
Abstract
Objective: To establish patients’ perception of the effect of sport on rehabilitation.
Design: Single investigator telephone questionnaire survey.
Setting: Spinal Cord Injuries Unit, Musgrave Park Hospital, Belfast, Northern Ireland, UK.
Method: A telephone questionnaire was administered to patients admitted over a 12-month period. Information on patient demographics, sports participation before and after injury and patients’ perception of the impact of sports on rehabilitation was recorded.
Results: In all, 33 (84.6%) of the 39 patients could be contacted and all completed the questionnaire.
Of the respondents 27 (81.8%) had a diagnosis of spinal cord injury.
Six (18.2%) were female and 20 (60.6%) were below 45 years.
A total of 15 (45.5%) patients previously participated in regular sporting activity. At least 24 (72.7%) tried one sport during admission. In all, 14 reported taking part in regular sporting activity after discharge, although 23 expressed a desire to do so. Of those 60% who had regularly exercised continued to do so and 27% of those who reported no regular sport, before injury, commenced regular active exercise. A general benefit of sporting activity was recognised by 78.8% and a rehabilitation benefit by 69.7%. Self-reported benefits included increase in fitness, quality of life, confidence and social contact.
Conclusion: A high proportion of patients perceived sporting activity as beneficial. Patients exercising before injury were more likely to exercise after injury. All inpatients were introduced to sport by staff, emphasising the importance of this rehabilitation opportunity in planning in-patient care.
Similar content being viewed by others

Introduction
Cardiovascular disease is now an increasing cause of mortality in chronic spinal cord injury (SCI).1 The role of sporting activity in primary and secondary prevention of cardiovascular disease is established.2 Regular exercise is an activity conferring positive health benefit in the SCI population. Specifically, in SCI it has been shown to decrease medical complications, increase life expectancy and improve both quality of life and social interaction.3, 4 The aims of rehabilitation are often to maximise function, thus promoting independence, and to establish sound guidelines for the future. The objective of incorporating sporting activity is to obtain both physical and psychological gain for the spinal cord-injured individual.
It has previously been shown that wheelchair athletes have fewer hospital visits and admissions and fewer pressure sores.3 Intensive exercise helps to preserve bone mass in the upper limbs of males with SCI.5 Improved glucose tolerance has been found following electrical stimulation-assisted cycling.6 Risk factors for cardiovascular disease are ameliorated in spinal cord-injured individuals by exercise with reported increased cardiac dimensions,7 higher maximal work rate,7 increase in peak oxygen consumption,8 reduced breathlessness,9 and improved lipid profiles and glucose metabolism.10, 11, 12
The emphasis on patient-centred goal setting and patient involvement in rehabilitation planning in current practice suggests the importance of patients' perception of the value of a given activity. We wished to establish the perception of the role of sporting activity in rehabilitation and in general health among patients who had recently undergone rehabilitation in a SCI unit (SCIU). Baseline data were collected in an attempt to confirm the staff's impression of a low level of sports participation following discharge from rehabilitation.
Many sports are available for the wheelchair user, including: archery, basketball, bowling, cycling, football, flying, golf, horse riding, motorcycling, power lifting, quad rugby, road racing, scuba diving, shooting, skiing, softball, swimming, table tennis, tennis, triathlon and water skiing. Of these, not all are available in the rehabilitation setting. We wished to establish the level of sports participation, among persons who had received rehabilitation, in a SCIU, both pre- and postdiagnosis and during their in-patient stay. Treating therapists, during inpatient rehabilitation, often introduce patients to new sports or a return to sporting activity. We wished to establish how often this occurred.
Methods
Setting
The SCIU at Musgrave Park Hospital is a 15-bedded in-patient unit serving the population of Northern Ireland (1.7 million). It primarily admits patients with SCI and Guillain–Barré syndrome for rehabilitation.
Participants
Admissions to the SCIU for the calendar year 2001 were identified. A single investigator contacted the patients and conducted a structured telephone questionnaire. Information on patient demographics, regular sports participation (defined as three or more times per week) before and after injury and patients' perception of the impact of sports on rehabilitation was recorded. The questionnaire allowed yes/no responses regarding injury, sports participation, introduction to sport after diagnosis, and whether sport was felt to be of benefit in rehabilitation and the general health context. Free speech responses were encouraged, as to which benefits patients considered that sport provided, as well as any reasons given for lack of participation in sport.
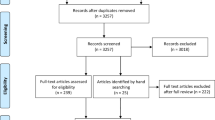
In all, 39 patients were identified for inclusion in the survey. They had been admitted for de novo rehabilitation from 1st January 2001 to 31st December 2001. Patients were nine to 23 months postdischarge at the time of questioning.
Results
Of the 39 patients, 33 (84. 6%) could be contacted and all completed the questionnaire.
Of the respondents, 27 (81.8%) had a diagnosis of SCI (paraplegia; n=12, tetraplegia; n=15) and six had Guillain–Barré Syndrome. A total of 16 (48.5%) were wheelchair users.
Six (18.2%) were female and 20 (60.6%) were below 45 years.
In all, 15 (45.5%) patients previously participated in regular sporting activity. Sporting activities included badminton, canoeing, cycling, football, golf, gymnasium workouts, hockey, jogging, rowing (coaching), squash, swimming, tennis and walking. Four sustained their injury as a result of sporting activity. During admission, at least one sport was tried by 24 (72.7%). All were introduced to these sports by the staff. The sports introduced in rehabilitation were bowling (n=19), archery (n=13), swimming (n=12), table tennis (n=7), basketball (n=1) and darts (n=1). Attending the United Kingdom Interspinal games allowed two patients to participate in sports unavailable locally (wheelchair rugby and shooting).
In all, 14 reported regular sporting activity after discharge (paraplegia; n=6, tetraplegia; n=4, GBS; n=4), although 23 expressed an aspiration to this. Those who regularly exercised after injury were mostly male (n=12) and aged 16–35 years (n=8), with three patients aged 36–55 years and three aged 56–65 participating in regular sport. Of those (60%) who had regularly exercised prediagnosis continued to do so after rehabilitation and 27% of those who reported no regular sport, before injury, commenced regular active exercise. Of the nine patients who did not try sports during rehabilitation, only two pursued regular sporting activity after discharge. Some patients offered reasons of poor access to sporting facilities and poor carer availability for exercise as their reason for lack of regular exercise (Table 1). The most popular exercise activity after rehabilitation was cardiovascular training at a gymnasium (n=6), followed by swimming (n=3) and bowling (n=2).
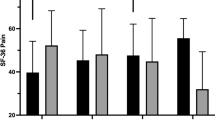
The general benefit of sporting activity was recognised by 78.8% of patients and the rehabilitation benefit by 69.7%. No perceived rehabilitation benefit from sporting activity was reported by 9.1%. Self-reported benefits were cited by 26 patients and included increases in fitness, quality of life, confidence and social contact (Table 2).
Discussion
This questionnaire study set out to establish the sports participation pre-and postdiagnosis of a group of patients after in-patient rehabilitation. The patient's opinions regarding the benefits, or otherwise, of sport in rehabilitation and general health were also sought.
It is well established that SCI is associated with reduced quality of life and increased incidence of anxiety and depression.13, 14 Wheelchair athletes have better psychological profiles than nonathletes.15 This benefit has been shown to increase with higher intensity participation.16 Based on measures of community integration, athletes with SCI score higher than nonathletes,4 implying improved social interaction as a result of exercise. Lack of adherence to an exercise programme has been shown to result in loss of the accrued psychological well being.17
Rehabilitation professionals should educate individuals with SCI about the potential adverse effects of sport also. A significant variation in prevalence of sports-related injuries (26–97%)18, 19 has been reported in wheelchair athletes. Injury has been attributed to trauma19 and overuse of functional limbs.20 Advice to wheelchair athletes on appropriate care of the shoulder in particular is recommended. Other adverse effects include autonomic dysreflexia and impaired temperature control21 in SCI lesions above T6 level. Careful consideration should be given to any return to contact sport. It has been suggested that those with permanent neurological deficit following cervical spine fracture should not partake in contact sport.22 An epidemiological study in Germany has reported 14.5% of traumatic SCI to be related to sport or diving accidents.23 Of patients admitted to Model Systems SCI care, 11.1% were reported to have sport as the aetiology of injury.24 Our sample has 10.3% of injuries due to sport.
The population studied reflects a 1 year admission intake for de novo rehabilitation within a regional unit. This, however, is a small sample. The mixed patient group with regard to age and sex may influence the likelihood of exercising as a leisure activity. The regional unit serves a mix of urban- and rural-based patients: the dynamics of local transport in rural areas, in particular, may influence accessibility to transport and sports venues. There were limited sports facilities available at the regional SCIU and the unit would seek to expand such services.
The rehabilitation team has an important opportunity to maximise health and potential to increase quality of life by introducing sport in rehabilitation. Patients, in this study group, appear to recognise that this is a positive and desirable area of rehabilitation. Patients, in this sample group who had previously regularly exercised were more likely than their counterparts to partake in sport after injury. It may be helpful therefore to strongly encourage and support those who have not had a previously active lifestyle. Promoting healthy living is an important aspect of rehabilitation, and the health benefits of regular exercise should be emphasised with patients given the opportunity to explore and establish exercise regimes with the therapy team after injury.
References
DeVivo MJ, Krause JS, Lammertse DP . Recent trends in mortality and causes of death among persons with spinal cord injury. Arch Phys Med Rehabil 1999; 80: 1411–1419.
Thompson PD et al. Exercise and physical activity in the prevention and treatment of atherosclerotic cardiovascular disease. A statement from the council on clinical cardiology (subcommittee on exercise, rehabilitation, and prevention) and the council on nutrition, physical activity, and metabolism (subcommittee on physical activity). Circulation 2003; 107: 3109–3116.
Curtis KA, McClanahan S, Hall KM, Dillon D, Brown KF . Health, vocational, and functional status in spinal cord injured athletes and nonathletes. Arch Phys Med Rehabil 1986; 67: 862–865.
Hanson CS, Nabavi D, Yuen HK . The effect of sports on level of community integration as reported by persons with spinal cord injury. Am J Occup Ther 2001; 55: 332–338.
Jones LM, Legge M, Goulding A . Intensive exercise may preserve bone mass of the upper limbs in spinal cord injured males but does not retard demineralization of the lower body. Spinal Cord 2002; 40: 230–235.
Jeon JY et al. Improved glucose tolerance and insulin sensitivity after electrical stimulation-assisted cycling in people with spinal cord injury. Spinal Cord 2002; 40: 110–117.
Schmid A et al. Physical performance and cardiovascular and metabolic adaptation of elite female wheelchair basketball players in wheelchair ergometry and in competition. Am J Phys Med Rehab 1998; 77: 527–533.
Jacobs PL, Nash MS, Rusinowski Jr JW . Circuit training provides cardiorespiratory and strength benefits in persons with paraplegia. Med Sci Sports Exerc 2001; 33: 711–717.
Ayas NT et al. Breathlessness in spinal cord injury depends on injury level. J Spinal Cord Med 1999; 22: 97–101.
Nash MS, Jacobs PL, Mendez AJ, Goldberg RB . Circuit resistance training improves the atherogenic lipid profiles of persons with chronic paraplegia. J Spinal Cord Med 2001; 24: 2–9.
Hjeltnes N et al. Exercise-induced overexpression of key regulatory proteins involved in glucose uptake and metabolism in tetraplegic persons: molecular mechanism for improved glucose homeostasis. FASEB J 1998; 12: 1701–1712.
Washburn RA, Figoni SF . High density lipoprotein cholesterol in individuals with spinal cord injury: the potential role of physical activity. Spinal Cord 1999; 37: 687–695.
Hancock KM, Craig AR, Dickson HG, Chang E, Martin J . Anxiety and depression over the first year of spinal cord injury: a longitudinal study. Paraplegia 1993; 31: 349–357.
Westgren N, Levi R . Quality of life and spinal cord injury. Arch Phys Med Rehab 1998; 79: 1433–1439.
Paulsen P, French R, Sherrill C . Comparison of wheelchair athletes and non-athletes on selected mood states. Percept Mot Skills 1990; 71: 1160–1162.
Muraki S, Tsunawake N, Hiramatsu S, Yamasaki M . The effect of frequency and mode of sports activity on the psychological status in tetraplegics and paraplegics. Spinal Cord 2000; 38: 309–314.
Ditor DS et al. Maintenance of exercise participation in individuals with spinal cord injury: effects on quality of life, stress and pain. Spinal Cord 2003; 41: 446–450.
Curtis KA, Dillon DA . Survey of wheelchair athletic injuries: common patterns and prevention. Paraplegia 1985; 23: 170–175.
Taylor D, Williams T . Sports injuries in athletes with disabilities: wheelchair racing. Paraplegia 1995; 33: 296–299.
Stiens SA, Haselkorn JK, Peters DJ, Goldstein B . Rehabilitation intervention for patients with upper extremity dysfunction: challenges of outcome evaluation. Am J Ind Med 1996; 29: 590–601.
Price MJ, Campbell IG . Thermoregulatory responses of spinal cord injured and able-bodied athletes to prolonged upper body exercise and recovery. Spinal Cord 1999; 37: 772–779.
Cantu RC, Bailes JE, Wilberger Jr JE . Guidelines for return to contact or collision sport after a cervical spine injury. Clin Sports Med 1998; 17: 137–146.
Schmitt H, Gerner HJ . Paralysis from sport and diving accidents. Clin J Sport Med 2001; 11: 17–22.
Nobunaga AI, Go BK, Karunas RB . Recent demographic and injury trends in people served by the Model Spinal Cord Injury Care Systems. Arch Phys Med Rehab 1999; 80: 1372–1382.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
O'Neill, S., Maguire, S. Patient perception of the impact of sporting activity on rehabilitation in a spinal cord injuries unit. Spinal Cord 42, 627–630 (2004). https://doi.org/10.1038/sj.sc.3101651
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.sc.3101651
