
Abstract
Background:
We investigated the feasibility of dose-dense neoadjuvant chemotherapy (NACT) with paclitaxel and carboplatin before radical chemoradiation (CRT) and assessed the response rate to such a regimen.
Methods:
CxII is a single-arm phase II trial of 46 patients, with locally advanced cervical cancer (stage Ib2-IVa). Patients received dose-dense carboplatin (AUC2) and paclitaxel (80 mg m−2) weekly for six cycles followed by CRT (40 mg m−2 of weekly cisplatin, 50.4 Gy, 28 fractions plus brachytherapy). The primary end point was response rate 12 weeks post-CRT.
Results:
Baseline characteristics were: median age at diagnosis 43 years; 72% squamous, 22% adenocarcinoma and 7% adenosquamous histologies; FIGO stage IB2 (11%), II (50%), III (33%), IV (7%). Complete or partial response rate was 70% (95% CI: 54–82) post-NACT and 85% (95% CI: 71–94) post-CRT. The median follow-up was 39.1 months. Overall and progression-free survivals at 3 years were 67% (95% CI: 51–79) and 68% (95% CI: 51–79), respectively. Grade 3/4 toxicities were 20% during NACT (11% haematological, 9% non-haematological) and 52% during CRT (haematological: 41%, non-haematological: 22%).
Conclusion:
A good response rate is achieved by dose-dense weekly NACT with carboplatin and paclitaxel followed by radical CRT. This treatment regimen is feasible as evidenced by the acceptable toxicity of NACT and by the high compliance to radiotherapy (98%).
Similar content being viewed by others

Main
Despite the fall in incidence of cervical cancer in countries with a screening programme, a large proportion of those diagnosed with invasive cancer have locally advanced disease at presentation. An audit by the Royal College of Radiologists in 2001–2002, of UK patients with cervical cancer treated non-surgically with curative intent, found a 5-year survival rate of 56% (Vale et al, 2010). Chemoradiation (CRT) has been the standard of care since 1999 (Keys et al, 1999; Morris et al, 1999; Whitney et al, 1999), and was widely adopted in the UK (McCormack et al, 2001). An individual patient data meta-analysis based on 18 trials from 11 countries confirmed the benefit of CRT. However, the estimated improvement in a 5-year overall survival (OS) was only 6% (i.e., from 60 to 66%, HR: 0.81), with a disease-free survival rate of 58% (CCCMAC - Chemoradiotherapy for Cervical Cancer Meta-analysis Collaboration, 2008). The benefit of adding chemotherapy to radiotherapy was seen regardless of age, histology and grade, but appeared to be lower in patients with more advanced tumours. In the decade since the introduction of CRT, there have been no further advances in the management of locally advanced cervical cancer. A single trial has reported a survival advantage with accent on n and a from the addition of adjuvant chemotherapy after CRT (Dueñas-González et al, 2011), but further randomised trials are required.
The role of neoadjuvant chemotherapy (NACT) has been examined in a number of trials. Although a meta-analysis of 21 randomised trials showed no improvement in OS with NACT, there was an association between outcome and short cycle length, or platinum with a dose intensity of more than 25 mg m−2 per week (NCLACCM - Neoadjuvant Chemotherapy for Locally Advanced Cervical Cancer Meta-analysis Collaboration, 2003). Trials with a cycle length of ⩽14 days were associated with an improvement in OS of approximately 7% at 5 years, whereas longer cycle lengths had a detrimental effect on outcome.
The combination of taxane and platinum is known to be active in advanced and recurrent cervical cancer with response rates of 40–50% (Papadimitriou et al, 1999; Rose et al, 1999). This combination is also active in the neoadjuvant accent on n and a setting with reported response rates of up to 90–95% (Dueñas-González et al, 2003; Park et al, 2004). Cisplatin and paclitaxel requires a longer infusion compared with carboplatin/paclitaxel combination, which is demonstrated to have acceptable toxicity and promising activity (Tinker et al, 2005; Moore et al, 2007; Mabuchi et al, 2010). We therefore postulated that a short course of weekly dose-dense paclitaxel and carboplatin chemotherapy before CRT might downstage local disease, lengthen the exposure to systemic treatment and improve outcome. This trial (called CXII) investigated the feasibility of NACT and assessed the overall response rate after the doublet chemotherapy and at 12 weeks after the completion of CRT.
Materials and methods
We conducted a single-arm phase II trial in women with locally advanced cervical cancer treated with neoadjuvant weekly paclitaxel and carboplatin chemotherapy followed immediately by concomitant CRT.
Study population and eligibility criteria
Patients, 18 years or older, with histological confirmation of squamous, adeno- or adenosquamous carcinoma of the cervix, FIGO stage Ib2-IVa who were suitable for radical CRT were eligible to participate. This included patients with histologically positive para-aortic lymph nodes (PALN). All patients had a biopsy, examination under anaesthetic (EUA) and imaging to complete the staging as detailed below. Patients were required to have an ECOG performance status 0–1; adequate renal function (glomerular filtration rate ⩾60 ml min−1 measured isotopically or by creatinine clearance); adequate liver function (ALT or AST <2.5 ULN, and bilirubin <1.25 ULN); adequate bone marrow function (WCC >3.0 × 109 per l, neutrophils >1.5 × 109 per l and platelets >100 × 109 per l); and a normal ECG. Patients with a hydronephrosis had a ureteric stent inserted regardless of renal function. Patients were excluded if they were pregnant or breast feeding, had a previous diagnosis of cancer except basal cell carcinoma, or had active cardiac disease. Ethics and regulatory approvals were obtained, and all patients gave written informed consent. Cervical tumour tissue samples were collected for future translational studies.
Treatment schedule
Neoadjuvant chemotherapy was given weekly for 6 weeks (on days 1, 8, 15, 22, 29 and 36) as follows: paclitaxel (80 mg m−2) over 1 h, followed by carboplatin (AUC 2- dose calculated by Calvert formula) over 30 min. Dose modifications were allowed for haematological toxicity. Both drugs were omitted on any week if neutrophils were <1.0 × 109 per l or platelets <75 × 109 per l on the day of treatment. In all subsequent cycles, paclitaxel was then given at 85% of full dose and carboplatin at AUC 1.6. In the event of further haematological toxicity NACT was discontinued. Patients with a significant hypersensitivity reaction to paclitaxel were withdrawn from the study, whereas those with a reaction to carboplatin were allowed to continue on paclitaxel alone. The glomerular filtration rate was repeated and carboplatin dose recalculated if there was a 10% rise in serum creatinine on up to two consecutive tests or if the serum creatinine became abnormal for the first time. Paclitaxel was stopped if patients experienced ⩾grade 2 peripheral neuropathy. If NACT was discontinued early, patients proceeded to radiation and cisplatin was commenced when blood counts had recovered.
Radiation, following NACT, began on week 7 with concomitant cisplatin (CRT) commencing as soon as haematological recovery permitted. Cisplatin (40 mg m−2, maximum 70 mg) was given with hydration over 1 h (before radiation), weekly for a minimum of four cycles and maximum of six cycles. Radiotherapy to the whole pelvis was given to a total dose of 50.4 Gy in 28 fractions over 5.5 weeks using 8–15 mV photons. Intracavitary brachytherapy was given towards the end of or following completion of external beam radiation. Patients received a total dose of 15 Gy in two fractions to point A HDR or an equivalent dose using LDR (25 Gy to point A).
The external beam radiation to the pelvis was delivered using a four-field (AP/PA and two lateral fields) arrangement. The conventional pelvic field extended from the top of L5 to the bottom of the obturator foramen or 2 cm below the lowest level of disease and laterally 1.5 cm beyond the bony pelvis. The lateral fields extended from the anterior border of the symphysis pubis to the S2/3 interspace posteriorly. However, fields were modified to take account of available information from pre-treatment MRI scans and EUA to ensure adequate tumour coverage. Shielding of the corners of AP/PA field was permitted. Where extended fields were used to treat PALN the superior field border was at T12/L1 and the inferior border at L4/5. This PALN strip was treated using an AP/PA field to a dose of 45 Gy in 25 fractions over 5 weeks. In patients with parametrial involvement or pelvic sidewall extension, a boost was permitted to a dose of 5.4 Gy in three fractions over 3 days using AP/PA fields. Every effort was made to ensure that the entire course of radiotherapy was completed within 50 days, and that the haemoglobin level was maintained at ⩾12.5 g dl−1 throughout the CRT.
Assessments
At baseline, all patients had an X-ray or CT of the chest and CT or MRI scan of the abdomen (within the previous 6 weeks), and an MRI of the pelvis. Full blood counts were performed weekly during NACT and twice weekly during CRT. Biochemistry and toxicity assessments were carried out weekly during treatment, then 4 weeks post-CRT and 3-monthly for 2 years. Severity of adverse events was categorised using NCI CTCAE version 3.0. Specific radiotherapy toxicities were classified according to RTOG criteria (Cox et al, 1995).
A pelvic MRI was performed at the end of the sixth week of NACT to assess response using RECIST criteria (Therasse et al, 2000). Overall response was determined using pelvic MRI 12 weeks after the completion of CRT. MRI scans were reviewed centrally at UCL Hospitals. Further radiological assessments were conducted as clinically indicated.
Statistical considerations
The primary end point was the response rate 12 weeks after completing all treatment. The target response rate was ⩾85% and no lower than 70% (which could be achieved with current practice). This required approximately 50 patients, with 80% power and a 5% one-sided test of statistical significance. The response rate to NACT was also assessed. Overall and progression-free survivals (PFSs) were measured from the date of study registration until progression, death from any cause or the date last seen alive. Adverse events were based on the maximum toxicity grade for each type of event. All analyses were intention-to-treat.
Results
Patient demographics
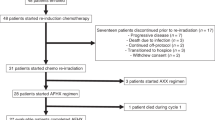
A total of 46 patients were recruited from three centres in London, Leicester and Birmingham between June 2005 and October 2008, with median follow-up of 39.1 months. Baseline characteristics are shown in Table 1. The median age was 43 years and 72% had squamous cell cancers. The majority of the cases were either FIGO stage IIb (50%) or IIIb (28%). In all, 11% (5/46) had positive PALN, 3 in FIGO IIb group and 2 in FIGO IIIb group.
Treatment compliance
Eighty percent of patients (37/46) completed all six cycles of NACT, 13% had a dose delay and 9% a dose reduction (Table 2). Forty-two patients (91%) had full doses of drugs for at least four cycles. Of the nine patients who did not complete six cycles (Supplementary Table 1), five had five cycles of chemotherapy, one had disease progression after four cycles, one stopped after three cycles due to chest infection and two stopped after one cycle (one due to dehydration/anaemia and the other anaphylaxis to paclitaxel).
Seventy eight percent (36/46) completed four to six cycles of cisplatin therapy during CRT (Supplementary Table 2). Five patients had three cycles and one patient had one cycle. The six patients who stopped cisplatin before cycle 4, did so because of toxicity (n=3) and unspecified reason (n=3). The toxicities were: haematological and abdominal pain/nausea/vomiting (n=1) and tinnitus with or without palpitation (n=2). Three patients did not start cisplatin due to disease progression (n=1), dehydration and anaemia (n=1) and allergic reaction (n=1). Four patients had a cisplatin dose reduction, because of haematological toxicity (n=1) and clinical reasons (n=3: COPD exacerbation, low creatinine clearance and weight change). Twenty patients had a treatment delay during CRT, mainly due to toxicity (n=10), clinician/patient decision (n=3) or administrative/logistical/other reasons (n=9).
Ninety eight percent (45/46) of patients had radiotherapy (Supplementary Table 3); one patient had an adenosquamous tumour and the disease (local and PALN) progressed on NACT. Ninety six percent had brachytherapy and 67% had a boost to the pelvic sidewall. Four of the five patients with positive PALN received extended field radiation as per protocol (one patient progressed after four cycles of NACT and was not given any further treatment). Most patients who had brachytherapy, received a dose of 15 Gy in two fractions HDR (30/44), and 10 patients had ⩾21 Gy in one fraction LDR and one 27 Gy in MDR.
Efficacy
The proportion who had a complete/partial response was 70% (32/46; 95% CI: 54–82), at the end of NACT, and 85% (39/46; 95% CI: 71–94), 12 weeks after completing CRT (Table 3). A complete response was seen in two women after NACT and in 29 patients 12 weeks after finishing CRT. The proportion of patients with stable disease after NACT and CRT was 22% (10/46) and 4% (2/46), respectively. Two patients (4%) progressed after NACT, one of whom had no further treatment because of rapidly progressing disease. The other had stable disease in the primary tumour but developed new nodal disease and progressed further after CRT. One patient progressed after CRT.
Kaplan–Meier plots for PFS and OS are shown in Figure 1. There were 14 events for PFS (4 with disease progression and 10 deaths), and the rates at 6 months and 1 year were 89% (95% CI: 76–95) and 80% (95% CI: 66–89), and at both 3 and 5 years were 68% (95% CI: 51–79).

Kaplan–Meier plots for progression-free survival (PFS; upper) and overall survival (OS; lower) for the 46 patients in the study. The PFS and OS rates are the same for 3 and 5 years (68% and 67%) as there were no PFS or OS events between 3 and 5 years.
Of the five patients with positive PALN at diagnosis, four patients completed all six cycles of NACT and three to five cycles of cisplatin. Three out of these four patients were without any evidence of disease during follow-up. One patient progressed on completing four cycles of NACT and died shortly after.
In all, 14 patients had died at the time of analysis: cervical cancer (n=11), haemorrhage (n=2; 28 days and 7 months after finishing cisplatin) and cardiac arrest (n=1). The OS rates at 6 months and 1 year were 91% (95% CI: 78–97), 80% (95% CI: 66–89), and at both 3 and 5 years were 67% (95% CI: 51–79) with no deaths or progression between 3 and 5 years.
Adverse events
Adverse events according to NCI CTCAE v3.0 and RTOG criteria are summarised in Table 4 and Supplementary Table 4.
NACT
Relatively few patients experienced a grade 3 or 4 adverse event during NACT. In all, 20% (9/46) had any type of event, of which 11% (5/46) were haematological and 9% (4/46) were non-haematological (Table 4).
CRT
A total of 52% of patients had a grade 3 or 4 adverse event during CRT. Haematological toxicity accounted for 41% (19/46), whereas 22% (10/46) had a non-haematological event (Table 4).
Overall treatment and follow-up
In total, 63% (29/46) had grade 3/4 toxicity at any time during treatment (NACT/CRT) or follow-up. Most were haematological (48%), and the most common non-haematological events were diarrhoea (13%), vomiting (9%), nausea (7%) and infection (7%). There were two reported suspected unexpected serious adverse reactions, confusion and pulmonary embolism, both considered by the treating clinician to be possibly related to cisplatin and carboplatin. 35% (16/46) had at most a grade 2 adverse event at any time during treatment or follow-up (Supplementary Table 4), 28% (13/46) of which were haematological. Other events included constipation, nausea, and alopecia. 39% (18/46) had a grade 2 RTOG toxicity recorded during follow up (Supplementary Table 4).
Discussion
The CxII trial used a novel approach of administering weekly carboplatin and paclitaxel chemotherapy for six weeks followed immediately by standard CRT commencing in week seven. The results from this trial confirm that a short course of dose-dense weekly NACT with carboplatin and paclitaxel, followed by radical CRT, is feasible with acceptable toxicity. The response rate to this short course of chemotherapy, as assessed radiologically within days of completing the sixth week, was 70% with an 85% overall response rate after CRT, and an OS rate of 67% at 3 years. Three out of the 5 patients with positive PALN were alive with no evidence of disease at the time of analysis. This approach may have particular merits in this patient population.
Previous trials investigating the role of NACT in cervical cancer have used a variety of different drugs with different schedules and a gap of up to 28 days in some trials between the completion of chemotherapy and the start of definitive radiotherapy. Both the protracted schedules and the gap between completing chemotherapy and radiotherapy are likely to have contributed to tumour cell repopulation thereby limiting the effectiveness of the additional chemotherapy (Kim and Tannock, 2005). Therefore strategies to limit this process may lead to an improvement in outcome.
Dose dense NACT is a feasible approach as it did not compromise chemoradiotherapy with 98% of patients completing the radiation phase within 50 days and 78% receiving at least 4 cycles of concomitant cisplatin, whilst 50% (23/46) received at least 5 cycles of cisplatin. A retrospective analysis of GOG trials by Monk et al (2007) showed that up to 50% of patients failed to complete 6 cycles of cisplatin with no apparent difference in OS between those completing 5 or more cycles. In the current study 50% of patients completed 5 or more cycles, similar to that recorded in the study by Rose et al (1999). More recently the meta-analysis of 18 randomised trials of chemoradiotherapy found no evidence that the effect of CRT was influenced by cycle length or dose intensity of cisplatin used (CCCMAC-Chemoradiotherapy for Cervical Cancer Meta-analysis Collaboration, 2008). Trials using short cycle-chemotherapy appears to be associated with an improvement in survival compared with those using a more prolonged cycle interval (NCLACCM-Neoadjuvant Chemotherapy for Locally Advanced Cervical Cancer Meta-analysis Collaboration, 2003).
In general NACT was well tolerated with only 20% of patients experiencing any grade 3/4 event and no treatment-related deaths. The G3/4 neutropenia rate of 9% in the current study compares favourably with the 7% observed in the Mori et al (2008) but is lower than the 15% reported by Dueñas-Gonzãlez et al (2003). The corresponding G2 neutropenia rates were 13%, 16.7% and 16.2% in the current study, Mori et al (2008) and Dueñas-González et al (2003), respectively. The current study confirms the observation by Mori et al that most adverse events during NACT were G1/2 alopecia and gastrointestinal symptoms.
There were more adverse events during CRT with 41% of patients having any grade 3/4 haematological toxicity. The grade 3/4 leucopenia rate during CRT in our trial was 33% (data not shown) whilst the grade 3 neutropenia rate was 30% which is considerably higher than the 6% reported by Dueñas-González et al (2003) and Dueñas-Gonzalez et al (2011) but comparable to that recorded for cisplatin and radiation (23%) by Rose et al (1999). Thus the incorporation of additional chemotherapy into the standard treatment regimens is likely to result in increased toxicity. Ongoing phase III trials will provide valuable information on overall toxicity and efficacy in relation to the timing of additional chemotherapy. In the INTERLACE trial (ClinicalTrials.gov NCT01566240), the aim is to investigate whether dose dense weekly chemotherapy (paclitaxel/carboplatin) for 6 weeks before standard CRT (using cisplatin) improves OS compared with CRT alone. The OUTBACK trial (ClinicalTrials.gov NCT01414608) is examining the role of adjuvant chemotherapy (4 cycles of carboplatin and paclitaxel) after standard CRT (using cisplatin) against standard CRT alone.
The observed response rate after NACT (70%) in this study is lower than that reported in other studies of NACT but this may reflect differences in patient selection, timing and method of assessment and the number of patients who actually received the NACT. Park et al (2009) noted a response rate of 91% (assessed clinically and radiologically 10 days post treatment) in women with FIGO Ib2-IIb treated with 3 cycles of 10-day cisplatin and paclitaxel prior to surgery. Similarly, Mori et al (2008) reported a response rate of 87% in 30 patients (all of whom completed all 6 weeks of NACT, compared to 80% in our trial) with FIGO stage Ib2-IVa treated with 6 weeks of carboplatin and paclitaxel prior to surgery. Patients with stage III/IVa disease comprised 39% of those treated in CXII compared with 16% in the Mori et al (2008) study. Dueñas-González et al (2003) reported response rates of 95% in 43 patients with FIGO Ib2- IIIb disease treated with 3 cycles of 3-weekly carboplatin and paclitaxel chemotherapy prior to radical hysterectomy and CRT. However in that study, response was assessed clinically (we used MRI) and the planned dose of chemotherapy was higher.
In our trial 10 patients (22%) had stable disease at the end of NACT and 4 of these patients subsequently died from their disease. Stable disease post-NACT has also been identified by others as a poor prognostic sign (Park et al, 2009). The overall response rate to treatment in the present study (complete and partial response) was 85% at 12 weeks post-CRT, and the 3-year PFS and OS rates were 68 and 67% respectively. This is better than the 56% seen in historical controls (population based audit of outcome from 42 UK centres) in this patient population in the UK (Vale et al, 2010). The PFS rates in the current study were comparable to those reported for CRT alone by Dueñas-González et al (2011) study (68% vs 65%) but marginally lower than that reported for the arm with additional chemotherapy given both with and following radiation 68% vs 74%). These differences may be explained by differences in patient selection (CxII included patients with positive PA lymph nodes) and the lower radiation dose in the current study. The recently launched phase III trial (INTERLACE) has mandated a higher radiation dose in line with that used in the Duenaz- Gonzalez study.
In summary, this trial has demonstrated a good response rate to NCAT followed by CRT in women with locally advanced cervical cancer. These results have been used to design an international randomised multicentre phase III trial, INTERLACE to determine whether this treatment strategy leads to a significant improvement in survival compared to standard CRT.
References
CCCMAC - Chemoradiotherapy for Cervical Cancer Meta-analysis Collaboration (2008) Reducing uncertainties about the effects of chemoradiotherapy for cervical cancer: A systematic review and meta-analysis of individual patient data from 18 randomised trials. J Clin Oncol 26: 5802–5812
Cox JD, Stetz J, Pajak TF (1995) Toxicity criteria of the Radiation Therapy Oncology Group (RTOG) and the European Organization for Research and Treatment of Cancer (EORTC). Int J Radiat Oncol Biol Phys 31: 1341–1346
Dueñas-González A, López-Graniel C, González-Enciso A, Cetina L, Rivera L, Mariscal I, Montalvo G, Gómez E, de la Garza J, Chanona G, Mohar A (2003) A phase II study of multimodality treatment for locally advanced cervical cancer: neoadjuvant carboplatin and paclitaxel followed by radical hysterectomy and adjuvant cisplatin chemoradiation. Ann Oncol 14 (8): 1278–1284
Dueñas-González A, Zarbá JJ, Patel F, Alcedo JC, Beslija S, Casanova L, Pattaranutaporn P, Hameed S, Blair JM, Barraclough H, Orlando M (2011) Phase III, open-label, randomised study comparing concurrent gemcitabine plus cisplatin and radiation followed by adjuvant gemcitabine and cisplatin versus concurrent cisplatin and radiation in patients with stage IIIB to IVA carcinoma of the cervix. J Clin Oncol 29: 1678–1685
Keys HM, Bundy BN, Stehman FB, Muderspach LI, Chafe WE, Suggs CL 3rd, Walker JL, Gersell D (1999) Cisplatin, radiation, and adjuvant hysterectomy compared with radiation and adjuvant hysterectomy for bulky stage IB cervical carcinoma. N Engl J Med 340: 1154–1161
Kim JJ, Tannock IF (2005) Repopulation of cancer cells during therapy: an important cause of treatment failure. Nat Rev Cancer 5: 516–525
Mabuchi S, Morishige K, Enomoto T, Kimura T (2010) Carboplatin and paclitaxel as an initial treatment in patiens with stage IVb cervical cancer: a report of 7 cases and a review of the literature. J Gynecol Oncol 21: 93–96
McCormack M, Brown RSD, Birtle AJ (2001) A national audit of chemo-radiation practice for cervical carcinoma in the United Kingdom. Royal College of Radiologists Annual Scientific Meeting 2001. Clinical Oncol 13: 318–319
Monk BJ, Tian C, Rose PG, Lanciano R (2007) Which clinical/pathologic factors matter in the era of chemoradiation as treatment for locally advanced cervical carcinoma? Analysis of two Gynecol Oncol Group (GOG) trials. Gynecol Oncol 105: 427–433
Moore KN, Herzog TJ, Lewin S, Giuntoli RL, Armstrong DK, Rocconi RP, Spannuth WA, Gold MA (2007) A comparison of cisplati/paclitaxel and carboplatin/paclitaxel in stage IVB, recurrent or persistent cervical cancer. Gynecol Oncol 105: 299–303
Mori T, Hosokawa K, Kinoshita Y, Watanabe A, Honjo H (2008) Neoadjuvant chemotherapy with weekly carboplatin and paclitaxel for locally advanced cervical carcinoma. Int J Gynecol Cancer 18: 85–89
Morris M, Eifel PJ, Lu J, Grigsby PW, Levenback C, Stevens RE, Rotman M, Gershenson DM, Mutch DG (1999) Pelvic radiation with concurrent chemotherapy compared with pelvic and para-aortic radiation for high-risk cervical cancer. N Engl J Med 340: 1137–1143
NCLACCM - Neoadjuvant Chemotherapy for Locally Advanced Cervical Cancer Meta-analysis Collaboration (2003) Neoadjuvant chemotherapy for locally advanced cervical cancer: a systematic review and meta-analysis of individual patient data from 21 randomised trials. Eur J Cancer 17: 2470–2486
Papadimitriou CA, Sarris K, Moulopoulos LA, Fountzilas G, Anagnostopoulos A, Voulgaris Z, Gika D, Giannakoulis N, Diakomanolis E, Dimopoulos MA (1999) Phase II trial of paclitaxel and cisplatin in metastatic and recurrent carcinoma of the uterine cervix. J Clin Oncol 17: 761–766
Park DC, Kim JH, Lew YO, Kim DH, Namkoong SE (2004) Phase II trial of neoadjuvant paclitaxel and cisplatin in uterine cervical cancer. Gynecol Oncol 92: 59–63
Park DC, Suh MJ, Yeo SG (2009) Neoadjuvant paclitaxel and cisplatin in uterine cervical cancer: long-term results. Int J Gynecol Cancer 9: 943–947
Rose PG, Blessing JA, Gershenson DM, McGehee R (1999) Paclitaxel and cisplatin as first-line therapy in recurrent or advanced squamous cell carcinoma of the cervix Gynecologic Oncology Group study. J Clin Oncol 17: 2676–2680
Therasse P, Arbuck SG, Eisenhauer EA, Wanders J, Kaplan RS, Rubinstein L, Verweij J, Van Glabbeke M, van Oosterom AT, Christian MC, Gwyther SG (2000) New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J Natl Cancer Inst 92: 205–214
Tinker AV, Bhagat K, Swenerton KD, Hoskins PJ (2005) Carboplatin and paclitaxel for advanced and recurrent cervical carcinoma: The British Columbia Cancer Agency experience. Gynecol Oncol 98: 54–58
Vale CL, Tierney JF, Davidson SE, Drinkwater KJ, Symonds P (2010) Substantial Improvement in UK Cervical Cancer Survival with Chemoradiotherapy: Results of a Royal College of Radiologists’ Audit. Clin Oncol 22: 590–601
Whitney CW, Sause W, Bundy BN, Malfetano JH, Hannigan EV, Fowler WC Jr, Clarke-Pearson DL, Liao SY (1999) Randomized comparison of fluorouracil plus cisplatin versus hydroxyurea as an adjunct to radiation therapy in stage IIB-IVA carcinoma of the cervix with negative para-aortic lymph nodes: a Gynecologic Oncology Group and Southwest Oncology Group study. J Clin Oncol 17: 1339–1348
Acknowledgements
We are grateful to all the patients who agreed to participate in this study. We thank all participating sites and site staff; the Cancer Research UK and UCL Cancer Trials Centre for managing and co-ordinating the trial. We also thank Nicky Gower (UCL Cancer Trials Centre) for her help in setting up the trial and Egla Aitkens (Gynaecological Clinical Nurse Specialist at University College London Hospital, London) for her support throughout the trial. This trial was supported by an unconditional educational grant from Bristol Myers Squibb; by the Cancer Research UK and UCL Cancer Trials Centre; and the University College London and University College London Hospital Comprehensive Biomedical Research Centre.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Presented as an abstract at ASCO, Chicago, USA, May 2009. J Clin Oncol 27: 15s (no. 5586).
Supplementary Information accompanies this paper on British Journal of Cancer website
Supplementary information
Rights and permissions
This work is licensed under the Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article
Cite this article
McCormack, M., Kadalayil, L., Hackshaw, A. et al. A phase II study of weekly neoadjuvant chemotherapy followed by radical chemoradiation for locally advanced cervical cancer. Br J Cancer 108, 2464–2469 (2013). https://doi.org/10.1038/bjc.2013.230
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/bjc.2013.230
Keywords
This article is cited by
-
Efficacy of treatment patterns based on concurrent chemoradiotherapy in patients with stage IIB cervical squamous cell carcinoma
BMC Cancer (2024)
-
Neoadjuvant chemotherapy with weekly cisplatin and paclitaxel followed by chemoradiation for locally advanced cervical cancer
BMC Cancer (2023)
-
Locally advanced squamous cervical carcinoma (M0): management and emerging therapeutic options in the precision radiotherapy era
Japanese Journal of Radiology (2023)
-
Comparison of outcomes and side effects for neoadjuvant chemotherapy with weekly cisplatin and paclitaxel followed by chemoradiation vs. chemoradiation alone in stage IIB–IVA cervical cancer: study protocol for a randomized controlled trial
Trials (2022)
-
Dose-dense paclitaxel/carboplatin as neo-adjuvant chemotherapy followed by radical surgery in locally advanced cervical cancer: a prospective phase II study
Cancer Chemotherapy and Pharmacology (2019)
