
Abstract
Both visual acuity (VA) and contrast sensitivity (CS) are important parameters for measuring visual function. In this research, we investigated the CS of patients with ametropic or anisometropic amblyopia, whose corrected visual acuity (CVA) recovered to 1.0. Fifty-five cases with amblyopia and 22 control cases with a normal visual acuity of 1.0 were enrolled. The CS of the patients whose ametropic amblyopia had recovered to a CVA of 1.0 at 18 cpd spatial frequency was still lower than that of the normal control group under both photopic and scotopic conditions (P = 0.001, 0.025), but there were no significant differences at low- and middle-spatial frequencies. The CS of amblyopic eyes of the patients with anisometropic amblyopia was lower than that of the normal control group at the 18 cpd spatial frequency under photopic conditions (P = 0.005), and at the 6 cpd, 12 cpd, and 18 cpd spatial frequencies under scotopic conditions (P = 0.008, <0.001, 0.004, respectively). The CS between the amblyopic eyes and the sound eyes of patients with anisometropic amblyopia presented significant differences at the 6 cpd, 12 cpd, and 18 cpd spatial frequencies under scotopic conditions (P = 0.025, 0.045, 0.019, respectively). We suggest that amblyopia treatment should involve not only the correction of VA but also the improvement of CS.
Similar content being viewed by others
Introduction
Amblyopia, which is the most common visual disorder among children, is a neurological disorder of binocular vision resulting from a disrupted visual experience during early visual development1. It affects visual acuity (VA), contrast sensitivity (CS), visual field, and stereoacuity2. VA and CS are two different but important parameters that are used to measure visual function. VA describes visual function under high contrast conditions3. CS testing, which characterizes the visual function under different spatial frequencies and different luminance, is another powerful technique to quantify the capability of the visual system4. However, CS is often neglected in clinical research. Compared with VA, CS can better describe the visual function in some cases5. Our research investigated the changes in CS among patients with ametropic or anisometropic amblyopia in achieving the corrected visual acuity (CVA) of 1.0.
Material and Methods
Participants
Patients with lower visual acuity than their normal peers were selected. All patients who cooperated with us in this study had no strabismus, no non-centric fixation, no keratopathy, and no cataracts or other diseases in their eyes. Fifty-seven cases (male 34, female 23; mean, 8.51 years; SD, 1.894 years) with ametropic and anisometropic amblyopia whose CVA had recovered to 1.0 after amblyopia therapy and 22 cases (male 17, female 5; mean, 8.23 years; SD, 1.541 years) with normal visual acuity of 1.0 were enrolled in this study between May 2011 and November 2012. Among the 57 cases with ametropic or anisometropic amblyopia, there were 34 cases (the spherical equivalent is 4.24 ± 2.130DS) with middle or high hyperopia of both eyes and 23 cases (the spherical equivalent of the amblyopic eye is 4.32 ± 2.175 DS, and the spherical equivalent of the non-amblyopic eye is 2.00 ± 1.663 DS) with anisometropia.
All patients were divided into three groups: the ametropic amblyopic group (MA), anisometropic amblyopic group (NA), and the normal control group (NC). The difference in spherical power and the astigmatic power between the two eyes was at least 1.5D and 1.0D, respectively, in the anisometropic amblyopic group.
Ethical approval and informed consent
Research protocol was approved by the Ethics Committee of Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology. The informed consents about the follow-up examination were obtained from all the patients. All experiments were performed in accordance with the Declaration of Helsinki.
Measurements of visual acuity
The measurements of visual acuity employed the international standard vision acuity chart (E chart, Shengde Company, China), the background luminance of which was 300 cd/m2 by a LCD monitor. The 1.0 lines of the chart were at the same height as the eyes. The chart was 5 meters away from the subject.
Measurements of contrast sensitivity
The refractive error of all patients with amblyopia was corrected by wearing glasses. The sinusoidal gratings were used as the contrast sensitivity testing standards to conduct the Functional Acuity Contrast Test (OPTEC® 6500 visual function tester (Stereo Company, U.S.)). The brightness values were 85 cd/m2 (light) and 3 cd/m2 (dark), respectively. The spatial frequencies of the sinusoidal grating were 1.5 cpd, 3.0 cpd, 6.0 cpd, 12.0 cpd, and 18.0 cpd. The right and left eyes were tested, separately. The test was carried out in the following steps: The remote switch was turned on to simulate the test distance of 6 m. Then, the Day button was pressed to test the bright mode using the 5 # to 9 # test pictures. Finally, the Night button was pressed for the dark mode test. If the answer was correct, the next test picture was presented; if not, the last correct answer was recorded6.
Statistical analyses
The data were analysed using a paired t-test by the Statistical Package for Social Sciences (SPSS) software (Version 17.0). P-values less than 0.05 were considered statistically significant.
Results
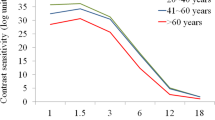
Table 1 and Fig. 1 show the contrast sensitivity of the three groups under photopic and scotopic conditions.

Error bars show 95%CIs. P-value of <0.05 was considered statistically significant.
The differences between the ametropic amblyopic group and the normal control group
Table 2 shows that the two groups exhibited significant differences at 18 cpd under both the photopic and the scotopic conditions (P = 0.001, 0.025).
The differences between the amblyopic eyes (AE) of the anisometropic amblyopic group and the normal control group
Table 3 shows significant differences at 18 cpd under the photopic conditions (P = 0.005) and 6 cpd, 12 cpd,and 18 cpd under the scotopic conditions (P = 0.008, <0.001, 0.004).
The differences between the non-amblyopic eyes (nAE) of the anisometropic amblyopic group and the normal control group
Table 4 shows no differences between the groups under both photopic and scotopic conditions at all spatial frequencies.
The differences between the non-amblyopic eyes and the corresponding amblyopic eyes in the anisometropic amblyopic group
Table 5 shows no differences between the non-amblyopic eyes and the corresponding amblyopic eyes in the anisometropic amblyopic group under photopic conditions. Differences were shown at 6 cpd, 12 cpd, and 18 cpd under scotopic conditions (P = 0.025, 0.045, 0.019).
Discussion
CS is an important parameter in detecting visual dysfunction. There are two pathways from the retina to cortex: the parvocellular and the magnocellular pathways7. Both of them could transform and distribute information to the visual cortex (V1)8. The parvocellular system is selectively sensitive to middle to high spatial frequencies (low temporal frequencies); however, the magnocellular system is sensitive to a very broad temporal frequency range (low spatial frequencies)9. The contrast-sensitivity function (CSF) is controlled by the spatiotemporal characteristics of the visual pathway. The magnocellular system forms the basis of the achromatic CSF and dominates close-to-threshold detection. When the magnocellular system saturates, the parvocellular system dominates the higher contrast detection10.
Amblyopia is a disease with visual abnormality, such as visual acuity, binocular function, and contrast sensitivity11. Amblyopia showed decreased contrast sensitivity under mesopic conditions and at intermediate spatial frequencies12. The visual acuity was significantly better correlated with improved CS during amblyopia treatment13. Despite the significant correlation between VA and CS, VA cannot predict CS14. VA is a measure of the resolution under high contrast. CS is a measure of the ability to distinguish the visual markers under different levels of contrast. The latter is more adaptively used in daily life. Unlike other studies that focused on the lower visual acuity of patients with ametropic amblyopia or anisometropic amblyopia, our study focused on the contrast sensitivity of those whose visual acuity had recovered to 1.0.
Our study demonstrated that different types of amblyopia still had contrast sensitivity dysfunction at different spatial frequencies, even when the CVA had recovered to 1.0. The CS dysfunction of the ametropic amblyopia emerged at a high spatial frequency. The CS dysfunction of the anisometropic amblyopia was observed at middle and high spatial frequencies, particularly under scotopic conditions. This result indicated that the recovery of the visual function was different from the low spatial frequency to the high spatial frequency during amblyopia treatment, and the parvocellular system remained uncured, even when the CVA recovered to 1.0.
Compared with photopic visual function mediated by the cone cells, mesopic visual function is more complex because it requires that the rod cells and the cone cells interact with each other properly15. This might be why the CS under scotopic conditions is more difficult to recover.
Although the visual acuity of patients with amblyopia had recovered to 1.0, their contrast sensitivity did not return to the normal range simultaneously. In other words, these patients had lower resolution capacities than did those with normal contrast sensitivity, especially under a dark environment. Therefore, we suggest that researchers focus on the improvement of visual acuity and the development of contrast sensitivity during the amblyopia treatment. Perhaps future studies should be directed toward evaluating the impact of reduced contrast sensitivity on the quality of life of patients with a history of amblyopia treatment in whom visual acuity was successfully restored to 1.0. Our findings have enriched the body of knowledge about amblyopia treatment in clinical work.
Additional Information
How to cite this article: Wang, G. et al. An Assessment of the Contrast Sensitivity in Patients with Ametropic and Anisometropic Amblyopia in Achieving the Corrected Visual Acuity of 1.0. Sci. Rep. 7, 42043; doi: 10.1038/srep42043 (2017).
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
Zhou, J., Thompson, B. & Hess, R. F. A new form of rapid binocular plasticity in adult with amblyopia. Scientific reports 3, 2638, doi: 10.1038/srep02638 (2013).
Webber, A. L. & Wood, J. Amblyopia: prevalence, natural history, functional effects and treatment. Clinical & experimental optometry 88, 365–375 (2005).
Bartholomew, A. J., Lad, E. M., Cao, D. et al. Individual Differences in Scotopic Visual Acuity and Contrast Sensitivity: Genetic and Non-Genetic Influences. PloS one 11, e0148192, doi: 10.1371/journal.pone.0148192 (2016).
Jindra, L. F. & Zemon, V. Contrast sensitivity testing: a more complete assessment of vision. Journal of cataract and refractive surgery 15, 141–148 (1989).
Richman, J., Spaeth, G. L. & Wirostko, B. Contrast sensitivity basics and a critique of currently available tests. Journal of cataract and refractive surgery 39, 1100–1106, doi: 10.1016/j.jcrs.2013.05.001 (2013).
Fahey, P. K. & Burkhardt, D. A. Effects of light adaptation on contrast processing in bipolar cells in the retina. Visual neuroscience 18, 581–597 (2001).
Nassi, J. J. & Callaway, E. M. Parallel processing strategies of the primate visual system. Nature reviews. Neuroscience 10, 360–372, doi: 10.1038/nrn2619 (2009).
Sincich, L. C. & Horton, J. C. The circuitry of V1 and V2: integration of color, form, and motion. Annual review of neuroscience 28, 303–326, doi: 10.1146/annurev.neuro.28.061604.135731 (2005).
Al-Hashmi, A. M., Kramer, D. J. & Mullen, K. T. Human vision with a lesion of the parvocellular pathway: an optic neuritis model for selective contrast sensitivity deficits with severe loss of midget ganglion cell function. Experimental brain research 215, 293–305, doi: 10.1007/s00221-011-2896-4 (2011).
Plainis, S. & Murray, I. J. Magnocellular channel subserves the human contrast-sensitivity function. Perception 34, 933–940 (2005).
McKee, S. P., Levi, D. M. & Movshon, J. A. The pattern of visual deficits in amblyopia. Journal of vision 3, 380–405, doi: 10.1167/3.5.5 (2003).
Lew, H., Seong, G. J., Kim, S. K. et al. Mesopic contrast sensitivity functions in amblyopic children. Yonsei medical journal 44, 995–1000, doi: 10.3349/ymj.2003.44.6.995 (2003).
Moseley, M. J., Stewart, C. E., Fielder, A. R. et al. Intermediate spatial frequency letter contrast sensitivity: its relation to visual resolution before and during amblyopia treatment. Ophthalmic & physiological optics: the journal of the British College of Ophthalmic Opticians 26, 1–4, doi: 10.1111/j.1475-1313.2005.00343.x (2006).
Haegerstrom-Portnoy, G., Schneck, M. E., Lott, L. A. et al. The relation between visual acuity and other spatial vision measures. Optometry and vision science: official publication of the American Academy of Optometry 77, 653–662 (2000).
Cao, D., Lee, B. B. & Sun, H. Combination of rod and cone inputs in parasol ganglion cells of the magnocellular pathway. Journal of vision 10, 4, doi: 10.1167/10.11.4 (2010).
Acknowledgements
This work is supported by the National Natural Science Foundation of China (No. 81272657).
Author information
Authors and Affiliations
Contributions
Ping Wang conceived and designed the experiments. Guipan Wang and Congling Zhao performed the experiments. Guipan Wang analyzed the data. Qiang Ding contributed reagents materials/analysis tools. Guipan Wang and Congling Zhao wrote the paper. Qiang Ding designed the software used in analysis.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Wang, G., Zhao, C., Ding, Q. et al. An Assessment of the Contrast Sensitivity in Patients with Ametropic and Anisometropic Amblyopia in Achieving the Corrected Visual Acuity of 1.0. Sci Rep 7, 42043 (2017). https://doi.org/10.1038/srep42043
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep42043
This article is cited by
-
Vision training with VEP biofeedback in amblyopia after the critical period
Documenta Ophthalmologica (2020)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
