
Abstract
We present a 31/3-year-old girl with severe Charcot–Marie–Tooth disease type 1 (Dejerine–Sottas disease), who was a compound heterozygote carrying a deletion of the whole peripheral myelin protein 22 (PMP22) and a deletion of exon 5 in the other PMP22 allele. Haplotype analyses and sequence determination revealed a 11.2 kb deletion spanning from intron 4 to 3′-region of PMP22, which was likely generated by nonhomologous end joining. Severely affected patients carrying a PMP22 deletion must be analyzed for the mutations of the other copy of PMP22.
Similar content being viewed by others

Introduction
Peripheral myelin protein 22 (PMP22) is a major constitutional protein of the peripheral myelin, mutation of which causes Charcot–Marie–Tooth disease type 1 (CMT1) or hereditary neuropathy with liability to pressure palsies. Most CMT1 patients associated with PMP22 have about 1.5 Mb duplication in chromosome 17p11.2 including PMP22; some have point mutations of PMP22 causing a gain of function (http://www.molgen.ua.ac.be/CMTMutations/default.cfm).1, 2 CMT1 is a clinically heterogeneous peripheral neuropathy. Its clinical manifestations range from slowly progressive distal muscle weakness and atrophy with late onset to severe phenotype with early onset, designated as Dejerine–Sottas disease.3, 4, 5 In contrast, hereditary neuropathy with liability to pressure palsies presents mild symptoms and is due to PMP22 haploinsufficiency.6 Most hereditary neuropathy with liability to pressure palsies patients have about 1.5 Mb deletion in chromosome 17p11.2 including PMP22 and some have PMP22 mutations leading to loss of function.7 However, when patients with PMP22 deletion have a point or deletion mutation of PMP22 on the other chromosome, they present severe symptoms.8, 9 Herein, we describe a severe CMT1 (Dejerine–Sottas disease) patient carrying a deletion of the whole PMP22 and a deletion of exon 5 in other PMP22.
Clinical report
The patient, a 31/3-year-old girl (III-1), was born by vacuum-extractor delivery at 38 weeks gestation. She showed hypotonia after neonatal period and delay in motor development: rolling over at 5 months of age, head control at 7 months and standing with support at 1 year 6 months with knees locked in hyperextension.
On physical examination at 2½ years, the patient stood with support, but could not walk without support. The musculature of the limbs was hypotonic. Deep tendon reflexes were diminished in the upper limbs and absent in the lower limbs. Cranial nerve functions and mental development was normal. Her brain magnetic resonance imaging was not remarkable. Cerebrospinal fluid examination revealed protein elevation: 74 mg 100ml−1.
Her mother (II-2) did not walk until 3 years of age and had not been good at exercise since childhood. She had frequent episodes of foot numbness, paresthesia and decrease in deep tendon reflexes of lower limbs, but with no muscle atrophy. Her maternal grandmother (I-1) also had similar symptoms. Her father (II-1) and younger brother (III-2) developed normally, reporting no subjective symptoms.
Peripheral nerve conduction velocity study revealed that the compound muscle action potential was markedly decreased in the patient and somewhat low in the mother (Supplementary Table 1). The sensory nerve action potential was not induced in the patient's median nerve and slightly reduced in the mother's median nerve. Her father showed normal results of nerve conduction velocity.
Genetic analysis
The ethics committee of the Yamagata University School of Medicine approved this study. Analyses of PMP22 dosage were performed by fluorescence in situ hybridization and multiplex ligation-dependent probe amplification.10, 11, 12, 13 Sequence of PMP22 was directly determined using genomic DNA. For determination of the haplotype and the deletion range of PMP22, small nucleotide polymorphisms and uniSTS (RH118519) were analyzed using sequencing.14
Results
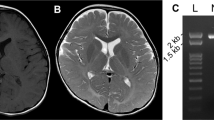
Fluorescence in situ hybridization analysis revealed a large deletion of PMP22 of the patient. Considering the severe symptoms of the patient, we analyzed other PMP22 allele and could not amply exon 5. Multiplex ligation-dependent probe amplification analysis revealed that the patient was a compound heterozygote with a deletion of the whole PMP22 and a deletion of PMP22 exon 5 on the other chromosome (Figure 1). We also confirmed that the father and mother were heterozygous for a deletion of the whole PMP22 and a deletion of PMP22 exon 5, respectively.

Multiplex ligation-dependent probe amplification analysis (MLPA) of PMP22 exons 1A–5. We developed a screening system for peripheral myelin protein 22 (PMP22) dosage using MLPA with specific probe sets (available on request) designed on the basis of genomic information. (a) Normal control; (b) proband's father; (c) proband's mother; (d) proband. Arrows indicate exons 1A–5 of PMP22. The dye signal intensity reveals only a single copy of each exon of PMP22 in the father and a single copy of exon 5 of PMP22 in the mother. The patient has a single copy of exons 1A–4 and no copy of exon 5 of PMP22.
Haplotype analyses confirmed the inheritance of each mutation and showed that the 5′-breakpoint was located between rs3785653 and RH118519, and the 3′-breakpoint was extended over the 3′-untranslated region and located between rs230936 and rs192046 (Figures 2 and 3). The sequence analysis showed that the deletion was about 11.2 kb in size, with a 4-bp overlapping sequence (microhomology) at the breakpoint.

Haplotype analysis using small nucleotide polymorphisms (SNPs). Haplotype analysis results clearly illustrate that the patient inherited a chromosome from her father in which all SNPs had been deleted and another chromosome from her mother in which the region between rs230936 and rs230938 had been deleted. The location of all SNPs is depicted in Figure 3. Open symbols represent unanalyzed persons; closed and slash symbols represent the persons carrying a deletion of the whole peripheral myelin protein 22 (PMP22) and a deletion of PMP22 exon 5, respectively.

Scheme of the structure of PMP22 and the deleted region in the patient. Exons are shown as boxes and identified by numbers above boxes. Solid black boxes and solid white boxes indicate protein coding sequences and untranslated sequences, respectively. The alternate PMP22 transcripts are tissue specific: exon 1A-containing transcripts are myelin specific and exon 1B-containing transcripts are for nonneural tissues. The breakpoint is located between rs3785653 and rs192046. The junction fragment containing the breakpoint was sequenced after amplifying using following primers: 5′-AGCTCAGTGTCTGCCCAAAT-3′ and 5′-GCTGAGCTGTTTCGGCTTTA-3′. The 4-bp sequence in the box represents the overlapping sequence. The underlined sequences show a deleted region in the patient and her mother.
Discussion
We present a 31/3-year-old girl with severe CMT1 (Dejerine–Sottas disease), who was a compound heterozygote carrying a deletion of the whole PMP22 and a deletion of exon 5 in the other PMP22 allele. The deletion of exon 5 shows the features of nonhomologous end joining: a lack of extensive homology and the presence of microhomology at the breakpoints.14
The father was a heterozygote carrying a deletion of the whole PMP22, but he did not have any symptoms with normal nerve conduction velocity. The mother carrying exon 5 deletion had a delay in motor development and frequent episodes of pressure palsies. Nerve conduction velocity studies indicated that the mother had mild axonal damage. By RT–PCR analysis, a small amount of mRNA from exon 5 deletion allele was amplified (data not shown), suggesting that the transcription of exon 5 deletion allele would escape from nonsense-mediated decay and produce mutant PMP22. Mutant PMP22 might damage the axon in a manner of a gain of function and be associated with her symptoms. It is well known that some MPZ mutations cause axonal damage probably by the disruption of Schwann cell–axonal interactions.15 PMP22 has been suggested to interact with MPZ to enforce adhesive interactions and the mutant PMP22 might cause axonal damage through interaction with MPZ.16, 17
Recently, Al-Thihli et al.9 reported on a patient with a severe phenotype of Dejerine–Sottas disease who was a compound heterozygote with a 1.5 Mb deletion in chromosome 17p11.2 and a deletion of exons 2 and 3 of PMP22. Severely affected patients carrying a PMP22 deletion must be analyzed for the mutations of the other copy of PMP22. Multiplex ligation-dependent probe amplification analysis is an easy and suitable detection method for a partial or whole deletion of PMP22.
References
Lupski, J. R., de Oca-Luna, R. M., Slaugenhaupt, S., Pentao, L., Guzzetta, V., Trask, B. J. et al. DNA duplication associated with Charcot–Marie–Tooth disease type 1A. Cell 66, 219–232 (1991).
Roa, B. B., Garcia, C. A., Suter, U., Kulpa, D. A., Wise, C. A., Mueller, J. et al. Charcot–Marie–Tooth disease type 1A. Association with a spontaneous point mutation in the PMP22 gene. N. Engl. J. Med. 329, 96–101 (1993).
Dyck, P. J., Chance, P., Lebo, R. & Carney, J. A. Hereditary motor and sensory neuropathies. in Peripheral Neuropathy (eds. Dyck P. J., Thomas P. K., Griffin J. W., Low P. A. & Poduslo J. F.) 1096–1136 (Saunders, Philadelphia, 1993).
Roa, B. B., Garcia, C. A., Pentao, L., Killian, J. M., Trask, B. J., Suter, U. et al. Evidence for a recessive PMP22 point mutation in Charcot–Marie–Tooth disease type 1A. Nat. Genet. 5, 189–194 (1993).
Roa, B. B., Dyck, P. J., Marks, H. G., Chance, P. F. & Lupskim, J. R. Dejerine–Sottas syndrome associated with point mutation in the peripheral myelin protein 22 (PMP22) gene. Nat. Genet. 5, 269–273 (1993).
Pareyson, D., Scaioli, V., Taroni, F., Botti, S., Lorenzetti, D., Solari, A. et al. Phenotypic heterogeneity in hereditary neuropathy with liability to pressure palsies associated with chromosome 17p11.2-12 deletion. Neurology 46, 1133–1137 (1996).
Chance, P. F., Alderson, M. K., Leppig, K. A., Lensch, M. W., Matsunami, N., Smith, B. et al. DNA deletion associated with hereditary neuropathy with liability to pressure palsies. Cell 72, 143–151 (1993).
Numakura, C., Lin, C., Oka, N., Akiguchi, I. & Hayasaka, K. Hemizygous mutation of the peripheral myelin protein 22 gene associated with Charcot–Marie–Tooth disease type 1. Ann. Neurol. 47, 101–103 (2000).
Al-Thihli, K., Rudkin, T., Carson, N., Poulin, C., Melançon, S. & Der Kaloustian, V. M. Compound heterozygous deletions of PMP22 causing severe Charcot–Marie–Tooth disease of the Dejerine–Sottas disease phenotype. Am. J. Med. Genet. A 146A, 2412–2416 (2008).
Patel, P. I., Roa, B. B., Welcher, A. A., Schoener-Scott, R., Trask, B. J., Pentao, L. et al. The gene for the peripheral myelin protein PMP-22 is a candidate for Charcot–Marie–Tooth disease type 1A. Nat. Genet. 1, 159–165 (1992).
Shaffer, L. G., Kennedy, G. M., Spikesm, A. S. & Lupski, J. R. Diagnosis of CMT1A duplications and HNPP deletions by interphase FISH: implications for testing in the cytogenetics laboratory. Am. J. Med. Genet. 69, 325–331 (1997).
Schouten, J. P., McElgunn, C. J., Waaijer, R., Zwijnenburg, D., Diepvens, F. & Pals, G. Relative quantification of 40 nucleic acid sequences by multiplex ligation-dependent probe amplification. Nucleic Acids Res. 30, e57 (2002).
Slater, H., Bruno, D., Ren, H., La, P., Burgess, T., Hills, L. et al. Improved testing for CMT1A and HNPP using multiplex ligation-dependent probe amplification (MLPA) with rapid DNA preparations: comparison with the interphase FISH method. Hum. Mutat. 24, 164–171 (2004).
Shaw, C. J. & Lupski, J. R. Non-recurrent 17p11.2 deletions are generated by homologous and non-homologous mechanisms. Hum. Genet. 116, 1–7 (2005).
Shy, M. E., Jani, A., Krajewski, K., Grandis, M., Lewis, R. A., Li, J. et al. Phenotypic clustering in MPZ mutations. Brain 127, 371–384 (2004).
D'Urso, D., Ehrhardt, P. & Muller, H. W. Peripheral myelin protein 22 and protein zero: a novel association in peripheral nervous system myelin. J. Neurosci. 19, 3396–3403 (1999).
Hasse, B., Bosse, F., Hanenberg, H. & Muller, H. Peripheral myelin protein 22 kDa and protein zero: domain specific trans-interactions. Mol. Cell Neurosci. 27, 370–378 (2004).
Acknowledgements
This work was supported by a Grant-in-Aid for Scientific Research from the Ministry of Education, Science, Culture and Sports of Japan and a Grant-in-Aid from the Research of Charcot–Marie–Tooth Disease from the Ministry of Health, Labour and Welfare of Japan.
Author information
Authors and Affiliations
Corresponding author
Additional information
Supplementary Information accompanies the paper on Journal of Human Genetics website
Supplementary information
Rights and permissions
About this article
Cite this article
Abe, A., Nakamura, K., Kato, M. et al. Compound heterozygous PMP22 deletion mutations causing severe Charcot–Marie–Tooth disease type 1. J Hum Genet 55, 771–773 (2010). https://doi.org/10.1038/jhg.2010.106
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/jhg.2010.106
Keywords
This article is cited by
-
Hereditary neuropathy with liability to pressure palsy (HNPP): report of a family with a new point mutation in PMP22 gene
Italian Journal of Pediatrics (2017)
-
Molecular analysis of the genes causing recessive demyelinating Charcot–Marie–Tooth disease in Japan
Journal of Human Genetics (2013)
-
The PMP22 Gene and Its Related Diseases
Molecular Neurobiology (2013)
-
Molecular diagnosis and clinical onset of Charcot–Marie–Tooth disease in Japan
Journal of Human Genetics (2011)
