
Abstract
Introduction The extent to which initial therapy has been provided prior to referral for periodontal disease remains unclear despite guidance provided by the British Society of Periodontology.
Aim This audit aimed to assess the information given in the referral letter, how this compared to patients' perception of treatment received, the referrers' reports of treatment provided and findings at consultation. The gold standard was taken from the British Society of Periodontology referral criteria which states that all patients should undergo initial periodontal therapy prior to referral.
Method Data were collected via questionnaires from 100 randomly selected patients referred for periodontal treatment from patients at consultation and subsequently from the referring practitioners.
Results All 100 patients had incomplete referrals with 12 patients having Basic Periodontal Examination (BPE) scores corresponding to those at consultation. Eighty-five patients reported receiving oral hygiene instructions (OHI) and 91 patients root surface debridement (RSD), prior to referral. Twenty-five dentists participated in the survey and reported spending more time providing initial therapy than the patients.
Discussion and conclusion Most patients reported having undergone initial periodontal treatment, however, the extent was at variance to the referrers' reports. BPE scores were inaccurate and the majority of referrers failed to provide a diagnosis, with incorrect terminology used. The study highlights the need for improving the management of periodontal disease in primary care.
Similar content being viewed by others

Key points
-
Although patients thought they had undergone initial treatment, this was at variance to the treatment GDPs stated they had provided.
-
There is scope to improve the quality and appropriateness of periodontal referrals.
-
There is need to improve the knowledge and understanding of periodontal disease diagnosis and the role of risk factors.
Introduction
The costs associated with treating patients with periodontitis have been estimated to be more than £2.8 billion annually.1 Periodontitis affects approximately 60% of the population as reported in the Adult Dental Health Survey with only 10-15% of patients suffering from severe disease.2 The latter is in line with figures reported worldwide of severe periodontitis.3 Clinical assessment of the disease is made using visual parameters including assessment of plaque and calculus, gingival tissue appearance, including oedema and erythema, as well as bleeding on probing, recession and probing depths. The disease has recently been classified in stages, Stage I being <15% or <2 mm attachment loss from the cemento-enamel junction, Stage II to the coronal third of the root, Stage III to the mid root and Stage IV to the apical third.4 The first steps in the management of periodontal disease involve initial phase therapy which comprises of oral hygiene instruction, followed by correction of any plaque retentive factors and RSD, usually under local anaesthesia, to remove any debris or deposits followed by reassessment approximately 6-8 weeks later.5 At the reassessment visit, the need for further treatment is ascertained and the patient then either managed within the practice setting or referred onwards for further intervention.
According to the British Society of Periodontology (BSP) guidelines, patients with mild to moderate disease as noted by BPE scores of 2-3 should be managed by the general dental practitioner (GDP) in the first instance, followed by a reassessment before making a decision to refer the patient either to a specialist provider within the hospital services, specialist centres or private practice for further periodontal intervention.6 Dentists refer patients for a number of reasons which include case complexity, patient management, competence/skill, second opinion and advice and patient requests.7,8,9 Irrespective of the reason for referral, the BSP guidelines state that prior to a decision for referral being made for a patient with periodontal disease, the referring dentist would have undertaken an assessment followed by the provision of initial phase therapy which would have included OHI, to improve the plaque control, and RSD.
A preliminary analysis of the referrals to the periodontology department of the Eastman Dental Hospital indicated that a number of patients were being referred with lack of clarity as to whether initial therapy had been provided despite the referral letter suggesting that this treatment had been completed with patients, when asked at consultation, being unaware of what had been provided.
This audit sought to assess the information given in the referral letter and how this compared to the patient's perception of treatment they had received prior to referral and the clinical findings at the consultation visit using a survey method. The referring dentist was also asked to complete a questionnaire to ascertain the initial treatment they had provided prior to making the referral.
Materials and methods
The gold standard was that all patients would undergo initial therapy prior to referral as per the BSP referral criteria.6 Two data collection forms were designed for the survey (Fig. 1 and Fig. 2). The first form was designed to collect information at the consultation visit and was completed by the clinician who saw the patient at this visit. It included information provided on the referral letter including the BPE scores, the patient reported information about the initial periodontal treatment they had received prior to their referral being made and the clinical findings at the consultation. The second form was designed for the referring practitioner to complete and captured information about the initial periodontal treatment they had provided prior to making the referral. The questions used were the same as those in the first form for ease of comparison and the questions were based on the BSP's parameters of care which state:6

Data collection form 1 used at the consultation visit

Data collection form 2 sent to the referring general dental practitioner
-
Any patient who has been referred for chronic periodontitis should have undergone a thorough course of initial therapy in primary care
-
The above should be reflected by the amount of time, number of visits and the use of local anaesthesia where appropriate.
One hundred sequential patients were selected from new patient clinics to participate in this audit. Patients attending the new patient clinics were given the option of taking part in the survey and those who agreed to participate were consented. Referring dentists to the hospital were also informed of the project and invited to participate. Data collection form 1 was completed on clinic and for each of the patients who participated, the referring dentist was contacted either by post or email after the appointment and invited to complete data collection form 2. The collected data were analysed using Apple Numbers.
Results
One hundred patients agreed to take part in the survey and 100 data collection forms were completed at the consultation visit. Of the 100 referring practitioners contacted, only 29 responded to our request despite sending two reminders. Four of the 29 who had responded, declined to take part leaving a total of 25 referring dental practitioners who returned the completed questionnaires.
Information provided in the referral letter
Forty-four of the referrers had stated the reason on the referral letter as 'chronic active periodontitis' and 46 had given no diagnosis on the referral letter. Of the remaining ten, three had stated a diagnosis of aggressive periodontitis, six of periodontal disease and one of gingival hyperplasia. None of the referral letters gave information about risk factors.
Ninety-six referrals had recorded the BPE score, however none of the referrals included details of all aspects of the initial therapy provided (that is, the length of the appointment, the use of local anaesthesia, the number of appointments and how many courses prior to referral, who had provided the treatment and when the RSD had been completed prior to the decision for referral) with only 49 giving some information about the initial therapy that had been provided (Table 1).
Information collected at the consultation appointment
Of the 100 patients, 44 were males and 56 were females with an average age of 46 years (range 24-76 years).
BPE scores
Only 12 patients had BPE scores that corresponded with those provided on the referral letter. Of the remaining 88, 58 of the BPE scores on the referral letter underestimated the severity of disease and 30 over-estimated the severity of the disease. The degree of variance in the under scoring of the BPE in the referral letter compared to that at consultation varied either by one score, that is, the GDP had reported a score of 2 on the referral letter when at consultation this was noted as 3 (n = 37), two scores (n = 19) or by three scores (n = 2) that is, the GDP had recorded a score of 1 when at consultation this was noted as 4. The degree of variance in the over scoring of the BPE in the referral letter compared to that at consultation varied either by one score (n = 22), two scores (n = 7) or three scores (n = 1) that is, the GDP had recorded a score of 4 but at consultation it was recorded as 1.
Diagnosis and risk factors
Eighty-six of the patients were diagnosed with chronic periodontitis, five with aggressive periodontitis, seven with plaque induced gingivitis, one with altered passive eruption and one with a perio-endo lesion.
Nine patients were current smokers and of the 91 non-smokers, 21 reported to be ex-smokers. Other risk factors confirmed at consultation included stress (13 patients), occlusal trauma (seven patients) and systemic conditions (four patients). Ten patients were noted to have at least two or more risk factors at consultation.
Patient responses collected at the consultation visit
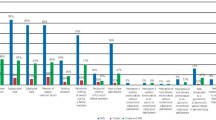
Eighty-seven patients reported to be regular attenders to the dentist and the remaining 13 were irregular attenders. Eighty-five of the regular attenders indicated they had received oral hygiene instruction prior to referral. Of these, 54 (64%) reported that <5 minutes were spent on giving them oral hygiene instruction with only 6 (7%) stating that >15 minutes was spent on giving them oral hygiene instruction (see Fig. 3). All smokers (n = 9) referred had received smoking cessation advice prior to referral. The details of the responses to questions 2, 5, 6, 7, 9 and 10 are given in Table 2. Ninety-one patients reported having undergone some RSD prior to referral with 33 (36%) stating 20-30 minutes were spent on the visit and seven (8%) stating that <10 minutes was spent on the visit (see Fig. 4). Just over half the patients stated that the RSD was undertaken by the dentist and just under half by a hygienist. Thirty-four (37%) of the 91 patients had undergone RSD under local anaesthesia and 57 (63%) stated that they had received more than one course of RSD in the previous 12 months with a range of 2 to 6 courses. Twenty-six patients (29%) stated that their last course of RSD had been at least 6 months prior to the referral being made with an overall range from 1 month to 1 year. Nine patients stated that they had not received RSD; however, the referral letters for 3 of these stated that they had been given RSD prior to the referral.

Time spent on being given oral hygiene instruction as reported by patients

Time spent on a debridement visit as reported by patients
Acceptance for treatment
Thirty-one of the 100 patients referred were accepted for treatment into the hospital based on the disease complexity and treatment needs. The average time taken from receipt of referral letter to assessment on the new patient clinic was 9 weeks.
Dentist responses collected by post
The information gathered from the 25 responding participants gives an insight into the treatment provided by the dentist prior to referral and how this compared with the patient's perception of the pre-referral treatment they had received. Table 3 shows these compared responses. The key variances relate to the provision of OHI and RSD. Dentists reported to have spent more time in providing OHI than perceived by the patients and they also reported longer duration for their appointment times for RSD than perceived by the patient. The level of oral hygiene reported by the dentists was noted to be similar to that recorded at the consultation visit. All 25 dentists and patients reported similar time frames between the last visit of RSD and the referral being made; however, dentists stated that local anaesthesia had been used more often than patients had reported. Three of the 25 dentists provided comments in the free text box shown in Box 1.
Discussion
This audit is the first of its kind where an attempt has been made to assess patients' perception of the initial phase therapy they received prior to being referred for periodontal disease compared to the initial therapy the referring dentist reported to have provided.
The audit showed that the quality of the referral letters was variable, with all of the referral letters failing to provide the required information about the extent of initial treatment provided to the patient prior to the referral being made. These findings are consistent with the findings of others reported in the literature.10,11 These reports have suggested the use of referral proformas to improve the quality of information in the referral.
A proportion of dentists either over scored or under scored the BPE. Under scoring can result in failure to execute appropriate treatment in practice.12 Over scoring could be due to the patient having undergone subsequent treatment with the dentist after the referral being made, post treatment healing or simply a case of the dentist over scoring to ensure acceptance of the referral.13 One important point is that the average time between receipt of referral and consultation was around 9 weeks, which could account for some discrepancy in BPE scores. Nevertheless, similar findings have already been reported in the literature.13,14 The audit does show that the majority of the referring dentists (98%) were providing a BPE score on the referral letter, compared to previous reports where <50% of GDPs provided this.13
The referrers' perception of the patient's oral hygiene largely corroborated with that recorded on the new patient clinic with almost one third of the referred patients having poor oral hygiene. These referrals would have been accepted for consultation based on the other information in the referral letter, ie complexity of periodontal disease. The role of bacterial plaque and oral hygiene in the successful management of periodontal disease has been well established.15,16,17 Patients' behavioural changes are integral to the successful outcome of periodontal disease interventions; however, the number of referrals received in secondary care for periodontal disease would suggest that perhaps this is an area where dentists need support and guidance in ensuring that they are making the diagnosis of the periodontal problems early, communicating this with the patient and initiating early intervention to prevent disease progression.18,19 Today, the role of behaviours and attitudes in managing chronic conditions has become an integral part of patient care, and it is essential that there is recognition of the challenges faced by the referring general dental practitioners in undertaking this under a general dental service (GDS) contract when time pressures often dictate the extent of communication and intervention that can be achieved. The time spent providing initial therapy was recorded as a potential surrogate marker of adequate initial therapy but there is inherently an aspect of recall bias with this type of survey.
Fifty-four of the referrals included a diagnosis in the referral letter; however, 14 of the diagnoses provided were inaccurate. This inability to make a diagnosis raises a number of challenges for the referring dentist as this could lead to under or over treatment and delays in treatment. The former would perhaps explain the increasing rate of medicolegal litigation in relation to the failure of diagnosing periodontal disease.20,21 In this audit seven patients were given a diagnosis of chronic active periodontitis on the referral letter but, at consultation, these patients had a diagnosis of dental biofilm induced gingivitis with five of the patients having poor oral hygiene. An accurate diagnosis would have allowed these patients to receive appropriate treatment more efficiently. Whilst a correct diagnosis does not necessarily relate to whether a referral was appropriate or not, it can help the referrer in identifying the correct management strategy and setting for the patient and remains an important factor. Only 31 of the 100 patients referred were accepted for treatment (examples shown in Fig. 5 and Fig. 6), suggesting that a number of patients did not require referral. If the referrers had an accurate diagnosis at the outset the number of inappropriate referrals would likely be lower.

An example of a case that was accepted for treatment due to disease severity, complex occlusal issues and fair-good oral hygiene

Another example of a case that was accepted for treatment due to the severity of bone loss, furcation involvement and infra-bony defects in combination with excellent oral hygiene
As a guide to referrers, in general, referral letters should contain the following information:
-
Reason for referral
-
Diagnosis, including risk factors
-
Complexity level according to the BSP referral policy6
-
Medical history
-
Treatment provided thus far, including:
-
Number of appointments for RSD
-
Number of courses of RSD
-
Use of local anaesthesia
-
Current BPE scores
-
Current oral hygiene level.
-
The audit also shows that patients' perception of the treatment they had received was not entirely consistent with the treatment that had been provided to them. This could be due to patients' lack of comprehension, along with the clarity of the communication received. The patient plays a key role in the management of periodontal disease, and thus time needs to be invested in ensuring that information about the disease is given in a way that can be understood and accepted by the patient. The current GDS contract has been highlighted as a barrier to achieving this.22
Although the BSP standards of care mention the steps dentists should follow in providing initial therapy, the audit indicated that not all referred patients had undergone initial phase therapy prior to the referral being made. In those patients who had received initial phase therapy, the treatment was often provided over one visit. There are a number of factors that have been reported to affect the provision of periodontal disease in general dental practice with the current GDS contract being the key one.22,23,24,25,26 The BSP guidelines stipulate that a referral depends not only on the severity of disease, complicating factors and complexity of treatment required but also on the GDP's knowledge, experience and training as well as the patient's desire to see a specialist or undergo specialist treatment.27 According to these guidelines, level 1 complexity patients would normally be treated in primary care, level 2 complexity patients would be treated in primary care only if the clinician has the relevant skills with the majority of level 3 complexity patients being referred. This audit would indicate that the majority of the patients were in complexity level 2 as noted by the number that were discharged back to the referring dentist. This is an issue that could potentially be addressed with wider implementation of managed clinical networks.
The survey did not look at how long the referring GDP had been qualified, what further training they had undergone or where they were based. Thus it is difficult to say if the observations made about the provision of the initial therapy related to the dentists' knowledge and skill and this should be explored further in future projects. Nevertheless, a newly qualified dentist should be able to diagnose the majority of periodontitis cases, which would facilitate appropriate referral and efficiency in treatment provision. A recent survey of final year undergraduate students reported that they felt adequately prepared to manage these cases.28 Foundation trainers report a decline in standards of new graduates and 83% felt that new graduates were satisfactory at managing periodontal disease.29 The comments made by three of the dentists would indicate that there may be some gap in the GDPs' knowledge of how to manage the disease.
Any conclusions from the survey of referrers should be interpreted with caution due to the low response rate of 29% compared to the average of approximately 60%, although our response rate was similar to that of other recent studies within dentistry.29,30,31
Dissemination of the audit findings to referrers and course organisation with the opportunity for discussion are the action points from this audit and will be re-audited in the future.
Conclusion
Within the limitations of the audit, the results highlight the importance of accurate assessment, diagnosis and the importance of adequate initial therapy in order to facilitate individual patients being treated in the appropriate setting in an efficient manner. The importance of communication with the patient about their disease along with the reason and type of treatment is also established and the role of risk factors. The audit further highlights the variance in patients' perception of the treatment they receive and the need for the treating dentist to be vigilant in providing clear communication to the patient with regards to periodontal disease and their role in disease management. There appears to be need for further interaction between primary and secondary care, education and potentially adjustment of the GDS contract with incorporation of managed clinical networks to improve the management of periodontal disease in primary care.
References
Britain's Plaque Plague Costing NHS More Than GBP 2 Billion. Available online at https://www.investegate.co.uk/articlePrint.aspx?id=20080410111900NY114 (accessed November 2019).
Fuller E, Steele J, Watt R, N N. 1: Oral health and function - a report from the Adult Dental Health Survey 2009. The NHS Information Centre, 2011.
Demmer R T, Papapanou P N. Epidemiologic patterns of chronic and aggressive periodontitis. Periodontol 2000 2010; 53: 28-44.
Dietrich T, Ower P, Tank M et al. Periodontal diagnosis in the context of the 2017 classification system of periodontal diseases and conditions - implementation in clinical practice. Br Dent J 2019; 226: 16-22.
Segelnick S L, Weinberg M A. Reevaluation of initial therapy: when is the appropriate time? J Periodontol 2006; 77: 1598-1601.
The British Society of Periodontology. Referral policy and parameters of care. England: The British Society of Periodontology, 2011.
Burke F M, Allen P F, McConnell R J, Ziada HM, O'Sullivan K. Prospective evaluation of the referral pattern to restorative dentistry consultation clinics in Ireland. Eur J Prosthodont Restor Dent 2007; 15: 104-107.
Cobb C M, Carrara A, El-Annan E et al. Periodontal referral patterns, 1980 versus 2000: a preliminary study. J Periodontol 2003; 74: 1470-1474.
Linden G J. Variation in periodontal referral by general dental practitioners. J Clin Periodontol 1998; 25: 655-661.
Shaffie N, Cheng L. Improving the quality of oral surgery referrals. Br Dent J 2012; 213: 411-413.
Djemal S, Chia M, Ubaya-Narayange T. Quality improvement of referrals to a department of restorative dentistry following the use of a referral proforma by referring dental practitioners. Br Dent J 2004; 197: 85-88; discussion 82; quiz 100-101.
FGDP. Clinical examination and record-keeping good practice guidelines. London: Faculty of General Dental Practice, 2016.
Kourkouta S, Darbar U R. An audit of the quality and content of periodontal referrals and the effect of implementing referral criteria. Primary Dent Care 2006; 13: 99-106.
Cheshire P D, Saner P, Lesley R, Beckerson J, Butler M, Zanjani B. Dental practitioners with a special interest in periodontics: the West Sussex experience. Br Dent J 2011; 210: 127-136.
Drisko C L. Periodontal self-care: evidence-based support. Periodontol 2000 2013; 62: 243-255.
Axelsson P, Nystrom B, Lindhe J. The long-term effect of a plaque control program on tooth mortality, caries and periodontal disease in adults. Results after 30 years of maintenance. J Clin Periodontol 2004; 31: 749-757.
Needleman I, Nibali L, Di Iorio A. Professional mechanical plaque removal for prevention of periodontal diseases in adultssystematic review update. J Clin Periodontol 2015; 42 (Suppl 16): S12-35.
Tonetti M S, Eickholz P, Loos B G et al. Principles in prevention of periodontal diseases: Consensus report of group 1 of the 11th European Workshop on Periodontology on effective prevention of periodontal and peri-implant diseases. J Clin Periodontol 2015; 42 (Suppl 16): S5-11.
Newton J T, Asimakopoulou K. Managing oral hygiene as a risk factor for periodontal disease: a systematic review of psychological approaches to behaviour change for improved plaque control in periodontal management. J Clin Periodontol 2015; 42 (Suppl 16): S36-46.
Dental Protection. Periodontal monitoring. Available online at https://www.dentalprotection.org/new-zealand/publications-resources/clinical-audit-tools/clinical-audit-tools-display/2014/08/27/periodontal-monitoring (accessed November 2019).
Probing deeper into periodontics claims. Available online at https://www.theddu.com/guidance-and-advice/journals/march-2014/probing-deeper-into-periodontics-claims (accessed 19 January 2019).
Ghotane S G, Harrison V, Radcliffe E, Jones E, Gallagher J E. Enhanced skills in periodontology: evaluation of a pilot scheme for general dental practitioners and dental care professionals in London. Br Dent J 2017; 222: 700-707.
Cheshire P D. Why undertake outreach into general dental practice? Br Dent J 2002; 192: 371-374.
Ofori-Attah S. Dentistry, and why it is a great career. Br Dent J 2017; 223: 81-84.
Modgill O, Shah A. Compliance with the guide for commissioning oral surgery: an audit and discussion. Br Dent J 2017; 223: 509-514.
Chapple I L. Management of chronic periodontal diseases within the NHS. Br Dent J 2004; 196: 505.
The British Society of Periodontology. The good practitioner's guide to periodontology. England: The British Society of Periodontology, 2016.
Ali K, Slade A, Kay E, Zahra D, Tredwin C. Preparedness of undergraduate dental students in the United Kingdom: a national study. Br Dent J 2017; 222: 472-477.
Oxley C J, Dennick R, Batchelor P. The standard of newly qualified dental graduates - foundation trainer perceptions. Br Dent J 2017; 222: 391-395.
Cook J V, Dickinson H O, Eccles M P. Response rates in postal surveys of healthcare professionals between 1996 and 2005: an observational study. BMC Health Serv Res 2009; 9: 160.
Al-Haboubi M, Eliyas S, Briggs P F, Jones E, Rayan R R, Gallagher J E. Dentists with extended skills: the challenge of innovation. Br Dent J 2014; 217: E6.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Kalsi, A., Darbar, U. Initial periodontal therapy before referring a patient: an audit. Br Dent J 227, 977–983 (2019). https://doi.org/10.1038/s41415-019-1048-2
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41415-019-1048-2
