
Abstract
Although various effective treatments for hypertension are available, novel therapies to reduce elevated blood pressure, improve blood-pressure control, treat resistant hypertension, and reduce the associated cardiovascular risk factors are still required. A novel angiotensin-receptor blocker (ARB) was approved in 2011, and additional compounds are in development or being tested in clinical trials. Several of these agents have innovative mechanisms of action (an aldosterone synthase inhibitor, a natriuretic peptide agonist, a soluble epoxide hydrolase inhibitor, and an angiotensin II type 2 receptor agonist) or dual activity (a combined ARB and neutral endopeptidase inhibitor, an ARB and endothelin receptor A blocker, and an endothelin-converting enzyme and neutral endopeptidase inhibitor). In addition, several novel fixed-dose combinations of existing antihypertensive agents were approved in 2010–2011, including aliskiren double and triple combinations, and an olmesartan triple combination. Upcoming fixed-dose combinations are expected to introduce calcium-channel blockers other than amlodipine and diuretics other than hydrochlorothiazide. Finally, device-based approaches to the treatment of resistant hypertension, such as renal denervation and baroreceptor activation therapy, have shown promising results in clinical trials. However, technical improvements in the implantation procedure and devices used for baroreceptor activation therapy are required to address procedural safety concerns.
Key Points
-
In 2010–2011, one novel antihypertensive—azilsartan—as well as several novel fixed-dose combinations of existing antihypertensive agents, including aliskiren double and triple combinations and an olmesartan triple combination were approved
-
Novel antihypertensive compounds in clinical development include an aldosterone synthase inhibitor, a natriuretic peptide agonist, and a soluble epoxide hydrolase inhibitor
-
An angiotensin II type 2 receptor agonist—compound 21—is in preclinical development
-
Novel antihypertensives with dual activity, including an angiotensin-receptor blocker and neutral endopeptidase inhibitor, an angiotensin-receptor blocker and endothelin receptor A blocker, and an endothelin-converting enzyme and neutral endopeptidase inhibitor, are in clinical development
-
Upcoming fixed-dose combinations of antihypertensives are expected to include calcium-channel blockers other than amlodipine, and diuretics other than hydrochlorothiazide (which are included in the current combinations)
-
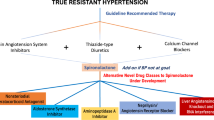
Nonpharmacological approaches for the treatment of resistant hypertension—renal denervation and baroreceptor activation—have shown promising results in clinical trials
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$209.00 per year
only $17.42 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout


Similar content being viewed by others

References
Redwood, H. Hypertension, society, and public policy. Eur. Heart. J. Suppl. 9 (Suppl. B), B13–B18 (2007).
Paulis, L. & Unger, T. Novel therapeutic targets for hypertension. Nat. Rev. Cardiol. 7, 431–441 (2010).
Drugs@FDA: FDA Approved Drug Products. FDA US Food and Drug Administration [online], (2011).
FDA Approved Drugs for Cardiology/Vascular Diseases. Center Watch [online], (2011).
New Medicines Database. PhRMA [online], (2011).
Unger, T., Paulis, L. & Sica, D. A. Therapeutic perspectives in hypertension: novel means for renin-angiotensin-aldosterone system modulation and emerging device-based approaches. Eur. Heart. J. 32, 2739–2747 (2011).
Dahlöf, B. et al. Cardiovascular morbidity and mortality in the Losartan Intervention for Endpoint Reduction in Hypertension study (LIFE): a randomised trial against atenolol. Lancet 359, 995–1003 (2000).
Julius, S. et al. Outcomes in hypertensive patients at high cardiovascular risk treated with regimens based on valsartan or amlodipine: the VALUE randomised trial. Lancet 363, 2022–2031 (2004).
ONTARGET Investigators. et al. Telmisartan, ramipril, or both in patients at high risk for vascular events. N. Engl. J. Med. 358, 1547–1559 (2008).
White, W. B. et al. Effects of the angiotensin receptor blocker azilsartan medoxomil versus olmesartan and valsartan on ambulatory and clinic blood pressure in patients with stages 1 and 2 hypertension. Hypertension 57, 413–420 (2011).
Bakris, G. L. et al. The comparative effects of azilsartan medoxomil and olmesartan on ambulatory and clinic blood pressure. J. Clin. Hypertens. (Greenwich) 13, 81–88 (2011).
Kurtz, T. W. & Klein, U. Next generation multifunctional angiotensin receptor blockers. Hypertens. Res. 32, 826–834 (2009).
Lane, D. A., Shah, S. & Beevers, D. G. Low-dose spironolactone in the management of resistant hypertension: a surveillance study. J. Hypertens. 25, 891–894 (2007).
Chapman, N. et al. Effect of spironolactone on blood pressure in patients with resistant hypertension. Hypertension 49, 839–845 (2007).
Nishizaka, M. K., Zaman, M. A. & Calhoun, D. A. Efficacy of low-dose spironolactone in subjects with resistant hypertension. Am. J. Hypertens. 16, 925–930 (2003).
Weinberger, M. H., Roniker, B., Krause. S. L. & Weiss, R. J. Eplerenone, a selective aldosterone blocker, in mild-to-moderate hypertension. Am. J. Hypertens. 15, 709–716 (2002).
Weinberger, M. H. et al. Effects of eplerenone versus losartan in patients with low-renin hypertension. Am. Heart J. 150, 426–433 (2005).
Karagiannis, A. et al. Spironolactone versus eplerenone for the treatment of idiopathic hyperaldosteronism. Expert Opin. Pharmacother. 9, 509–515 (2008).
Pitt, B. et al. The effect of spironolactone on morbidity and mortality in patients with severe heart failure. Randomized Aldactone Evaluation Study Investigators. N. Engl. J. Med. 341, 709–717 (1999).
Pitt, B. et al. Effects of eplerenone, enalapril, and eplerenone/enalapril in patients with essential hypertension and left ventricular hypertrophy: the 4E-left ventricular hypertrophy study. Circulation 108, 1831–1838 (2003).
Pitt, B. et al. Eplerenone, a selective aldosterone blocker, in patients with left ventricular dysfunction after myocardial infarction. N. Engl. J. Med. 348, 1309–1321 (2003).
Pitt, B. et al. Eplerenone reduces mortality 30 days after randomization following acute myocardial infarction in patients with left ventricular systolic dysfunction and heart failure. J. Am. Coll. Cardiol. 46, 425–431 (2005).
Sica, D. A. & Flack, J. M. Treatment considerations with aldosterone receptor antagonists. J. Clin. Hypertens. (Greenwich) 13, 65–69 (2011).
Amar, L. et al. Aldosterone synthase inhibition with LCI699: a proof-of-concept study in patients with primary aldosteronism. Hypertension 56, 831–838 (2010).
Calhoun, D. A. et al. Effects of a novel aldosterone synthase inhibitor for treatment of primary hypertension: results of a randomized, double-blind, placebo- and active-controlled phase 2 trial. Circulation 124, 1945–1955 (2011).
Osterberg, L. & Blaschke, T. Adherence to medication. N. Engl. J. Med. 353, 487–497 (2005).
Funder, J. W. Mineralocorticoid receptors: distribution and activation. Heart Fail. Rev. 10, 15–22 (2005).
Dietz, J. D. et al. A number of marketed dihydropyridine calcium channel blockers have mineralocorticoid receptor antagonist activity. Hypertension 51, 742–748 (2008).
Arhancet, G. B. et al. Stereochemical requirements for the mineralocorticoid receptor antagonist activity of dihydropyridines. J. Med. Chem. 53, 4300–4304 (2010).
Fagart, J. et al. A new mode of mineralocorticoid receptor antagonism by a potent and selective nonsteroidal molecule. J. Biol. Chem. 285, 29932–29940 (2010).
Akizuki, O. et al. Blockade of T-type voltage-dependent Ca2+ channels by benidipine, a dihydropyridine calcium channel blocker, inhibits aldosterone production in human adrenocortical cell line NCI-H295R. Eur. J. Pharmacol. 584, 424–434 (2008).
Isaka, T. et al. Azelnidipine inhibits aldosterone synthesis and secretion in human adrenocortical cell line NCI-H295R. Eur. J. Pharmacol. 605, 49–52 (2009).
Imagawa, K. et al. Inhibitory effect of efonidipine on aldosterone synthesis and secretion in human adrenocarcinoma (H295R) cells. J. Cardiovasc. Pharmacol. 47, 133–138 (2006).
Pandey, K. N. Guanylyl cyclase / atrial natriuretic peptide receptor-A: role in the pathophysiology of cardiovascular regulation. Can. J. Physiol. Pharmacol. 89, 557–573 (2011).
Li, Y., Madiraju, P. & Anand-Srivastava, M. B. Knockdown of natriuretic peptide receptor-A enhances receptor C expression and signalling in vascular smooth muscle cells. Cardiovasc. Res. 93, 350–359 (2012).
Sabrane, K., Kruse, M. N., Gazinski, A. & Kuhn, M. Chronic endothelium-dependent regulation of arterial blood pressure by atrial natriuretic peptide: role of nitric oxide and endothelin-1. Endocrinology 150, 2382–2387 (2009).
Jordan, R. et al. Phase 1 study of the novel A-type natriuretic receptor agonist, PL-3994, in healthy volunteers. Presented at the 12th scientific meeting of the Heart Failure Society of America.
Sica, D., Jordan, R. & Fischkoff, S. A. Phase IIa study of the NPR-agonist, PL-3994, in healthy adult volunteers with controlled hypertension. Presented at the 13th scientific meeting of the Heart Failure Society of America.
Imig, J. D., Zhao, X., Capdevila, J. H., Morisseau, C. & Hammock, B. D. Soluble epoxide hydrolase inhibition lowers arterial blood pressure in angiotensin II hypertension. Hypertension 39, 690–694 (2007).
Yu, Z. et al. Soluble epoxide hydrolase regulates hydrolysis of vasoactive epoxyeicosatrienoic acids. Circ. Res. 87, 992–998 (2000).
Davis, B. B. et al. Inhibitors of soluble epoxide hydrolase attenuate vascular smooth muscle cell proliferation. Proc. Natl Acad. Sci. USA 99, 2222–2227 (2002).
Anandan, S. K. et al. 1-(1-acetyl-piperidin-4-yl)-3-adamantan-1-yl-urea (AR9281) as a potent, selective, and orally available soluble epoxide hydrolase inhibitor with efficacy in rodent models of hypertension and dysglycemia. Bioorg. Med. Chem. Lett. 21, 983–988 (2010).
Imig, J. D., Carpenter, M. A. & Shaw, S. The soluble epoxide hydrolase inhibitor AR9281 decreases blood pressure, ameliorates renal injury and improves vascular function in hypertension. Pharmaceuticals 2, 217–227 (2009).
Chen, D. et al. Pharmacokinetics and pharmacodynamics of AR9281, an inhibitor of soluble epoxide hydrolase, in single- and multiple-dose studies in healthy human subjects. J. Clin. Pharmacol. http://dx.doi.org/10.1177/0091270010397049.
Steckelings, U. M., Kaschina, E. & Unger, T. The AT2 receptor—a matter of love and hate. Peptides 26, 1401–1409 (2005).
Wan, Y. et al. Design, synthesis, and biological evaluation of the first selective nonpeptide AT2 receptor agonist. J. Med. Chem. 47, 5995–6008 (2004).
Kaschina, E. et al. Angiotensin II type 2 receptor stimulation: a novel option of therapeutic interference with the renin–angiotensin system in myocardial infarction? Circulation 118, 2523–2532 (2008).
Rompe, F. et al. Direct angiotensin II type 2 receptor stimulation acts anti-inflammatory through epoxyeicosatrienoic acid and inhibition of nuclear factor κB. Hypertension 55, 924–931 (2010).
Rehman, A. et al. Angiotensin type 2 receptor agonist compound 21 reduces vascular injury and myocardial fibrosis in stroke-prone spontaneously hypertensive rats. Hypertension 59, 291–299 (2012).
Paulis, L. et al. Direct angiotensin II type 2 receptor stimulation in Nω-nitro-L-arginine-methyl ester-induced hypertension: the effect on pulse wave velocity and aortic remodeling. Hypertension 59, 485–492 (2012).
Campbell, D. J. Vasopeptidase inhibition: a double-edged sword? Hypertension 41, 383–389 (2003).
Tabrizchi, R. Omapatrilat. Bristol-Myers Squibb. Curr. Opin. Investig. Drugs 2, 1414–1422 (2001).
Packer, M. et al. Comparison of omapatrilat and enalapril in patients with chronic heart failure: the Omapatrilat Versus Enalapril Randomized Trial of Utility in Reducing Events (OVERTURE). Circulation 106, 920–926 (2002).
Ruilope, L. M., Dukat, A., Böhm, M., Lacourcière, Y., Gong, J. & Lefkowitz, M. P. Blood-pressure reduction with LCZ696, a novel dual-acting inhibitor of the angiotensin II receptor and neprilysin: a randomised, double-blind, placebo-controlled, active comparator study. Lancet. 375, 1255–1266 (2010).
Kirkby, N. S., Hadoke, P. W. F., Bagnall, A. J. & Webb, D. J. The endothelin system as a therapeutic target in cardiovascular disease: great expectations or bleak house? Br. J. Pharmacol. 153, 1105–1119 (2008).
Dhaun, N., Pollock, D. M., Goddard, J. & Webb, D. J. Selective and mixed endothelin receptor antagonism in cardiovascular disease. Trends Pharmacol. Sci. 28, 573–579 (2007).
Feldstein, C. & Romero, C. Role of endothelins in hypertension. Am. J. Therapeutics 14, 147–153 (2007).
Weber, M. A. et al. A selective endothelin-receptor antagonist to reduce blood pressure in patients with treatment-resistant hypertension: a randomised, double blind, placebo-controlled trial. Lancet 374, 1423–1431 (2009).
Bakris, G. L. et al. Divergent results using clinic and ambulatory blood pressures: report of a darusentan-resistant hypertension trial. Hypertension 56, 824–830 (2010).
Sica, D. A. Endothelin receptor antagonism: what does the future hold? Hypertension 52, 460–461 (2008).
Webb, D. J. DORADO: Opportunity postponed: lessons from studies of endothelin receptor antagonists in treatment-resistant hypertension. Hypertension 56, 806–807 (2010).
New Medical Therapies: Hypertension (High blood pressure) CenterWatch [online] (2011).
PS433540 (DARA compounds). EvaluatePharma® [online], (2010).
Thöne-Reinke, C. et al. Inhibition of both neutral endopeptidase and endothelin-converting enzyme by SLV306 reduces proteinuria and urinary albumin excretion in diabetic rats. J. Cardiovasc. Pharmacol. 44 (Suppl. 2), 76–79 (2004).
Müller, D. N. et al. Endothelin-converting enzyme inhibition ameliorates angiotensin II-induced cardiac damage. Hypertension 40, 840–846 (2002).
Dickstein, K. et al. Effect of single doses of SLV306, an inhibitor of both neutral endopeptidase and endothelin-converting enzyme, on pulmonary pressures in congestive heart failure. Am. J. Cardiol. 94, 237–239 (2004).
Wengenmayer, C. et al. Novel therapy approach in primary stroke prevention: simultaneous inhibition of endothelin converting enzyme and neutral endopeptidase in spontaneously hypertensive, stroke-prone rats improves survival. Neurol. Res. 33, 201–207 (2011).
Düsing, R. Optimizing blood pressure control through the use of fixed combinations. Vasc. Health Risk Manag. 6, 321–325 (2010).
Mancia, G. et al. 2007 Guidelines for the management of arterial hypertension: the task force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J. Hypertens. 25, 1105–1187 (2007).
Kappert, K., Kusserow, H. & Unger, T. The pharmacological rationale behind polypharmacy in heart failure. Heart Fail. Monit. 6, 20–27 (2008).
Sica, D. A. Rationale for fixed-dose combinations in the treatment of hypertension: the cycle repeats. Drugs 62, 443–462 (2002).
Philipp, T. et al. Two multicenter, 8-week, randomized, double-blind, placebo-controlled, parallel-group studies evaluating the efficacy and tolerability of amlodipine and valsartan in combination and as monotherapy in adult patients with mild to moderate essential hypertension. Clin. Ther. 29, 563–580 (2007).
Conlin, P. R. et al. Angiotensin II antagonists for hypertension: are there differences in efficacy? Am. J. Hypertens. 13, 418–426 (2000).
Pool, J. L. et al. Comparison of valsartan/hydrochlorothiazide combination therapy at doses up to 320/25 mg versus monotherapy: a double-blind, placebo-controlled study followed by long-term combination therapy in hypertensive adults. Clin. Ther. 29, 61–73 (2007).
Zeng, F., Patel, B. V., Andrews, L., Frech-Tamas, F. & Rudolph, A. E. Adherence and persistence of single-pill ARB/CCB combination therapy compared to multiple-pill ARB/CCB regimens. Curr. Med. Res. Opin. 26, 2877–2887 (2010).
Littlejohn, T. W. 3rd, Trenkwalder, P., Hollanders, G., Zhao, Y. & Liao, W. Long-term safety, tolerability and efficacy of combination therapy with aliskiren and amlodipine in patients with hypertension. Curr. Med. Res. Opin. 25, 951–959, 2009.
Chrysant, S. G. Single-pill triple-combination therapy: an alternative to multiple-drug treatment of hypertension. Postgrad. Med. 123, 21–31 (2011).
Parving, H. H. et al. Aliskiren trial in type 2 diabetes using cardio-renal endpoints (ALTITUDE): rationale and study design. Nephrol. Dial. Transplant. 24, 1663–1671 (2009).
Novartis. Novartis announces termination of ALTITUDE study with Rasilez®/Tekturna® in high-risk patients with diabetes and renal impairment. Novartis Global [online], (2011).
Calhoun, D. A., Lacourcière, Y., Chiang, Y. T. & Glazer, R. D. Triple antihypertensive therapy with amlodipine, valsartan, and hydrochlorothiazide: a randomized clinical trial. Hypertension 54, 32–39 (2009).
Jamerson, K. et al. Benazepril plus amlodipine or hydrochlorothiazide for hypertension in high-risk patients. N. Engl. J. Med. 359, 2417–2428 (2009).
US National Library of Medicine. Clinical trials.gov [online], (2012).
US National Library of Medicine. Clinical trials.gov [online], (2012).
Krum, H. et al. Catheter-based renal sympathetic denervation for resistant hypertension: a multicentre safety and proof-of-principle cohort study. Lancet 373, 1275–1281 (2009).
Krum, H. et al. Novel procedure- and device-based strategies in the management of systemic hypertension. Eur. Heart J. http://dx.doi.org/10.1093/eurheartj/ehq457.
Krum, H. et al. Device-based antihypertensive therapy: therapeutic modulation of the autonomic nervous system. Circulation 123, 209–215 (2011).
Symplicity HTN-2 Investigators. et al. Renal sympathetic denervation in patients with treatment-resistant hypertension (The Symplicity HTN-2 Trial): a randomised controlled trial. Lancet 376, 1903–1909 (2010).
Symplicity HTN-1 Investigators. Catheter-based renal sympathetic denervation for resistant hypertension: durability of blood pressure reduction out to 24 months. Hypertension 57, 911–917 (2011).
Kline, R. L. & Mercer, P. F. Functional reinnervation and development of supersensitivity to NE after renal denervation in rats. Am. J. Physiol. 238, R353–R358 (1980).
Nomura, G., Kurosaki, M., Takabatake, T., Kibe, Y. & Takeuchi, J. Reinnervation and renin release after unilateral renal denervation in the dog. J. Appl. Physiol. 33, 649–655 (1972).
DiBona, G. F. Renal innervation and denervation: lessons from renal transplantation reconsidered. Artif. Organs 11, 457–462 (1987).
Hansen, J. M. et al. The transplanted human kidney does not achieve functional reinnervation. Clin. Sci. (Lond). 87, 13–20 (1994).
Stefanadis, C. Renal denervation in resistant hypertension: radiofrequency ablation and chemical denervation. Hellenic J. Cardiol. 52, 481–482 (2011).
Ng, M. M., Sica, D. A. & Frishman, W. H. Rheos: an implantable carotid sinus stimulation device for the nonpharmacologic treatment of resistant hypertension. Cardiol. Rev. 19, 52–57 (2011).
Scheffers, I. J. et al. Novel baroreflex activation therapy in resistant hypertension: results of a European multi-center feasibility study. J. Am. Coll. Cardiol. 56, 1254–1258 (2010).
Schmidli, J. 4-year results of the Rheos® trial for control of intractable hypertension by carotid sinus baroreceptor stimulation. Presented at the 38th Annual Vascular and Endovascular Issues, Techniques and Horizons Symposium.
Bisognano, J. D. et al. Baroreflex activation therapy lowers blood pressure in patients with resistant hypertension: results from the double-blind, randomized, placebo-controlled Rheos pivotal trial. J. Am. Coll. Cardiol. 58, 765–773 (2011).
Hasenfuss, G. 2nd generation baroreflex activation therapy and ongoing clinical trials. Presented at the European Society for Cardiology Congress.
Acknowledgements
This work was supported by the EUREKA's Eurostars program of the EU and by the grant VEGA 1/0831/09 from the Scientific and Grant Agency of the Slovak Republic.
Author information
Authors and Affiliations
Contributions
L. Paulis and T. Unger researched the data for the article, provided a substantial contribution to discussions of the content, wrote the article and reviewed and/or edited the manuscript before submission. U. M. Steckelings provided a substantial contribution to discussions of the content, and reviewed and/or edited the manuscript before submission.
Corresponding author
Ethics declarations
Competing interests
T. Unger declares that he has acted as a consultant or speaker and has a modest financial interest in Vicore Pharma. M. U. Steckelings declares that she has acted as a consultant and has received research supplies from Vicore Pharma. L. Paulis declares no competing interests.
Rights and permissions
About this article
Cite this article
Paulis, L., Steckelings, U. & Unger, T. Key advances in antihypertensive treatment. Nat Rev Cardiol 9, 276–285 (2012). https://doi.org/10.1038/nrcardio.2012.33
Published:
Issue Date:
DOI: https://doi.org/10.1038/nrcardio.2012.33
This article is cited by
-
Synthesis and evaluation of new sartan derivatives
Medicinal Chemistry Research (2022)
-
Replacement of Amlodipine and Lercanidipine by Barnidipine: Tolerability and Effectiveness in a Real-Life Study
High Blood Pressure & Cardiovascular Prevention (2017)
-
Systolic hypertension: an increasing clinical challenge in Asia
Hypertension Research (2015)
-
New Developments in the Pharmacological Treatment of Hypertension: Dead-End or a Glimmer at the Horizon?
Current Hypertension Reports (2015)
-
Drug Therapy of Apparent Treatment-Resistant Hypertension: Focus on Mineralocorticoid Receptor Antagonists
Drugs (2015)
