
Abstract
Using an adenoviral system as a delivery mediator of therapeutic gene, we investigated the therapeutic effects of the use of combined MDR1 shRNA and human NIS (hNIS) radioiodine gene therapy in a mouse colon xenograft model. In vitro uptake of Tc-99m sestamibi was increased approximately two-fold in cells infected with an adenovirus vector that expressed MDR1 shRNA (Ad-shMDR1) and I-125 uptake was 25-fold higher in cells infected with an adenovirus vector that expressed human NIS (Ad-hNIS) as compared with control cells. As compared with doxorubicin or I-131 treatment alone, the combination of doxorubicin and I-131 resulted in enhanced cytotoxicity for both Ad-shMDR1- and Ad-hNIS-infected cells, but not for control cells. In vivo uptake of Tc-99m sestamibi and Tc-99m pertechnetate was twofold and 10-fold higher for Ad-shMDR1 and Ad-hNIS-infected tumors as compared with tumors infected with a control adenovirus construct that expressed β-galactrosidase (Ad-LacZ), respectively. In mice treated with either doxorubicin or I-131 alone, there was a slight delay in tumor growth as compared to mice treated with Ad-LacZ. However, combination therapy with doxorubicin and I-131 induced further significant inhibition of tumor growth as compared with mice treated with Ad-LacZ. We have shown successful therapeutic efficacy of combined MDR shRNA and hNIS radioiodine gene therapy using an adenoviral vector system in a mouse colon cancer model. Adenovirus-mediated cancer gene therapy using MDR1 shRNA and hNIS would be a useful tool for the treatment of cancer cells expressing multi-drug resistant genes.
Similar content being viewed by others


Introduction
The human sodium/iodide symporter (NIS) protein is an active iodide transporter.1 As the transfer of the NIS gene and the subsequent functional expression of NIS protein induce cancer cells to accumulate therapeutic radionuclides (I-131 and Re-188) from plasma, NIS gene transfer represents a possible type of radionuclide gene therapy. Several investigators have reported that human sodium/iodide symporter (hNIS) mediated radionuclide gene therapy would offer a potential means of cancer therapy.2, 3, 4, 5, 6
Multidrug resistance (MDR) is the most common impediment to successful chemotherapy for various cancers. Classic MDR is characterized by cross resistance to antineoplastic drugs and is caused by overexpression of the MDR1 gene that encodes P-glycoprotein (Pgp), a member of the ATP-binding cassette transporter superfamily.7 Most efforts to reverse MDR during the past decades have focused on the use of compounds that modulate Pgp activity. However, the efficiency of these drugs was difficult to assess because of inherent adverse side effects such as hypotension and heart failure. Moreover, tumor cells can acquire resistance to the applied chemosensitizer's so-called tertiary resistance.
Experimental therapeutic strategies to reverse MDR are under investigation. These strategies included gene therapeutic approaches with the use of antisense oligonucleotides, ribozymes or DNAzymes and, most recently, the application of RNA interference (RNAi) technology.8, 9 RNAi is a conserved cellular mechanism where double-stranded RNA silences the corresponding homologous gene.8, 9 Double-stranded small-interfering RNA (siRNA) molecules with a length of 19–25 nucleotides can direct degradation of eukaryotic mRNAs in a sequence-specific manner. Transient RNAi can be attained by application of siRNAs, whereas stable RNAi-mediated gene silencing can be achieved by transfection of mammalian cells with short hairpin RNA (shRNA) encoding expression cassettes that are localized on plasmid or viral vectors.
Previously, we have reported on the increased therapeutic effects of combination MDR1, shRNA and hNIS radioiodine gene therapy in human cancer cells in vitro using stable transfectants that express MDR1 shRNA for the MDR1 gene and human NIS (hNIS) gene.10 Although the in vitro study showed a therapeutic effect in a human colon cancer model, the application of our findings in a clinical setting is not straightforward. We have attempted to identity a new method to treat drug-resistance cancer effectively in vivo, which mimics the clinical situation. Among various therapeutic strategies, we have focused on the use of adenovirus-mediated therapeutic gene delivery in an in vivo cancer model. An adenoviral vector is the major delivery system commonly used for gene therapy in vivo.11, 12 The use of an adenoviral vector system has been reported to have several beneficial features as compared with other viral vector systems, such as efficient transfection in various cells including both quiescent and dividing cells, and high level expression of the gene of interest by the use of a cytomegalovirus promoter during the short term.
In this study, we have attempted to show whether adenovirus-mediated MDR1 shRNA plus hNIS gene transfer in a human colon cancer model would be potentially visualized by the use of nuclear imaging and subsequently generate strong therapeutic effects in vivo.
Materials and methods
Cells and animals
The human colon cancer cell line HCT-15 was maintained in RPMI 1640 containing 20% fetal bovine serum (Hyclone, Logan, UT) and 50 units ml–1 streptomycin/penicillin (GibcoBRL, Grand Island, NY) at 37 °C in a humidified atmosphere containing 5% CO2. Specific pathogen-free 6-week-old male BALB/c nude mice were obtained from SLC (Hamamatsu, Japan).
Construction of an adenovirus vector expressing MDR1 shRNA or hNIS gene
The shRNA sequence targeting the human MDR1 gene corresponded to the coding region at positions 79–99: 5′-AAGGAAAAGAAACCAACTGTC-3′) (GenBank accession number NM_000927). shRNA duplexes with the following sense and antisense sequences were used: 5′-TCGAGCGACAGTTGGTTTCTTTTCCGCGGCCGCAGGAAAAGAAACCAACTGTCTTTTTTCCAAA (sense) and 5′-AGCTTTTGGAAAAAAGACAGTTGGTTTCTTTTCCTGCGGCCGCGGAAAAGAAACCAACTGTCGC (antisense). All of the shRNA duplexes were synthesized by Bioneer (Daejon, Korea) and were annealed. shRNA for targeted MDR1 mRNA was cloned into the XhoI and HindIII sites of the pRNAT H1-1 vector (GenScript, Piscataway, NJ) using an adenoviral vector system.
Ad-shMDR1 is a recombinant adenovirus expressing the human MDR1 shRNA and the green fluorescent protein gene under the control of the immediate early promoter of cytomegalovirus. The shuttle pRNAT H1-1 vector was homologously recombined with pAdEasy-1 (the E1–E3 early region has been deleted) vector into electro-competent BJ5183 bacteria and was selected on kanamycin LB plates. The complete Ad-shMDR1 virus was recovered by transfection of 10 μg Pac I digested DNA into human embryonic kidney (HEK 293) cells by a lipofectamine-based procedure. Adenoviruses expressing the human NIS gene were kindly provided by Dr KH Lee. Recombinant adenoviruses encoding β-galactosidase (Ad-LacZ) were used as negative controls for the in vitro study.
All viral stocks were prepared from infected human embryonic kidney cells (HEK 293) by the use of standard procedures. After two-step purification on CsCl gradients, viral stocks were desalted by the use of G50 columns (Pharmacia, Orsay, France) and were frozen at −70 °C in PBS containing 10% glycerol. Viral titers were calculated by determination of the TCID50 or with the use of the adeno-X rapid titer kit (BD Bioscience, Palo Alto, CA). Titers are expressed as either multiplicity of infection (MOI) or as plaque forming units (PFU)/ml.
Western blotting
Cells were washed twice with PBS. Cells in cold PHI buffer (50 mM Tris-HCl (pH 8.0), 150 mM NaCl, 5 mM Na2EDTA, 0.5% NP-40, 100 μM phenylmethylsulphonyl fluoride, 1 μg ml–1 aprotinin, 1 μg ml–1 leupeptin, 1 mM DTT) were scraped from dishes and left on ice for 30 min with occasional vortexing. The lysates were cleared by centrifugation at 12 000 r.p.m. for 10 min at 4 °C. Identical amounts (40 and 80 μg of protein) of cell lysates were resolved by 8% SDS-PAGE (polyacrylamide gel electrophoreseis). Proteins were transferred to nitrocellulose membranes in transfer buffer with or without methanol and the membranes were incubated in blocking solution consisting of 5% skim milk with TBST (10 mM Tris-HCl (pH 8.0), 150 mM NaCl and 0.1% Tween 20) at room temperature for 1 h. The membranes were then immunoblotted with monoclonal anti-Pgp antibody C219 (170 kDa; Calbiochem, La Jolla, CA), monoclonal anti-NIS FP5A (90 kDa; Lab Vision, Fremont, CA), monoclonal anti-β-actin antibody (Sigma-Aldrich, St Louis, MO) and monoclonal anti-α-tubulin antibody (Sigma-Aldrich). Enzyme-linked chemiluminescence was performed to measure absorbance according to the manufacturer's protocol (ECL; Amersham Pharmacia Biotech, Piscataway, NJ). Expression of each protein was verified by exposure to X-ray film.
In vitro Tc-99m sestamibi uptake
Tc-99m sestamibi (MIBI) (Cardiolite; Bristol-Myers Squibb Medical Imaging, Columbus, OH) is a lipophilic cationic radiopharmaceutical for myocardial and cancer imaging with a gamma camera, and is believed to be transported as a common transport substrate by P-glycoportein (Pgp).13 The decreased intracellular level of substrate is because of enhanced efflux by membrane transporters,14 and reduced MIBI uptake in an MDR-expressing tumor is related to Pgp.
Cells were seeded at 1 × 106 cells per well in 6-well plates 1 day before viral infection. The Tc-99m sestamibi uptake assay was performed at 48 h after virus infection of 200 MOI of Ad-shMDR1 with or without 20 MOI of Ad-hNIS. Cells were washed once with 2 ml PBS and were then initiated by the addition of 0.1 ml PBS containing 370 kBq of Tc-99m sestamibi per well. After incubation for 30 min at 37 °C in 5% CO2, cells were washed two times with cold PBS. The radioactivity incorporated in cells was measured with a well gamma-counter (Packard Canberra, Downers Grove, IL). The radioactivity incorporated in cells was normalized for total protein, which was measured with a bicinchoninic acid protein assay (Pierce, Rockford, IL). Uptake of Tc-99m sestamibi was expressed as c.p.m. per mg protein.
I-125 uptake assay
Cells were plated at 2 × 105 cells per well in 24-well plates and iodide uptake experiments were performed at 48 h after virus infection of 200 MOI of Ad-shMDR1 with or without 20 MOI of Ad-hNIS. Cells were washed once with 1 ml HBSS and then the iodide uptake assay was initiated by the addition of 0.5 ml HBSS containing 3.7 kBq carrier-free I-125 and/or 10 μM sodium iodide (specific activity, 740 MBq mM1) per well. After incubation with I-125 for 30 min at 37 °C, cells were washed two times with cold HBSS. The radioactivity of cells was quantified with a well gamma-counter (Packard Canberra). The radioactivity of cells was normalized for total protein and I-125 uptake was expressed as c.p.m. mg–1 protein. For the inhibition study, radioiodine uptake was measured after pretreatment with 50 μM potassium perchlorate for 1 h and radioactivity incorporated in cells was measured.
In vitro cytotoxicity of doxorubicin
At 1 day before viral infection, 2 × 104 cells were seeded in 96-well plates and co-infected with both 20 MOI of Ad-shMDR1 and 200 MOI of Ad-hNIS. Infected cells were incubated at 37 °C in a humidified atmosphere containing 5% CO2 for 48 h in the presence of 0.01, 0.1, 1, 60, 250, 500 and 1000 μM doxorubicin (Sigma Aldrich). Two days after doxorubicin treatment, a 10 μl cell count solution (CCK-8; Dojindo, Tokyo, Japan) was added to the culture medium of cells treated with doxorubicin and plates were incubated at 37 °C for 4 h. Absorbance was measured at a wavelength of 450 nm using a microplate reader and cellular viability (%) was determined.
In vitro clonogenic assay
The clonogenic assay has been described previously.4 Briefly, non-infected cells or cells co-infected with both Ad-shMDR1 and Ad-hNIS were grown in a 75-cm2 flask and were incubated with either 5 ml HBSS (control) or HBSS containing 9.25 and 18.5 MBq of I-131. At 7 h after incubation with I-131, cells were washed twice with cold HBSS, trypsinized and counted. Treated cells were plated in 6-well plates 1000 (1000 cells per well) and were incubated with or without 1 or 10 μM doxorubicin at 37 °C for 1 week. Cells were then washed twice with PBS and were stained with a crystal violet solution. Colonies of more than 30 cells were counted and the results are expressed as the percentage of surviving colonies obtained after treatment with I-131 or doxorubicin or I-131 plus doxorubicin as compared with cells treated only with HBSS.
In vivo imaging of tumor-bearing mice
A total of 1 × 107 HCT-15 cells were challenged to both thighs of nude mice. When the tumor volume reached approximately 100 mm3, Ad-shMDR1 (2 × 109 PFU) and Ad-hNIS (1 × 109 PFU) were co-injected into the mouse tumors. Ad-LacZ was administered as a control. Each virus was introduced to mice by multiple injections of virus into each tumor.
Two days after viral infection, 18.5 MBq Tc-99m sestamibi or Tc-99m pertechnetate was injected into tumor-bearing mice via the tail vein. At 60 min after the injection of the radiotracer, scintigraphic imaging was acquired with the use of a multipurpose gamma camera (Infinia, GE, Milwaukee, WI) equipped with a pinhole collimator. An enhanced green fluorescent protein fluorescence image was obtained using OPtix (Advanced Research Technologies, Montreal, Canada).
In vivo animal tumor therapy
A total of 1 × 107 cells HCT-15 cells were s.c injected into both thighs of nude mice. When the diameter of tumors were approximately ⩾100 mm3 (approximately 10 days after injection), cancer therapy was started. Mice were subdivided into four groups for in vivo therapy (control mice treated with PBS only, mice treated with doxorubicin, mice treated with I-131 and mice given combination treatment with doxorubicin and I-131). For I-131 therapy, mice received a low-iodine diet with T4 supplementation in drinking water for 2 weeks to maximize radioiodine uptake in tumors and to reduce iodide uptake by the thyroid gland. Ad-shMDR1 (2 × 109 PFU) and Ad-hNIS (1 × 109 PFU) was co-injected into tumors in the left thigh (for mice that underwent therapy). Ad-LacZ as a control was administered into tumors in the right thigh (control mice). Two days later, a single injection of either 55.5 MBq I-131 or 0.5 mg kg–1 doxorubicin was i.p injected once per 3 days for 9 days. The tumor volume (length × width × height × 0.52) was measured at 3-day intervals for 21 days.
Histopathological analysis
Tumor masses were removed from mice and were preserved in 10% formalin until required. All tumor masses were embedded in paraffin, sectioned at 5 μm and were stained with hematoxylin and eosin (H&E staining).
For immunohistological analysis of Pgp and hNIS, the paraffin sections were incubated for 1 h with anti-Pgp and anti-NIS antibodies at a 1:100 and 1:50 dilution, respectively. Sections were then incubated for 30 min with a goat anti-rabbit secondary antibody conjugated to peroxidase (Immunotech, Marseille, France).
For immunohistological analysis of β-galactosidase, 5 μm cryosections were washed with 2 ml PBS at room temperature. A 5 ml solution of cell fixative (2% formaldehyde, 0.2% glutaraldehyde and 1 × PBS) was added and the slides were then washed once with PBS. Slides were incubated with X-gal staining solution for 14 h at 37 °C in the dark and were examined under a light microscope (magnification, × 200).
Statistical analysis
Data are presented as the mean±s.d. Inter-group differences were assayed using the two-tailed Student's t-test. P-values of <0.05 were considered as statistically significant.
Results
Increased uptake of Tc-99m sestamibi and I-125 in Ad-shMDR1/Ad-hNIS-infected HCT-15 cells
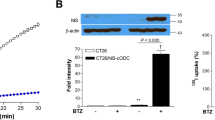
Increased human NIS protein expression was observed in Ad-hNIS-infected cells, and decreased P-glycoprotein expression was found in Ad-shMDR1-infected cells as determined by western blotting. Also, it was shown that the I-125 uptake was increased up to 25-fold higher in Ad-hNIS-infected cells as compared with non-infected cells, and specifically inhibited in the presence of potassium perchlorate (known inhibitors of hNIS function). A reduction of MDR1 gene expression was determined by RT-PCR analysis in Ad-shMDR1-infected cancer cells, as reported previously.15
The uptake of Tc-99m sestamibi was significantly increased in Ad-shMDR1 or in both Ad-shMDR1 and Ad-hNIS-infected HCT-15 cells, but not in parental cells (Figure 1a, P<0.05) and uptake was approximately two-fold higher for the use of both constructs as compared with that of the parental cells. Concurrently, I-125 uptake was 26-fold and 22-fold higher in Ad-hNIS or Ad-shMDR1/Ad-hNIS-infected HCT-15 cells, respectively, as compared with the parental cells (Figure 1b, P<0.05). I-125 uptake in Ad-hNIS-infected cells was slightly higher as compared with uptake for both Ad-hNIS and Ad-shMDR1 infected cells, but did not reach statistical significance. I-125 uptake in hNIS-expressing cells was almost completely inhibited by treatment with perchlorate, a competitive NIS inhibitor.

Functional uptake of Tc-99m sestamibi and I-125 in Ad-shMDR1 or Ad-hNIS-infected HCT-15 cells. HCT-15 cells were infected with Ad-shMDR1 (200 MOI) or Ad-shMDR1 (200 MOI) plus Ad-hNIS (20 MOI) for 48 h and were incubated with 370 kBq Tc-99m sestamibi for 30 min (a). I-125 uptake was performed in transfected HCT15 cells with Ad-hNIS (20 MOI) or Ad-hNIS (20 MOI) plus Ad-shMDR1 (100 MOI). I-125 uptake was then initiated for 30 min by the addition of 0.5 ml HBSS containing 3.7 kBq of I-125 per well and was blocked in the presence of potassium perchlorate, a known inhibitor of NIS function (b). Results are expressed as the mean of c.p.m. per protein concentration. The data shown are the means of experiments performed in triplicate. Bars represent means±s.d.; NS, not significant; *statistically significant.
In vitro treatment with doxorubicin and I-131
The survival rates of cells in the presence of 1 and 60 μM doxorubicin were significantly lower for Ad-shMDR1 or Ad-shMDR1/Ad-hNIS infected cells as compared with non-infected-parental cells (Figure 2a, P<0.05). In vitro clonogenic assays showed that viability was reduced in Ad-hNIS-infected HCT-15 cells in a dose-dependent manner, but not in parental cells; treatment with 37 MBq I-131 markedly decreased viability (Figure 2b, P<0.05). Subsequently, combination treatment with I-131 and doxorubicin generated more enhanced cellular cytotoxic effects in Ad-shMDR1/Ad-hNIS-infected HCT-15 cells as compared with that of control cells (Figure 3). Particularly, the highest cellular cytotoxicity was observed in cells treated with the combination of 18.5 MBq I-131 and 10 μM doxorubicin as compared with control cells (control cells and both 18.5 MBq I-131 and 10 μM doxorubicin-treated cells, 19 and 100%, respectively).

Cytotoxic effects of doxorubicin or I-131 in Ad-shMDR1 and Ad-hNIS-infected cancer cells. HCT-15 cells (infected with HBSS, 20 MOI Ad-hNIS, 200 MOI Ad-shMDR1 and both 200 MOI Ad-shMDR1 and 20 MOI Ad-hNIS) were incubated in the presence of 0, 0.01, 0.1, 1, 60, 250, 500 and 1000 μM doxorubicin for 48 h at 37 °C (a). HC-T15 cells infected with 20 MOI of Ad-hNIS were treated with 0, 9.25, 18.5 and 37.0 MBq of I-131 in HBSS or HBSS alone for 7 h. Cellular viability assessed by the use of a clonogenic assay was compared to treatment with I-131 or with HBSS alone (b). The data shown are the means of experiments performed in triplicate. Bars represent means±s.d.; NS, not significant; *statistically significant

Cellular cytotoxic effects of combined doxorubicin and I-131 in both Ad-shMDR1 and Ad-hNIS-infected HCT15 cells. HCT-15 cells were infected with both Ad-shMDR1 (200 MOI) and Ad-hNIS (20 MOI) for 48 h. At 48 h after viral infection, cells were treated with HBSS, 9.25 and 18.5 MBq of I-131 for 7 h. I-131-treated cells (1000 cells per well) were incubated with or without 1 or 10 μM doxorubicin at 37 °C for 1 week. Cells were stained with a crystal violet solution and colonies of more than 30 cells were counted. Results are expressed as the percentage of surviving colonies. The data shown are the means of experiments performed in triplicate. Bars represent means±s.d.
In vivo imaging of tumors treated with both Ad-shMDR1 and Ad-hNIS
Scintigraphic imaging revealed increased uptake of Tc-99m sestamibi in Ad-shMDR1/Ad-hNIS-infected tumors, but not in Ad-LacZ-infected tumors (Figure 4a). In addition, higher uptake of Tc-99m pertechnetate was observed in Ad-shMDR1/Ad-hNIS-infected HCT-15 tumors as compared with Ad-LacZ-infected HCT-15 tumors by the use of a gamma camera (Figure 4b). Physiological uptake of Tc-99m was seen in the thyroid and stomach expressing hNIS. Fluorescence imaging showed an enhanced green fluorescent protein signal in Ad-shMDR1/Ad-hNIS-infected tumors, but not in Ad-LacZ-infected tumors (Figure 4c).

In vivo imaging of tumor-bearing mice infected with both Ad-shMDR1 and Ad-hNIS. A total of 1 × 107 HCT-15 cells were s.c injected into both thighs of mice. When the tumor volume reached approximately 100 mm3, Ad-shMDR1 (2 × 109 PFU) and Ad-hNIS (1 × 109 PFU) were intratumorally injected into the tumor-bearing mice. Ad-LacZ as a control was intratumorally injected to tumor-bearing mice. At 2 days after virus injection, gamma camera imaging was performed to detect Tc-99m sestamibi and Tc-99m pertechnetate (a and b). A fluorescence image was obtained using the OPtix imaging system (c). Experiments were performed in triplicate; n=5 mice/group.
Immunohistological analysis of Ad-shMDR1/Ad-hNIS or Ad-LacZ-infected tumors
Immunohistological staining using anti-P-glycoprotein and anti-hNIS revealed that P-glycoprotein expression was reduced in Ad-shMDR1/Ad-hNIS-infected tumors, but not in Ad-LacZ-infected tumors (Figures 5b and e), whereas increased expression of hNIS protein was only detected in Ad-shMDR1/Ad-hNIS-infected tumors, but not in Ad-LacZ-infected tumors (Figures 5a and d). LacZ (E. coli β-galactosidase) protein expression was detected in Ad-LacZ-infected tumors, but not in Ad-shMDR1/Ad-hNIS-infected tumors by the use of X-gal (Figures 5c and f).

Histopathological analysis of both Ad-shMDR1 and Ad-hNIS-infected tumors. Extracted tumors were fixed with 4% formalin overnight. For immunohistological examination of Pgp and hNIS, paraffin sections (5 μm thick) were incubated with anti-NIS (a, d) and anti-Pgp (b, e). Ad-LacZ-infected tumors (control) were stained with X-gal stain solution (c) and were examined under a light microscope ( × 200 magnification).
In vivo therapy with doxorubicin, I-131 and doxorubicin plus I-131
Figure 6a shows the scheme of in vivo tumor treatment to evaluate of therapeutic effects of combination therapy. As shown in Figure 6b, weak inhibition of tumor growth was observed in a tumor model infected with Ad-shMDR1 or Ad-hNIS, followed with either I-131 or doxorubicin treatment alone for 21 days post-tumor challenge. For mice treated either with I-131 or doxorubicin, 248±21 and 227±21% of the initial tumor volume was determined, respectively. However, the tumor volume rapidly increased and reached to 380±45% of the initial tumor volume for mice treated with PBS (PBS versus doxorubicin or I-131-treated mice, P<0.05, respectively). Combination therapy using doxorubicin plus I-131 generated significant tumor growth inhibition in tumor-bearing mice injected with virus mixture (Ad-shMDR1 and Ad-hNIS), and the tumor volume increased only 75±23% of the initial tumor volume at 21 days (mice treated with PBS, I-131 and doxorubicin versus mice treated with doxorubicin plus I-131, P<0.05). However, no therapeutic effects with either I-131 and doxorubicin treatment alone or I-131 plus doxorubicin were observed in the Ad-LacZ-infected tumor model (the tumor volume increases for the PBS, doxorubicin, I-131 and doxorubicin plus I-131 treatment groups were 380±60, 420±77, 416±50 and 354±80%, respectively, Figure 6c).

In vivo therapy of HCT15 colon tumor xenografts. Mice were divided into four groups to assess combination therapy in vivo when the diameters of tumors reached approximately 100 mm3 (▪, PBS; ▴, doxorubicin; ♦, I-131; •, doxorubicin plus I-131). A virus mixture of Ad-shMDR1 (2 × 109 PFU) and Ad-hNIS (1 × 109 PFU) was administered to mice by multiple injections of virus. Ad-LacZ as a control was intratumorally injected to mice by multiple injections of virus. At 2 days after virus injection, a single dose of I-131 (55.5 MBq) was injected and doxorubicin treatment (0.5 mg kg–1) was followed at 3-day intervals for 21 days (a). Tumor-bearing mice were injected with either virus mixture (Ad-shMDR1 plus Ad-hNIS) (b) or Ad-LacZ (c) followed by treatment with PBS, doxorubicin, I-131 or doxorubicin+I-131. Tumor volume was measured using a caliper over time. Experiments were performed in triplicate, n=8 mice/group. *statistically significant.
Discussion
RNA interference (RNAi) has currently been used as a valuable research tool to induce the suppression of specific genes of interest using siRNA or micro RNA, double-strand RNA molecules of short fragments of 19–25 bp.9 Several reports have shown the successful regulation of the MDR1 gene and cancer treatment by the use of RNA interference with in vivo models. Wu et al.16 have reported that small-interfering RNA-induced suppression of MDR1 restores sensitivity to multidrug-resistant human breast cancer cells by analysis of paclitaxel and doxorubicin uptake in cancer cells and by the use of methods such as RT-PCR analysis. Alexandra et al. have also shown the stable and complete suppression of MDR1/P-glycoprotein-mediated multidrug resistance in human gastric or pancreatic carcinoma cell lines using adenovirus expressing-MDR1 siRNA.17 More recently, Xueshi et al.18 showed suppression of MDR1-mediated multi-drug resistance using a lentivirus that expressed MDR1 shRNA in human leukemia cells.
We have previously reported the additive therapeutic effects of the combination of vector-based MDR1 RNA interference and hNIS radioiodine gene therapy in human colon cancer cells in vitro.10 Although this new therapeutic strategy was effective in vitro, some problems remain to be solved for application in a clinical situation. Namely, a stable transfectant expressing hNIS and MDR1 shRNA is an artificial model to examine the therapeutic effects of the combination of hNIS radioiodine gene therapy and MDR1 shRNA therapy. Thus, new targeted methods should be developed where MDR1 shRNA and the NIS gene are only expressed in cancer models. Several investigators have described tissue-specific delivery methods of therapeutic genes in various cancer models using an adenoviral system.19, 20, 21, 22 These investigators have shown that an adenovirus-mediated gene delivery system can induce strong expression of therapeutic genes and effective anti-tumor effects in some cancer models.
On the basis of these previous studies, we adopted the use of an adenovirus-mediated delivery system for effective expression of MDR1 shRNA and hNIS in a human colon cancer model, a therapeutic strategy closer to the clinical situation than that of the use of stable transfectants as was reported previously. Although there are some strategies for multiple therapeutic gene expression such as the use of a bicistronic vector (IRES) and the fusion vector approach,23 we constructed two types of adenovirus expressing MDR1 shRNA or the human NIS gene. An adenovirus mixture (Ad-shMDR1 and Ad-hNIS) was used for in vitro and in vivo therapy experiments. Previous studies have shown effective gene expression of therapeutic genes and tumor growth inhibition by co-injection of separate adenoviruses into tumors.24, 25
By the use of Tc-99 sestamibi uptake analysis, we found that an adenovirus-expressing MDR1 shRNA effectively inhibited P-glycoprotein expression and caused an increase in the uptake of Tc-99m sestamibi in infected human colon cancer cells in vitro or in vivo (Figures 1a and 4). Furthermore, we observed that Ad-hNIS infection of cancer cells induced increased uptake of I-125 and Tc-99m pertechnetate in infected human colon cancer cells in in vitro and in vivo models (Figures 1a and 4). An in vitro cellular cytotoxic assay showed increased cytotoxic effects with the use of combination therapy (doxorubicin and+ I-131) as compared with the use of single therapy either with doxorubicin or I-131 (Figures 2 and 3). More interestingly, the use of in vivo tumor therapy showed that the adenovirus-mediated therapeutic strategies generated significant inhibition of tumor growth for mice treated with combination therapy, whereas slight tumor growth inhibition effects were observed in mice treated with a single therapy (Figure 6). The enhanced therapeutic effects in vitro and in vivo can be explained based on the following mechanisms. (1) Suppression of the MDR1 gene and overexpression of NIS promoted the uptake of radiotracers such as Tc-99m sestamibi, I-131 and Tc-99m pertechnetate, (2) facilitated the accumulation of a therapeutic drug such as doxorubicin and I-131 and subsequently (3) induced strong tumor growth inhibition in mice treated with combination therapy. Particularly, hNIS radioiodine gene therapy could concentrate the beta ray emitting therapeutic radionuclide (I-131) in tumors. Beta rays emitted from I-131 travel 0.2 to 2.4 mm in tissue,26 which results in the death of cells near hNIS-expressing cancer cells by cross-fire effects.
Although the anti-tumor effects and usefulness of combination therapy was shown in the experiments, we did not consider that the anti-tumor effects of combination therapy were related to adenovirus toxicity. Several investigators have reported toxicity related to adenovirus application to living organisms. For example, toxicity such as an increase of aspartate aminotransferase and alanine aminotransferase levels and low stability of the system are suggested as risk factors for the therapeutic use of an adenoviral vector delivery system. However, continued trials for viruses packaged into HEK 293 cells or local application of small particles into limited areas, as was performed in our study, have successfully reduced the risks of infection and other definitive risk factors.11, 12 As described above, a further study should be performed to investigate the safety of combination therapy of MDR1 shRNA therapy and hNIS radioiodine gene therapy using the adenoviral system.
In conclusion, combined Ad-shMDR1 gene therapy and hNIS radioiodine gene therapy (1) enhanced the uptake of Tc-99m sestamibi and Tc-99m pertechnate in vitro and in vivo, (2) increased the cellular cytotoxic effects of doxorubicin and I-131 in vitro and (3) generated stronger anti-tumor effects in a mouse colon cancer model. Combination therapy strategies using an adenovirus-mediated method may have clinical potential in cancer patients who are non-responsive to conventional chemotherapy.
Accession codes
References
Chung JK . Sodium iodide symporter: its role in nuclear medicine. J Nucl Med 2002; 43: 1188–1200.
Cho JY . A transporter gene (sodium iodide symporter) for dual purposes in gene therapy: imaging and therapy. Curr Gene Ther 2002; 2: 393–402.
Chen L, Altmann A, Mier W, Eskerski H, Leotta K, Guo L et al. Radioiodine therapy of hepatoma using targeted transfer of the human sodium/iodide symporter gene. J Nucl Med 2006; 47: 854–862.
Mandell RB, Mandell LZ, Link Jr CJ . Radioisotope concentrator gene therapy using the sodium/iodide symporter gene. Cancer Res 1999; 59: 661–668.
Jeon YH, Choi Y, Kim HJ, Kim CW, Jeong JM, Lee DS et al. Human sodium iodide symporter gene adjunctive radiotherapy to enhance the preventive effect of hMUC1 DNA vaccine. Int J Cancer 2007; 121: 1593–1599.
Jeon YH, Choi Y, Yoon SO, Kim CW, Chung JK . Synergistic tumoricidal effect of combined hMUC1 vaccination and hNIS radioiodine gene therapy. Mol Cancer Ther 2008; 7: 2252–2260.
Schinkel AH, Jonker JW . Mammalian drug efflux transporters of the ATP binding cassette (ABC) family: an overview. Adv Drug Deliv Rev 2003; 55: 3–29.
Fire A, Xu S, Montgomery MK, Kostas SA, Driver SE, Mello CC . Potent and specific genetic interference by double-stranded RNA in Caenorhabditis elegans. Nature 1998; 391: 806–811.
Hannon GJ . RNA interference. Nature 2002; 418: 244–251.
Park SY, Kwak W, Thapa N, Jung MY, Nam JO, So IS et al. Combination therapy and noninvasive imaging with a dual therapeutic vector expressing MDR1 short hairpin RNA and a sodium iodide symporter. J Nucl Med 2008; 49: 1480–1488.
St George JA . Gene therapy progress and prospects: adenoviral vectors. Gene Therapy 2003; 10: 1135–1141.
Brunetti-Pierri N, Ng P . Progress and prospects: gene therapy for genetic diseases with helper-dependent adenoviral vectors. Gene Therapy 2008; 15: 553–560.
Ballinger JR . Imaging multidrug resistance with radiolabeled substrates for P-glycoprotein and multidrug resistance protein. Cancer Biother Radiopharm 2001; 16: 1–7.
Moretti JL, Hauet N, Caglar M, Rebillard O, Burak Z . To use MIBI or not to use MIBI? That is the question when assessing tumour cells. Eur J Nucl Med Mol Imaging 2005; 32: 836–842.
Ahn SJ, Lee YJ, Lee YL, Choi CL, Lee SW, Yoo JS et al. Increases in doxorubicin sensitivity and radioiodide uptake by transfecting shMDR and sodium/Iodide symporter gene in cancer cells expressing multidrug resistance. Nucl Med Mol Imaging 2007; 41: 209–217.
Wu H, Hait WN, Yang JM . Small interfering RNA-induced suppression of MDR1 (P-glycoprotein) restores sensitivity to multidrug-resistant cancer cells. Cancer Res 2003; 63: 1515–1519.
Kaszubiak A, Holm PS, Lage H . Overcoming the classical multidrug resistance phenotype by adenoviral delivery of anti-MDR1 short hairpin RNAs and ribozymes. Int J Oncol 2007; 31: 419–430.
Ye X, Liu T, Gong Y, Zheng B, Meng W, Leng Y . Lentivirus-mediated RNA interference reversing the drug-resistance in MDR1 single-factor resistant cell line K562/MDR1. Leuk Res 2008.
Willhauck MJ, Sharif Samani BR, Klutz K, Cengic N, Wolf I, Mohr L et al. Alpha-fetoprotein promoter-targeted sodium iodide symporter gene therapy of hepatocellular carcinoma. Gene Therapy 2008; 15: 214–223.
Spitzweg C, O’Connor MK, Bergert ER, Tindall DJ, Young CY, Morris JC . Treatment of prostate cancer by radioiodine therapy after tissue-specific expression of the sodium iodide symporter. Cancer Res 2000; 60: 6526–6530.
Dwyer RM, Bergert ER, O’Connor MK, Gendler SJ, Morris JC . Sodium iodide symporter-mediated radioiodide imaging and therapy of ovarian tumor xenografts in mice. Gene Therapy 2006; 13: 60–66.
Spitzweg C, Morris JC . Approaches to gene therapy with sodium/iodide symporter. Exp Clin Endocrinol Diabetes 2001; 109: 56–59.
Iyer M, Sato M, Johnson M, Gambhir SS, Wu L . Applications of molecular imaging in cancer gene therapy. Curr Gene Ther 2005; 5: 607–618.
Gao Y, Ng SS, Chau DH, Yao H, Yang C, Man K et al. Development of recombinant adeno-associated virus and adenovirus cocktail system for efficient hTERTC27 polypeptide-mediated cancer gene therapy. Cancer Gene Ther 2008; 15: 723–732.
Zhang X, Xu J, Lawler J, Terwilliger E, Parangi S . Adeno-associated virus-mediated antiangiogenic gene therapy with thrombospondin-1 type 1 repeats and endostatin. Clin Cancer Res 2007; 13: 3968–3976.
Vallabhajosula S . Radiopharmaceuticals in oncology. In: Khalkhali I MJ, Goldsmith SJ, eds (ed). Nuclear Oncology: Diagnosis and Therapy. PA: Lippincot, Williams & Wilkins: Philadelphia, 2001 pp 31–62.
Acknowledgements
This work was supported by Ministry of Education, Science & Technology(MEST) and National Research Foundation of Korea (NRF) through Nuclear R&D Program, 2009 (No. 007-8572), the Korean Ministry of Education, Science and Technology (The Regional Core Research Program/Medical Convergence Technology Development Consortium for Anti-aging and Well-being), and the Basic Atomic Energy Research Institute (BAERI, 2009-0078234) and BK21 (2009).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
This work is licensed under the Creative Commons Attribution Noncommercial Share Alike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article
Cite this article
Ahn, S., Jeon, Y., Lee, Y. et al. Enhanced anti-tumor effects of combined MDR1 RNA interference and human sodium/iodide symporter (NIS) radioiodine gene therapy using an adenoviral system in a colon cancer model. Cancer Gene Ther 17, 492–500 (2010). https://doi.org/10.1038/cgt.2010.3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/cgt.2010.3
Keywords
This article is cited by
-
Sodium/iodide symporter gene transfection increases radionuclide uptake in human cisplatin-resistant lung cancer cells
Clinical and Translational Oncology (2015)
-
Sodium iodide symporter (NIS) in extrathyroidal malignancies: focus on breast and urological cancer
BMC Cancer (2014)
-
Complementary treatment of siTERT for improving the antitumor effect of TERT-specific I-131 therapy
Cancer Gene Therapy (2012)
