
Abstract
Robert Heinrich Herman Koch, a German physician and microbiologist, received Nobel Prize in 1905 for identifying the specific causative agent of tuberculosis (TB). During his time it was believed that TB was an inherited disease. However he was convinced that the disease was caused by a bacterium and was infectious, tested his postulates using guinea pigs, and found the causative agent to be slow growing mycobacterium tuberculosis. TB is the second most common cause of death from infectious diseases after HIV/AIDS. Drug-resistant TB poses serious challenge to effective management of TB worldwide. Multidrug-resistant TB accounted for about half a million new cases and over 200,000 deaths in 2013. Whole-genome sequencing (first done in 1998) technologies have provided new insight into the mechanism of drug resistance. For the first time in 50 y, new anti TB drugs have been developed. The World Health Organization (WHO) has recently revised their treatment guidelines based on 32 studies. In United States, latent TB affects between 10 and 15 million people, 10% of whom may develop active TB disease. QuantiFERON TB Gold and T-SPOT.TB test are used for diagnosis. Further research will look into the importance of newly discovered gene mutations in causing drug resistance.
Similar content being viewed by others


Main
Tuberculosis (TB) is a potentially curable disease yet so challenging. Historically, it is referred to as “Captain of death” (1). Tuberculosis is a global problem as such every nation is battling with new cases especially among immigrant populations. Although death related to tuberculosis has declined in the last decade, it remains a threat to mankind. Worldwide control measures are underway but progress is hindered by the HIV-1 epidemic, drug resistance and other factors like malnutrition, diabetes, overcrowding, and poor resources (2). Tuberculosis in children has additional challenges; is under-reported; diagnosis is difficult, and those less than 2 y old are at higher risk of extra-pulmonary tuberculosis.
Mycobacterium tuberculosis is an acid-fast bacillus. Humans are the only reservoir. Its intrinsic nature and other epidemiologic factors make eradication difficult. Once inhaled by aerosol, a human’s immune system can eradicate an infection (50–75%) or succumb to active tuberculosis disease (5–10%). The infection can remain dormant for many years as latent TB (90–95% of patients) or it can reactivate into active disease (3,4).
Mycobacterium has existed for thousands of years based on the evidence of disease found in Egyptian mummies more than 5,000 y ago and was considered an inherited disease until Hermann Heinrich Robert Koch, a German physician and microbiologist, identified it as the specific causative agent for tuberculosis in1882. TB was noted in East Africa over 70,000 y ago before the Europeans’ arrival in the 19th century. Migration of humans carrying this disease was explained by the description of TB in other countries like India and China (5). Before Koch’s discovery, Hippocrates recognized it as phthisis and consumption, Clarisssimus Galen wrote about it. Fransiscus de la Boë coined the term tubercle found in the lungs; scrofula was recognized in Europe during the Middle Ages and was cured by royal touch. Laennec described the pathology of TB, and an experimental animal study was first done on rabbits in 1865. Since then, there has been tremendous progress in tests, medications, and management ( Figure 1 ) related to TB (6). Traditionally for diagnosis, AFB smear test has poor sensitivity and standard culture is limited by the long 6–8 wk needed for growth of Mycobacterium. New developments such as the interferon-γ Release Assay (IGRA) and Xpert MTB/RIF are revolutionizing the diagnosis of tuberculosis. Xpert MTB/RIF has shortened drug susceptibility testing results as well (7).

Timeline in tuberculosis associated with events and discoveries by notable people.
Whole-genome sequencing technologies first done in1998 have provided new insight into the mechanism of drug resistance. For the first time in 50 y, new anti-TB drugs have been developed. Enough new information based on 32 studies has become available that WHO has recently revised their treatment guidelines. Centers for Disease Control and Prevention now recommends 3-mo directly observed therapy using Isoniazid (INH) and Rifapentine (RPT) as an option for treating latent TB infection (LTBI) based on the results of randomized controlled studies (8). SHINE trial was launched in July 2016 which is a large-scale randomized pediatric TB trial over 4 y period to examine the effectiveness of 4 mo treatment course. This review article focuses on the changing landscape in the diagnosis of TB in children and the future diagnostics and therapeutics for multidrug-resistant tuberculosis (MDR-TB).
Epidemiology
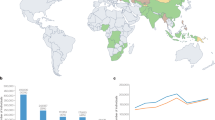
Worldwide, TB and HIV dominate the world’s biggest health threats. Around 9.6 million (6 million new cases were reported to the WHO) people were diagnosed with TB in 2014, of which 12% were in HIV positive patients. The death toll from TB in 2014 was 1.5 million people including 140,000 children, of whom 55,000 were coinfected with HIV. With a concerted global effort, TB mortality and prevalence has fallen by an estimated 47 and 42%, respectively, lower than in 1990; with the greatest improvement observed starting in year 2000. Demographics remain unchanged with the majority of cases in South-East Asia and the Western Pacific regions (58%). A large number of cases come from the African region (28%), India (23%), Indonesia (10%), and China (10%). These countries also hold the highest record for MDR-TB.
Among these 9.6 million reported cases, 5.4 million are men, 3.2 million are women and 1million are children. TB rates in US-born children are higher if one parent is foreign-born compared to if both parents are US-born (9). The WHO notes that estimating TB incidence among children poses a challenge due to rare bacteriological confirmation, under-reporting by pediatricians, lower likelihood of diagnosis in children when compared to adults cases in high-burden countries, and differing estimation methodologies (10).
Latent Tuberculosis Infection (LTBI) in Children and Adolescents
It is estimated that 1/3 of the world’s population has LTBI but true incidence is limited since it is not required to be reported (6). Children represent a vulnerable group to TB and an important goal for the WHO in their 2015 END TB strategy is to identify children at risk for TB infection, test them for infection, and provide effective treatment for any with latent infection in order to prevent progression to disease (11). In particular, children under the age of 5 y are at increased risk of progression to disease shortly after infection occurs and are at risk for the most serious manifestations of TB disease such as meningitis, which still carries a high mortality even in developed countries (7). Therefore any child in close contact with a contagious source case of TB should undergo testing for evidence of infection. In countries that are upper middle-income to high-income and have a low TB incidence (<100 cases per 100,000 population), the WHO now recommends expanded testing. Targeted groups should include children immigrating from any country with a high burden of TB, or if the child has disease that may alter the immunity against TB, such as a transplant recipient, a requirement for hemodialysis or the need for anti-tumor necrosis factor therapy (12).
Diagnosis of TB Infection in Children
The tuberculin skin test (TST) continues to be the mainstay in detecting tuberculosis infection in children, especially in those under age 5 (10,12). In use among children for the past 10 y, IGRAs are another diagnostic tool that can be used in certain clinical settings to improve specificity, such as in children who are BCG-immunized. These assays can also be used along with the TST to increase sensitivity in detecting infection in children who may be at higher risk for progression to disease and warrant treatment. A positive result can also be supportive evidence for TB disease in a child who has another symptom that may suggest the disease is present (13,14). The WHO has recommended the use of either TST or IGRA for screening at-risk children who reside in countries with a low burden of disease where there are ample resources for performing both tests (12). Other immunologic assays, such as interferon-inducible protein 10 (IP-10), continue to be explored for use in detecting TB infection in children. A recent prospective study investigated the correlation between the IP-10 levels in children who were household contacts to infectious TB cases with their later TST and (QuantiFERON) QFT results and identified value in its use for diagnosing TB infection. It maintains the limitation which TST and IGRAs possess but IP-10 levels cannot distinguish between LTBI and TB disease (6,15).
Once infection is established, the clinician must identify the status of the infection, specifically if it is latent or if there is disease. This evaluation requires three core components: patient history, physical exam, and radiography (10,12). Symptoms of TB disease can be nonspecific in children. Young children with TB disease have a lower bacterial load compared to adults which usually result in a different clinical presentation. Physical exam may also be normal in children with disease; so, radiography is necessary, which may show typical patterns associated with TB. Additionally, cultures in children can be difficult to obtain (hard to induce sputum and uncomfortable to intubate nasogastric tube for gastric aspirate) and may often be negative (paucibacillary disease). Sputum may be collected for acid-fast bacilli (AFB) smears but this is limited by the children who cannot produce sputum. At least 103 AFB per milliliter of sputum are needed in order to be detected on the smear. Recently, the use of Xpert MTB/RIF has now been endorsed by the WHO for use in detection of TB disease in children due to its improved sensitivity (20.6%, 95% CI: 13.7; 27.5) over the AFB smear method (9.2%, 95% CI: 4.2; 14.1) as well as offering the ability to identify Rifampin resistance simultaneously (3,16). The lower sensitivities can be explained by the fact young children with TB disease have a lower bacterial load compared to adults which usually results in a different clinical presentation. Hence, a negative test for TB does not rule out disease.
Biomarker research in children are promising but limited by sample size; which includes urine lipoarabinomannan with poor sensitivity (48.3%) and specificity (60.8%) (17), C-reactive protein (18), T-cell activation marker-tuberculosis assay (TAM-TB) with 83.3% sensitivity and 96.8% specificity (19), RNA expression signatures (51-transcript signature) with 82.9% sensitivity and 83.6% specificity, Gene expression signatures (LTBI—sensitivity and specificity 86%) (20).
Treatment of LTBI in Children and Adolescents
A prospective study looked at children who were contacts to infectious household source cases and used symptoms, TST and CXR and followed for 1 y. Children with LTBI who were <5 y old were placed on Isoniazid (INH) while those >5 y old were not (in accordance with global guidelines). Among children who went on to develop disease, it was noted that they were all in the >5 y old group and therefore had not received INH (21). Treatment of LTBI in pediatrics has expanded from a single regimen to now include three options: Isoniazid, Rifampin, or Isoniazid combined with Rifapentine. Treatment duration depends on the selected agent: 6–9 mo for Isoniazid, 4 mo for Rifampin and 3 mo for Isoniazid combined with Rifapentine (22). If the child is intolerant of one agent or has a suspected mono-resistant strain, then an alternate antibiotic should be chosen for therapy. If the child could be infected with a multidrug-resistant strain, close clinical monitoring is needed but there is no consensus on the best treatment regimen. Two studies involving pediatric contacts to a source case with MDR-disease are ongoing. Simplified regimens and more pediatric-friendly formulations are also needed in order to promote adherence and completion of therapy (10,12).
Multidrug-Resistant TB (MDR TB) and Extensively Drug-Resistant TB (XDR TB)
MDR TB is resistant to at least Isoniazid and Rifampicin. XDR TB is defined as MDR with additional resistance to any fluoroquinolones and any of the three second-line injectable agents-kanamycin, amikacin, or capreomycin. XDR TB has been reported in 105 countries (10,23,24,25). Globally, an estimated 3.3% (95% CI: 2.2–4.4%) of new cases and 20% (95% CI: 14–27%) of previously treated cases have MDR-TB; similarly children with MDR-TB was estimated around 3% (26,27). On average, an estimated 9.7% (95% CI: 7.4–12%) of people with MDR-TB have XDR-TB; it is estimated that 0.15% of children are with XDR-TB (27). Globally, only 50% of patients on MDR-TB treatment were successfully treated, largely due to high rates of mortality and loss to follow-up (10).
Mechanism of Intrinsic Drug Resistance of M. Tuberculosis
The bacterium has unusual structure of mycolic acid-containing cell wall which confers a low permeability and limits drug uptake for many antibiotics and chemotherapeutic agents (23,28). The other known mechanisms for drug resistance are active efflux systems that extrudes the drug molecules that enter the cell (also responsible for resistance to other antimicrobials) (29), physiologic adaptations that occurs within the host (23,30), asymmetric growth and division which result in growth phase-dependent antibiotic survival (27), and intrinsic resistance which favors in a high level of drug resistance (23).
Mechanism of Acquired Drug Resistance of M. Tuberculosis
Spontaneous mutations in chromosomal genes are mainly responsible for acquired drug resistance, producing the selection of resistant strains during suboptimal drug therapy (23,31). The most commonly used drugs; Isoniazid (KatG/mabA-inhA), Rifampicin (rpoB), Pyrazinamide (pncA), and Streptomycin (rpsL/rrs) develop resistance by mutation in gene and more mutations vary by geographic locations (23,32,33,34,35).
Advances in the Diagnosis of Drug-Resistant (DR) TB and New Drugs
The diagnosis of drug-resistant TB has been dependent on phenotypic, culture based methods for decades with a disadvantage of diagnostic delay. The lack of available globally-approved diagnostic tests capable of rapidly determining MDR and XDR TB remains a serious problem.
Xpert MTB/RIF assay (Cepheid, Sunnyvale, CA) was launched in 2004 and in 2010 WHO recommended its use. This assay rapidly (2 h) identifies MTB and resistance to rifampicin (36,37). WHO recommends Xpert MTB/RIF as a primary diagnostic test for adults with suspected DR-TB, children and adults with HIV with suspected TB in areas with high HIV prevalence, and detecting extra-pulmonary TB (10,36). It can detect smear negative TB in HIV-infected individuals (1). In children, where induced sputum or gastric aspirate is a challenge, this assay can diagnose TB from nasopharyngeal aspirate. This assay compared to culture in pediatric pulmonary TB showed that the pooled sensitivities and specificities of detection as 62% (95% CI: 51–73) and 98% (95% CI: 97–99), respectively. Similarly, sensitivity and specificity to detect rifampicin resistance was 86% (95% CI: 53–98) and 98% (95% CI: 94–100), respectively (38). This test may be used along with but does not replace conventional microscopy and culture diagnosis in children as Xpert MTB/RIF is not studied in outpatient settings or with different clinical or severity of TB disease. Since limited data, it is not recommended to test on urine, blood, or stool.
Line Probe Assays detecting INH and Rifampicin resistance (39), direct drug susceptibility (40), pyrosequencing (41), and microscopic observation drug susceptibility (41) are studied sparsely in children.
New Drugs
Bedaquiline kills both dormant and actively multiplying mycobacteria by inhibiting mycobacterial ATP synthase, thus interfering with energy production and disrupting intracellular metabolism ( Table 1 ). It is active against both drug-susceptible and DR-TB. Adding it to WHO recommended MDR-TB regimen reduced the time of sputum culture conversion in pulmonary MDR-TB (42). However, it is not recommended in children, not even for compassionate use (43).
Delamanid kills MTB by inhibition of mycolic acid biosynthesis. Two phase II trials are underway for pediatric treatment of MDR TB (clinicaltrials.gov; NCT01859923 and NCT01856634).
Sutezolid acts by binding to 23sRNA, blocking translation and thereby protein synthesis (5). It is not approved for children.
Fluoroquinolones are the key components of current MDR-TB treatment regimens. They accumulate in macrophages and granulocytes with intracellular drug concentration exceeding extracellular concentration by at least four- to fivefold. Several studies have shown their efficacy where first line drugs could not be used. Levofloxacin and Moxifloxacin have been shown to be superior to Ofloxacin (24).
Conclusion
Childhood TB accounts for 6–10% of all TB cases worldwide, resulting in significant morbidity and mortality (44). Children with TB can present with symptoms of common childhood illnesses, and not with typical cough, fever, weight loss as seen in adults. Up to 50% of children may be asymptomatic in the early stages of the disease (44). Once they are infected, they progress more quickly than adults to active disease, disseminated TB, and death, if untreated. Due to paucibacillary nature of the disease in children, culture may be negative in children, even though they are infected. In many countries, one of the reasons for inadequate access to diagnosis and treatment of drug-resistant TB is that the management of drug-resistant TB (PMDT) is too centralized. Hospital-based models of care, which are still dominant in many countries, are a barrier to the expansion of PMDT because they depend on hospitals or referral centers. Greater use of ambulatory care is necessary to expand access.
Highly sensitive and more specific tests for the diagnosis of latent TB infection have been developed, both of the interferon- release assays showed high diagnostic value in bacteriologically confirmed childhood TB (45). Recent advances in diagnosis with Xpert MTB/RIF with a rapid turnaround time, with high positivity rates than smear microscopy, is important for early detection particularly in smear negative cases (44). It should be offered upfront in TB endemic areas, where rapid screening is of utmost importance. Advances in treatment include 4 mo of Rifampicin alone or 2 mo of Rifampicin and Pyrazinamide for latent TB (44). Efforts are under way to develop vaccines to control disease in latent TB patients (45). More than 10 vaccine candidates have entered clinical trials in the last few years (45,46). Future research should aim to find a noninvasive point of care TB test, new, shorter, safer regimen consisting of only oral medicines that are well tolerated in children, and those should be accessible to families living in poverty (47). MDR-TB in children will mainly be from transmission from an adult, so history of contact with MDR-TB case is very crucial, in order to achieve the goal of end TB strategy which aims to reduce TB deaths by 90% between 2015 and 2035.
References
Heemskerk D, Caws M, Marais B, Farrar J. Tuberculosis in adults and children. Vol. 2. London: Springer 2015:1–66.
Lawn SD, Zumla AI. Tuberculosis. Lancet 2011;378:57–72.
Wlodarska M, Johnston JC, Gardy JL, Tang P. A microbiological revolution meets an ancient disease: improving the management of tuberculosis with genomics. Clin Microbiol Rev 2015;28:523–39.
Salgame P, Geadas C, Collins L, Jones-López E, Ellner JJ. Latent tuberculosis infection–Revisiting and revising concepts. Tuberculosis (Edinb) 2015;95:373–84.
Murray JF. A century of tuberculosis. Am J Respir Crit Care Med 2004;169:1181–6.
Daniel TM. The history of tuberculosis. Respir Med 2006;100:1862–70.
Chiang SS, Swanson DS, Starke JR. New Diagnostics for Childhood Tuberculosis. Infect Dis Clin North Am 2015;29:477–502.
Sterling TR, Villarino ME, Borisov AS, et al.; TB Trials Consortium PREVENT TB Study Team. Three months of rifapentine and isoniazid for latent tuberculosis infection. N Engl J Med 2011;365:2155–66.
Pang J, Teeter LD, Katz DJ, et al.; Tuberculosis Epidemiologic Studies Consortium. Epidemiology of tuberculosis in young children in the United States. Pediatrics 2014;133:e494–504.
World Health Organiszation. Global tuberculosis report 2015. Geneva: WHO (http://www.who.int/tb/publications/global_report/en/).
Güneş A, Uluca Ü, Aktar F, et al. Clinical, radiological and laboratory findings in 185 children with tuberculous meningitis at a single centre and relationship with the stage of the disease. Ital J Pediatr 2015;41:75.
World Health Organization. Guidelines on the management of latent Tuberculosis infection. Geneva: WHO (http://www.who.int/tb/publications/latent-tuberculosis-infection/en/) 2015.
Laurenti P, Raponi M, de Waure C, Marino M, Ricciardi W, Damiani G. Performance of interferon-γ release assays in the diagnosis of confirmed active tuberculosis in immunocompetent children: a new systematic review and meta-analysis. BMC Infect Dis 2016;16:131.
Starke JR ; Committee On Infectious Diseases. Interferon-γ release assays for diagnosis of tuberculosis infection and disease in children. Pediatrics 2014;134:e1763–73.
Biraro IA, Kimuda S, Egesa M, et al. The use of interferon gamma inducible protein 10 as a potential biomarker in the diagnosis of latent tuberculosis infection in Uganda. PLoS One 2016;11:e0146098.
Giang do C, Duong TN, Ha DT, et al. Prospective evaluation of GeneXpert for the diagnosis of HIV- negative pediatric TB cases. BMC Infect Dis 2015;15:70.
Nicol MP, Allen V, Workman L, et al. Urine lipoarabinomannan testing for diagnosis of pulmonary tuberculosis in children: a prospective study. Lancet Glob Health 2014;2:e278–84.
Pavan Kumar N, Anuradha R, Andrade BB, et al. Circulating biomarkers of pulmonary and extrapulmonary tuberculosis in children. Clin Vaccine Immunol 2013;20:704–11.
Portevin D, Moukambi F, Clowes P, et al. Assessment of the novel T-cell activation marker-tuberculosis assay for diagnosis of active tuberculosis in children: a prospective proof-of-concept study. Lancet Infect Dis 2014;14:931–8.
Sweeney TE, Braviak L, Tato CM, Khatri P. Genome-wide expression for diagnosis of pulmonary tuberculosis: a multicohort analysis. Lancet Respir Med 2016;4:213–24.
Triasih R, Robertson CF, Duke T, Graham SM. A prospective evaluation of the symptom-based screening approach to the management of children who are contacts of tuberculosis cases. Clin Infect Dis 2015;60:12–8.
Villarino ME, Scott NA, Weis SE, et al.; International Maternal Pediatric and Adolescents AIDS Clinical Trials Group; Tuberculosis Trials Consortium. Treatment for preventing tuberculosis in children and adolescents: a randomized clinical trial of a 3-month, 12-dose regimen of a combination of rifapentine and isoniazid. JAMA Pediatr 2015;169:247–55.
Almeida Da Silva PE, Palomino JC. Molecular basis and mechanisms of drug resistance in Mycobacterium tuberculosis: classical and new drugs. J Antimicrob Chemother 2011;66:1417–30.
Wallis RS, Maeurer M, Mwaba P, et al. Tuberculosis–advances in development of new drugs, treatment regimens, host-directed therapies, and biomarkers. Lancet Infect Dis 2016;16:e34–46.
Jarlier V, Nikaido H. Mycobacterial cell wall: structure and role in natural resistance to antibiotics. FEMS Microbiol Lett 1994;123:11–8.
Jenkins HE, Tolman AW, Yuen CM, et al. Incidence of multidrug-resistant tuberculosis disease in children: systematic review and global estimates. Lancet 2014;383:1572–9.
Dodd PJ, Sismanidis C, Seddon JA. Global burden of drug-resistant tuberculosis in children: a mathematical modelling study. Lancet Infect Dis 2016;16:1193–201.
De Rossi E, Aínsa JA, Riccardi G. Role of mycobacterial efflux transporters in drug resistance: an unresolved question. FEMS Microbiol Rev 2006;30:36–52.
Flores AR, Parsons LM, Pavelka MS Jr . Genetic analysis of the beta-lactamases of Mycobacterium tuberculosis and Mycobacterium smegmatis and susceptibility to beta-lactam antibiotics. Microbiology 2005;151(Pt 2):521–32.
Kochi A, Vareldzis B, Styblo K. Multidrug-resistant tuberculosis and its control. Res Microbiol 1993;144:104–10.
Zhang Y, Heym B, Allen B, Young D, Cole S. The catalase-peroxidase gene and isoniazid resistance of Mycobacterium tuberculosis. Nature 1992;358:591–3.
Banerjee A, Dubnau E, Quemard A, et al. inhA, a gene encoding a target for isoniazid and ethionamide in Mycobacterium tuberculosis. Science 1994;263:227–30.
Blanchard JS. Molecular mechanisms of drug resistance in Mycobacterium tuberculosis. Annu Rev Biochem 1996;65:215–39.
Hazbón MH, Brimacombe M, Bobadilla del Valle M, et al. Population genetics study of isoniazid resistance mutations and evolution of multidrug-resistant Mycobacterium tuberculosis. Antimicrob Agents Chemother 2006;50:2640–9.
Spies FS, da Silva PE, Ribeiro MO, Rossetti ML, Zaha A. Identification of mutations related to streptomycin resistance in clinical isolates of Mycobacterium tuberculosis and possible involvement of efflux mechanism. Antimicrob Agents Chemother 2008;52:2947–9.
Umubyeyi AN, Bonsu F, Chimzizi R, et al. The role of technical assistance in expanding access to Xpert(®) MTB/RIF: experience in sub-Saharan Africa. Public Health Action 2016;6:32–4.
WHO. Automated real-time nucleic acid amplification technology for rapid and simultaneous detection of tuberculosis and rifampicin: Xpert MTB/RIF system. Geneva, Switzerland: WHO. 2011.
Detjen AK, DiNardo AR, Leyden J, et al. Xpert MTB/RIF assay for the diagnosis of pulmonary tuberculosis in children: a systematic review and meta-analysis. Lancet Respir Med 2015;3:451–61.
Eliseev P, Balantcev G, Nikishova E, et al. The impact of a line probe assay based diagnostic algorithm on time to treatment initiation and treatment outcomes for multidrug resistant TB patients in Arkhangelsk region, Russia. PLoS One 2016;11:e0152761.
Zhang T, Lv CF, Wang J, et al. Direct tuberculosis drug susceptibility testing: time-saving and cost-effective in detecting MDR-TB. Int J Tuberc Lung Dis 2016;20:323–8.
Catanzaro A, Rodwell TC, Catanzaro DG, et al. Performance comparison of three rapid tests for the diagnosis of drug-resistant tuberculosis. PLoS One 2015;10:e0136861.
Field SK. Bedaquiline for the treatment of multidrug-resistant tuberculosis: great promise or disappointment? Ther Adv Chronic Dis 2015;6:170–84.
Tadolini M, Garcia-Prats AJ, D’Ambrosio L, et al. Compassionate use of new drugs in children and adolescents with multidrug-resistant and extensively drug-resistant tuberculosis: early experiences and challenges. Eur Respir J 2016;48:938–43.
Raizada N, Sachdeva KS, Nair SA, et al. Enhancing TB case detection: experience in offering upfront Xpert MTB/RIF testing to pediatric presumptive TB and DR TB cases for early rapid diagnosis of drug sensitive and drug resistant TB. PLoS One 2014;9:e105346.
Kumar MK, Kumar P, Singh A. Recent advances in the diagnosis and treatment of childhood tuberculosis. J Nat Sci Biol Med 2015;6:314–20.
Kaufmann SH. Future vaccination strategies against tuberculosis: thinking outside the box. Immunity 2010;33:567–77.
MDR-TB in Children: A Q&A with Partners In Health’s Dr. Mercedes Becerra. (http://www.pih.org/blog/mdr-tb-in-children-a-qa-with-pihs-dr.-mercedes-becerra). 2014.
Acknowledgements
Disclosures: Above authors have no financial support for this manuscript preparation and declare no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
PowerPoint slides
Rights and permissions
About this article

Cite this article
Khatua, S., Geltemeyer, A. & Gourishankar, A. Tuberculosis: Is the landscape changing?. Pediatr Res 81, 265–270 (2017). https://doi.org/10.1038/pr.2016.205
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/pr.2016.205
This article is cited by
-
Identification of volatile compounds from bacteria by spectrometric methods in medicine diagnostic and other areas: current state and perspectives
Applied Microbiology and Biotechnology (2021)
