (r = 0.37, P = 0.034), and a positive trend for physical anhedonia (r = 0.25, P = 0.088) whereby the SASPAS scores were negatively associated with TPQ-RD scores (r = −0.51, P = 0.003), with social anhedonia (r = −0.64, P < 0.001) as strongest predictor. The SASPAS scores were strongly negatively associated with reward sensitivity of the TPQ (r = 0.754, P < 0.001).
Discussion
This is the first human study examining the relationship between of peripheral eCB concentrations and reward-related brain function, and reward dependence in a sample of healthy subjects. The findings of this study revealed (1) that basal AEA concentrations were positively correlated with putamen activity to rewarding stimuli, and (2) that basal AEA concentrations were negatively correlated with the personality measure reward dependence. Additionally, a main effect of AEA concentrations was found showing a positive association between AEA concentrations and widespread brain activation, e.g., comprising prefrontal areas, the putamen, and the bilateral thalamus extending to the hippocampus, independently from condition. No relationships were detected between 2-AG concentrations and brain reward function.
Our finding that basal AEA concentrations were positively correlated with increased brain functional activity within the putamen after reward was in line with our primary hypothesis and suggests the eCB system may relate to neuronal reward outcome processing in humans. In line with these suggestions, activity of the putamen has been found to be positively associated with reward-related learning [44], with prediction error during reward-related learning [1] and motivation to learn [45]. CB1Rs are densely present in the putamen [46,47,48,49] on neurons positive for D1 and D2 receptors [50, 51] and glutamatergic terminals [52]. The AEA hydrolyzing enzyme FAAH is also expressed in the striatum and in projection areas [53]. Thus, AEA may be able to modulate information processed in the putamen by influencing and enhancing dopaminergic inputs from important mesocorticolimbic structures such as the VTA [54, 55], the substantia nigra [56, 57], and glutamatergic afferents of the prefrontal cortex [52]. The eCB system might significantly influence the neural activity of the putamen via AEA acting on CB1Rs and therefore fine-tune in particular motivational processes and learning in reward-related processes. Reward presentation might result in higher dopamine release and more positive reward perception mediated by basal AEA signaling. In line with these suggestions, 385A carriers of the functional FAAH C385A single nucleotide polymorphism, associated with reduced enzyme and possibly increased eCB signaling, show a positive correlation between ventral striatal reactivity and reward, and between ventral striatal reactivity and delay discounting, an index of impulsivity [58]. Childs et al. [59] showed acute administration of delta-9-tetrahydrocannabinol to dampen negative emotional processing and fMRI BOLD cortico-limbic responses to social threat [60, 61]. Another study [62] showed that 3-day-abstinent regular marijuana users, carrying the 385C allele of the functional FAAH C385A single nucleotide polymorphism which is associated with lower peripheral AEA [63], exhibited greater activation in widespread areas within the reward circuits in response to a marijuana cue-elicited craving paradigm using fMRI. As acutely craving marijuana users instead of healthy adults were investigated and a cue-elicited craving paradigm instead of a monetary reward paradigm was used, the result is not in contrast to our results.
The second finding of this study was that basal AEA concentrations were negatively correlated with the personality measure reward dependence. The finding stands in contrast to our primary hypothesis, which could be because of several reasons. Our original hypothesis as regards the TPQ was based on the literature in patients (or people at risk of) psychiatric disorders, where low reward dependence is usually associated as a risk personality profile [64,65,66]. In fact, the present study did not investigate patients with psychiatric disorders and the sample only comprised young healthy subjects, showing a “normal” variance of reward dependence, far away from “pathological scores”. It cannot be ruled out that healthy controls even show a divergent pattern of the reported associations compared to patient populations. Although speculative, it might be that healthy subjects with high reward dependence scores are constantly in need of (and seek) social reward because of low AEA levels and a less hedonic neural reward (lower striatal response to monetary reward, respectively) in order to reach hedonic experience and to sustain higher degrees of well-being. There remains an urgent need for studies investigating the relationship in patients with psychiatric disorders and compare them with a healthy control sample to address this hypothesis, to either find support/evidence or counterevidence for this interpretation. Furthermore, human studies are required to determine long-term environmental or genetic influences on individual basal AEA concentrations and their impact on brain function, such as chronic stress [67] or CB1R gene (CNR1) [68], and FAAH gene variations [58].
Secondly, it might be that the monetary reward task used is less appropriate for investigating neural reward functions associated with the personality construct reward dependence. Although social reward (TPQ-RD) differs from monetary reward (task), fMRI studies show that rewarding stimuli of social and monetary reward share common neural correlates in brain functional activity, especially within the ventral striatum, which has repeatedly shown to be activated not only during monetary reward processing [69,70,71], but also during social reward processing such as while watching beautiful faces [72] and during social cooperation [73]. However, there remain differences between monetary and social rewards in secondary reward-related neural activity, e.g., in higher cortical areas. Therefore, future studies should address this, investigating endocannabinoids in humans using a specific social reward task.
Thirdly, the exploratory analysis of gender showed a slightly stronger association in females than in males, although the direction of associations with TPQ-RD scores were present in both genders. Owing to small subsample-sample sizes and being rather exploratory in nature, these results might provide a good basis for hypotheses for future studies that aim to directly address gender effects in larger samples.
Regarding 2-AG concentrations, we did neither find associations with reward dependence nor brain function. The absence of a relationship may be due to the relatively small sample. Also, there was a higher individual variability in 2-AG concentrations in this study possibly masking potential associations between brain activity after reward presentation and 2-AG. Several studies with humans also reported stronger associations between AEA compared to 2-AG with different outcome measures such as acute stress response [22], affect regulation [38], depression [21], or hedonic eating in binge eating disorder [74].
The well characterized sample is a strength of the study. We used validated outcome measures and standardized BMI, physical activity, and time of the day. All subjects had no history of psychiatric disorders and did not use any drugs or medication. All these factors are known to possibly affect concentrations of circulating eCBs [19]. In summary, the findings provide first insights into the associations between eCBs system, neural reward outcome processing, and personality factors in healthy humans and could provide a valuable contribution for the development and the potential use of endocannabinoid associated therapeutic targets.
However, there are important limitations of the study. First, our sample was relatively small. The sample was also demographically homogeneous, as we controlled for confounding variables related to age, weight, psychiatric symptomatology, and prior drug use. However, larger replication studies—potentially including more heterogeneous samples—are needed, ideally including different subgroups of subjects. Particularly, the supplementary gender sub-analyses are based on small sample sizes and should therefore be regarded with caution. Second, the present study did not control for previous trauma or current life event, both of which are thought to influence the eCB system [67]. Third, only one-time MRI and blood samples were obtained to measure basal AEA concentrations. Repeated blood sample assessments may provide a more realistic estimate of individual differences in basal concentrations, and provide novel information about the sensitivity of the concentrations to environmental factors (e.g., the task or the scan procedure). Fourth, we neither obtained a second reward paradigm nor a second reward questionnaire and the MRI scan and blood draw were obtained at two study visits within 7 days due to larger study protocols. Although paradigm-based functional MRI, in general, is sometimes criticized in terms of retest reliability [75], using standardized MRI acquisitions at similar daytimes followed by standardized preprocessing of imaging data, may help increase the reliability [76]. Furthermore, the use of block designs (vs. event-related designs) and a robust and standardized task further improves the reliability. In addition, there is evidence that basal serum endocannabinoid concentrations are relatively stable and reproducible at least within 7 days without any life events occurring during this period. A previous study [22] used a similar study protocol to ours with subjects undergoing two highly standardized visits in randomized order within 7 days. Subjects did not show significant differences in baseline AEA (general linear model with repeated measures: P = 0.633, F(1, 68) = 0.23) and 2-AG (general linear model with repeated measures: P = 0.509, F(1, 69) = 0.44) concentrations between both visits. There was no significant association between visit order and baseline AEA and 2-AG concentrations. Supplementary Figure 2 provides descriptive scatterplots for both visits. There was a significant correlation between baseline AEA concentrations of visit 1 and 2 (Pearson’s correlation, two-sided, P = 0,01) shown in the scatter plot in Supplementary Fig. 3.
These results highly suggest that AEA concentrations are stable and reproducible under standardized circumstances within 7 days and can be related to standardized fMRI and questionnaire data acquired at a different time.
Finally, although there is a certain overlap in neural brain function—particularly in the primary reward system—the fMRI task primarily investigates monetary, while the TPQ scale reward dependence rather characterizes social reward and, so, do not completely one another. Future studies are required that applying a social reward paradigm.
In conclusion, this is the first human study providing evidence that the eCB system is a possible modulator of brain functional reward processing during outcome phase, and of the personality trait reward dependence in healthy subjects. Our findings are consistent with preclinical evidence in animals [5, 28, 29, 31, 77]. Future studies are needed to characterize the nature of the endocannabinoids influence and response, including its time course and associations with different forms of reward. It will be important to use other outcome measures such as behavioral measures and genetic or epigenetic analyses to better understand the physiological role of the eCBs and to determine their potential in psychiatric treatment.
Funding and disclosure
This research was supported by grants from the Innovative Medizinische Forschung (IMF) at the University of Muenster (I-DL111019 to AD, RE111604 to RR, and RE111722 to RR), by the German Research Foundation (DFG, grant FOR2107 DA1151/5–1 and DA1151/5–2 to UD; SFB-TRR58, Projects C09 and Z02 to UD) and the Interdisciplinary Center of Clinical Research (IZKF) of the Medical Faculty of Muenster (grant Dan3/012/17 to UD). The authors declare no competing interests.
References
Schultz W, Dayan P, Montague PR. A neural substrate of prediction and reward. Science. 1997;275:1593–9.
Haber SN. Neuroanatomy of reward: a view from the ventral striatum. 2011.
Parsons LH, Hurd YL. Endocannabinoid signalling in reward and addiction. Nat Rev Neurosci. 2015;16:579–94.
Bloomfield MAP, Ashok AH, Volkow ND, Howes OD. The effects of Δ9-tetrahydrocannabinol on the dopamine system. Nature. 2016;539:369–77.
Solinas M, Justinova Z, Goldberg SR, Tanda G. Anandamide administration alone and after inhibition of fatty acid amide hydrolase (FAAH) increases dopamine levels in the nucleus accumbens shell in rats. J Neurochem. 2006;98:408–19.
Solinas M, Scherma M, Tanda G, Wertheim CE, Fratta W, Goldberg SR. Nicotinic facilitation of delta9-tetrahydrocannabinol discrimination involves endogenous anandamide. J Pharm Exp Ther. 2007;321:1127–34.
Kano M, Ohno-Shosaku T, Hashimotodani Y, Uchigashima M, Watanabe M. Endocannabinoid-mediated control of synaptic transmission. Physiol Rev. 2009;89:309–80.
Melis M, Pistis M. Hub and switches: endocannabinoid signalling in midbrain dopamine neurons. Philos Trans R Soc Lond B Biol Sci. 2012;367:3276–85.
Trezza V, Baarendse PJJ, Vanderschuren LJMJ. The pleasures of play: pharmacological insights into social reward mechanisms. Trends Pharm Sci. 2010;31:463–9.
Silvestri C, Di Marzo V. The endocannabinoid system in energy homeostasis and the etiopathology of metabolic disorders. Cell Metab. 2013;17:475–90.
Panagis G, Mackey B, Vlachou S. Cannabinoid regulation of brain reward processing with an emphasis on the role of CB1 receptors: a step back into the future. Front Psychiatry. 2014;5:92.
Suzanne N, Haber BK. The reward circuit linking primate anatomy and imaging. Neuropsychopharmacol Rev. 2010;35:4–26.
Oldham S, Murawski C, Fornito A, Youssef G, Yücel M, Lorenzetti V. The anticipation and outcome phases of reward and loss processing: a neuroimaging meta-analysis of the monetary incentive delay task. Hum Brain Mapp. 2018;39:3398–418.
Liu X, Hairston J, Schrier M, Fan J. Common and distinct networks underlying reward valence and processing stages: a meta-analysis of functional neuroimaging studies. Neurosci Biobehav Rev. 2011;35:1219–36.
Wood JT, Williams JS, Pandarinathan L, Courville A, Keplinger MR, Janero DR, et al. Comprehensive profiling of the human circulating endocannabinoid metabolome: clinical sampling and sample storage parameters. Clin Chem Lab Med. 2008;46:1289–95.
Côté M, Matias I, Lemieux I, Petrosino S, Alméras N, Després J-P, et al. Circulating endocannabinoid levels, abdominal adiposity and related cardiometabolic risk factors in obese men. Int J Obes (Lond). 2007;31:692–9.
Di Marzo V, Bisogno T, De Petrocellis L, Melck D, Orlando P, Wagner JA, et al. Biosynthesis and inactivation of the endocannabinoid 2-arachidonoylglycerol in circulating and tumoral macrophages. Eur J Biochem. 1999;264:258–67.
McCarron RM, Chen Y, Tomori T, Strasser A, Mechoulam R, Shohami E, et al. Endothelial-mediated regulation of cerebral microcirculation. J Physiol Pharmacol. 2006;57(Suppl 1):133–44.
Hillard CJ. Circulating endocannabinoids: from whence do they come and where are they going? Neuropsychopharmacology. 2018;43:155–72.
Hillard CJ, Weinlander KM, Stuhr KL. Contributions of endocannabinoid signaling to psychiatric disorders in humans: genetic and biochemical evidence. Neuroscience. 2012;204:207–29.
Hill MN, Miller GE, Ho W-SV, Gorzalka BB, Hillard CJ. Serum endocannabinoid content is altered in females with depressive disorders: a preliminary report. Pharmacopsychiatry. 2008;41:48–53.
Dlugos A, Childs E, Stuhr KL, Hillard CJ, de Wit H. Acute stress increases circulating anandamide and other N-acylethanolamines in healthy humans. Neuropsychopharmacology. 2012;37:2416–27.
Klein C, Hill MN, Chang SCH, Hillard CJ, Gorzalka BB. Circulating endocannabinoid concentrations and sexual arousal in women. J Sex Med. 2012;9:1588–601.
Forbes EE, Hariri AR, Martin SL, Silk JS, Moyles DL, Fisher PM, et al. Altered striatal activation predicting real-world positive affect in adolescent major depressive disorder. Am J Psychiatry. 2009;166:64–73.
Redlich R, Dohm K, Grotegerd D, Opel N, Zwitserlood P, Heindel W, et al. Reward processing in unipolar and bipolar depression: a functional MRI study. Neuropsychopharmacology. 2015;40:2623–31.
Cloninger CR, Przybeck TR, Svrakic DM. The Tridimensional Personality Questionnaire: U.S. normative data. Psychol Rep. 1991;69:1047–57.
Bajraktarov S, Gudeva-Nikovska D, Manuševa N, Arsova S. Personality characteristics as predictive factors for the occurrence of depressive disorder. Open Access Maced J Med Sci. 2017;5:48–53.
Burgdörfer G, Hautzinger M. Physische und soziale Anhedonie. Eur Arch Psychiatry Neurol Sci. 1987:223–9.
Chapman LJ, Chapman JP, Raulin ML. Scales for physical and social anhedonia. J Abnorm Psychol. 1976;85:374–82.
Der-Avakian A, Markou A. The neurobiology of anhedonia and other reward-related deficits. Trends Neurosci. 2012;35:68–77.
Wacker J, Dillon DG, Pizzagalli DA. The role of the nucleus accumbens and rostral anterior cingulate cortex in anhedonia: Integration of resting EEG, fMRI, and volumetric techniques. Neuroimage. 2009;46:327–37.
Wittchen H-U, Wunderlich U, Gruschwitz S, Zaudig M. Strukturiertes Klinisches Interview für DSM-IV. Goettingen: Hogrefe; 1997.
Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry. 1960;23:56–62.
Maier W, Buller R, Philipp M, Heuser I. The Hamilton Anxiety Scale: reliability, validity and sensitivity to change in anxiety and depressive disorders. J Affect Disord. 1988;14:61–8.
Hamilton M. The assessment of anxiety states by rating. British J Med Psychol. 1959;3:50–5.
Forbes EE, Brown SMM, Kimak M, Ferrell REE, Manuck SBB, Hariri AR, et al. Genetic variation in components of dopamine neurotransmission impacts ventral striatal reactivity associated with impulsivity. Mol Psychiatry. 2009;14:60–70.
Opel N, Redlich R, Grotegerd D, Dohm K, Haupenthal C, Heindel W, et al. Enhanced neural responsiveness to reward associated with obesity in the absence of food-related stimuli. Hum Brain Mapp. 2015;36:2330–7.
Coccaro EF, Hill MN, Robinson L, Lee RJ. Circulating endocannabinoids and affect regulation in human subjects. Psychoneuroendocrinology. 2018;92:66–71.
Hermanson DJ, Hartley ND, Gamble-George J, Brown N, Shonesy BC, Kingsley PJ, et al. Substrate-selective COX-2 inhibition decreases anxiety via endocannabinoid activation. Nat Neurosci. 2013;16:1291–8.
Redlich R, Stacey D, Opel N, Grotegerd D, Dohm K, Kugel H, et al. Evidence of an IFN-gamma by early life stress interaction in the regulation of amygdala reactivity to emotional stimuli. Psychoneuroendocrinology. 2015;62:166–73.
Redlich R, Grotegerd D, Opel N, Kaufmann C, Zwitserlood P, Kugel H, et al. Are you gonna leave me? Separation anxiety is associated with increased amygdala responsiveness and volume. Soc Cogn Affect Neurosci. 2015;10:278–84.
Tzourio-Mazoyer N, Landeau B, Papathanassiou D, Crivello F, Etard O, Delcroix N, et al. Automated anatomical labeling of activations in SPM using a macroscopic anatomical parcellation of the MNI MRI single-subject brain. Neuroimage. 2002;15:273–89.
Maldjian JA, Laurienti PJ, Kraft RA, Burdette JH. An automated method for neuroanatomic and cytoarchitectonic atlas-based interrogation of fMRI data sets. Neuroimage. 2003;19:1233–9.
Mizuno K, Kawatani J, Tajima K, Sasaki AT, Yoneda T, Komi M, et al. Low putamen activity associated with poor reward sensitivity in childhood chronic fatigue syndrome. NeuroImage Clin. 2016;12:600–6.
Watanabe Y, Evengård B, Natelson BH, Jason LA, Kuratsune H. Fatigue science for human health. New York: Springer Science + Business Media; 2008.
Herkenham M, Lynn AB, de Costa BR, Richfield EK. Neuronal localization of cannabinoid receptors in the basal ganglia of the rat. Brain Res. 1991;547:267–74.
Herkenham M, Lynn AB, Johnson MR, Melvin LS, de Costa BR, Rice KC. Characterization and localization of cannabinoid receptors in rat brain: a quantitative in vitro autoradiographic study. J Neurosci. 1991;11:563–83.
Herkenham M, Lynn AB, Little MD, Johnson MR, Melvin LS, de Costa BR, et al. Cannabinoid receptor localization in brain. Proc Natl Acad Sci USA. 1990;87:1932–6.
Tsou K, Brown S, Sañudo-Peña MC, Mackie K, Walker JM. Immunohistochemical distribution of cannabinoid CB1 receptors in the rat central nervous system. Neuroscience. 1998;83:393–411.
Hermann H, Marsicano G, Lutz B. Coexpression of the cannabinoid receptor type 1 with dopamine and serotonin receptors in distinct neuronal subpopulations of the adult mouse forebrain. Neuroscience. 2002;109:451–60.
Robbe D, Kopf M, Remaury A, Bockaert J, Manzoni OJ. Endogenous cannabinoids mediate long-term synaptic depression in the nucleus accumbens. Proc Natl Acad Sci USA. 2002;99:8384–8.
Fitzgerald ML, Shobin E, Pickel VM. Cannabinoid modulation of the dopaminergic circuitry: implications for limbic and striatal output. Prog Neuropsychopharmacol Biol Psychiatry. 2012;38:21–9.
Egertová M, Giang DK, Cravatt BF, Elphick MR. A new perspective on cannabinoid signalling: complementary localization of fatty acid amide hydrolase and the CB1 receptor in rat brain. Proc Biol Sci. 1998;265:2081–5.
Riegel AC, Lupica CR. Independent presynaptic and postsynaptic mechanisms regulate endocannabinoid signaling at multiple synapses in the ventral tegmental area. J Neurosci. 2004;24:11070–8.
Szabo B, Siemes S, Wallmichrath I. Inhibition of GABAergic neurotransmission in the ventral tegmental area by cannabinoids. Eur J Neurosci. 2002;15:2057–61.
Melis M, Gessa GL, Diana M. Different mechanisms for dopaminergic excitation induced by opiates and cannabinoids in the rat midbrain. Prog Neuropsychopharmacol Biol Psychiatry. 2000;24:993–1006.
Szabo B, Wallmichrath I, Mathonia P, Pfreundtner C. Cannabinoids inhibit excitatory neurotransmission in the substantia nigra pars reticulata. Neuroscience. 2000;97:89–97.
Hariri AR, Gorka A, Hyde LW, Kimak M, Halder I, Ducci F, et al. Divergent effects of genetic variation in endocannabinoid signaling on human threat- and reward-related brain function. Biol Psychiatry. 2009;66:9–16.
Childs E, Lutz JA, de Wit H. Dose-related effects of delta-9-THC on emotional responses to acute psychosocial stress. Drug Alcohol Depend. 2017;177:136–44.
Phan KL, Angstadt M, Golden J, Onyewuenyi I, Popovska A, de Wit H. Cannabinoid modulation of amygdala reactivity to social signals of threat in humans. J Neurosci. 2008;28:2313–9.
Rabinak CA, Sripada CS, Angstadt M, de Wit H, Phan KL. Cannabinoid modulation of subgenual anterior cingulate cortex activation during experience of negative affect. J Neural Transm. 2012;119:701–7.
Filbey FM, Schacht JP, Myers US, Chavez RS, Hutchison KE. Individual and additive effects of the CNR1 and FAAH genes on brain response to marijuana cues. Neuropsychopharmacology. 2010;35:967–75.
Mayo LM, Asratian A, Lindé J, Holm L, Nätt D, Augier G, et al. Protective effects of elevated anandamide on stress and fear-related behaviors: translational evidence from humans and mice. Mol Psychiatry. 2018. https://doi.org/10.1038/s41380-018-0215-1.
Farmer A, Mahmood A, Redman K, Harris T, Sadler S, McGuffin P. A sib-pair study of the temperament and character inventory scales in major depression. Arch Gen Psychiatry. 2003;60:490–6.
Kampman O, Poutanen O. Can onset and recovery in depression be predicted by temperament? A systematic review and meta-analysis. J Affect Disord. 2011;135:20–7.
Takahashi M, Shirayama Y, Muneoka K, Suzuki M, Sato K, Hashimoto K. Personality traits as risk factors for treatment-resistant depression. PLoS ONE. 2013;8:e63756.
Hill MN, Bierer LM, Makotkine I, Golier JA, Galea S, McEwen BS, et al. Reductions in circulating endocannabinoid levels in individuals with post-traumatic stress disorder following exposure to the World Trade Center attacks. Psychoneuroendocrinology. 2013;38:2952–61.
Domschke K, Dannlowski U, Ohrmann P, Lawford B, Bauer J, Kugel H, et al. Cannabinoid receptor 1 (CNR1) gene: impact on antidepressant treatment response and emotion processing in major depression. Eur Neuropsychopharmacol. 2008;18:751–9.
Delgado MR, Nystrom LE, Fissell C, Noll DC, Fiez JA. Tracking the hemodynamic responses to reward and punishment in the striatum. J Neurophysiol. 2000;84:3072–7.
Elliott R, Friston KJ, Dolan RJ. Dissociable neural responses in human reward systems. J Neurosci. 2000;20:6159–65.
Knutson B, Adams CM, Fong GW, Hommer D. Anticipation of increasing monetary reward selectively recruits nucleus accumbens. J Neurosci. 2001;21:1–5.
Aharon I, Etcoff N, Ariely D, Chabris CF, O’Connor E, Breiter HC. Beautiful faces have variable reward value: fMRI and behavioral evidence. Neuron. 2001;32:537–51.
Rilling JK, Gutman DA, Zeh TR, Pagnoni G, Berns GS, Kilts CD. A neural basis for social cooperation. Neuron. 2002;35:395–405.
Monteleone AM, Piscitelli F, Dalle Grave R, El Ghoch M, Di Marzo V, Maj M, et al. Peripheral endocannabinoid responses to hedonic eating in binge-eating disorder. Nutrients. 2017;9:1377. https://doi.org/10.3390/nu9121377.
Elliott ML, Knodt AR, Ireland D, Morris ML, Poulton R, Ramrakha S, et al. What is the test-retest reliability of common task-functional MRI measures? New empirical evidence and a meta-analysis. Psychol Sci. 2020;31:792–806.
Herting MM, Gautam P, Chen Z, Mezher A, Vetter NC. Test-retest reliability of longitudinal task-based fMRI: Implications for developmental studies. Dev Cogn Neurosci. 2018;33:17–26.
Scherma M, Masia P, Satta V, Fratta W, Fadda P, Tanda G. Brain activity of anandamide: a rewarding bliss? Acta Pharm Sin. 2019;40:309–23.
Acknowledgements
We thank Kathrin Schwarte for her skillful technical support. We offer many thanks to the participants.
Author information
Authors and Affiliations
Contributions
CR and AD have both contributed equally to the present work and should therefore both be regarded as first authors. UD and RR have supervised this work equally and should therefore both be regarded as last authors. AD, KD, VA, RR, and UD have substantially contributed to the conception and design of the work as well as the analysis and the interpretation of the data. In particular, CR but also VE and KF were involved in subject recruitment and data acquisition. DK helped with subject screening and running the study sessions. MH and SP carried out the endocannabinoid analyses. CR, AD, RR, and UD drafted and revised the work for important intellectual content. All authors gave their final approval of the version to be published and the agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Corresponding author
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Redlich, C., Dlugos, A., Hill, M.N. et al. The endocannabinoid system in humans: significant associations between anandamide, brain function during reward feedback and a personality measure of reward dependence. Neuropsychopharmacol. 46, 1020–1027 (2021). https://doi.org/10.1038/s41386-020-00870-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41386-020-00870-x
