
Key Points
-
Reports two audit periods of patient compliance with a prolonged, staged periodontal treatment protocol. In the second audit period, compliance with smoking cessation advice is also reported.
-
Patient adherence in this primary care setting was found to be quite high for both of these parameters.
-
Patients in the second audit series who did not complete treatment were contacted where possible to try and determine the reasons for non compliance with the periodontal therapy.
Abstract
Objective Recently the issue of patient adherence with prolonged periodontal therapy and the importance of smoking and its influence as a significant co-factor in the outcome of treatment for patients with periodontal disease has been of interest to health care professionals. This paper is an audit of adherence in regard to both smoking cessation for those who admitted to a smoking habit at the initial examination and patient compliance with a periodontal treatment protocol.
Design During the initial examination, patients referred to the practice with periodontal problems were photographed both with and without lip retractors as part of their clinical record, and a charting of the teeth made with any 5 mm or greater probing depths recorded. Tooth mobility and furcation involvement of molar teeth were also charted. Two separate time periods (Series 1 and Series 2) were audited in this study. Patients enrolled in Series 2 were routinely asked about their smoking habits at the initial examination. Two time periods were audited, as the initial purpose of the investigation was to audit the success of the practice in treating this group of patients, and to identify any improvements that could be made in care provision as each audit cycle was completed.
Setting Primary care setting.
Results Patient adherence rates were high through all the various stages of periodontal therapy, even though the treatment protocol took over 18 months to complete. Approximately 55% of patients in both time periods presented for the one-year post treatment re-evaluation appointments. 56.5% of the patients reported they had smoked to within five years of their initial consultation, of which 38% reported that they had stopped by the time they had completed the initial hygiene phase of treatment.
Conclusions With a comprehensive and clearly defined supportive periodontal care programme (SPC), this paper demonstrates that high adherence levels can be achieved in a primary care setting. The results suggest that treatment should include not only the teaching of an effective oral hygiene regime, but also include giving advice in relation to smoking cessation for those patients who admit to a smoking habit at the initial examination. Patients who smoked and chose to have treatment for their periodontal condition went on to report good adherence with smoking cessation advice. Continuing supportive smoking cessation (SSC) advice should be part of any effective SPC programme. New methods of treating periodontal disease that become available to practitioners in the future should use established benchmarks against which to evaluate the success of any new treatment strategy.
Similar content being viewed by others


Introduction
A recent review of the natural history of periodontal disease and its prevalence in populations suggested that around the world between eight and 20% of adults suffer from periodontal disease.1 As far as assessment of the presence of periodontal disease is concerned the same author stated 'Epidemiological studies of chronic inflammatory periodontal diseases have assessed a wide range of clinical features including gingivitis, pocket probing depth, clinical attachment level and have radiographically assessed alveolar bone loss, all in a particularly inconsistent manner'.
This criticism of previously published epidemiological papers explains why comparison of different study populations has been notoriously difficult to make in the past. However some attempt must be made to understand the size of the problem in the general population to enable sensible planning for future care provision.
A study published by the author of a 12 year retrospective analysis of patients in his then general practice in 1985-6 indicated that 21% of the adult patients at initial examination had at least one tooth with a probing depth of greater than or equal to 7 mm.2 This compares with the findings of the Adult Dental Health Survey in the UK3 that found only 8% of the dentate population over 16 years of age had a site with at least 6 mm of periodontal attachment loss.
Extrapolating from the data from the Adult Dental Health Survey, which is at the conservative end of the range, there are potentially over three million patients who have a periodontal problem in the UK.4Periodontal therapy is known to be successful in maintaining the vast majority of patients' teeth over time.5
In a subsequent paper using the same patient cohort from the author's general practice, over the 12 year period of study of patients originally seen in 1985-6, a total rate of tooth loss of 0.08 teeth per person per year was achieved when the 157 patients were given regular dental care and a SPC programme dependent on individual patients' needs.6 It was also found that between 1 and 2% of the patients developed a new 7 mm or greater probing depth each year, indicating that the vast majority of patients followed in this study population were maintained with stable periodontal health, whether they demonstrated significant periodontal problems at the initial examination or not. The rate of occurrence of new 7 mm probing depths in this study can be seen in Figure 1.

Percentage of patients with no new 7 mm probing depth recorded for each year of study
These previously published results support the view that treatment of periodontal disease in a primary care setting can be successful over a prolonged period of time when outcomes like tooth loss and incidence of new 7 mm or greater probing depths are used as endpoint measures.7 However, it is also clear from previously published papers that periodontal therapy without compliance with a maintenance regime is of doubtful value.8 How many patients do not complete their periodontal treatment plan, or fail to attend for their SPC programme? Most reports show low levels of compliance with maintenance therapy, with results varying between 11 and 45%.9,10 Nevins suggested overall adherence rates of no greater than 40% for patients receiving periodontal therapy in private practice.11 However, no indication is made in these previous studies of how far each of the patients progressed through the stages of their treatment plan. Neither is any mention of patients' smoking habits made or any indication given as to whether patients were adherent with advice to give up.
On entry to the GDC specialist list for periodontology in 2000, the author accepted many referrals from local general dental practitioners for patients with periodontal problems needing treatment. He became interested to know what was the adherence and non-adherence at specific points in the periodontal therapy provided amongst those referred patients so that the success of the practice's treatment strategy could be assessed, and hopefully then improved. Two audit cycles were completed.
Clear staging of treatment was identified for the two study groups in this retrospective analysis.
As referred patients to the practice were photographed at the initial examination as part of the initial records, the photographic records of those patients accepted originally between 1 March 2001 and 28 February 2002 (Series 1) were used to create a list of consecutive patients. A further series of patients whose initial examination occurred between 1 September 2003 and 31 March 2004 was also produced (Series 2). The reason why two separate time periods were audited was to see if there was any improvement in compliance during the second audited period as compared to the first. No major changes were made in regard to how patients were treated during the two time periods studied.
Further photographs were taken in both series at the one-year review appointment (Figs. 2 and 3). In Series 1, only patients with periodontal problems affecting their anterior teeth were photographed. In the time period covered in Series 2, all patients were photographed regardless of which teeth were affected by periodontal problems.

Patient at initial presentation

Patient at final review
Treatment was staged in the following way:
-
1
Having attended the first examination for full charting and diagnosis, stage one involved starting hygiene therapy with one of the practice hygienists. This included oral hygiene instruction, and scaling and root planing of the teeth. It also involved advice on smoking cessation where appropriate.
-
2
Completion of this initial therapy after at least three visits with the hygienist.
-
3
Two months after the completion of initial therapy, patients were asked to attend a further review with the author when a new probing depth chart was completed and the patient treatment planned. The options offered to the patient at this stage depended upon their adherence with the therapy to date.
-
4
If indicated, open or closed root planing of those areas where there were still probing depths greater than or equal to 5 mm. For this stage, the author himself provided the open or closed root planing.
-
5
Twelve months following completion of all treatment and having attended a three monthly SPC programme, a final review appointment to assess the patients periodontal health. This involved a further probing depth charting, photographs, and correspondence with the referring dentist to discuss any restorative treatment required.
Referring dentists were advised of the completion or otherwise of each stage by letter.
Patients' smoking status was routinely recorded at the initial examination in Series 2 as it was one of the questions asked in the pro forma medical history given to all patients to fill out before their first clinical appointment. This was not the case in Series 1 because the medical questionnaire provided for patients in 2001-2 did not enquire about the patients' smoking habits. Patients were recorded as smokers if they reported having smoked within the five years prior to the initial examination. Furthermore, if the patient reported having given up smoking within the previous five years, or during the treatment period itself, they were recorded as having stopped smoking.
The records for patients in Series 1 were reviewed again three years and eight months following the final review appointment to assess whether they had continued annual review with the author, or had been returned 'treatment complete' to the original referring dentist where their SPC programme had hopefully been continued. Fardal recently published an assessment of interviewed patients that were non compliant with a SPC programme but later returned to his practice.12 He found they were compliant for 3.4 years (SD 3.2) with a SPC programme before they became non compliant.12 In this current study, only compliant patients were followed. Those in Series 1 whose records were reviewed at three years and eight months following their annual review had remained compliant for over five years from their initial examination.
The aim of this study was therefore to audit adherence in regard to both smoking cessation for those who admitted to a smoking habit at the initial examination, and to record patient compliance with a periodontal treatment protocol including a SPC programme.
Results
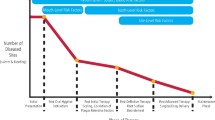
The results for the patients in both series can be seen in Figure 4. Forty-three patients were enrolled in Series 1, 69 patients in Series 2. The patients all presented with adult chronic periodontitis with probing depths of 7 mm or greater affecting many of their teeth at initial presentation. They were predominantly Caucasian and from a middle class background.

Compliance for both study periods
In Series 2, 39 (57%) admitted to being smokers when challenged, of which 15 (38%) reported becoming non-smokers (Fig. 5).
-
1
In Series 1, 42 patients left the initial examination and consultation, and made further appointments with one of the practice hygienists for oral hygiene instruction and scaling and root planing (97.7%), 66 (95.6%) in Series 2.
-
2
Thirty-seven (86%) completed the hygiene phase in Series 1, 65 (94.2%) in Series 2.
-
3
Thirty-six (83.7%) attended the review appointment two months following initial therapy in Series 1 while 60 (86.9%) completed this stage in Series 2. At this appointment, a decision was taken whether to progress to open or closed root planing with the author. For some (between 14 and 16%), treatment was felt to have been successful enough for the patient to be enrolled immediately on a SPC programme, because all the periodontal problems present at initial examination had resolved through the initial therapy. They were referred back to their general dental practitioner. Some didn't progress because their oral hygiene wasn't good enough (10% both series), or because they were still smoking, but were seriously intending to give up in the near future (4% Series 2). If they were intending to stop smoking in the near future, open and closed root planing was delayed in Series 2 to benefit from the better healing response seen in a non-smoker as compared to a smoker. If they had no intention of stopping smoking, further treatment was not necessarily denied to these patients.
-
4
Of those patients who required further open or closed root planing, in Series 1, 20 (69.2%) completed this stage of treatment, while in Series 2, 33 (72.8%) progressed through this stage.
-
5
In Series 1, 24 (55.8%) returned for review after SPC one year following the active phase of treatment. In Series 2, 38 (55%) completed this stage.
-
6
In Series 1, 10 (45.7%) patients were still enrolled in SPC over three years after their initial examination, and were still attending annual reviews with the periodontist.

Proportion of smokers to non smokers
In Series 2 those who were not compliant gave various reasons for their non-adherence when contacted (Fig. 6). Three (4%) had moved away, while two (3%) gave financial problems as their reason for not progressing. Four (6%) decided not to progress treatment through their own choice, while for 14 (20%) no reason for non-compliance could be elicited.

Reasons given for not completing treatment
Discussion
The periodontal therapy described in this paper takes in the region of 18 months to complete, which is a very long time to expect a patient to remain compliant with the treatment staging. It is therefore encouraging how well most patients progressed through the stages of treatment. Those that did not attend the final review may well be following a SPC programme very successfully at their own originally referring practice.
The rate at which patients reported stopping smoking is also very encouraging and suggests an important further role for the dentist and the hygienist other than just giving oral hygiene instruction and cleaning teeth. It must be remembered however that the only evidence that the patient had stopped smoking was because they reported they had stopped, and therefore some care should be exercised in accessing this reported success.
One of the disadvantages of retrospective analysis of this kind is that they often don't address why those patients who didn't complete treatment chose not to do so. Some attempt was made to follow up the non-attending patients, and the reasons given for not completing treatment are reported. However, the study is open to the usual criticism that there may be bias towards patients who were satisfied with the treatment they received, causing the statistics to be too optimistic if extrapolated to the general population.
Donabedian13 suggested that the quality of healthcare could be assessed under the headings of structure (material and human resources available), process (how things are done), and outcome (the results and benefits).
Modern quality assurance programmes concentrate heavily on structure and process because they are easier to measure in cross-sectional designed audits. It is then often extrapolated in many quality programmes that if structure and process are good, so too will be the outcome. It is my belief that more attention should be paid to the outcomes achieved and patient compliance with the treatment protocol offered, as I believe too much emphasis is placed on structure and process.
Conclusions
With a comprehensive and clearly defined supportive periodontal care programme (SPC), this paper demonstrates that high adherence levels can be achieved in a primary care setting.
Treatment must include not only the teaching of an effective oral hygiene regime, but also advice in relation to smoking. A continuing supportive smoking cessation programme should be part of any effective SPC programme. Support should be provided to dental practitioners to be able to achieve this, both in general practice and in specialist practice.
References
Papapanou P N . Periodontal diseases: epidemiology. Ann Periodontol 1996; 1: 1–36.
Nicholls C . A 12-year retrospective audit study of tooth loss in a general dental practice. Br Dent J 2000; 189: 98–99. Erratum in: Br Dent J 2000; 189: 294.
Kelly M, Steele J, Nuttall N et al. Adult Dental Health Survey: Oral Health in the United Kingdom 1998. London: The Stationary Office, 2000.
Snoad R . Description of a system designed to assist primary dental care clinicians in decision-making with regard to specialist periodontal referrals and report of two clinical audits using the system. Primary Dent Care 2004; 12: 135–141.
Hirschfield L, Wasserman B . A long term survey of tooth loss in 600 treated periodontal patients. J Periodontol 1978; 49: 225–237.
Nicholls C . Periodontal disease incidence, progression and rate of tooth loss in a general dental practice: the results of a 12-year retrospective analysis of patient's clinical records. Br Dent J 2003; 194: 485–488.
Hugoel P P, DeRouen T A . A survey of endpoint characteristics in periodontal clinical trials published 1988-1992, and implications for future studies. J Clin Periodontol 1995; 22: 397–407.
Buckley L A, Crowley M J . A longitudinal study of untreated periodontal disease. J Clin Periodontol 1984; 11: 523–530.
Mendoza A R, Newcomb G M, Nixon K C . Compliance with supportive periodontal therapy. J Periodontol 1991; 62: 731–736.
Wilson T G Jr, Hale S, Temple R . The results of efforts to improve compliance with supportive periodontal treatment in private practice. J Periodontol 1984; 5: 468–473.
Nevins M . Long-term periodontal maintenance in private practice. J Clin Periodontol 1996; 23: 273–277.
Fardal O . Interviews and assessments of returning non-compliant periodontal maintenance patients. J Clin Periodontol 2006; 33: 216–220.
Donabedian A . The quality of care. How can it be assessed? 1988. Arch Pathol Lab Med 1997; 121: 1145–1150.
Author information
Authors and Affiliations
Corresponding author
Additional information
Refereed Paper
Rights and permissions
About this article
Cite this article
Nicholls, C. A retrospective study of compliance (adherence) with a care pathway in periodontal therapy in a primary care setting. Br Dent J 201, 709–712 (2006). https://doi.org/10.1038/sj.bdj.4814303
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.4814303
