
Abstract
Study design:
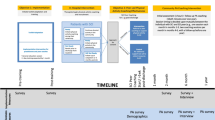
Quasi-experimental pre–post design with 6-month follow-up.
Objectives:
Active Living Leaders Training Program (ALLTP) equips individuals with knowledge and skills to encourage those with spinal cord injury (SCI) to increase their leisure-time physical activity (LTPA). The purpose of this pilot study was to, first, (i) evaluate participants’ perceptions of the relevance/usefulness of ALLTP material/presentation, (ii) examine changes in participants’ self-efficacy to promote LTPA, (iii) identify program components associated with greater self-efficacy and, second, measure participants’ use of ALLTP skills and resources over the subsequent 6 months.
Setting:
Canada.
Methods:
Six SCI fitness trainers and six adults with SCI completed the three sections of ALLTP and, after each section, provided feedback. Six months later, participants’ use of resources and skills was assessed. Means, standard deviations, repeated measures analysis of variance and Pearson’s correlations were computed.
Results:
Relevance/usefulness of the program was rated favorably. Self-efficacy to speak about and encourage LTPA remained high throughout the ALLTP and was positively correlated with the relevance/usefulness of program content and presentation. At follow-up, participants had discussed LTPA with an average of seven people with disabilities and reported using at least one skill and resource from the ALLTP during those discussions.
Conclusions:
Users had positive perceptions of ALLTP and reported using the training to promote LTPA to others with disabilities. Participant feedback has been used to improve ALLTP. ALLTP can now be used to train people with SCI and SCI fitness trainers to promote LTPA to others with disabilities.
Similar content being viewed by others


Introduction
Despite the known benefits of physical activity, 50% of adults with spinal cord injury (SCI) do not engage in any leisure-time physical activity (LTPA), which are the physical activities that people choose to do in their leisure time such as sports and exercise.1, 2 To address physical inactivity, informational resources, such as the Physical Activity Guidelines for Adults with SCI, have been developed.3 Yet, information alone is insufficient to increase LTPA, given the numerous barriers and challenges to participation faced by people with SCI.4
Within the limited research investigating the dissemination of LTPA guidelines within special populations, one study examined the effectiveness of a dissemination event to mobilise the LTPA guidelines among individuals with SCI.5 This study revealed that initial increases in confidence to adopt the LTPA guidelines after the dissemination event were not sustained 1 month later, nor were there increases in LTPA participation. This study’s findings highlight the need for interpersonal communication and strategies to disseminate evidence-based physical activity guidelines.6
Peer mentors may have an important role in communicating such guidelines and motivating efforts to achieve the guidelines. In a recent systematic review,7 the authors concluded that trained peer mentors are as effective as professional counselors for increasing LTPA behavior across a wide range of populations. Among people with SCI, peers have been identified as a preferred source of LTPA information.8 Indeed, a peer-mediated strength-training session positively influenced the uptake of the Physical Activity Guidelines for Adults with SCI3 among individuals with SCI who were previously inactive.9 Four weeks after the peer-mediated strength-training session, the majority of participants were still achieving the Physical Activity Guidelines for Adults with SCI3 as evidenced by their continued participation in strength-training activities. These data provide support for the involvement of peers in disseminating and encouraging people to achieve the Physical Activity Guidelines for Adults with SCI.3
Peers might be a particularly powerful source of motivation and encouragement for LTPA participation because they provide social support. In addition to information dissemination, peer mentors can provide people with SCI with much needed social support. For example, research conducted by Rees et al.10 has found that social support is an important resource for individuals who have recently experienced a SCI. Although individuals with SCI felt adequately supported immediately after their injury in the hospital setting, there appeared to be a lack of support outside of the hospital. Offering support for individuals with SCI through LTPA peer mentoring may help address this lack of support beyond the hospital. People with SCI often identify social contacts and interactions with other physically active adults with disabilities as a primary facilitator for LTPA.11 Furthermore, a qualitative meta-synthesis of the SCI literature on LTPA barriers and facilitators concluded that social support, from networks including friends, family, peers, disability groups and activity centers, is crucial in facilitating LTPA.12 Given the important role that social networks can have in promoting LTPA to adults with SCI and other disabilities, it is important to provide those who may be in a position to promote LTPA with skills and information to do so effectively.
One possible way to enhance peer mentors’ ability to promote LTPA is to provide them with training in the use of transformational leadership (TFL) behaviors. TFL is a leadership style and set of skills that, when used by a leader, can elevate followers’ goals and provide them with the confidence to strive beyond minimum expectations.13 TFL is comprised of four behavioral dimensions that include 'idealized influence' (for example, leading by example), 'intellectual stimulation' (for example, thinking about old problems in new ways), 'individualized consideration' (for example, displaying an understanding of others’ needs) and 'inspirational motivation' (for example, articulating a compelling vision for the future).13 Use of these leadership behaviors has been associated with followers’ enhanced self-efficacy to participate in LTPA.14, 15 As such, there would be merit in teaching peer mentors to use TFL skills that could be used when promoting LTPA to individuals with disabilities.
Presumably, individuals will be more likely to use newly developed leadership skills if they have strong self-efficacy to use those skills. According to Self-Efficacy Theory, of the four sources of self-efficacy (vicarious experiences, mastery experiences, verbal persuasion and physiological/affective arousal), mastery experiences have the greatest influence on self-efficacy.16 Thus, in leadership training programs, self-efficacy could be enhanced through individuals engaging in successful practice of their newly acquired skill set.16 Indeed, several studies have shown that academic mentor training programs containing practical components as well as information and skills training have significantly increased participants’ confidence in their ability to provide academic mentorship to others.17, 18, 19 Furthermore, there is evidence from various fields of study to suggest that self-efficacy to perform a specific task is positively associated with how well the corresponding task is performed. 20, 21, 22, 23, 24 Given the importance of self-efficacy in the use of leadership/mentorship skills, it is important that mastery experiences be built into training programs that are designed to develop these skills.
The Active Living Leaders Training Program (ALLTP) is an online mentorship training program, designed to meet the preferences of individuals with SCI to receive physical activity-enhancing information from peers with SCI and knowledgeable others.25 The aim of ALLTP is to provide peers with SCI, and others who may come in contact with adults with SCI, with (i) evidence-based information identified as important for promoting LTPA in the SCI community,4 (ii) training in the use of TFL behaviors and (iii) the opportunity to practice newly acquired knowledge and skills to mentor those with SCI to increase their LTPA. The format of ALLTP was based on the Knowledge Mobilization Training Series, a program designed to disseminate information and resources to health-care professionals to promote LTPA among individuals with SCI, and that has received positive user ratings.26 Before launching ALLTP as a national program, a pilot study was undertaken to elicit feedback27 and identify any necessary program modifications.
Therefore, the primary objective of this pilot study was to (i) evaluate participants’ perceptions of the relevance/usefulness of the ALLTP material and its presentation (ii) examine the effects of the training on users’ self-efficacy to promote LTPA and (iii) identify components of the program (that is, type of information, practicum component) that are associated with participants’ self-efficacy. It was hypothesised that (i) users will rate the relevance/usefulness of ALLTP information and its presentation favorably;26 (ii) users’ self-efficacy would increase from pre–post training;17 (iii) characteristics of the implementation (information and structure) that were compatible with participants’ needs27 would be positively associated with participants’ self-efficacy as they may contribute to participants’ mastery experiences.16 The second objective of this pilot study was to determine whether participants used the skills developed during ALLTP over a 6-month follow-up.
Materials and methods
Program overview
The ALLTP consists of an online program (www.activelivingleaders.ca) and accompanying handbook with three sections: LTPA knowledge, TFL skills and practice interactions. See Table 1 for a full description of each ALLTP section. In the first two sections of the online program, information and resources are presented on screen with voice-overs delivered by a knowledge translation specialist (LTPA knowledge section) and a professor (TFL skills section). The third section is completed using the handbook whereby participants are given sample scenarios and case studies and are asked to engage in six practice interactions with a partner to practice their newly acquired knowledge and skills.
Participants
Participants were healthy adults with chronic SCI, as well as able-bodied exercise trainers drawn from three community-based SCI exercise facilities. Six adults with SCI (83% male; age range=20 to 60+ years) and six SCI exercise trainers (50% male; age range=20–60 years) were enrolled. Participants were recruited via word of mouth and advertisements posted in the exercise facilities.
Measures and procedure
Feedback surveys
After each section, participants completed an online survey to assess the following: perceptions of relevance and usefulness of content, presentation of material, program preferences and self-efficacy to speak about LTPA (that is, convey specific information about physical activity guidelines, fitness benefits and so on) and encourage LTPA (that is, provide support/encouragement through TFL skills) among individuals with SCI (see Table 2 for survey items). Participants were also asked to report the number of practice interactions that they completed during Section Three. Most survey items were adapted from non-standardised scales assessing participants’ perceptions of programs with similar purposes.26, 28
Six-month follow-up
Participants were invited to complete an online survey. One item was used to determine whether, since completing ALLTP, participants had spoken to someone with a disability about LTPA. For participants who responded ‘yes’, they then reported how many people they had spoken with and, on average, the duration of each discussion in minutes. Eight LTPA-promoting resources described in ALLTP were listed, and participants indicated which of the resources they had shared with people with a disability. Finally, the four TFL behaviors were listed, and respondents indicated which ones they had used during their discussions and provided specific examples of how they used the behavior.
Procedure
All study materials and procedures were approved by the institutional research ethics board prior to study commencement. Participants provided informed consent before completing a demographic and a baseline measure of self-efficacy. Next, they were sent a link to the ALLTP website. Upon completion of each section, participants completed the corresponding feedback survey. Participants received a $10 gift card for each completed survey and a certificate of completion upon completing all three ALLTP sections. A link to the follow-up survey was sent 6 months later.
Data analysis
Missing data points were replaced with the group mean for the corresponding survey item.29 Given that there were no significant differences between adults with SCI and exercise trainers’ responses, responses were grouped for analysis. Descriptive statistics were calculated for survey items with continuous and categorical response options. Open-ended responses were analyzed using inductive content analysis. Repeated measures analysis of variance were used to test for changes in self-efficacy. Pearson’s correlations were used to explore which components of the program were associated with participants’ self-efficacy to speak about/encourage LTPA to individuals with SCI and their desire to recommend the training.
Results
In all, 10 of the 12 participants completed all 3 sections of the ALLTP. Mean scores for all items were high, ranging between 3.90 and 4.67 on a 5-point scale, representing favorable ratings of the relevance/usefulness of the ALLTP material/presentation and high self-efficacy (see Table 3 for means and standard deviations). Thematic analyses (see Table 4 for a summary of the coding themes) indicated that many elements of the program were perceived favorably, including the format of presentation, how the material was explained and the inclusion of resources. A consistent suggestion was to include additional resources for each section. There were few program dislikes; however, some participants noted barriers created by technology, as well as difficulty scheduling practice interactions. Furthermore, there was also a request for more experiential learning. Participants completed an average of 4 practice interactions (s.d.=1.29) during section 3. Self-efficacy to speak about LTPA did not significantly differ between time points, F(2, 22)=0.88, P=0.43, nor did self-efficacy to encourage LTPA, F(3, 33)=0.16, P=0.93.
Participants’ self-efficacy to speak to people with SCI about LTPA and encourage adults with SCI to participate in LTPA was positively correlated with perceptions that the program was informative/provided ideas (all r-values=0.41 to 0.71, all P-values<0.25), that the development, explanations and benefits of following the Physical Activity Guidelines for Adults with SCI3 and using TFL behaviors were relevant/useful (all r-values=0.35 to 0.82, all P-values<0.26) and that the presentation was clear/stimulating and was appropriately paced (all r-values=0.45 to 0.73, all P-values<0.14). Participants’ likelihood of recommending ALLTP was also positively correlated with positive perceptions of most of the program characteristics (Table 5).
Nine participants completed the 6-month follow-up (Table 6). Eight out of nine had spoken with at least one other person with a physical disability about LTPA since completing ALLTP. They reported speaking with an average of seven people (s.d.=3.02) and spending ~15 min (s.d.=18.71) discussing LTPA with each person. Seven out of the eight participants (87.5%) shared at least one resource presented in ALLTP; the remaining participants shared information about a local adapted physical activity program. Information was shared most frequently for the following resources: Get in Motion Physical Activity Counseling Service30 (44.4%); Canadian Wheelchair Sports Association (44.4%); SCI Action Canada31 (33.3%); and Active Homes Strength Training Guide32 (33.3%). Most participants (87.5%) used at least one TFL skill during their peer mentorship interaction. Inspirational motivation (77.8%) and individualised consideration (66.7%) were used most often. Examples of how participants used those behaviors are presented in Table 6.
Discussion
This pilot study of the ALLTP revealed that participants had favorable ratings of the usefulness and relevance of the content and resources and their presentation. Contrary to our hypothesis, there was no statistically significant change in participants’ self-efficacy to speak about or encourage LTPA to others from pre to post training. However, the implementation characteristics that met participants’ needs (program content and its presentation) were positively correlated with users’ self-efficacy to speak about and encourage LTPA to others. At follow-up, participants had discussed LTPA with an average of seven people with disabilities, and reported using at least one TFL skill and sharing at least one resource from the ALLTP during those discussions, suggesting that participants utilised the information and skills taught during training.
Overall, participants rated the utility/relevance of the ALLTP content/resources and its presentation favorably. These findings are consistent with the evaluation of a program designed to disseminate information to health-care providers to promote LTPA among individuals with SCI, which had similar content and presentation formatting.33 Our findings, taken together with reported ‘likes’ of the program, suggest that participants valued learning about the Physical Activity Guidelines for Adults with SCI3 and the benefits of LTPA, how to use TFL skills and practicing application of these skills and knowledge. Participants valued the webinar format and the clarity and conciseness of the material’s presentation. Positive ratings of most of these elements were associated with a greater likelihood that participants would recommend the training to others. According to Durlak’s and DuPre’s27 framework for the factors that affect implementation of promotion and prevention programs, positive perceptions of the value of a program, specifically its need and benefits, can positively influence program implementation. Participants’ reported value of the program may be rooted in their perceived need and benefit of the program. Taken together, the evidence suggests that the format and content of the program are appealing to the intended users of the ALLTP, which could increase the use of the program.
Participants did, however, identify some ‘dislikes’ and areas for improvement, which have been addressed in subsequent revisions of the program. Given that some participants suggested adding more examples and detailed descriptions of LTPA for individuals with SCI, the ALLTP handbook now includes links to video demonstrations of different types of exercise and sport activities for people with SCI. Exposure to these videos could bolster participants’ self-efficacy to discuss or even demonstrate such activities to others.16 In addition, upon completion of the program, participants are mailed a copy of the SCI Get Fit Toolkit34 that provides sample activity plans for individuals with SCI. Some participants felt that the didactic presentation format used in Section Two (TFL training) was impersonal. A meta-analysis of educational interventions for health-care professionals revealed that the combination of interactive and didactic education was more effective for improving behavior than either alone.35 Drawing on this evidence, we subsequently attempted to deliver the TFL training using a live, interactive webinar whereby trainees could interact with a TFL expert. Unfortunately, this approach proved technologically challenging and unsustainable. We have, however, reduced the number of practice interactions in Section Three from six to three in response to participants’ feedback. According to the Theory of Deliberate Practice by Ericsson et al,36 accumulating hours of practice does not necessarily result in exceptional skill. More importantly, it is individuals’ deliberate effort put towards the practice that contributes to skill development, and this requires not only outlining explicit goals but also possessing sufficient resources, such as time. There were reported scheduling difficulties for the practice interactions, and the average number of completed practice interactions was almost half of the suggested number. Suggesting additional practice interactions beyond this value may discourage deliberate practice, as individuals may not have sufficient resources to do so. Instead, it may encourage individuals to merely complete the practice with a lack of effort, which has been to shown to halt skill improvement. Hence, as suggested by the Theory of Deliberate Practice, a few effortful practice interactions may be more likely to contribute to skill development compared with many practice interactions without invested effort or the required resources.
Participants’ self-efficacy to speak about and encourage LTPA to others did not significantly change from pre to post training. This result contradicts findings from a similar training program for health-care professionals, whereby participants’ self-efficacy to promote LTPA and parasport to individuals with physical disabilities increased from pre to post training.28 However, unlike that study,28 our participants were recruited from exercise facilities for individuals with SCI. Participants may have had previous experiences discussing and encouraging LTPA that contributed to their initial high levels of self-efficacy16 (both Ms ≥ 4.17 out of 5) and resulted in a ceiling effect for this outcome. Future users of the ALLTP who begin the program with lower confidence to speak about and encourage LTPA to people with SCI may benefit from coached practice and/or videos of effective mentor–mentee interactions incorporated into Section Three as previous academic mentor training programs containing practical components have increased participants’ confidence to mentor others.17, 18, 19 These strategies could contribute to users’ self-efficacy to talk to others about LTPA by contributing to their mastery and by providing vicarious experiences.16
Participants reported using TFL skills during the 6-month follow-up period. To the best of our knowledge, this is the first study to directly assess the extent to which mentors are using TFL behaviors to promote LTPA to individuals with disabilities. This is an encouraging finding, given that the use of TFL skills by physical education teachers is associated with higher levels of LTPA self-efficacy and motivation in their students.14, 15 If LTPA information is presented to people with disabilities vis a vis TFL skills, they may be more likely to act on that information. Additional research is needed to test this hypothesis.
Taken together, the results of this pilot study suggest that the ALLTP is perceived favorably by targeted end-users and that participants are using the skills taught during the training. As well, the results have informed important modifications that should enhance the effectiveness of the program. Yet, more work is needed to continue assessing the ALLTP’s effectiveness. The framework for the design and evaluation of complex health interventions created by Campbell et al.37 outlines five phases that must be completed to develop evidence for a program’s efficacy and effectiveness: Theory, Modelling, Exploratory Trial, Definitive Randomized Controlled Trial and Long-term Implementation. This project is a study reflecting the exploratory trial phase. Therefore, the subsequent phase would be to compare the ALLTP with a control condition to determine whether the program is more effective for improving participants’ ALLTP knowledge, mentoring skills and confidence compared with receiving no training at all. This phase has shown to be invaluable within the context of assessing mentor training programs, as a randomised controlled trial successfully revealed an academic mentor training program’s positive impact on mentors’ skills in comparison with that of those in a control condition.18
A couple of study limitations warrant mention. First, participants’ previous experiences discussing LTPA or mentoring were not measured and could have helped explain participants’ initially high levels of self-efficacy to talk about and encourage LTPA to others.16 Second, given the focus on participants enrolled in the ALLTP, we did not assess their influence on others. According to Campbell et al.37, this comprises the fourth phase of acquiring evidence for the effectiveness and efficacy of an intervention. In alignment with Campbell et al.37, our subsequent research will evaluate whether people with SCI become more physically active after discussing LTPA with an ALLTP trained mentor. Third, there was no evaluation of self-efficacy at the 6-month follow-up after training completion, which may be worthwhile to investigate in order to assess the program’s long-term effects and to determine whether ongoing mentor support is required. There have been inconsistent findings with regard to post-training mentoring self-efficacy. Some studies assessing academic mentoring programs have revealed that participants’ self-efficacy remained elevated 1 year post training,38 whereas a study evaluating a training program for health-care providers to promote LTPA among individuals with SCI showed that self-efficacy had decreased 6 months post training.33 Durlak and DuPre’s27 framework of factors that affect implementation outlines ongoing technical and emotional support provided to trainees as an important element to consider. Assessing self-efficacy at the 6-month post-training follow-up for ALLTP would provide greater insight into the appropriate and relevant type of ongoing support that could be provided to mentors in this specific context.
In summary, the results of this pilot study suggest that ALLTP can be used to train people with SCI and SCI fitness trainers to promote LTPA to others with disabilities. The findings also provide direction for the development of programs to train people with SCI to deliver other types of information related to living with an SCI (e.g., health, sexuality, employment).
Data Archiving
There were no data to deposit.
References
Crawford A, Hollingsworth HH, Morgan K, Gray DB . People with mobility impairments: physical activity and quality of participation. Disabil Health J 2008; 1: 7–13.
Martin Ginis KA, Arbour-Nicitopoulos KP, Latimer AE, Buchholz AC, Bray SR, Craven BC et al. Leisure time physical activity in a population-based sample of people with spinal cord injury part II: activity types, intensities, and durations. Arch Phys Med Rehabil 2010; 91: 729–733.
Martin Ginis K, Hicks AL, Latimer AE, Warburton DER, Bourne C, Ditor DS et al. The development of evidence-informed physical activity guidelines for adults with spinal cord injury. Spinal Cord 2011; 49: 1088–1096.
Foulon BL, Lemay V, Ainsworth V, Martin Ginis KA . Enhancing physical activity guidelines: a needs survey of adults with spinal cord injury and health care professionals. Adapt Phys Activ Q 2012; 29: 329–345.
Gainforth HL, Latimer-Cheung AE, Athanasopoulos P, Martin Ginis KA . Examining the effectiveness of a knowledge mobilization initiative for disseminating the physical activity guidelines for people with spinal cord injury. Disabil Health J 2013; 6: 260–265.
Latimer AE, Brawley LR, Bassett RL . A systematic review of three approaches for constructing physical activity messages: what messages work and what improvements are needed? Int J Behav Nutr Phys Act 2010; 7: 36.
Martin Ginis KA, Nigg CR, Smith AL . Peer-delivered physical activity interventions: an overlooked opportunity for physical activity promotion. Transl Behav Med 2013; 3: 434–443.
Faulkner G, Gorczynski P, Arbour K, Letts L, Wolfe D, Martin GKA Messengers and methods of disseminating health information among individuals with spinal cord injury: a scoping review. In: Berkovsky TC (ed.). Handbook of spinal cord injuries: types, treatments and prognosis. Nova: Hauppauge, NY, USA, 2009..
Latimer-Cheung AE, Arbour-Nicitopoulos KP, Brawley LR, Gray C, Wilson AJ, Prapavessis H et al. Developing physical activity interventions for adults with spinal cord injury. Part 2: motivational counseling and peer-mediated interventions for people intending to be active. Rehabil Psychol 2013; 58: 307–315.
Rees T, Smith B, Sparkes AC . The influence of social support on the lived experiences of spinal cord injured sportsmen. Sport Psychol 2003; 17: 135–156.
Jaarsma EA, Dijkstra PU, Geertzen JHB, Dekker R . Barriers to and facilitators of sports participation for people with physical disabilities: a systematic review. Scand J Med Sci Sport 2014; 24: 871–881.
Williams TL, Smith B, Papathomas A . The barriers, benefits and facilitators of leisure time physical activity among people with spinal cord injury: a meta-synthesis of qualitative findings. Health Psychol Rev 2014; 8: 404–425.
Bass BM, Riggio RE . Transformational leadership. second edn. Psychology Press: New Jersey, USA. 2006.
Beauchamp MR, Barling J, Morton KL . Transformational teaching and adolescent self-determined motivation, self-efficacy, and intentions to engage in leisure time physical activity: a randomized controlled pilot trial. Appl Psychol Health Well Being 2011; 3: 127–150.
Morton KL, Keith SE, Beauchamp MR . Transformational teaching and physical activity: a new paradigm for adolescent health promotion? J Health Psychol 2010; 15: 248–257.
Bandura A . Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev 1977; 84: 191.
Feldman MD, Huang L, Guglielmo BJ, Jordan R, Kahn J, Creasman JM et al. Training the next generation of research mentors: the University of California, San Francisco, clinical & translational science institute mentor development program. Clin Transl Sci 2009; 2: 216–221.
Pfund C, Spencer KC, Asquith P, House SC, Miller S, Sorkness CA . Building national capacity for research mentor training: an evidence-based approach to training the trainers. CBE Life Sci Educ 2015; 14: ar24.
Tsen LC, Borus JF, Nadelson CC, Seely EW, Haas MA, Fuhlbrigge AL . The development, implementation, and assessment of an innovative faculty mentoring leadership program. Acad Med 2012; 87: 1757.
Bandura A Toward an agentic theory of the self. In: Marsh HW, Craven RG, McInerney DM (eds). Self-processes, learning and enabling human potential: dynamic new approaches. Information Age Publishing: Charlotte, NC, USA, 2008..
Bandura A . On the functional properties of perceived self-efficacy revisited. J Manag 2012; 38: 9–44.
Moritz SE, Feltz DL, Fahrbach KR, Mack DE . The relation of self-efficacy measures to sport performance: a meta-analytic review. Res Q Exerc Sport 2000; 71: 280–294.
Sadri G, Robertson IT . Self‐efficacy and work‐related behaviour: a review and meta‐analysis. Appl Psychol-Int Rev 1993; 42: 139–152.
Schwarzer R . Self-Efficacy: Thought Control of Action. Taylor & Francis: New York, NY, USA. 2014.
Letts L, Martin Ginis KA, Faulkner G, Colquhoun H, Levac D, Gorczynski P . Preferred methods and messengers for delivering physical activity information to people with spinal cord injury: a focus group study. Rehabil Psychol 2011; 56: 128–137.
Jeske S, Tomasone T, Arbour-Nicitopoulos, Ginis S, Martin Ginis K . Knowledge Mobilization Training Series (KMTS) quality improvement study. J Spinal Cord Med 2014; 37: 646 (abstract).
Durlak JA, DuPre EP . Implementation matters: a review of research on the influence of implementation on program outcomes and the factors affecting implementation. Am J Community Psychol 2008; 41: 327–350.
Tomasone JR, Martin Ginis KA, Estabrooks PA, Domenicucci L . ‘Changing Minds’: determining the effectiveness and key ingredients of an educational intervention to enhance healthcare professionals’ intentions to prescribe physical activity to patients with physical disabilities. Implement Sci 2014; 9: 30–41.
Tabachnick BG, Fidell LS . Using multivariate statistics. 4th edn. Allyn and Bacon: Needham, MA, USA. 2001.
Arbour-Nicitopoulos KP, Tomasone JR, Latimer-Cheung AE, Martin Ginis KA . Get in motion: an evaluation of the reach and effectiveness of a physical activity telephone counseling service for Canadians living with spinal cord injury. PM R 2014; 6: 1088–1096.
Martin Ginis KA, Latimer-Cheung A, Corkum S, Ginis S, Anathasopoulos P, Arbour-Nicitopoulos K et al. A case study of a community-university multidisciplinary partnership approach to increasing physical activity participation among people with spinal cord injury. Transl Behav Med 2012; 2: 516–522.
Latimer AE, Brawley LR, Martin Ginis KA, Prapavessis H, Tomasone J Active Homes: a preliminary evaluation of a peer‐mediated, home-based strength training session for people with paraplegia. Poster presented at: the annual meeting of the Canadian Society for Psychomotor Learning and Sport Psychology; October 28–30, 2010; Ottawa, Ontario, Canada.
Tomasone JR, Martin Ginis KA, Estabrooks PA, Domenicucci L . Changing minds, changing lives from the top down: an investigation of the dissemination and adoption of a Canada-wide educational intervention to enhance health care professionals’ intentions to prescribe physical activity. Int J Behav Med 2014; 22: 336–344.
Arbour-Nicitopoulos KP, Martin Ginis KA, Latimer-Cheung AE, Bourne C, Campbell D, Cappe S et al. Development of an evidence-informed leisure time physical activity resource for adults with spinal cord injury: the SCI Get Fit Toolkit. Spinal Cord 2013; 51: 491–500.
Forsetlund L, Bjørndal A, Rashidian A, Jamtvedt G, O’Brien MA, Wolf F et al. Continuing education meetings and workshops: effects on professional practice and health care outcomes. Cochrane Database Syst Rev 2009; 2: 1–99.
Ericsson KA, Krampe RT, Tesch-Römer C . The role of deliberate practice in the acquisition of expert performance. Psychol Rev 1993; 100: 363.
Campbell M, Fitzpatrick R, Haines A, Kinmonth AL, Sandercock P, Spiegelhalter D, Tyrer P . Framework for design and evaluation of complex interventions to improve health. BMJ 2000; 321: 694–696.
Feldman MD, Steinauer JE, Khalili M, Huang L, Kahn JS, Lee KA et al. A mentor development program for clinical translational science faculty leads to sustained, improved confidence in mentoring skills. Clin Transl Sci 2012; 5: 362–367.
Acknowledgements
The ALLTP is funded by the Government of Canada’s Social Development Partnerships Program – Disability Component (SDPP-D).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Salci, L., Perrier, M., Ginis, S. et al. Active Living Leaders Training Program for adults with spinal cord injury: a pilot study. Spinal Cord 54, 662–669 (2016). https://doi.org/10.1038/sc.2015.168
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2015.168
This article is cited by
-
Dissemination and implementation strategies for physical activity guidelines among adults with disability, chronic conditions, and pregnancy: a systematic scoping review
BMC Public Health (2022)
-
Pilot study of a training program to enhance transformational leadership in Spinal Cord Injury Peer Mentors
Spinal Cord Series and Cases (2018)
