
Key Points
-
Indicates the lack of a universal approach to the management of peri-implant diseases in both Australia and the UK.
-
While specialists reported seeing peri-implant pathology in no greater than 25% of their patients, they estimated the prevalence in the general population to be significantly higher.
-
Local antibiotics are more popular among UK specialists, with systemic antibiotics more frequently used in Australia.
Abstract
Background Pathology of the peri-implant tissues, namely peri-implant mucositis and peri-implantitis are conditions that are often encountered and can threaten the long term survival of the implants.
Aim This study aimed to compare the attitudes of registered specialists in periodontology in Australia and the UK towards aetiology, prevalence, diagnosis and management of mucositis and peri-implantitis.
Methods A validated questionnaire was used and the sample consisted of UK and Australian specialists.
Results There were differences in the demographics of specialists in the two countries, with the Australian specialists being significantly younger. Most specialists in both countries identified the prevalence of peri-implant pathology between 0-25%. Although there was agreement as to the role of plaque in the aetiopathogenesis of the diseases, UK specialists were more likely to include adverse loading and smoking as etiological factors. There were significant differences in the management of the disease between the groups, including the use of mouth rinses, local and systemic antibiotics. Australians were more likely to use systemic antibiotics than in the UK.
Conclusions The results suggested that differences in professional demographics, educational resources and market factors, and the absence of consensus treatment standards can significantly affect the treatment modalities patients finally receive.
Similar content being viewed by others

Introduction
Treatment with dental implants is considered today an effective and predictable option for replacement of missing teeth. As a result of more than three decades of research and development, dental implants are now available to an increasing proportion of the population, and cover a wide range of indications. Despite the increasingly successful outcomes, dental implant treatments often present complications, which pose significant challenges to the clinician.1 Pathology of the peri-implant tissues, namely peri-implant mucositis and peri-implantitis, are conditions that can threaten the long term survival of the implants.2
With mucositis and peri-implantitis being relatively new pathological entities, there is little scientific evidence to suggest a standard treatment modality at present. Although there have been several studies demonstrating clinical resolution using different treatment modalities, there is insufficient evidence to provide a 'gold standard' protocol.3 With an increase in the number of implants being placed and the fact that peri-implantitis prevalence increases with the number of years in function,4 one can expect that the management of peri-implant pathology will be one major challenge in the near future.
Peri-implant mucositis is a reversible inflammatory reaction causing redness and swelling localised to the soft tissue around implants.1 The European Consensus workshop suggests its incidence is around 80% in subjects with 50% of implant sites affected.1,2 Peri-implantitis is an inflammatory reaction that is associated with loss of the surrounding supporting bone of the functioning implant.1,2 Some studies place the prevalence in the range of 2-10%,5,6 however, the Consensus Report of the Sixth European Workshop suggests that it affects between 28% and 56% of implants placed.2 These estimations, however, are based on only two studies originating from patients in one country, while there are very few data available from other parts of the world.
Australia, like many other areas of the world, is undergoing a rapid growth in the market for implant dentistry7 The number of implants placed each year is rapidly increasing, even though implant dentistry is a fairly new treatment modality for a large proportion of the population. As a consequence, the available observation periods of functioning implants are shorter than those encountered in major European countries, thus the prevalence of peri-implantitis appears far lower than what appears in studies based on European populations.5 In contrast the UK is a more established market and the growth rate of dental implants is much slower than in Australia; however, there is a greater length of time for observation periods. With regards to peri-implantitis in particular, this might be an important factor, as the prevalence of pathology is shown to increase with the increase of time of the implant in function.4
The training of specialists within periodontology in Australia and the UK has followed a similar pathway of development and has the same major learning outcomes today. As it appears that the range of treatments for dental implants have some differing characteristics between the UK and Australia, one might expect this to result in differences in the current prevalence of peri-implant disease. Whether such differences are also reflected in the attitudes, perceptions and management strategies of practicing specialists, is open to investigation.
Aims
This study aimed to compare and contrast the attitudes of registered specialists in periodontology both in Australia and the UK towards prevalence, diagnosis and management of mucositis and peri-implantitis. The study aims were to:
-
Investigate the prevalence of peri-implant pathology in the UK and Australia, as perceived by the specialists in periodontology in the two countries
-
Investigate the relative management schemes used by specialists to treat peri-implant pathology
-
Compare the potential of treatment modalities between Australia and the UK, as perceived by the specialist practitioners
-
Investigate the concepts of aetiology and pathogenesis shared among UK and Australian specialists practitioners, as well as identify common and different perceptions with regards to the prevention and management of the disease itself, which may be helpful in the future teaching of the subject.
Material and methods
A questionnaire designed and previously validated in Australia (Griffith University) and Sweden (University of Malmo) was used to determine attitudes and management schemes of periodontologists towards peri-implantitis.8 The questionnaire was initially developed and validated in Sweden via a pilot with a group of periodontology specialists. A translation in English was undertaken by one of the investigators involved in the development of the Swedish version (NM) and validation of the English version through a focus group of six Australian specialists followed in May 2009. The questionnaire is available at http://www.mattheos.net/files/QuestPeriImpl.pdf.
UK sample
The questionnaire was mailed out to all the periodontology specialists listed on the General Dental Council website of the UK with a stamped addressed envelope included to allow the questionnaires to be returned. The questionnaire was posted on 1 May 2010 and responses were collected until 15 June 2010. The questionnaire section of demographics was slightly modified for suitability in the UK. Remaining sections were kept identical as with the one originally used in Australia and Sweden.
Australian sample
Data from Australian specialists were collected during the fourteenth scientific meeting of the Australian/New Zealand Academy of Periodontology (ANZAP), which took place in Adelaide, between 20-23 May 2009. Attendance was limited to ANZAP members who were either registered specialists of periodontology in an Australian state or New Zealand or postgraduate students in accredited periodontology programmes. The questionnaires were distributed at the beginning of a plenary session and a five minute introduction was given by one of the authors (NM) on the purpose and aims of the study. Filled questionnaires were collected at the end of the day in a special box at the exit of the theatre. Questionnaires from students or New Zealand specialists were excluded from the sample of the present study.
Two periodontology specialists were interviewed from Australia, and two from the UK to aid analysis of quantitative data. The interviews followed a semi-structured methodology where the specialists were invited through open questions to comment on the basic findings of the study on the basis of their experience. These interviews helped the authors to extrapolate from the results of the study and attempt to reach hypotheses based on practice realities in the two countries.
Data were analysed using the software Stats Direct to determine descriptive and frequency analysis for all fields. Differences between the two sample populations were tested for statistical significance with the Mann-Whitney U test. In the two cases of matched observations (the frequency of diagnosis of mucositis/peri-implantitis as opposed to perceived prevalence in general population), statistically significant differences were analysed with a Wilcoxon signed rank test. Fisher's exact test was used to examine the association between two variables measured at the nominal level. Cramer's V was used as a post test to determine strengths of association where statistical differences were discovered. Any statistically significant differences were discussed using additional information from interviews undertaken and comments made from specialists on receipt of questionnaires as an aid.
Results
Response rates
Of 303 questionnaires mailed out to the UK, 105 completed responses were returned. One participant felt that his permission had not been sought for analysis for the data therefore his input was excluded from the results in order to satisfy any objections. Four questionnaires were received outside of the specified return date and excluded from the analysis. Thus, the response rate was 33% in the UK.
Of a possible 110 eligible attendants in Australia, 70 completed questionnaires were included in the sample resulting in a 65% response rate. Questionnaires originating from postgraduate students and NZ based specialists were excluded from the present analysis.
Demographics
The Australian sample was composed of significantly younger specialists (median age = 35-44 years) than the UK sample (median age = 45-54 years), p = 0.038. Australian specialists reported significantly less years of professional practice, (p = 0.0004) with the median years of practice for Australians being between 6-10 and for UK specialists being more than 10 (Fig. 1).

Distribution of years in specialty practice of periodontology between the UK and Australia
The distribution of gender was similar, with male specialists amounting to 75.3% in Australia and 69.9% in the UK sample. Surgically placing implants did not have a gender perspective in Australian specialists, as the proportion of female dentists placing implants was similar to the proportion of males (AU: female 72%, male 75%). The same is not true, however, for the UK, as 75% of males were reported placing implants as opposed to 38% of females, which is a significant difference (p = 0.005).
The percentage of overseas trained specialists in the two countries was similar with 13.4% in AU and 17.2% in the UK. Half of all UK specialists in this sample were trained in the two centres the UCL Eastman and Kings College London, compared to a wider distribution between centres in Australia.
With regards to practice settings, the majority of specialists in both countries were active in private practice (AU 76%, UK 73.7%). The second largest affiliation in the UK was with a hospital (33% of specialists), while hospital affiliation existed for only 5% of Australian specialists. Both Australian (18%) and UK specialists (23%) reported university affiliation. In Australia 75% of specialists were involved purely in private practice compared to 42.71% in the UK.
Frequency of mucositis/peri-implantitis
The frequency of mucositis diagnosis was similar in both countries, with the great majority of specialists reporting it within 0-25% range of the implant patients seen (AU 78%, UK 82% of specialists). The agreement was even greater in the case of peri-implantitis, where 0-25% was the encountered prevalence for 96% of the Australians and 93% of the UK.
However, when the specialists were asked to estimate the frequency of peri-implantitis and mucositis in the general population, they considered the general prevalence to be higher. The difference between the prevalence specialists diagnose and what they project in the general population was significant for both samples; mucositis (AU p = 0.0001, UK p = 0.0001) and peri-implantitis (AU p = 0.05, UK p = 0.0001). This deviation was greater among UK specialists, who estimated less prevalence than their Australian colleagues. The most pronounced was the case of mucositis (mucositis experienced diagnosis median in UK is 0-25%, mucositis perceived prevalence in general population median is 26-50%) (Table 1).
Aetiology of mucositis/peri-implantitis
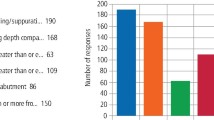
Bacterial plaque was the most popular aetiologic factor reported by 100% of the Australian and 98.8% of the UK specialists. However, there was a significant difference between countries with regards to smoking (p = 0.001) and adverse loading (p = 0.004). Forty-three percent of the Australian and 77% of UK specialists marked smoking as an aetiologic factor, while 15% and 36% respectively indicated adverse loading (Fig. 2).

Comparison of specialists opinions with regards to smoking and adverse loading as aetiological factors of peri-implantitis
Management schemes for mucositis/peri-implantitis
Oral hygiene/antimicrobial mouth rinses
Specialists from both countries considered oral hygiene instruction to be key in the management of the diseases. There was no significant difference (p = 0.07) with the use of an antimicrobial mouth rinse/gel for the treatment of mucositis, with 42.19% of Australian specialists reporting that they used it compared to UK 31.87%. There was, however, a significant difference when it comes to peri-implantitis, where 64.61% of Australian specialists reported using antimicrobial mouth rinses compared to 47.78% of UK specialists (p = 0.02).
Local antibiotics
There was a significant difference between the two countries on the view for applying local antibiotics. Australian specialists reported using local antibiotics as an adjunct less than the UK. In the treatment of mucositis, 67.21% of Australian specialists reported never using local antibiotics compared to 42.53% of their UK counterparts (p = 0.001). This was similarly reflected in treatment of peri-implantitis (AU 57.38% UK 20%, p = 0.001). The UK median value for local antibiotics use shows that they were sometimes being used, whereas in comparison, they were never used in Australia.
Systemic antibiotics
Both Australian and UK specialists reported a similar approach in the use of systemic antibiotics in the treatment of mucositis. In contrast, Australian specialists reported using systemic antibiotics more frequently in the treatment of peri-implantitis (p = 0.0002). Systemic antibiotics were always used by 37.31% of Australians yet only by 14.78% in the UK. 11.36% of UK specialists never use systemic antibiotics compared to 1.50% of AU specialists.
There was a significant difference with regards to the timing of use of systemic antibiotics in the treatment of peri-implantitis (p = 0.001) with Australian specialists appearing more likely to use postoperative antibiotics (frequency of always: AU 33.85%, UK 19.04%). Both countries maintain that the median use was often for pre-op antibiotics in peri-implantitis.
The place of practice appears significantly correlated with the frequency of use of antibiotics in Australia (p = 0.0002, Cramer's V: r = 0.400), with the specialists in private practice using antibiotics significantly more than their colleagues in hospital/university and public service clinics. This correlation was not found significant in the UK sample. However, because of the statistical analysis requirement for mutually exclusive groups in this part of the questionnaire, the sample size was greatly reduced and may have affected the results.
No correlation was found between age or years of experience and frequency of use of systemic antibiotics for both Australia and UK. Table 2 and Table 3 show the frequency of dosage of different types of antibiotics and their use within the two countries. Antibiotic regimes have been reported as they were seen in the questionnaire (original responses). It is apparent that the UK generally uses lower dosages than that of Australia, which is consistent with their lower frequency of use. There was also wider variety of use of antibiotics in Australia given that the sample size was smaller. The most common antibiotic used within both countries is amoxicillin + metronidazole (AU 56.25%, UK 68.85%) although the dosage varies significantly. The most common dosage in the UK was 250 mg amoxicillin + 200 mg metronidazole (36.65%) whereas in Australia the most common dosage was 500 mg amoxicillin + 400 mg metronidazole (22.91%). Only 9.83% of the British samples reported using this dosage.
Instrumentation
There was a significant difference between the choice of instrument between countries, p = 0.001. The Australians reported a preference for stainless steel instruments compared to the UK (AU 55.88%, UK 25.80%) who reported a preference for titanium (AU 25%, UK 46.24%) or plastic instruments (AU 39.70, UK 65.59%). However, they all seem to be in agreement with regards to the use of ultrasonic scalers (Fig. 3). Finally, success of treatment of peri-implantitis is given as median of moderately effective in both countries.

Specialists' opinions of instrument use
Maintenance
A visit every third month was the most popular choice among both samples as an appropriate maintenance recall after treatment of peri-implantitis. Specialists in each country reported six months as appropriate radiographic recall after treatment of peri-implantitis.
Discussion
Peri-implantitis is recognised as a condition that may lead to the loss of osseointegration and eventual failure of implants. While the general dentist will encounter such problems with increased frequency, referral to specialists will be inevitable in many cases. This study looked at the attitudes towards the aetiopathogenesis, as well as treatment regimes employed by periodontologists in both the UK and Australia. The results clearly indicate a wide diversity in treatment options but also certain differences in the attitudes towards aetiology and pathogenesis of peri-implant pathology. These findings have direct implications for the education process of specialists, as they point out areas where more research and evidence-based guidelines are needed if we are to secure the optimal standards of care. In particular, the use of antibiotics appears very diverse and based on empirical factors, rather than evidence. Certain differences exist in the professional demographics, but also the marketing of implant dentistry in these two countries may be reflected in these results.
There was a greater proportion of male to female specialists and this might be in accordance with other resources stating that the profession worldwide is generally more male dominated.9 However, the demographics of dentistry are changing in the Western world with greater female enrolment into dental schools,10 which will eventually lead to a balancing of the male:female ratio. It has been reported that women tend to work part time in general practice compared to their male counter parts, with males taking a more active role in continuing education.11 This may reflect the lower proportion of women specialists in both countries.
The UK specialists were older in years than their Australian counterparts with a greater number of years of experience. One would expect the median age to be similar given that population statistics show the average age of the two countries to be 37.4 years and 39.9 years respectively and the age demographic to be similar in proportion;12,13 however the results do not reflect this. The national periodontology specialty list was established in 1998 in the UK. Specialists in Australia have been registered with a state or territory board and as of July 1 2010 a national registration board has also been introduced. This may have some influence on the differences in years of experience owing to potential variation in criteria for specialty registration; however, this argument is open to speculation and requires additional research. What is noted is that 'oral surgery' was not recognised as a speciality in itself until July 2010 in Australia. Undertaking a specialist programme in periodontology in Australia was for some the only formal pathway towards development of specialist level dento-alveolar surgical skills, whereas in the UK this could be achieved through both the periodontology or oral surgery specialist lists. This would account for periodontology having been an attractive prospect for new graduates in Australia interested in surgical procedures.
What also must be considered in regards to experience is that to obtain specialty status in Australia, specific postgraduate qualifications are required.14,15 This is also required in the UK;16 however, previously dentists were able to gain speciality status with existing long standing speciality practice by the 'grandparenting' method in the UK, within the first two years of the specialty instigation. Periodontology became a specialty within dentistry in 1998, with people given two years to apply for specialty status by mediated entry. This is obviously no longer available, however, the results reflect that 13.8% of specialists achieved status by this method. This would allow for an older specialist population, although no formative additional qualification was obtained.
It was found that fewer women specialists in the UK are placing implants compared to their Australian counterparts. This may require further investigation to determine the background of this result. A larger proportion of Australian specialists work solely in private practice, which may influence treatment choices. It is an interesting finding that private practitioners tend to prescribe antibiotics for the treatment of peri-implantitis more frequently than their colleagues working in public healthcare settings. This difference has been also identified in previous research with Swedish specialists.8 In the present study, the difference was very significant in the Australian sample, but not in the UK. However, due to the type of the analysis, much of the sample with affiliations both in private and public practice had to be excluded, resulting in a much smaller sample in this field. This fact might have affected the results as the proportion of private practitioners with affiliation to public healthcare/hospitals is much higher in the UK sample.
The majority of the UK sample of specialists was trained by two centres – the UCL Eastman and Kings College London, compared to a broad range over the Australian centres. It is reasonable to expect a significant influence on the opinions and attitudes of specialists owing to the source of their training. This may reflect the fact that although plaque is seen to be an unquestionable aetiological factor by all specialists, there is some controversy as to the role of smoking and adverse loading. The controversy with regards to the role of smoking in peri-implantitis is probably carried on from similar discussions in the pathogenesis of periodontitis. Literature suggests that smokers have greater attachment loss, bone loss and increased level of pocketing.17 Some advocate that smoking is an aetiological factor in periodontal disease, affecting vasculature and causing immunological changes and ultimately increasing the risk of periodontal disease. compared to non-smokers independent of the level of oral hygiene.18,19 Others, however, believe that smoking is a modifying factor determining the severity of the disease and the healing response, and that it is only the bacteria in the plaque that is the aetiologic or true risk factor. It seems that the UK specialists are more in favour of smoking being an aetiological factor for peri-implantitis, whereas Australians are in favour of it being a modifying factor. Similarly, UK specialists are of the opinion that adverse loading is an aetiological factor.
Both Australia and the UK suggest a similar frequency of mucositis and peri-implantitis; however, they expect there to be a higher prevalence in the general population. This perhaps is influenced by the varying classifications for incidence of disease and a concern that true disease is under-reported due to lack of differentiation between health and disease. Also this might reflect a fear that effective maintenance schemes are not always utilised. True prevalence is difficult to determine and there is insufficient research in this area, which may account for the wide variation.
The results show no universal treatment approach and there is intra- and inter-variation. Both countries believe oral hygiene instruction to be key in the management of peri-implant pathology; however Australians believe antimicrobial mouth rinses to be a key adjunct. In addition, local antibiotics are rarely used in Australia compared to the UK. This might reflect differences not only in the education/attitudes of specialists, but also the effect of the pharmaceutical market in the two countries. Local antibiotics are not available in the Australian market, although there is no reason for this type of drug not to be licensed. Market trends and the choices made by the pharmaceutical industry might significantly influence treatment modalities, through the availability of drugs/substances. This could be another factor involved in the increased use of systemic antibiotics in Australia.
Both countries are consistent in the use of amoxicillin and metronidazole as their primary systemic antibiotic. However, the dominant prescription regime for Australia is amoxicillin 500 mg + metronidazole 400 mg, compared to the UK where half of that dose is advocated (amoxicillin 250 mg + metronidazole 200 mg). The UK results show increased consistency in the use of this dosage of antibiotic; however, in Australia the range is far wider. What is interesting to note for educational purposes is that the dosage depicted for treatment of peri-implantitis in the UK is the same as that used to treat aggressive periodontal disease. Bearing in mind the increasing prevalence of peri-implantitis and the consequences of systemic antibiotics, this appears to be an important area where we need to urgently develop a critical mass of evidence as to the role and optimal dosage of antibiotics in the treatment of peri-implantitis. Streamlining specialist education with evidence-based guidelines will ensure optimal patient care while preventing abuse of systemic antibiotics. Finally there is a noted difference in instrument choice between countries. The UK specialists prefer the use of plastic or titanium instruments whereas Australians would rather use stainless steel. Both countries have similar perceptions that success of treatment is only moderately effective. While ultrasonic instruments are used widely on the natural dentition, there is still an ongoing debate on their use on implant surfaces. Research has shown that there is damage and alteration of the titanium surface with both metal and plastic coated ultrasonic scalers.20
These results should be seen under the limitations of the study. The questionnaires have been previously validated and used, however, the response rate between the two countries is very different. This might be due to the difference in the collection of the sample. In Australia the sample was collected in person during one day, in a small size biannual specialist conference, which is attended by the great majority of specialists in the country. The study and its aims were previously introduced by one of the investigators (NM). This obviously allowed for a response rate in Australia which was unusually high for questionnaire surveys. Such a possibility did not exist, however, in the UK sample during the period of the study. The impersonal post-based sample collection resulted in a much lower response rate. Consequently, although the Australian sample size is adequately representative of Australian periodontology specialists, the danger exists that the UK sample might be somewhat 'skewed' due to the selection method. It is unclear if the method of posting questionnaires can bias towards specific characteristics of the specialists sampled, however, the results should be interpreted with caution, especially when the differences observed are marginal. In spite of this low return in the UK, this work does highlight variability in the approach of specialists to the treatment of peri-implantitis which in certain cases is extreme and unlikely to be affected by a bias in the sampling, such as in the use of antibiotics.
Conclusion
The data collected shows that there are some clear differences in both the opinions and attitudes of specialists, as well as their approaches to management of peri-implant pathology. This is not surprising, considering the fact that there is no strong consensus today worldwide with regards to the treatment of peri-implantitis. This study showed that the use and dosage of local and systemic antibiotics, the role of mouth rinses, smoking and adverse loading in the aetiology and pathogenesis of the disease and the selection of instruments are all areas of controversy that should be targeted by research aiming to develop evidence-based treatment guidelines as soon as possible. The scientific background of the two groups of specialists is very similar, as the training they have received is comparable. However, it appears that differences in professional demographics, educational resources and market factors, in the absence of consensus treatment standards can significantly affect the treatment modalities patients finally receive.
References
Zitzmann N U, Berglundh T . Definition and prevalence of peri-implant diseases. J Clin Periodontol 2008; 35: 286–291.
Lindhe J, Meyle J . Peri-implant diseases: Consensus Report of the Sixth European Workshop on Periodontology. J Clin Periodontol 2008; 35: 282–285.
Faggion C M Jr, Chambrone L, Gondim V, Schmitter M, Tu Y K . Comparison of the effects of treatment of peri-implant infection in animal and human studies: systematic review and meta-analysis. Clin Oral Implants Res 2010; 21: 137–147.
Roos-Jansåker A M. Long time follow up of implant therapy and treatment of Peri-implantitis. Swed Dent J Suppl 2007; (188): 7–66.
Nixon K C, Chen S T, Ivanovski S . A retrospective analysis of 1,000 consecutively placed implants in private practice. Aust Dent J 2009; 54: 123–129.
Karoussis I K, Salvi G E, Heitz-Mayfield L J, Brägger U, Hämmerle C H, Lang N P . Long-term implant prognosis in patients with and without a history of chronic periodontitis: a 10-year prospective cohort study of the ITI Dental Implant System. Clin Oral Implants Res 2003; 14: 329–339.
Kalorama Market Reports. Implant-based dental reconstruction: world dental implant and bone graft market. 3rd edition. 2009. Online article available at http://www.kaloramainformation.com/Implant-Based-Dental-2284095 (accessed December 2011).
Sköldenklint M, Dageborn J, Jansson H, Mattheos N . Treatment methods of peri Implant mucositis and peri Implantitis. A questionnaire survey to Sweden's periodontologists. Sweden: Centre for Oral Health Sciences, Malmo University; 2009; 8: 080. (SWE-English Abstract). Online article available on request at Malmo University Electronic Publishing (MUEP) at http://dspace.mah.se/.
Dolan T A, Lewis C E . Gender trends in the career patterns of recent dental graduates. J Dent Educ 1987; 51: 639–645.
Carlisle L D. The gender shift, the demographics of women in dentistry. What impact will it have? Online article available at http://www.spiritofcaring.com/public/488.cfm (accessed January 2011).
Matthews R W, Scully C . Working patterns of male and female dentists in the UK. Br Dent J 1994; 176: 463–466.
Australian Bureau of Statistics. Population by age and sex, Australian states and territories. June 2009; 3201.0. Online article available at http://www.abs.gov.au/AUSSTATS/abs@.nsf/DetailsPage/3201.0Jun%202009?OpenDocument (accessed February 2011).
Directgov UK. Government, citizens and rights. Key facts about the United Kingdom. Available online at http://www.direct.gov.uk/en/Governmentcitizensandrights/LivingintheUK/DG_10012517 (accessed January 2012).
Australian Dental Association Inc. Policy statement specialisation in dentistry. Online article available at http://www.ada.org.au/app_cmslib/media/lib/0703/m52282_v1_2.4specialisation.pdf (accessed January 2011).
Australian Government Medicare. For health professionals. Online articles available at http://www.medicareaustralia.gov.au/provider/index.jsp (accessed January 2011).
General Dental Council. Specialist lists. Online lists available at http://www.gdc-uk.org/Dentalprofessionals/Specialistlist/Pages/default.aspx (accessed January 2011).
Heitz-Mayfield L J. Peri-implant diseases: diagnosis and risk indicators. J Clin Periodontol 2008; 35: 292–304.
Bergstrom J. Tobacco smoking and chronic destructive periodontal disease. Odontology 2004; 92: 1–8.
Bergström J, Eliasson S, Dock J . A 10-year prospective study of tobacco smoking and periodontal health. J Periodontol 2000; 71: 1338–1347.
Mann M, Parmer D, Walmsley A D, Lea S C . Effect of plastic covered ultrasonic scalers on titanium implant surfaces. Clin Oral Implants Res 2011; doi: 10.1111/j1600-0501.2011.02186.x (epub ahead of print).
Acknowledgements
The authors would like to express their gratitude to Professor Iain Chapple, University of Birmingham, Professor Saso Ivanovski, Griffith University, and Dr Sven Bohnsted, Griffith University for their insight and input in the execution of this study.
Author information
Authors and Affiliations
Corresponding author
Additional information
Refereed paper
Rights and permissions
About this article
Cite this article
Mattheos, N., Collier, S. & Walmsley, A. Specialists' management decisions and attitudes towards mucositis and peri-implantitis. Br Dent J 212, E1 (2012). https://doi.org/10.1038/sj.bdj.2012.1
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.2012.1
This article is cited by
-
The referral pattern and treatment modality for peri-implant disease between periodontists and non-periodontist dentists
BMC Oral Health (2023)
-
Evaluation of implants in smoking and non-smoking patients with peri-implant disease risk analysis and esthetic scores: an observational study
BMC Oral Health (2023)
-
The efficacy of systemic antibiotics as an adjunct to surgical treatment of peri-implantitis: a systematic review
BMC Oral Health (2021)
-
Knowledge, awareness, and perception of dental students, interns, and freshly graduated dentists regarding dental implant complications in Saudi Arabia: a web-based anonymous survey
BMC Oral Health (2021)
-
Experience with bruxism in the everyday oral implantology practice in the Netherlands: a qualitative study
BDJ Open (2018)
