
Abstract
Study design:
Retrospective cohort study.
Objective:
To describe the characteristics of patients with work-related traumatic spinal cord injuries (TSCI) in Chile.
Setting:
Hospital del Trabajador in Santiago, Santiago, Chile.
Methods:
Patients suffering from TSCI incurred at the workplace from 1986 to 2005 were identified through records of the Asociación Chilena de Seguridad (ACHS, Chilean Safety Association).
Results:
The medical records of 173 patients, 172 men and 1 woman, were analyzed. The yearly average incidence was 7.8 per million workers. Age at TSCI onset was 38.2±12.1 years. The principal external causes for TSCI incurred at the workplace were falls from a height in 86 cases (49.7%) and trauma blows to the vertebral spine in 61 cases (35.3 %). More falls occurred in the field construction, and other traumas occurred as a result of traumatic blows caused by tree trunks and stones in forestry and mining sectors. Mortality in this series was 8.7%, and the worst prognosis was for older patients with complete tetraplegia. The paraplegia:tetraplegia ratio was 3.2:1.
Conclusions:
The characteristics of workplace TSCI are specific to this population. It is important therefore to develop prevention programs for specific work-related TSCI.
Similar content being viewed by others

Introduction
Because of the major personal biopsychological impact and the serious short- and long-term socioeconomical consequences, a knowledge of the incidence and prevalence of spinal cord lesions is important.1
Although rare, SCI is one of the most devastating and debilitating lesions a person can suffer from; nevertheless, little has been published in the international medical literature about traumatic spinal cord injuries (TSCI) in the workplace.2, 3, 4, 5
Some studies mention that occupational causes account for 12–18% of the causes of TSCI.2, 3, 4, 6, 7, 8, 9 An Australian study showed that the incidence of TSCI in the workplace is as high as 4 per million workers.2
Studies on occupational TSCI that occur in a working situation describe a population with characteristics that are very different from that of the general population;2, 3, 4, 5, 9 men comprise about 95% of the cases. According to the study by Rosenberg et al.,4 the average age of presentation of TSCI in the workplace is 38.9 years, which is 5 years older than that of the general population. The occupations most affected by TSCI occurring at work are those in construction, services, agriculture and mining, with the most frequent external causes being falls from a height (36–50%), and injury to the vertebral spine caused by falling objects (18.9–24% of the cases).2, 3, 4, 5, 9 The most frequent type and level of TSCI in the workplace is complete paraplegia and the least frequent is complete tetraplegia; the reported paraplegia:tetraplegia ratio is 2.2/1.2
The purpose of this study is to describe the characteristics of patients with occupational TSCI in Chile, such as incidence, prevalence, age, gender, external causes, type and neurological level, and to identify those occupations most at risk so as to direct preventive measures in the workplace.
Materials and methods
The study was carried out at the Hospital del Trabajador in Santiago (HTS), Chile, a company of Asociación Chilena de Seguridad (ACHS), a private, nonprofit insurance company founded in 1958. Its function is to administer the law that governs workplace injuries and occupational diseases. ACHS is the largest insurance company in Chile, currently representing 25% of the active working population of the country, from 609 179 affiliated workers in 1986 to 1 617 835 in 2005.
The accidents insurance covers only TSCI—accidents at the workplace, as well as those incurred to and from work. All accidents are documented regarding the mechanism and site of occurrence, and each patient is assessed by a physician specialized in trauma before being entered into the ACHS database. It offers treatment and rehabilitation during the life of the patient and also financial compensation.
A retrospective cohort study of patients who suffered from TSCI at the workplace was carried out from 1986 to 2005; patients were covered by the law of workplace accidents and affiliated to ACHS.
For the purpose of this study, only patients who suffered accidents at the workplace and who were alive when they arrived at the hospital or ACHS care centers were analyzed (hospital incidence).
As this is a closed population with periodic and free care, there was no loss to follow-up.
The central computerized system of ACHS was consulted, as well as the records of admissions to intensive care, to the rehabilitation service of the HTS and certificates of disability and death. The database server DB2-400 from IBM, AS-400 was used to consult keywords such as ‘spine fracture or trauma (cervical, thoracic or lumbar) with neurological injury’, ‘paraplegia’, ‘tetraplegia’, ‘cauda equina syndrome’ in patients both alive and dead. ACHS coding is based, in general terms, on valid international classifications. By law, all patients who present with permanent injuries (sequelae) must be assessed for disability; all the disability registries of the study period were reviewed.
Demographic variables were analyzed, including age at the time of TSCI, gender and mortality.
Definition of variables
Traumatic spinal cord lesion, as defined by the Center for Disease Control of Atlanta, is the occurrence of an acute traumatic lesion of the neural elements in the spinal canal, the spinal cord and the cauda equina, resulting in a temporal or permanent sensitive, motor deficit or vesical/intestinal dysfunction.10 Completeness and level of SCI is defined according to the American Spinal Injury Association/International Spinal Cord Society scales.11 Hospital incidence rate is calculated as the number of workers who suffer from TSCI divided by the total work force affiliated to ACHS in the same year, calculated as the average between the total work force at the beginning and at the end of each year. The hospital incidence rate considers the workers who arrive at the hospital and does not include those who die at the place where the accident took place or those who die on the way to the care center. Prevalence rate is calculated as the number of workers who present with TSCI—including new cases and cases of previous years that survive TSCI, subtracting those who died during the year—divided by the total labor force affiliated to ACHS per year. Hospital mortality is calculated as the number of workers who died after reaching the hospital because of TSCI divided by the number of workers who suffered from TSCI between 1986 and 2005.
Description of variables or factors
The population studied in whom spinal cord lesions related to work occurredwas divided according to gender, age, place of residence, occupation causes to and from work.
The causes of TSCI are classified as falls from a height (for example, scaffolds, trees, posts or others) suffered by the subjects studied and injury by trauma blow, caused by objects and or people falling on the subjects.2
The occupations considered in this study include agriculture, construction, services, mining, manufacturing industry, transportation, commerce, electricity, gas, water and health services.
Statistics
TSCI patients were categorized by gender, age and year of the lesion. Cause, occupation, type and level of the lesion and the relationship between the fields of the different occupations and external cause of the lesion were considered.
The χ2-test was used for comparison between proportions; for comparison between the different means, Student's t-test was used. A statistical level of significance of 5% was used; all confidence intervals (CI) are expressed at 95%. The statistical package STATA 9.2 (StataCorp, College Station, TX, USA) was used in the data analysis.
Results
In this study, we analyzed the data of the 173 TSCI patients who suffered from accidents at the workplace between 1986 and 2005. The rate of average yearly incidence was 7.8±3.6 per million workers (minimum 3 per million in 1998 and maximum 17.5 in 1987) Figure 1.

Hospital incidence rate of TSCI at the workplace.
The prevalence rate was 112 cases per million active affiliated workers for 2005.
The distribution according to gender was 172 men (99.4%) and 1 woman who suffered from workplace accidents (including those who fell from a height while employed in agricultural work).
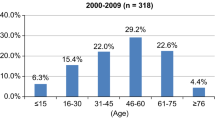
Age at the time of TSCI was 38.2±12.1 years. The most frequently affected age ranged from 25 to 34 years (28.4%; Figure 2).

Age distribution for TSCI at the workplace.
Place of residence: 90 patients (39.3%) lived in the metropolitan region of Santiago and the remaining 139 patients (60.7%) resided in regions distant from the capital.
The occupations most frequently seen in workplace accidents were in the industrial, agricultural and construction sectors (Table 1).
External causes of TSCI in the workplace were falls in 86 cases (49.7%), trauma blow to the vertebral spine in 61 cases (35.3%), traffic accidents in 15 cases (8.7%) and other causes in 11cases.
The age of patients who suffered falls and had TSCI was 40.1±12.8 years and the age of those who suffered TSCI because of trauma blow to the vertebral spine was 35.6±10.7 years, P<0.025.
When analyzing the different occupations and the external cause of accidents, we found that construction workers suffered a greater frequency of falls from a height (80.8%; P<0.005), whereas those who worked in forestry and mining suffered more traumas to the vertebral spine from falling tree trunks and stones (73.9 and 65.8%, respectively; P<0.01) (Figure 3).

Association between occupation and mechanism of TSCI at the workplace.
In all, 78 (45.1%) patients presented with complete paraplegia, 54 (31.2%) had incomplete paraplegia, 18 (10.4%) suffered from complete tetraplegia and 23 (13.3%) had incomplete tetraplegia. The paraplegia:tetraplegia relationship was 3.2:1. The neurological level and completeness of TSCI in the workplace in two decades is shown in Table 2.
During the 20 years of observation of the study, there were 15 deaths recorded because of TSCI in 173 patients (hospital mortality: 8.7%). Four patients died in the first month of the accident and the other 11 died later on in the chronic period. All the patients who died were men, age at TSCI was 50.9±11.6 years compared with 37.0±11.5 years for men who survived TSCI, P<0.0005. The most frequent type and level of lesion was complete tetraplegia in 40% of cases (6out of 15) compared with 7.6% of men surviving TSCI, P<0.001.
Discussion
In this study, we observed distinctive epidemiological characteristics in our population related to occupation.
The high predominance of men with TSCI in the workplace is very similar to that reported by the literature;2, 3, 4, 5, 9 this fact can be the result of a high percentage of men employed in industries with higher risks for TSCI in Chile. The average age of presentation of TSCI in our study is round about 38 years of age, similar to that reported by other previous studies.4, 5, 9
The two predominant external causes of TSCI occurring in the workplace are falls from a height and traumatic injuries and blows to the vertebral spine. We see that falls are the most prevalent cause and traumatic injurious blows to the spine are the second most prevalent cause; this observation is also comparable to the results of other studies.2, 4, 5, 9
Hospital mortality (8% of patients) is very similar to that reported by Ekong and Tator.3 An older age at the time of TSCI and the presence of tetraplegia are factors for worse prognosis for survival, a fact that must be kept in mind.
Occupations most frequently related to TSCI in the workplace vary in different studies; in our study, we saw a greater frequency of industrial and agricultural occupations. O'Connor found that agriculture had the greatest incidence,2 but Rosenberg et al.4 observed that these accidents were more prevalent in construction. In the ACHS, the manufacturing industry takes the second place in frequency of distribution, and agriculture holds the fifth place; in O'Connor's study, agriculture held the third place and industry held the fifth place.
When correlating the external causes of TSCI in the workplace, we saw a relationship between external cause and occupation or productive activity, with a greater frequency of falls in the construction sector, which was previously reported by Rosenberg et al.4
The type and level of TSCI we saw were very similar to those reported by O'Connor,2 having a high frequency of complete paraplegia and a low frequency of complete tetraplegia. The paraplegia:tetraplegia ratio in our series is greater than that reported and this may be because of the fact that we included all the TSCI including those with a favorable prognosis.
The incidence of work-related TSCI has remained stable in the last few years in our study, about 8 per million workers, and this is higher than that reported by O'Connor in Australia,2 who places it at around 4 per million workers.
Our study has limitations. It was difficult to obtain the information because we did not have ICD-9 or ICD-10. Our sample is not representative of the population of the whole of Chile per se, but only of what happens in the work force. The incidence rates presented are hospital incidences; we did not consider the patients who died at the site of the accident or before reaching an ACHS care center.
We consider that the value of our study is the assessment of a numerically important cohort in a period of 20 years that allows us to evaluate different demographical variables, including the analysis of survival and mortality. As our study population is a closed population, we managed to follow them up completely.
References
Wyndaele M, Wyndaele J-J . Incidence, prevalence and epidemiology of spinal cord injury: what learns a worldwide literature survey? Spinal Cord 2006; 44: 523–529.
O'Connor PJ . Work related spinal cord injury, Australia 1986-1997. Inj Prev 2001; 7: 29–34.
Ekong CE, Tator CH . Spinal cord injury in the work force. Can J Surg 1985; 28: 165–167.
Rosenberg NL, Gerhart K, Whiteneck G . Occupational spinal cord injury: demographic and etiologic differences from non-occupational injuries. Neurology 1993; 43: 1385–1388.
Webster B, Giunti G, Young A, Pransky G, Neasthurai S . Work-related tetraplegia: cause of injury and annual medical costs. Spinal Cord 2004; 42: 240–247.
Mazaira J, Labanda F, Romero M, García C, Ganbarruta C, Sanchez A et al. Epidemiología de la lesión medular y otros aspectos. Rehabilitación (Madr) 1998; 32: 365–372.
Exner G, Meinecke FW . Trends in the treatment of patients with spinal cord lesions seen within a period of 20 years in German centers. Spinal cord 1997; 35: 415–419.
Biering-Sorensen F, Pedersen V, Clausen S . Epidemiology of spinal cord lesions in Denmark. Paraplegia 1990; 28: 105–118.
Pagliacci MC, Celani MC, Zampolini M, Spizzichino L, Franceschini M, Baratta S, Gruppo Italiano Studio Epidemiologico Mielolesioni et al. An italian survey of traumatic spinal cord injury. The Gruppo Italiano Studio Epidemiologico Mielolesioni Study. Arch Phys Med Rehabil 2003; 84: 1266–1275.
Thurman DJ, Sniezek JE, Johnson D . Guidelines for surveillance of central nervous system injury. Atlanta. US Department of Health and Human Services. Centres for Disease Control and Prevention 1995.
Maynard FM, Bracken MB, Creasey G, Ditunno JF, Donovan WH, Ducker TB et al. International standards for neurological and functional classification of spinal cord injuries. Spinal Cord 1997; 35: 266–274.
Acknowledgements
We thank Dr Alejandra Sotomayor, Ignacio Barañao, Ruperto Correa, Cristián Llull, Amada Valenzuela, Teresa Jimenez; Dr Alonso Mujica, Chief of the Rehabilitation Service of HTS; and Dr Verónica Herrera, Health Director of ACHS. We especially thank Alicia Barra and Valeria Rojas, secretaries of the Rehabilitation Service of HTS.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Correa, G., Finkelstein, J., Burnier, L. et al. Work-related traumatic spinal cord lesions in Chile, a 20-year epidemiological analysis. Spinal Cord 49, 196–199 (2011). https://doi.org/10.1038/sc.2010.71
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2010.71
Keywords
This article is cited by
-
Demographic and clinical characteristics of individuals with traumatic spinal cord injury in Argentina from 2015 to 2019: a multicenter study
Spinal Cord Series and Cases (2020)
-
Two-year survival following discharge from hospital after spinal cord injury in Bangladesh
Spinal Cord (2016)
-
Incidence of traumatic spinal cord injury worldwide: a systematic review
European Spine Journal (2015)
