
Abstract
Study design:
Retrospective study.
Objectives:
To analyze the neurogenic bladder characteristics and treatment approaches in patients with upper and lower cervical spinal cord injury (SCI) in order to make proper and reasonable decisions to the relevant patients.
Setting:
Rehabilitation center in Ankara, Turkey.
Method:
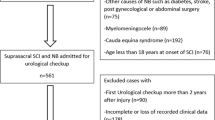
Ninety patients with cervical SCI were included. The urodynamic analyses of the patients were conducted retrospectively by using the urodynamic laboratory records. The patients were divided into two groups as the upper cervical SCI (UCSCI) group (C1-C5) and lower cervical SCI (LCSCI) group (C6-C8).
Results:
In this study, 82 male (91.1%) and 8 (8.9%) female patients were included. There were 51 UCSCI patients with the mean age of 34.2±16.1 years and 39 LCSCI patients with the mean age of 30.4±12.5 years. Detrusor overactivity and preservation of the bladder-filling sensation were significantly more frequent in the UCSCI group than in the LCSCI group (P=0.048, P=0.000 respectively). Moreover, there were statistically significant differences between the groups regarding the bladder-emptying methods, residual volume and the frequency of anticholinergic and alpha blocker use (all P<0.05). No significant difference was found between the groups regarding the frequency of autonomic dysreflexia, detrusor hypocompliancy and the bladder-storage and -emptying disorders (all P>0.05).
Conclusion:
Our results demonstrate that there are differences in the upper and lower SCI cases in terms of neurogenic bladder characteristics and treatment approaches.
Similar content being viewed by others


Introduction
Spinal cord injury (SCI) is a disease that is resulted by traumatic or nontraumatic reasons, and it causes restriction of self-care, mobilization and daily activities of the patients to a considerable degree. The SCI incidence was reported to be 15–40 per million.1, 2 The damage as a result of this injury not only limits the movement of the patient but also causes vital changes in the functions of many organs and lead to life-threatening complications. The aforementioned problems are more severe in cases of cervical SCI. Neurogenic bladder is commonplace in SCI patients. It decreases life span and adversely affects the quality of life.3, 4, 5, 6 Although the neurogenic bladder was one of the most important cause of morbidity/mortality in SCI patients in the past when the examination and treatment were not sufficiently developed, it has reached to a curable level today as a result of new developments.
The purpose of this study was to analyze the neurogenic bladder characteristics and treatment approaches retrospectively in the cervical SCI cases by using the urodynamic records of our hospital. As there were some differences in the functional abilities like hand function, sitting balance, and so on in upper (C1-C5) and lower (C6-C8) cervical SCI patients, we hypothesized that neurogenic bladder characteristics and treatment approaches would also differ in these groups. The aim of this study was to make proper and reasonable decisions for the neurogenic bladder treatment approaches in relevant patients with cervical SCI.
Materials and methods
Ninety patients with traumatic cervical SCI who had been referred to the urodynamics laboratory because of neurogenic bladder between 2002 and 2011 were included in this study. The age, gender, interval between the SCI and the urodynamic examination and etiological factor and SCI level according to American Spinal Injury Association Impairment Scale (AIS) classification of the patients were recorded. The patients were divided into two groups as the upper cervical SCI (UCSCI) group (C1-C5) and lower cervical SCI (LCSCI) group (C6-C8).
The urodynamic analyses of the patients were conducted retrospectively by using the urodynamic laboratory records. Urodynamic investigations were performed by the same investigator (ME) using a Libra+ (MMS, Enschede, The Netherlands) urodynamic measurement system. Each patient was positioned a supine on a urological table. An 8-Fr 2-lumen catheter for adult patients and a 6-Fr 2-lumen catheter for pediatric patients were introduced transurethrally for bladder filling. The bladder was emptied. Continuous medium fill cystometry was performed at 50 ml min−1 for adults at 20 ml min−1 for children with room temperature sterile saline. Blood pressure monitoring was carried out during the cystometric examinations, and signs or symptoms of autonomic dysreflexia were monitored. The patients were informed about the bladder-filling sensations (the first sensation of bladder filling, the first desire to void and a strong desire to void) before the investigation and were asked to report all sensations related to bladder filling, but not to report if they do not feel anything.7, 8, 9 Filling was terminated when the patient had a strong desire to void, when significant leakage occurred, when intravesical pressure reached 40 cm H2O, observation of autonomic dysreflexia (AD) and blood pressure changes (systolic blood pressure >140 mm Hg or 20–40 mm Hg increase in the systolic blood pressure in adults and 15 mm Hg increase in the systolic blood pressure in children10). The detrusor type and compliance, bladder-filling sensation, expected bladder capacity for children, maximum cystometric capacity, volume of micturated urine and residual volume were analyzed. The presence of storage and emptying disorder were determined according to the results of parameters analyzed in the filling and voiding phases. Additionally, the prescribed medical treatments and emptying methods were recorded.
The type of detrusor was classified as overactive, normoactive and underactive, detrusor hypocompliance was classified as present or absent11 and bladder-filling sensation was classified as absent, partially preserved and preserved.9 The compliance was considered as normal when the detrusor pressure was ⩾20 ml per cm H2O and it was considered as hypocompliance when the detrusor pressure was <20 ml per cm H2O.11 The expected bladder capacity was calculated according to the age formula in the children (for children <2 years old: (2 × age+2) × 28 ml and for children >2 years old: (age/2+6) × 28 ml).12 The lower limit of the normal bladder capacity was determined as 300 ml for adult patients.13, 14, 15, 16 The lower limit was determined as 300 ml in the children who were ⩾10 years old, similar to adult patients, as the expected bladder capacity measured with the formula was >300 ml in these children. Storage disorder presence was accepted if the maximum cystometric capacity measured during the filling phase was <300 ml in adult patients and in children >10 years and if the maximum cystometric capacity measured during the filling phase was lower than the expected bladder capacity in children <10 years. Besides, it was accepted that there was emptying disorder when the residual volume was ⩾50 ml in the adult patients and ⩾20 ml in the pediatric patients at the end of the voiding phase. The prescribed medical treatment (anticholinergic, alpha blocker and baclofen) and the prescribed emptying method (spontaneous voiding, emptying without catheter, intermittent catheterization and indwelling catheter) were recorded. The frequencies of self-intermittent catheterization and intermittent catheterization performed by the caregiver were also recorded.
SPSS software Version 15.0 (SPSS Inc., Chicago, IL, USA) was used in the evaluation of the data and P<0.05 was considered as statistically significant. T-test for independent samples was used in the comparison of descriptive statistics and measured parameters. Chi-square test or Fischer’s exact test was used when appropriate in the comparison of categorical parameters.
Results
Demographic and clinical features of the patients are shown in Table 1. The comparisons of the urodynamic findings and therapeutic approaches are given in Table 2. Detrusor overactivity and preservation of the bladder-filling sensation were significantly more frequent in the UCSCI group than in the LCSCI (P=0.048, P=0.000 respectively). Moreover, there were significant differences between the groups regarding bladder-emptying methods, residual volume and frequency of anticholinergic and alpha blocker use (all P<0.05). The less number of the patients who were administered baclofen in our study population limited the comparison of the usage of this agent in the groups. No significant difference were found between the groups regarding the frequencies of AD, detrusor hypocompliancy and bladder-storage and -emptying disorders (all P>0.05).
We conducted Chi-square test, Fischer’s exact test and T-test for independent samples for comparisons of complete UCSCI and LCSCI patients and incomplete UCSCI and LCSCI patients. There was no statistically significant difference between the complete UCSCI (n=19) and complete LCSCI (n=31) patients with respect to residual volume and frequencies of AD, detrusor hypocompliancy, detrusor overactivity, bladder-storage and -emptying disorders and bladder-emptying methods (P>0.05). There was no statistically significant difference between incomplete UCSCI (n=32) and incomplete LCSCI (n=8) patients with respect to residual volume and frequencies of AD, detrusor hypocompliancy, detrusor overactivity, bladder-storage and -emptying disorders and bladder-emptying methods (P>0.05). Comparisons of bladder-filling sensation could not be conducted because of the very low expected counts in Chi-square test.
Discussion
The urinary system is one of the most important organ system that is involved in the SCI. Therefore, the urodynamic findings of the patients with cervical SCI were evaluated, and results were also significant by dividing the patients into two groups as UCSCI and LCSCI according to the neurogenic lesion levels in our study. Cases in the UCSCI and LCSCI groups were classified as complete (AIS-A) and incomplete (AIS B–E). In the UCSCI group, incomplete injured patients were significantly more than complete injured patients in our study. This significant difference may be explained by the higher mortality rates in complete UCSCI patients than in incomplete UCSCI patients.17
There was statistically significant difference in favor of the UCSCI group regarding bladder-filling sensation. This was attributed to the higher incomplete injury rate in the UCSCI group. The presence of bladder-filling sensation may be useful in the timing of bladder emptying.9 As the loss of bladder-filling sensation is frequent in the LCSCI group, we feel that strict and close follow-up for the bladder-emptying timing and volume is required in this patient group.
The frequency of detrusor overactivity was significantly high in the UCSCI group. It is difficult to explain the underlying mechanism. A possible explanation may be the significantly higher number of incomplete injured patients in the UCSCI group. Higher rate of spasticity and hypereflexia in the incomplete injury than in the complete injury has been reported previously.18 In the light of this phenomenon, it is possible to say that higher rate of hypereflexia in detrusor muscle in the patients with incomplete lesions in the UCSCI group may be the reason for this significant difference.
Statistically significant difference was determined between the two groups when the patients were evaluated in terms of bladder-emptying method. Additionally, there was statistically significant difference between the groups in favor of the UCSCI group when the patients were compared in terms of residual volume. In the scope of these statistical data, the UCSCI group, including higher number of incomplete injured patients than in the LCSCI group, was in better condition in terms of urinary-emptying function reserve due to the higher frequency of spontaneous voiding and emptying without catheter and lower residual urine volume than the LCSCI group. This finding may be useful while making decisions on medical treatment and clinical approaches for neurogenic bladder in cervical SCI patients.
When the patients were evaluated in terms of anticholinergic and alpha blocker usage, statistically significant difference was observed between the groups. Frequencies of spontaneous voiding and emptying without catheter were higher and mean residual volume was lower in the UCSCI group than in the LCSCI group. Thus, alpha blocker prescribed in order to support and enhance the preserved emptying function was more frequent in the UCSCI group. On the other hand, higher rate of complete injury in the patients in the LCSCI group led to severe storage and emptying dysfunction of bladder. It is crucial to improve the bladder capacity in these patients. The higher rate of anticholinergic use in the LCSCI group was probably due to the severity in decrease of both the urinary storage and emptying function reserve in our study. Baclofen, which has positive effect on bladder-emptying function by relaxing the external sphincter, is commonly used in SCI patients. However, the small number of the patients who were administered baclofen in our study population limited the comparison of the usage of this agent in the groups.
Self or third-party intermittent catheterization rates were not different statistically in the groups, although higher rate of intermittent self-catheterization was observed in the LSCSI group. Cardenas et al.19 reported that self-clean aseptic catheterization rate is higher in LCSCI patients than in UCSCI patients. The small number of patients in the subgroups and the higher rate of incomplete patients in the UCSCI group may be the reasons why there was no statistically significant difference between the two groups.
There was no statistically significant difference between the groups regarding AD rate during the urodynamic evaluations. However, AD symptom findings were determined in 55.6% of the patients. This rate indicates that proper precautions must be taken for the relevant patients.
Absence of statistical significant difference between complete UCSCI and complete LCSCI patients and between incomplete UCSCI and incomplete LCSCI patients with rescpect to residual volüme, the frequencies of AD, detrusor hypocompliancy, detrusor overactivity, bladder-storage and -emptying disorders and bladder-emptying methods gave the impression that the higher rate of incomplete patients in the UCSCI group may have had a major role in the statistically significant differences observed between UCSCI and LCSCI patients in general. However, patient numbers in the complete and incomplete UCSCI and LCSCI subgroups were small, and further studies with larger sample sizes are required. Nevertheless, statistically significant differences observed between UCSCI and LCSCI patients in general is a clinical reality and keeping this finding in mind may be helpful in daily practice.
The small patient numbers in the complete and incomplete UCSCI and LCSCI subgroups, absence of uniform sphincteric electromyographic monitoring and relatively high filling rates appeared as limitations of our study. In our study, continuous medium fill cystometry was performed at 50 ml min−1 for adults and at 20 ml min−1 for children. Although 50 ml min−1 is the upper limit for medium fill cystometry, it can provoke detrusor overactivity and AD in patients with cervical lesions, and the significances of the urodynamic findings may be unclear, so the results should be interpreted accordingly. As this is a retrospective study including a period of 10 years, presence of some methodological limitations could not be avoided. Despite these limitations, we feel that our study is informative about the neurogenic bladder characteristics and neurogenic bladder treatment approaches in patients with cervical SCI.
Conclusion
In conclusion, the findings of the study not only provide comprehensive information about the neurogenic bladder in patients with cervical SCI, but also show that there are differences in the upper and lower SCI cases in terms of neurogenic bladder characteristics and therapeutic approaches. Herein presenting our study, we would like to contribute to the clinical approaches for neurogenic bladder.
Data archiving
There were no data to deposit.
References
Sekhon LH, Fehlings MG . Epidemiology, demographics and pathophysiology of acute spinal cord injury. Spine 2001; 26 (24 Suppl.): S2–12.
Karacan I, Koyuncu H, Pekel Ö, Sümbüloğlu G, Kırnap M, Dursun H et al. Traumatic spinal cord injuries in Turkey: a nation-wide epidemiologic study. Spinal Cord 2000; 38: 697–701.
Lee YH, Creasey GH, Lim H, Song J, Song K, Kim J . Detrusor and blood pressure responses to dorsal penile nerve stimulation during hyperreflexic contraction of the bladder in patients with cervical cord injury. Arch Phys Med Rehabil 2003; 84: 136–140.
Morita H, Sazawa A, Kanno T, Keyanagi T . Long term urinary prognosis of cervical cord injury patients. Paraplegia 1994; 32: 30–35.
Kaplan SA, Chancellor MB, Blaivas JG . Bladder and sphincter behavior on patients with spinal cord lesions. J Urol 1991; 146: 113–117.
Ando M . Neurogenic bladder in patients with cervical cord compression disorders. Nihon Hinyokika Gakkai Zasshi 1990; 81: 243–250.
Wyndaele JJ . The normal pattern of perception of bladder filling during cystometry studied in 38 young healthy volunteers. J Urol 1998; 160: 479–481.
Wyndaele JJ, Wachter SD . Cystometrical sensory data from a normal population: comparison of two groups of young healthy volunteers examined with 5 years interval. Eur Urol 2002; 42: 34–38.
Ersöz M, Akyüz M . Bladder filling sensation in patients with spinal cord injury and the potential for sensation-dependent bladder emptying. Spinal Cord 2004; 42: 110–116.
Consortium For Spinal Cord Medicine, Clinical Practice Guidelines, August 2006.
Guidelines on Neurogenic Lower Urinary Tract Dysfunction. European Association of Urology 2012.
Ersöz M . Neurogenic bladder and bowel in pediatric spinal cord injury patients. Turk J Phys Med Rehab 2008; 2: 75–80.
Robertson AS, Griffiths CJ, Ramsden PD, Neal DE . Bladder function in healthy volunteers: ambulatory monitoring and conventional urodynamic studies. Br J Urol 1994; 73: 242–249.
Abdel-Rahman M, Coulombe A, Devroede G, Toppercer A, Duguay C, Lapointe L et al. Urorectodynamic evaluation of healthy volunteers. Urology 1982; 19: 559–564.
Dmochowski R . Cystometry. Urol Clin North Am 1996; 23: 243–252.
Ersöz M, Tunç H, Akyüz M, Özel S . Bladder storage and emptying disorder frequencies in hemorrhagic and ischemic stroke patients with bladder dysfunction. Cerebrovasc Dis 2005; 20: 395–399.
DeVivo MJ, Krause JS, Lammertse DP . Recent trends in mortality and causes of death among persons with spinal cord injury. Arch Phys Med Rehabil 1999; 80: 1411–1419.
Kirshblum S . Rehabilitation of SCI. In: DeLisa JA, Gans BM (eds). Physical Medicine and Rehabilitation, Principles and Practice 4th edn. Lippincott Williams & Wilkins: Philadelphia, PA, USA. 2005 pp 1715–1751.
Cardenas DD, Mayo ME . Management of bladder dysfunction. In: Braddom RL (ed.). Physical Medicine and Rehabilitation 4th edn. Saunders Elsevier: Philadelphia, PA, USA. 2010 pp 626.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Sayılır, S., Ersöz, M. & Yalçın, S. Comparison of urodynamic findings in patients with upper and lower cervical spinal cord injury. Spinal Cord 51, 780–783 (2013). https://doi.org/10.1038/sc.2013.83
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2013.83
Keywords
This article is cited by
-
Urodynamic findings and therapeutic approaches for neurogenic lower urinary tract dysfunction in patients with thoracic spinal cord injury
Irish Journal of Medical Science (1971 -) (2023)
-
Combining different evaluations of sensation to assess the afferent innervation of the lower urinary tract after SCI
Spinal Cord (2021)
-
Autonomic dysreflexia and repeatability of cardiovascular changes during same session repeat urodynamic investigation in women with spinal cord injury
World Journal of Urology (2016)
-
Iatrogenic urological triggers of autonomic dysreflexia: a systematic review
Spinal Cord (2015)
-
Urodynamic findings, bladder emptying methods and therapeutic approaches in patients with upper lumbar and lower lumbar–sacral spinal cord injury
Neurological Sciences (2015)
