
Abstract
Inducible nitric oxide synthase (iNOS) plays an important role in the pathogenesis of atrial fibrillation (AF). The iNOS promoter has a CCTTT-repeat length polymorphism that can determine the level of gene transcription. This study enrolled 200 AF patients and 240 controls. The length of CCTTT-repeat polymorphism in the iNOS promoter region was examined by polymerase chain reactions, with the alleles with ≤11 repeats designated as S and alleles with ≥12 repeats designated as L alleles. AF patients carried significantly higher frequencies of the LL genotype than control subjects (40.0% versus 28.3%, P = 0.010). Multivariate analysis showed that the presence of LL genotype was significantly associated with AF (odds ratio: 1.87, 95% CI = 1.10–3.17, P = 0.021). In vitro, transient transfection assay in HL-1 atrial myocytes showed that the responsiveness of iNOS transcriptional activity to tachypacing was correlated with the length of the CCTTT-repeats. Right atrial tissues from patients with chronic AF were investigated with immunoconfocal microscopy. Patients with LL genotype exhibited greater oxidative stress and substrate remodeling in their atria than those with non-LL genotypes. Our results suggest that the iNOS microsatellite polymorphism may contribute to the genetic background of AF in Chinese-Taiwanese patients.
Similar content being viewed by others

Introduction
Atrial fibrillation (AF) is an abnormal heart rhythm that occurs as a consequence of atrial electrical or structural remodeling1. AF is frequently associated with other cardiovascular diseases such as hypertension, ischemic heart disease, valvular heart disease, and heart failure. However, 10% to 20% of patients with AF are free of concomitant diseases and do not have any known causes (so-called lone AF)1.
Although AF has been considered to be a non-genetic disorder, emerging evidence suggests a heritable linkage in many patients2,3. Genetic association studies have also demonstrated the significant contribution of single gene mutations and single nucleotide polymorphisms in the development of AF. For example, variations or polymorphisms in ion channel-, calcium handling protein-, fibrosis-, conduction-, and inflammation-related genes may render certain individuals susceptible to electrical or structural remodeling and eventually fibrillation in the atrium2,3.
Nitric oxide (NO) produced in the heart by nitric oxide synthase (NOS) is a highly reactive signaling molecule and an important modulator of myocardial function. NOS catalyzes the conversion of L-arginine to L-citrulline and NO, however under certain circumstances reactive oxygen species (ROS) can be formed instead of NO (uncoupling)4. Three NOS isoforms are found in the heart: neuronal NOS (nNOS, NOS1), endothelial NOS (eNOS, NOS3) and inducible NOS (iNOS, NOS2). nNOS and eNOS are Ca2+-dependent and constitutively present enzymes in distinct subcellular locations within cardiomyocytes5, whereas iNOS is absent in a healthy heart, however its expression is Ca2+-independent and induced by pro-inflammatory mediators and/or pathological states such as hypertrophy or heart failure6,7,8,9. The responsiveness of iNOS varies according to an individual’s inherited genetic profile. A (CCTTT)n pentanucleotide repeat polymorphism has been identified in the promoter region of the iNOS gene, and possible associations with various infectious, atopic, nasal polyp, inflammatory and autoimmune diseases have been investigated10,11,12,13,14,15,16,17,18. Studies using in vitro assays have revealed that iNOS promoter activity increases in parallel with the number of (CCTTT)n repeats, and that longer forms have higher transcription activity16,17,18. Nevertheless, relatively little is known about its role in predisposing individuals to AF. Since many studies have linked oxidative stress to the pathogenesis of AF19,20,21,22, the present study aims to test if rapid pacing would induce iNOS expression by the atrial myocyte, and to elucidate the association between the iNOS promoter microsatellite polymorphisms, the iNOS expression in atrial tissue, and the risk of AF.
Results
CCTTT repeat length polymorphisms in the iNOS promoter were associated with AF
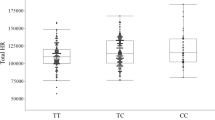
Table 1 presents the baseline characteristics of the 200 AF patients and 240 controls enrolled in this study. The frequencies of the classical risk factors for AF including hypertension, diabetes, and history of coronary artery disease (CAD) were slightly, but not significantly higher in the AF patients than in the controls. The concomitant use of medications was significantly different between the two groups. The allele frequencies of the (CCTTT)n microsatellites in the iNOS promoter region in the study population are shown in Fig. 1. The distribution of allele frequencies of the (CCTTT)n microsatellites in the iNOS promoter region was similar to that reported in a study from Japan10. The number of repeats ranged from 8 to 18. The difference in overall iNOS (CCTTT)n allelic distribution between the two groups was not significant, as determined by the Kolmogorov-Smirnov test (P = 0.739). The distribution of the number of (CCTTT)n repeats was skewed to the right, with (CCTTT)10 to (CCTTT)13 being the four most common alleles in our study cohort. Therefore, we classified the alleles into two subgroups in accordance with the best-fit grouping criteria and confirmed by sensitivity analysis (supplementary Table S1): short alleles (class S) including alleles with ≤11 repeats, and long alleles (class L) including alleles with ≥12 repeats. The subjects were then classified as having SS, SL, or LL genotypes according to each of their iNOS alleles. When the proportions of allele and genotype frequencies of the study population were analyzed, no significant differences were found in the distribution of allele frequencies between the control and AF groups (P = 0.167, Table 2). However, the distribution of genotypes was significantly different between the control and AF groups (P = 0.010, Table 2). The AF patients carried significantly higher frequencies of the LL genotype than the control subjects (40.0% versus 28.3%; P = 0.010). After adjusting for age, gender, body mass index (BMI), hypertension, diabetes, smoking, hypercholesterolemia, CAD, and the concomitant use of medications, the presence of the LL genotype remained significantly and independently associated with the risk of AF (odds ratio = 1.87, 95% confidence interval = 1.10–3.17; P = 0.021).

Frequency distribution of the (CCTTT)n repeats in normal controls (n = 240) and AF patients (n = 200).
Effect of the CCTTT repeats on iNOS transcriptional activity in rapidly paced HL-1 myocytes
Previous studies have demonstrated that rapid pacing of cultured HL-1 myocytes mimics the phenotypic feature of tachycardia-induced atrial remodeling in vivo23,24,25. Accordingly, we used this atrial-derived system to evaluate the effect of tachypacing in vitro. As shown in Fig. 2, time-dependent associations between the iNOS production of HL-1, as quantified by Western blot analysis, and the duration of atrial pacing were observed. To investigate whether the length of the CCTTT repeats affected the transcriptional regulation of the iNOS promoter by tachypacing, human iNOS promoter constructs containing different numbers of CCTTT repeats (5, 10, 14, 16, 17 and 19) were generated and transfected into HL-1 myocytes. As shown in Fig. 3, no significant differences between the baseline promoter activity and the length of the CCTTT repeats were observed in the HL-1 cells. However, there was a progressive increase in pacing-induced iNOS promoter activity with the plasmids contained increasing numbers of CCTTT repeats (Fig. 3). These results suggest that the length of the CCTTT repeats may modulate the responsiveness of iNOS transcriptional activity to tachypacing.

HL-1 cells were subjected to 4 Hz pacing for the indicated times. Bottom panel: the relative expression levels of iNOS and tubulin were quantified by densitometry and normalized to the control level, which was set at 1.0. Each value represents the mean ± SE of four independent experiments. One-way ANOVA with post hoc Tukey’s tests was applied for two groups and multiple comparisons. *P = 0.027 versus the controls. #P = 0.007 versus the controls.

Luciferase activity was assayed as described in the Methods section. HL-1 cells were transfected with plasmids containing various lengths of CCTTT repeats (N) in the iNOS promoter for 24 hours with/without subsequent tachypacing (4 Hz) for 2 hours. Each value (mean ± SE, at least three independent experiments) is expressed as a fold change in luciferase activity relative to the control (N = 0) condition. Two-way ANOVA reported a significant effect of various lengths of CCTTT repeats (P = 0.005), of pacing (P = 0.001), and of the interaction between the main effects (P = 0.001).
Association of the length of the CCTTT repeats with atrial oxidative stress in AF tissues
Our previous study showed that tachypacing promotes atrial structural remodeling, and especially myofibril degradation in atrial myocytes through increased oxidative stress25. To determine whether the CCTTT repeat polymorphisms affected AF-related oxidative stress and substrate remodeling, seven AF patients with four non-LL genotype and three LL genotype were chosen for comparison. Two sinus rhythm (SR) patients were designated as controls. The baseline characteristics of these nine patients are shown in the Table 3. We consistently found that oxidative stress (indicated by increased ROS generation, Fig. 4) and myofibril degradation (indicated by decreased myosin heavy chain (MHC) expression, Fig. 5) were more severe in the atria of the AF patients with LL genotype than in those with non-LL genotype and SR control. Taken together, these findings suggest that CCTTT repeat length polymorphisms may affect iNOS expression and consequent atrial structural remodeling responses in AF tissues.

Atrial tissues were stained with dihydroethidium to detect ROS generation as described in the Methods section. Representative confocal images show ROS production in the atria of seven AF patients (4 non-LL and 3 LL) and two controls (with sinus rhythm [SR]). Relative fluorescence density in the α-actin-expressing area was quantified (right). Data are expressed as mean ± SE. *Represents significant differences versus the controls (P = 0.001 for non-LL versus SR, P < 0.001 for LL versus SR). #Represents significant differences between non-LL and LL groups (P < 0.001). One-way ANOVA with post hoc Tukey’s tests was applied for two groups and multiple comparisons.

Representative confocal images show myosin degradation in the atria of seven AF patients (4 non-LL and 3 LL) and two controls (with sinus rhythm [SR]). Relative intensity of MHC in the α-actin-expressing area was quantified as described in the Methods section. Data are expressed as mean ± SE. *P = 0.004, SR versus LL groups. #P = 0.004, non-LL versus LL groups. One-way ANOVA with post hoc Tukey’s tests was applied for two groups and multiple comparisons.
Discussion
In this study, we demonstrated a significant association between (CCTTT)n pentanucleotide repeat polymorphisms in the iNOS gene promoter and susceptibility to AF in a Han Chinese population living in Taiwan. Individuals carrying two alleles with 12 or more repeats (high promoter activity genotype) exhibited a substantially increased risk of developing AF. Our results suggest that this functional iNOS gene polymorphism may contribute to the genetic background of AF.
The iNOS protein expression is barely detectable or undetectable in normal hearts. However, it can be highly expressed during heart failure due to stimulation via increased pro-inflammatory cytokine production such as interleukin-6 and tumor necrosis factor-alpha4,6. In humans, studies on gene expressions have shown an overexpression of iNOS mRNA and protein in the myocardium of patients with heart failure compared to that from unaffected controls8. Its expression has been detected in all four chambers, and it appears to be associated with the condition of heart failure per se rather than being related to the etiology of heart failure8,9. At low concentrations, NO may protect against apoptotic cell death induced by various stimuli, whereas it is cytotoxic at high concentrations26. In a recent study, Han et al. reported a significantly higher apoptosis index in the right atrium of patients with permanent AF compared to patients with SR, and a positive correlation with the expression of 3-nitrotyrosine (3NT; a biological marker of peroxynitrite), which was related to the increased expressions of iNOS and eNOS27. These findings suggest that an imbalance between iNOS and eNOS may contribute to cell apoptosis by affecting the expression of 3NT27. Of note, the left ventricle size and ejection fraction were comparable between the permanent AF and SR groups in Han’s study, suggesting that the induction of iNOS was not due to heart failure, but rather due to AF itself. Nishijima et al. recently reported increased iNOS and reduced tetrahydrobiopterin (BH4) expressions in failing atria in a 16-week canine tachypacing model of heart failure28. The authors found that this was associated with NOS uncoupling, as there was reduced NO production and increased O2• production in atrial tissue with increased atrial oxidative stress as measured by electron paramagnetic resonance spectroscopy. Furthermore, BH4 and L-arginine treatment reduced inducible AF and normalized the heart failure-induced shortening of the duration of left atrial myocyte action potential28. In a rat model of ischemic heart failure, increased atrial iNOS and Rac-1 activity was associated with atrial fibrosis and increased vulnerability to AF, both could be prevented by treatment with simvastatin which decreased myocardial oxidative stress and inflammation29. Taken together, these findings support that the induction of iNOS plays a role in contributing to atrial remodeling in AF.
Tachycardia-induced oxidative stress has been reported to be an important mediator in promoting and perpetuating AF1. Studies from our group and others have shown that oxidative stress mediates tachycardia-stimulated atrial remodeling25,30,31. Therefore, the responsiveness of an individual atrium to oxidative stress may determine its vulnerability to AF. Our findings support the notion that long CCTTT repeats in the iNOS promoter region may enhance its gene transcription in parallel with tachycardia, and subsequently increase oxidative stress and atrial remodeling. Longer CCTTT repeats have been found to increase iNOS transcriptional activity in several other cell types, including DLD-1 cells16 (human colon carcinoma cell line), human fibroblasts17 and HaCaT cells18 (human keratinocyte cell line). In this study, we did not find a significant association between baseline promoter activity and the length of the CCTTT repeats in HL-1 cells. However, we found that tachypacing-induced iNOS promoter activity in HL-1 cells was correlated with the length of the CCTTT repeats in the iNOS promoter. We further demonstrated that AF patients with LL genotype exhibited greater oxidative stress and substrate remodeling in their atria than AF patients with non-LL genotype and the SR controls, which was reflected by increased ROS generation and myofibril degradation in the atria of the AF patients homozygous for longer CCTTT repeats. It is conceivable that iNOS may locally damage the atrium by oxidative stress-induced remodeling. Taken together, our findings suggest that a combination of genetic polymorphisms and the consequent variations in NO-redox balance are involved in the pathogenesis of AF. However, we still cannot rule out the possibility that the observed association in our study is through other functional polymorphisms in linkage disequilibrium with the CCTTT repeats polymorphisms.
There are several limitations to this study. First, our findings were obtained from only one sample with a modest size. The same sample has been used in three genetic association studies before32,33,34. Thus, the study has a suspect validity when a multiple testing correction is stringently applied in multiple hypothesis-testing on the same sample (Bonferroni correction required p < 0.0125) and in the best-fit cutoff analysis. Replication in a second cohort with larger sample size would improve the strength of the analysis. However, our previous studies have different hypotheses under different a priori knowledge, which may not be a situation exactly like the multiple comparison scenario. Further, we and others consistently observed that the number of iNOS (CCTTT)n repeats above a certain threshold may be part of the causal pathway leading to the susceptibility of diseases11,12,13,14,15,17,18. The reason for the different (CCTTT)n cutoff points among different diseases could be that the effect size of iNOS (CCTTT)n repeats may not be exactly the same in different diseases and different study populations due to different environmental or genetic modifiers. Second, we did not assess the effect of the iNOS promoter CCTTT repeat polymorphisms on the local iNOS expression and 3NT levels in the atria of the patients with AF. Third, the cross-sectional nature of our study meant that we could not identify the cause and effect relationships between iNOS expression and AF-related atrial remodeling, or whether iNOS promoter polymorphisms could predict the future occurrence of AF in a normal individual. Finally, the study subjects were ethnically Chinese, and hence caution should be exercised when extrapolating our results to other ethnic groups.
Conclusion
In summary, we demonstrated that the length of the polymorphism of the CCTTT repeats in the iNOS promoter was associated with the risk of AF and AF-related structural remodeling. These findings provide further evidence that genetic variations may influence the responsiveness to oxidative stress and the susceptibility to AF.
Methods
Ethics Statement
The study protocol was approved by the Human Research Ethics Committee at Chang Gung Memorial Hospital (Chang Gung Medical Foundation Institutional Review Board 101–5030B and 100–3196C1), and this study was conducted in accordance with the Declaration of Helsinki Principles. Written informed consent was obtained from each participant.
Study population
The inclusion criteria were patients aged less than 65 years with unexplained causes of AF. Patients who had a history of hyperthyroidism, significant valvular heart disease (>grade II mitral regurgitation and/or aortic regurgitation), or congestive heart failure (left ventricular ejection fraction <50%) were excluded. A control group of patients with SR, comparable for age and gender, were recruited from individuals receiving routine health examinations. The demographic details of the study and control groups have been described elsewhere32,33,34.
Clinical assessment
The presence of AF was documented by patient history, serial electrocardiograms (ECGs), and/or ambulatory ECG monitoring. Transthoracic echocardiography was performed to assess left atrial and left ventricular functions and to detect significant valvular diseases. Left atrial enlargement and left ventricular dysfunction were defined as a diameter >40 mm and ejection fraction <50%, respectively. Hypertension was defined as blood pressure ≥140/90 mmHg and/or the use of antihypertensive medication. Definitions of hypercholesterolemia and diabetes mellitus were in accordance with the third report of the National Cholesterol Education Program and the guidelines of the American Diabetes Association, respectively.
Genomic DNA extraction
Genomic DNA was extracted from peripheral blood leukocytes and/or tissues using a Puregene DNA Isolation Kit (Qiagen, Minneapolis, MN).
Genotyping of iNOS promoter microsatellite polymorphisms
The 5′-flanking region containing (CCTTT)n repeats of the iNOS gene was amplified by polymerase chain reaction (PCR) with a FAM-labeled sense primer, 5′-ACCCCTGGAAGCCTACAACTGCAT-3′, and an antisense primer, 5′-GCCACTGCACCCTAGCCTGTCTCA-3′, according to a published procedure35. The PCR products were mixed together with GenoType TAMRA DNA ladder (size range, 50–500 bp; GibcoBRL) and analyzed on an automated DNA sequencer (ABI Prism 377). The respective sizes of the (CCTTT)n repeats were calculated using GeneScan Analysis software (PE Applied Biosystems). To further confirm the sizes of the (CCTTT)n repeats, three PCR products were subcloned into the pCRII vector (Invitrogen), and the resulting purified plasmid DNA was subjected to sequence analysis. For quality control purposes, approximately 10% of the samples were re-genotyped in a blind fashion, and the same results were obtained.
Human samples
Right atrial appendages were obtained from seven patients with AF and two controls with SR undergoing open heart surgery. After excision, the atrial appendages were immediately frozen in liquid nitrogen and stored at −85 °C. Subsequently, genomic DNA from each subject was sent for genotyping as described above.
Immunohistochemical analysis
Immunohistochemical analysis was performed using α-actin, iNOS, and MHC primary antibodies (Abcam, Cambridge, MA) followed by fluorescein isothiocyanate or Cy3-conjugated secondary antibodies (Chemicon, Temecula, CA). Nuclei were visualized by DAPI staining. Myosin degradation was quantified as the area containing cytoplasmic myosin (MHC) divided by the area containing nuclei. For each analysis, at least five random fields were chosen to observe >30 myocytes. ROS in the atria were measured using a fluorescent dye, dihydroethidium, a cell-permeable indicator of ROS. The tissue samples were pre-incubated with 10 μmol/L dihydroethidium for 30 minutes at room temperature, and ROS-mediated fluorescence was observed under a confocal microscope (Leica TCS SP2, Wetzlar, Germany), with excitation at 543 nm using an argon laser and emission recorded using a long pass (>600 nm) filter set to acquire two-dimensional images (512 × 512 pixels).
Cell culture and tachypacing
HL-1 atrial myocytes were maintained in Claycomb medium as described previously36. HL-1 cells (≥1 × 106 cells) on 4-well rectangular dishes (Nunclon, Netherlands) were placed into C-Dish 100TM-Culture Dishes (IonOptix, Milton, MA). The HL-1 cells were then subjected to field stimulation with 10-ms stimuli of 40 V intensity at 4 Hz frequency (1.5 V/cm field strength; C-Pace EP culture pacer, IonOptix)23,24,25. The spontaneous contraction rate was about 0.5 to 1 Hz, and a capture efficiency of >90% was confirmed by microscopic examination.
Constructs and transfection
The iNOS promoters (−1557 bp to +58 bp) were amplified from genomic DNA by PCR using the forward primer 5′-GAAACGCGTGATTCTGACTCTTTCC-3′ and reverse primer 5′-CAAAGATCTGGAATGAGGCTGAGTTC-3′. The PCR products were inserted into the pGL3 basic vector (Promega, Madison, WI) at the MluI/BglII restriction sites. The iNOS promoters containing various lengths of CCTTT repeats were amplified from the genomic DNAs of the patients with AF by PCR using the forward primer 5′-CCTGGTACCCCTGGAAGCCTACAACTG-3′ and reverse primer 5′- CAAACGCGTGGCTGCAGAGAGCTA-3′ according to a previously published procedure17. The PCR products were then cloned into the upstream of the inserted iNOS gene promoter in pGL3 at KpnI/MluI restriction sites. For transient transfection assays, HL-1 myocytes grown to 50% to 60% confluence were transfected with the indicated plasmids using LipofectAMINE 2000 (Invitrogen) according to the manufacturer’s instructions. The transfection efficiency using this method was approximately 60%. Luciferase activities were measured with a luminometer (Luminoskan TL PMS, Thermo Lab Systems, Grand Rapids, OH).
Statistical analysis
Continuous variables were expressed as mean ± SD and tested using a two-sample t-test. The chi-square test was used to examine differences in categorical variables and to compare allele and genotype frequencies. The Kolmogorov-Smirnov test was used to compare the shape of the allele frequency distribution. Sensitivity analysis was used to test all possible grouping criteria, which then classified the (CCTTT)n repeats into two groups in the logistic regression models, using AF as the dependent variable and the allele groups as independent variables. Binary logistic regression analysis was used to evaluate the independent effect of genotype on the association with AF after adjusting for age, gender, BMI, hypertension, diabetes, smoking, hypercholesterolemia, CAD, and the use of concomitant medications. One-way ANOVA with post hoc Tukey’s tests were used for two groups and multiple comparisons. A two-way ANOVA was used to assess the main effects of various lengths of CCTTT repeats, tachypacing and their interaction on the iNOS transcriptional activity. A value of p < 0.05 using a two-sided test was considered to be statistically significant. All statistical analyses were performed using SPSS software version 20.0 (SPSS Inc., Chicago, IL). Missing data were approached with listwise deletion.
Additional Information
How to cite this article: Hsu, L.-A. et al. Association evidence of CCTTT repeat polymorphism in the iNOS promoter and the risk of atrial fibrillation in Taiwanese. Sci. Rep. 7, 42388; doi: 10.1038/srep42388 (2017).
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
Schotten, U., Verheule, S., Kirchhof, P. & Goette, A. Pathophysiological mechanisms of atrial fibrillation: a translational appraisal. Physiol. Rev. 91, 265–325 (2011).
Andalib, A., Brugada, R. & Nattel, S. Atrial fibrillation: evidence for genetically determined disease. Curr. Opin. Cardiol. 23, 176–183 (2008).
Tsai, C. T., Lai, L. P., Hwang, J. J., Lin, J. L. & Chiang, F. T. Molecular genetics of atrial fibrillation. J. Am. Coll. Cardiol. 52, 241–250 (2008).
Umar, S. & van der Laarse, A. Nitric oxide and nitric oxide synthase isoforms in the normal, hypertrophic, and failing heart. Mol. Cell. Biochem. 333, 191–201 (2010).
Barouch, L. A. et al. Nitric oxide regulates the heart by spatial confinement of nitric oxide synthase isoforms. Nature 416, 337–339 (2002).
Balligand, J. L. et al. Cytokine-inducible nitric oxide synthase (iNOS) expression in cardiac myocytes. Characterization and regulation of iNOS expression and detection of iNOS activity in single cardiac myocytes in vitro . J. Biol. Chem. 269, 27580–27588 (1994).
Winlaw, D. S. et al. Increased nitric oxide production in heart failure. Lancet 344, 373–374 (1994).
Haywood, G. A. et al. Expression of inducible nitric oxide synthase in human heart failure. Circulation 93, 1087–1094 (1996).
Vejlstrup, N. G. et al. Inducible nitric oxide synthase (iNOS) in the human heart: expression and localization in congestive heart failure. J. Mol. Cell. Cardiol. 30, 1215–1223 (1998).
Xu, W. et al. Survey of the allelic frequency of a NOS2A promoter microsatellite in human populations: assessment of the NOS2A gene and predisposition to infectious disease. Nitric Oxide 4, 379–383 (2000).
Ohashi, J. et al. Significant association of longer forms of CCTTT Microsatellite repeat in the inducible nitric oxide synthase promoter with severe malaria in Thailand. J. Infect. Dis. 186, 578–581 (2002).
Konno, S., Hizawa, N., Yamaguchi, E., Jinushi, E. & Nishimura, M. (CCTTT)n repeat polymorphism in the NOS2 gene promoter is associated with atopy. J. Allergy Clin. Immunol. 108, 810–814 (2001).
Pascual, M. et al. (CCTTT)n polymorphism of NOS2A in nasal polyposis and asthma: a case-control study. J Investig Allergol Clin Immunol. 18, 239–244 (2008).
Gonzalez-Gay, M. A. et al. Inducible but not endothelial nitric oxide synthase polymorphism is associated with susceptibility to rheumatoid arthritis in northwest Spain. Rheumatology 43, 1182–1185 (2004).
Martin, J. et al. Inducible nitric oxide synthase polymorphism is associated with susceptibility to Henoch-Schönlein purpura in northwestern Spain. J. Rheumatol. 32, 1081–1085 (2005).
Warpeha, K. M. et al. Genotyping and functional analysis of a polymorphic (CCTTT)(n) repeat of NOS2A in diabetic retinopathy. FASEB J. 13, 1825–1832 (1999).
Kawaguchi, Y. et al. NOS2 polymorphisms associated with the susceptibility to pulmonary arterial hypertension with systemic sclerosis: contribution to the transcriptional activity. Arthritis Res. Ther. 8, R104 (2006).
Chang, Y. C. et al. The (CCTTT)n pentanucleotide repeat polymorphism in the inducible nitric oxide synthase gene promoter and the risk of psoriasis in Taiwanese. Arch. Dermatol. Res. 307, 425–432 (2015).
Dudley, S. C. Jr. et al. Atrial fibrillation increases production of superoxide by the left atrium and left atrial appendage: role of the NADPH and xanthine oxidases. Circulation 112, 1266–1273 (2005).
Kim, Y. M. et al. A myocardial Nox2 containing NAD(P)H oxidase contributes to oxidative stress in human atrial fibrillation. Circ. Res. 97, 629–636 (2005).
Adam, O. et al. Role of Rac1 GTPase activation in atrial fibrillation. J. Am. Coll. Cardiol. 50, 359–367 (2007).
Kim, Y. M. et al. Association of atrial nicotinamide adenine dinucleotide phosphate oxidase activity with the development of atrial fibrillation after cardiac surgery. J. Am. Coll. Cardiol. 51, 68–74 (2008).
Yang, Z., Shen, W., Rottman, J. N., Wilswo, J. P. & Marray, K. T. Rapid stimulation causes electrical remodeling in cultured atrial myocytes. J. Mol. Cell Cardiol. 38, 299–308 (2005).
Mace, L. C. et al. Transcriptional remodeling of rapidly stimulated HL-1 atrial myocytes exhibits concordance with human atrial fibrillation. J. Mol. Cell Cardiol. 47, 485–492 (2009).
Yeh, Y. H. et al. Transforming growth factor-beta and oxidative stress mediate tachycardia-induced cellular remodeling in cultured atrial-derived myocytes. Cardiovasc. Res. 91, 62–70 (2011).
Kröncke, K. D., Fehsel, K. & Kolb-Bachofen, V. Inducible nitric oxide synthase in human diseases. Clin. Exp. Immunol. 113, 147–156 (1998).
Han, W. et al. Nitric oxide overproduction derived from inducible nitric oxide synthase increases cardiomyocyte apoptosis in human atrial fibrillation. Int. J. Cardiol. 130, 165–173 (2008).
Nishijima, Y. et al. Tetrahydrobiopterin depletion and NOS2 uncoupling contribute to heart failure-induced alterations in atrial electrophysiology. Cardiovasc. Res. 91, 71–79 (2011).
Cho, K. I. et al. Simvastatin attenuates the oxidative stress, endothelial thrombogenicity and the inducibility of atrial fibrillationin a rat model of ischemic heart failure. Int. J. Mol. Sci. 15, 14803–14818 (2014).
Carnes, C. A. et al. Ascorbate attenuates atrial pacing-induced peroxynitrite formation and electrical remodeling and decreases the incidence of postoperative atrial fibrillation. Circ. Res. 89, 32e–38e (2001).
Shiroshita-Takeshita, A., Schram, G., Lavoie, J. & Nattel, S. Effect of simvastatin and antioxidant vitamins on atrial fibrillation promotion by atrial-tachycardia remodeling in dogs. Circulation 110, 2313–2319 (2004).
Tung, Y. C. et al. C-Reactive Protein Gene Polymorphisms and the Risk of Atrial Fibrillation in a Chinese Population in Taiwan. Acta Cardiologica Sinica 29, 208–216 (2013).
Hsu, L. A. et al. Microsatellite polymorphism in the heme oxygenase-1 gene promoter and the risk of atrial fibrillation in Taiwanese. PLoS One 9, e108773 (2014).
Hsiao, F. C. et al. MMP9 Rs3918242 Polymorphism Affects Tachycardia-Induced MMP9 Expression in Cultured Atrial-Derived Myocytes but Is Not a Risk Factor for Atrial Fibrillation among the Taiwanese. Int. J. Mol. Sci. 17(4) (2016).
Xu, W., Liu, L. Z., Emson, P. C., Harrington, C. R. & Charles, I. G. Evolution of a homopurine-homopyrimidine pentanucleotide repeat sequence upstream of the human inducible nitric oxide synthase gene. Gene 204, 165–170 (1997).
Claycomb, W. C. et al. HL-1 cells: a cardiac muscle cell line that contracts and retains phenotypic characteristics of the adult cardiomyocyte. Proc. Natl. Acad. Sci. USA 95, 2979–2984 (1998).
Acknowledgements
This study was supported by grants from the Ministry of Science and Technology [102-2314-B-182-034- to L-A Hsu] and Chang Gung Research Grant Foundation [CMRPG3E1591 to F-C Tsai, and CMRPG3F0041 to C-T Kuo].
Author information
Authors and Affiliations
Contributions
L.A.H. participated in genotyping, performed statistical analysis and drafted the manuscript. W.J.C., C.T.K., C.L.W., Y.H.Y., L.A.H., C.J.C. and F.C.T. participated in sample collection. H.Y.T. prepared the DNA samples and participated in the promoter assays. H.Y.T., Y.H.C. and Y.H.Y. participated in cell culture and tachypacing. W.J.C. and H.Y.T. participated in immunohistochemical analysis. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Supplementary information
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Hsu, LA., Yeh, YH., Chen, WJ. et al. Association evidence of CCTTT repeat polymorphism in the iNOS promoter and the risk of atrial fibrillation in Taiwanese. Sci Rep 7, 42388 (2017). https://doi.org/10.1038/srep42388
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep42388
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
