
Abstract
Diabetes mellitus is a strong, independent risk factor for cardiovascular events, and a key determinant of the level of this risk is the degree of glucose elevation. Clinical trials have not demonstrated that lowering glucose levels in people with established, long-duration diabetes mellitus has a clear cardiovascular benefit, and one trial reported that this approach increased mortality. In individuals with recent-onset diabetes mellitus, however, control of glucose level has established benefits on diabetes-related eye disease and kidney disease (which are themselves cardiovascular risk factors), and 10 years of intensive glucose control in these patients reduces the 15–20-year risk of myocardial infarction and mortality. These observations, along with the facts that the prevalence of diabetes mellitus is growing and that people typically have the disease for 20–40 years of their lives, support the importance of controlling glucose level and preventing its progressive rise over time. Currently available evidence suggests that therapeutic efforts that target hyperglycemia early in the course of diabetes have a long-term cardiovascular benefit.
Key Points
-
Diabetes mellitus is an independent risk factor for cardiovascular disease
-
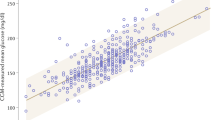
The degree of blood glucose elevation is an independent risk factor for cardiovascular disease in the general population, regardless of diabetes status
-
Completed clinical trials that examined intensive versus standard glycemic control in people with well-established diabetes mellitus have not proved whether either strategy has cardiovascular benefit
-
Intensive glycemic control in people with newly diagnosed diabetes mellitus reduces their long-term risk of cardiovascular disease
-
Several ongoing trials are assessing the effects that different agents or strategies used for lowering levels of glucose have on cardiovascular outcomes
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$209.00 per year
only $17.42 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout

Similar content being viewed by others

References
[No authors listed] Report of the expert committee on the diagnosis and classification of diabetes mellitus. Diabetes Care 20, 1183–1197 (1997).
Huxley, R., Barzi, F. & Woodward, M. Excess risk of fatal coronary heart disease associated with diabetes in men and women: meta-analysis of 37 prospective cohort studies. BMJ 332, 73–78 (2006).
Yusuf, S. et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case–control study. Lancet 364, 937–952 (2004).
Selvin, E. et al. Meta-analysis: glycosylated hemoglobin and cardiovascular disease in diabetes mellitus. Ann. Intern. Med. 141, 421–431 (2004).
Selvin, E. et al. Glycemic control and coronary heart disease risk in persons with and without diabetes: the atherosclerosis risk in communities study. Arch. Intern. Med. 165, 1910–1916 (2005).
Khaw, K. T. et al. Association of hemoglobin A1c with cardiovascular disease and mortality in adults: the European prospective investigation into cancer in Norfolk. Ann. Intern. Med. 141, 413–420 (2004).
Khaw, K. T. et al. Glycated haemoglobin, diabetes, and mortality in men in Norfolk cohort of European prospective investigation of cancer and nutrition (EPIC-Norfolk). BMJ 322, 15–18 (2001).
Gerstein, H. C. et al. The hemoglobin A1c level as a progressive risk factor for cardiovascular death, hospitalization for heart failure, or death in patients with chronic heart failure: an analysis of the Candesartan in Heart failure: Assessment of Reduction in Mortality and Morbidity (CHARM) program. Arch. Intern. Med. 168, 1699–1704 (2008).
Lawes, C. M. et al. Blood glucose and risk of cardiovascular disease in the Asia–Pacific region. Diabetes Care 27, 2836–2842 (2004).
Brunner, E. J. et al. Relation between blood glucose and coronary mortality over 33 years in the Whitehall Study. Diabetes Care 29, 26–31 (2006).
Gerstein, H. C. Epidemiologic analyses of risk factors, risk indicators, risk markers, and causal factors. The example of albuminuria and the risk of cardiovascular disease in diabetes. Endocrinol. Metab. Clin. North Am. 31, 537–551 (2002).
Action to Control Cardiovascular Risk in Diabetes Study Group et al. Effects of intensive glucose lowering in type 2 diabetes. N. Engl. J. Med. 358, 2545–2559 (2008).
ADVANCE Collaborative Group et al. Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N. Engl. J. Med. 358, 2560–2572 (2008).
Abraira, C. et al. Design of the cooperative study on glycemic control and complications in diabetes mellitus type 2: Veterans Affairs Diabetes Trial. J. Diabetes Complications 17, 314–322 (2003).
Abraira, C., Duckworth, W. C., Moritz, T. & VADT group. Glycaemic separation and risk factor control in the Veterans Affairs Diabetes Trial: an interim report. Diabetes Obes. Metab. 11, 150–156 (2008).
Duckworth, W. et al. Glucose control and vascular complications in veterans with type 2 diabetes. N. Engl. J. Med. 360, 129–139 (2009).
Holman, R. R. et al. 10-year follow-up of intensive glucose control in type 2 diabetes. N. Engl. J. Med. 359, 1577–1589 (2008).
UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet 352, 837–853 (1998).
UK Prospective Diabetes Study (UKPDS) Group. Effect of intensive blood glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34). Lancet 352, 854–865 (1998).
Selvin, E. et al. Cardiovascular outcomes in trials of oral diabetes medications: a systematic review. Arch. Intern. Med. 168, 2070–2080 (2008).
Dormandy, J. et al. Secondary prevention of macrovascular events in patients with type 2 diabetes in the Proactive Study (Prospective pioglitazone clinical trial in macrovascular events): a randomised controlled trial. Lancet 366, 1279–1289 (2005).
Home, P. D. et al. Rosiglitazone evaluated for cardiovascular outcomes—an interim analysis. N. Engl. J. Med. 357, 28–38 (2007).
Home, P. D. et al. Rosiglitazone RECORD study: glucose control outcomes at 18 months. Diabet. Med. 24, 626–634 (2007).
Milicevic, Z. et al. Hyperglycemia and its effect after acute myocardial infarction on cardiovascular outcomes in patients with type 2 diabetes mellitus (HEART2D) study design. J. Diabetes Complications 19, 80–87 (2005).
Magee, M. F., Isley, W. L. & BARI 2D Trial Investigators. Rationale, design, and methods for glycemic control in the Bypass Angioplasty Revascularization Investigation 2 Diabetes (BARI 2D) trial. Am. J. Cardiol. 97, 20G–30G (2006).
Bypass Angioplasty Revascularization Investigation 2 Diabetes Study Group. Baseline characteristics of patients with diabetes and coronary artery disease enrolled in the Bypass Angioplasty Revascularization Investigation 2 Diabetes (BARI 2D) trial. Am. Heart J. 156, 528–536 (2008).
Look Ahead Research Group et al. Baseline characteristics of the randomised cohort from the Look AHEAD (Action for Health in Diabetes) study. Diab. Vasc. Dis. Res. 3, 202–215 (2006).
Ryan, D. H. et al. Look AHEAD (Action for Health in Diabetes): design and methods for a clinical trial of weight loss for the prevention of cardiovascular disease in type 2 diabetes. Control Clin. Trials 24, 610–628 (2003).
TECOS Clinical Trial. http://www.merck.com/mrl/clinical_trials/outcomes_study.html (accessed 23 February 2009).
Origin Trial Investigators et al. Rationale, design, and baseline characteristics for a large international trial of cardiovascular disease prevention in people with dysglycemia: the ORIGIN Trial (Outcome Reduction with an Initial Glargine Intervention). Am. Heart J. 155, 26–32 (2008).
Califf, R. M. et al. Prevention of diabetes and cardiovascular disease in patients with impaired glucose tolerance: rationale and design of the Nateglinide And Valsartan in Impaired Glucose Tolerance Outcomes Research (NAVIGATOR) Trial. Am. Heart J. 156, 623–632 (2008).
Acarbose Cardiovascular Evaluation. http://www.dtu.ox.ac.uk/index.php?maindoc=/ace/overview.php (accessed 23 February 2009).
Shichiri, M., Kishikawa, H., Ohkubo, Y. & Wake, N. Long-term results of the Kumamoto Study on optimal diabetes control in type 2 diabetic patients. Diabetes Care 23 (Suppl. 2), B21–B29 (2000).
Ohkubo, Y. et al. Intensive insulin therapy prevents the progression of diabetic microvascular complications in Japanese patients with non-insulin-dependent diabetes mellitus: a randomized prospective 6-year study. Diab. Res. Clin. Pract. 28, 103–117 (1995).
Acknowledgements
H. C. Gerstein holds the McMaster University Population Health Institute Chair in Diabetes Research (sponsored by Aventis).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The author declared associations with the following companies: Bayer, GlaxoSmithKline, Merck and Sanofi-Aventis (consultant and grant/research support).
Rights and permissions
About this article
Cite this article
Gerstein, H. Is it possible to reduce cardiovascular risk with glucose-lowering approaches?. Nat Rev Endocrinol 5, 270–275 (2009). https://doi.org/10.1038/nrendo.2009.49
Issue Date:
DOI: https://doi.org/10.1038/nrendo.2009.49
This article is cited by
-
Dysglycaemia and the risk of acute myocardial infarction in multiple ethnic groups: an analysis of 15,780 patients from the INTERHEART study
Diabetologia (2010)
-
Carbohydrate biomarkers for future disease detection and treatment
Science China Chemistry (2010)
