
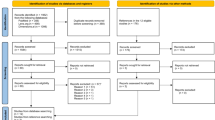
Key Points
-
Presents an analysis of the results of an online survey of current registrants of the BDJ UCL Eastman CPD programme.
-
As with a previous study, this survey confirms that the programme remains a popular means of obtaining verifiable CPD.
-
Confirms that the majority of registrants would prefer to have a broader range of study options and the award of verifiable CPD to be made more robust.
Abstract
Objective To ascertain from participants of the BDJ UCL Eastman CPD programme its value to their professional endeavours, and in particular to determine whether they would object to making it more robust especially in the way that the CPD hours are achieved.
Design An online questionnaire survey.
Method Participants were encouraged to complete an online survey of nine questions by 31 July 2012.
Results Of the 3,292 participants who began the survey, it was completed by 3,070 (93.2%). Of those, 2,952 (91.1%) thought that additional learning tools would be helpful. The ability to resubmit incorrect answers was preferred by 2,549 (80.1%) of the respondents. Two thousand two hundred and fourteen participants (69.9%) raised no objection to making the scoring system more robust and 953 (30.1%) objections to this proposition were recorded. Ninety-eight percent (3,128) favoured the regular inclusion and flagging of core subjects and 95% of these respondents thought it would be useful to record these separately. The most preferred method of obtaining verifiable CPD was cited by 1,075 (39.5%) participants as reading journals followed by attending lectures and hands-on courses. The BDJ was the preferred journal to achieve both verifiable and general CPD. Most participants (1,930; 67.7%) use a home computer to take part in this initiative while a significant minority use tablets and smart-phones.
Conclusion This survey showed that the BDJ UCL Eastman CPD journal-based verifiable CPD programme remains a popular method of fulfilling the GDC regulations and that the majority of participants are in favour of making the process more rigorous.
Similar content being viewed by others

Introduction
In 2003 the British Dental Journal (BDJ) in partnership with UCL Eastman CPD as the academic lead and Smile-on (Healthcare Learning Company Ltd) as the platform provider established a programme to enable all UK dental practitioners to collect a maximum of 48 hours of verifiable CPD per annum. Since 2003 each issue of the BDJ has contained two papers selected for verifiable CPD, with four multiple choice questions linked to each article. Practitioners received one hour of verifiable CPD per paper, giving a potential total of two verifiable CPD hours per BDJ issue. The template for this initiative was borrowed from the Journal of the American Dental Association (JADA) but differs in the way that the CPD hours are obtained in that participants are able to check whether they have answered correctly. If not, they are able to re-enter the quiz and repeat the exercise. There is a delay in the answers, which are published two issues later. In the JADA, the CPD hour is obtained only if three of the four questions are answered correctly. In the current scheme this is not the case and over the years has led to complaints that a less than scrupulous individual could obtain the points by scanning the articles1 or without having read the articles.2,3
This matter has been addressed in several editorials and was comprehensively defended in a paper by Hancocks4 stating, 'we are criticised in some quarters for the apparent ease with which users can obtain CPD hours from our programme. Detractors point out that the hours are given irrespective of how many questions are answered correctly. In essence, it is possible to fraudulently complete the answers. Yes, true. But what a sad reflection of our view of our fellow professionals and one that is not borne out by the figures: the majority of respondents get the majority of the questions right most of the time. Interestingly the attitude of the General Dental Council (GDC) on matters of this nature is that the important aspect is that dentists have read the material and reflected on it rather than necessarily getting all the answers right first time.'
In fact, as a more recent editorial notes,5 over the nine years of the project there have been regular discussions regarding the scoring system, namely whether to follow the JADA model making the process of obtaining verifiable CPD more robust. It was decided to canvas the views of the readers of the BDJ on this and other topics relevant to CPD by means of an online survey. The closing date was 31 July 2012.
Method
Using an online program (www.surveymonkey.com) the following nine questions were posed with the offer of a prize draw for all who completed the survey:
-
1
Currently, CPD activities in the BDJ are all article-related and question-based. Would it be helpful to vary the programme by introducing additional learning tools (for example, questions on a clinical photograph or radiograph)?
-
2
Verifiable CPD is currently received on submitting answers to the questions irrespective of whether answers are correct or not. If incorrect, would it enhance the learning experience to be informed of this and given the opportunity to revisit the article and resubmit any previously incorrect answers?
-
3
In order to make the process of granting verifiable CPD as robust as possible, would you have any objection to verifiable CPD being granted only if the participant answers at least three out of four questions correctly on each article?
-
4
If you answered 'YES' to question three (that is, you do have an objection), please explain why.
-
5
Would it be helpful if core CPD articles were to be included regularly in the CPD programme and flagged as such?
-
6
If you answered 'YES' to question five (that is, it would be helpful to include core CPD articles), would it then be helpful to record verifiable CPD on the core CPD articles separately in line with the mandatory domains?
-
7
How do you prefer to obtain verifiable CPD from the options below with 1 as the most preferred and 6 as the least preferred?
Dental journals: 1 2 3 4 5 6
Attending lectures: 1 2 3 4 5 6
Hands-on courses: 1 2 3 4 5 6
E-learning: 1 2 3 4 5 6
Webinars: 1 2 3 4 5 6
Other (see below):
If you have ticked 'Other' please specify below
-
1
If you undertake journal-based CPD, please list your preferred journals for this method of obtaining verifiable CPD and non-verifiable CPD
-
2
If you undertake any web-based CPD, which is your preferred method for access with 1 as the most preferred and 5 as the least preferred?
Work computer: 1 2 3 4 5
Home computer: 1 2 3 4 5
Mobile phone: 1 2 3 4 5
Tablet (eg iPad): 1 2 3 4 5
Other (see below):
If you have ticked 'Other' please specify below.
Results
While 3,292 dentists started the survey, it was completed by 3,070 (93.2%).
Figure 1 (Question 1) shows that the vast majority thought that questions making use of clinical photographs and or radiographs, as examples of additional learning tools, would be helpful.

Results for Question 1
Figure 2 (Question 2) indicates that a majority would like to be informed when an answer is incorrect and thus be able to review the article once again and resubmit the answer.

Results for Question 2
Figure 3 (Question 3) shows that 69% of the dentists did not object to (that is, supported) the verifiable CPD hour only being granted if at least three out four answers were correct.

Results for Question 3
Participants who had given a negative response to Question 3 were invited to explain the reason for their opposition. Of the 2,214 who had voted 776 offered varying views.
The following is a selection:
-
'A 75% score is too high and 50% would be more fair'
-
'CPD is a personal effort and should not be treated as an examination'
-
'You don't have to answer questions after attending a lecture for CPD'
-
'An incorrect answer would mean having to spend more time in reviewing the article and there would be no compensation for this'
-
'Ticking the wrong box by mistake would lose your chance of obtaining CPD'
-
'The questions are too often unclear, ambiguous, with double negatives and “tricky”'
-
'The questions often do not test the comprehension of the article'
-
'Why should the majority be penalised for the dishonest action of a few?'
Figure 4 (Question 5) shows that almost all the dentists would find it helpful to include flagged core CPD articles.

Results for Question 5
Figure 5 (Question 6) indicates that the overwhelming majority of those who had agreed with the proposition in Question 5 would also like the results from the Core CPD articles to be recorded separately.

Results for Question 6
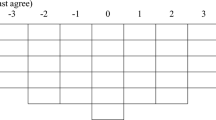
Figure 6 (Question 7) A Likert scale sets out which form of CPD is most favoured. Dental journals, attending lectures and hands-on-courses lead followed by e-learning and webinars. 'Other' forms, the least favoured, included sponsored CPD in practice, mandatory courses provided by the NHS and peer review meetings.

Results for Question 7
Question 8 requested the preferred journal(s) for verifiable and non-verifiable CPD.
For the former, the BDJ was most frequently cited. Also mentioned were BDA News, Dental Update, Endodontics, Independent, Aesthetic Dentistry, Dental Review, Vital, Oral B, Dental Summary Review, Evidence-Based Dentistry, FGDP Journal, British Journal of Disability, Primary Dental Health, Dental Practice, Private Dentistry and the Probe.
A similar pattern emerged for non-verifiable CPD but the list also included specialist journals, both UK and/or international, and textbooks.
Figure 7 (Question 9) indicates which are the preferred methods of accessing web-based CPD. The results show the home computer as being the preferred group followed by computers at work, tablets and mobile phones.

Results for Question 9
Discussion
In 2011 the GDC commissioned a literature review of the impact of CPD activity on individual practice and competence assurance of the dental profession.6
The authors concluded that although there were perceived benefits to personal learning plans, there 'were no high quality studies to demonstrate the effectiveness of CPD in terms of quality of care delivered, performance, professional standards, competence, public satisfaction or safety or their longer-term effects on knowledge retention and application.' In addition, no studies were found that demonstrated 'the regulatory purposes of making CPD a mandatory requirement'.
At present the GDC is undertaking a review project to develop a model of mandatory CPD that is fit for ongoing regulatory purposes and meets future requirements of revalidation.7 As part of the purpose of the review 'adapted or enhanced requirements should enable us to have greater confidence in the contribution CPD will make to demonstrating continued fitness to practise through revalidation and to our general regulatory approach'.
The value of the BDJ UCL Eastman CPD programme was demonstrated by Tredwin et al.8 They carried out a postal survey, sending questionnaires to 400 (out of then 7,242) randomly selected BDJ UCL Eastman CPD participants to elicit their views on the programme.
Among their conclusions were the following:
-
Journal based verifiable CPD appears to be a valuable method of undertaking lifelong learning
-
The level of the articles selected in the BDJ is appropriate
-
The majority of participants felt that this form of CPD increased their knowledge and had resulted in a change in their clinical practice.
In the current survey, 3,070 of 19,000 registrants (out of 38,000 dentists in the UK) indicated that journals are still the main source of both general and verifiable CPD (Fig. 7). The BDJ was the most frequently cited journal from which to gain both general and verifiable CPD and these were most often accessed from home or work computers (Question 9).
Since Tredwin et al.,8 the general availability of CPD has greatly expanded and the advent of more powerful electronic devices and techniques has resulted in greater expectations from the site. Thus it is not surprising that the vast majority of survey respondents welcomed additional learning tools with the introduction of, for example, questions on clinical photographs and radiographs as opposed to simply continuing with articles and related question-based activities alone (Fig. 1).
Of those who voiced their opposition to the change in scoring, a substantial proportion took the opportunity to complain about the style and content of the multiple-choice questions (MCQ). MCQs are an effective way of gaining summative information but there are disadvantages.9 It is acknowledged that the construction of effective questions can be difficult. The MCQ is made up of the correct answer surrounded by distracters. The latter must not be so far from the truth that the correct answer is patently obvious. When MCQs are used for courses of study, the compilers have the whole syllabus to choose from and thus can employ subtlety in their question design. The MCQs can then have a formative as well as summative value. BDJ articles are in the main confined to 3,000 words all chosen for a specific subject. This often makes the choice of the distracters difficult.
The purpose of this form of CPD is self-learning, the questions are superfluous to the test of how well the reader has understood or absorbed the information. They are constructed to limit the ability to answer merely by guessing and due to the restricted material can sometimes appear convoluted. They are the equivalent of the act of signing-in to a lecture to obtain proof of verifiable CPD.
Questions 2 and 3 are linked. The issue at stake is the fact that the CPD score is given as a maximum even if the answer is wrong. Since its inception this has been a bone of contention with a view that this has made the project a tick box exercise and doubts the effectiveness of CPD by this method. A recent paper10 questions the true lasting value of all types of CPD and how it can be proved that it has produced a true public benefit. The author recommends that proof should be obtained from the attendee not only of attendance but that they should be able to demonstrate whether they have absorbed the information by obtaining more than 60% correct answers in a test. Several correspondents have advanced this argument in various forms almost from the start decrying what Kelleher10 calls 'verifiable CPD tokenism'.1,2,3
Upcoming revalidation has spurred the GDC's CPD review to ascertain whether the current model of CPD will give the public confidence that the profession is keeping up to date and thus maintaining its skills and knowledge. This matter of confidence is emphasised by Kelleher 'in a cynical UK society, which increasingly questions the integrity and motivations of almost all professions, it is important that one can stress that the outcome (this being the application of any knowledge gained) for whichever CPD activity, produces safer or better treatment outcomes for patients.'10 Is there any evidence for this opinion?
In a survey11 Australian patients were given open-ended questions asking why they chose their regular medical practitioner and what constituted a good or bad GP. They concluded that the patients surveyed tended not to think of themselves as consumers. Being trustful of their doctor, they did not spend time investigating his or her knowledge in relation to the services. In their literature review, Lupton et al.11 noted that underlying UK health policy is a concept of consumerist behaviour.
Is the average dental professional likely to be questioned by their patients as to the amount of CPD that they have acquired or whether they have undertaken any at all? Can it not be assumed that the confidence the patient has is implicit in their preparedness to undergo treatment?
A survey of UK medical practitioners alludes to this question.12 Lay people were asked whether they considered their doctor's medical knowledge to be good, fair or poor. They were asked to give their reasons for their opinions and, in particular, the authors were curious to discover if the media affected their perception of the GPs medical knowledge.
They concluded that, 'asking patients about their general practitioner's medical knowledge may yield invalid results.' This is partly because patients defined medical knowledge in different ways, and partly because it appears that relatively few patients had enough knowledge about their own particular illnesses, or about possible alternative treatments, to make informed judgments. With reference to the effect of the media, relatively few people remarked that the media had affected their perception of their own GP's medical knowledge. It is of interest to note that a definition of knowledge offered by patients was the GP's ability to acknowledge uncertainty and refer patients to a specialist when necessary. The authors concluded, 'What is crucial is to assess quality from different stakeholder perspectives, but using measures that are valid and reliable.'12
A profession can be defined as 'a collective of expert service providers who have jointly and publicly committed to always give priority to the existential needs and interests of the public they serve above their own interests, and in turn are trusted by the public to do so.'13 Patients in general are unable to assess the work of their professional service providers objectively and thus 'individual professionals must be willing to review their peers and to submit themselves to eradicate 'rotten apples' or to appease disgruntled patients.'14
Even though there is no compelling evidence of the efficacy of CPD the drive to upgrade must be considered as 'best practice', for as the GDC stipulates, 'patients are right to expect that all members of the dental team are keeping their skills and knowledge up to date throughout their careers. We ensure this is happening by making CPD a requirement of all dental professionals' registration with us.'9
The wish by a majority of the participants to make the verifiable CPD programme more robust is testament to their acceptance that CPD should not only be done but also seen to be done and the authors wholeheartedly support these aspirations.
Conclusion
Key questions relating to the nature of verifiable CPD are:
-
Will it satisfy the participant's quest for knowledge and thereby enhance ability?
-
Will it satisfy the GDC's guidelines?
-
Will it give confidence to the public?
-
Will it allow an unprofessional token response?
This survey showed that the BDJ UCL Eastman CPD journal-based verifiable CPD programme remains a popular method of fulfilling the GDC regulations. A majority of participants support the suggestion that a verifiable CPD hour should only be achieved if three out of the four questions are answered correctly. There is a wish to obtain CPD by other ways than simple article-based means and to be made aware of core subjects when they occur as well being able to record the results of this activity separately.
References
Storrar I . An easy ride? Br Dent J 2003; 195: 230.
Gould A . Accumulating CPD hours. Br Dent J 2008; 204: 478.
Wilson S . Asinine system. Br Dent J 2012; 212: 574.
Hancocks S . CPD revisited Br Dent J 2007; 202: 703–704.
Hancocks S . Does D put the dilemma in CPD? Br Dent J 2012; 212: 461.
Eaton K, Brooke J, Patel R, Batchelor P, Merali F, Narain A . The impact of continuing professional development in dentistry: a literature review. London: GDC, 2011
General Dental Council. Project initiation document (PID) CPD Review 2011–2013. Version 2. London: GDC: 2012.
Tredwin C J, Eder A, Moles D R, Faigenblum M J . British Dental Journal based continuing professional development: a survey of participating dentists and their views. Br Dent J 2005; 199: 665–669.
Kramer G A, Albino J E, Andrieu S C et al. Dental student assessment toolbox. J Dent Educ 2009; 73: 12–35.
Kelleher M . The difficulties of making 'CPD verifiability' a legitimate measure of learning outcomes. Br Dent J 2012 213: 383–384.
Lupton D, Donaldson C, Lloyd P . Caveat emptor or blissful ignorance? Patients and the consumerist ethos. Soc Sci Med 1991 33: 559–568.
Chapple A, Campbell S, Rogers A, Roland M . Users' understanding of medical knowledge in general practice. Soc Sci Med 2002 54: 1215–1224.
Welie J V . Is dentistry a profession? Part 3. Future challenges. J Can Dent Assoc 2004 70: 676.
Welie J V . Is dentistry a profession? Part 2. The hallmarks of professionalism. J Can Dent Assoc 2004 70: 600.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Faigenblum, M., Eder, A. & Louca, C. BDJ UCL Eastman CPD programme: an online survey. Br Dent J 214, 519–523 (2013). https://doi.org/10.1038/sj.bdj.2013.507
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.2013.507
This article is cited by
-
Critical feedback
British Dental Journal (2013)
