
Abstract
Precision oncology is described as the matching of the most accurate and effective treatments with the individual cancer patient. Identification of important gene mutations, such as BRCA1/2 that drive carcinogenesis, helped pave the way for precision diagnosis in cancer. Oncoproteins and their signaling pathways have been extensively studied, leading to the development of target-based precision therapies against several types of cancers. Although many challenges exist that could hinder the success of precision oncology, cutting-edge tools for precision diagnosis and precision therapy will assist in overcoming many of these difficulties. Based on the continued rapid progression of genomic analysis, drug development, and clinical trial design, precision oncology will ultimately become the standard of care in cancer therapeutics.
Similar content being viewed by others

Introduction
Improving efficacy, minimizing the adverse side effects of drugs, and overcoming acquired resistance to drug treatment have been major goals and emphases in cancer therapy. In order to attain the objectives of precision oncology, basic and clinical researchers have identified and clarified differences derived from genetic features between individuals. The existence of specific genetic differences between individuals is exemplified by the finding in 1932 that phenylthiocarbamide (PTC) exhibits the unusual property of either tasting very bitter or having no taste at all based on the individual’s genetics. Notably, this trait is inherited to the next generation.1, 2 The “one-size-fits-all strategy” is no longer relevant to cancer treatment. The tailoring of distinct treatments to each specific individual became known as “personalized medicine”3 and later the name was changed to “precision medicine”.4 Many countries have now launched government-driven projects focusing on precision medicine, including the Precision Medicine Initiative (National Institutes of Health, USA),4 Cancer Moonshot program5 (National Cancer Institute, USA) and HORIZON 2020 Work Program for 2016–2017 (EU).6
The accelerating momentum of precision medicine, and especially precision oncology, has stemmed from the increasing amount of “-omics” information acquired from patients and, importantly, the successful integration of the fields of basic and clinical cancer research. Next-generation sequencing instrumentation is capable of sequencing several genomes a day at a cost of about $1000 each, making this technology an essential and straightforward part of translational cancer research.7 Driver-gene mutations identified from comprehensive genome analyses are now frequently detected in many cancer patients,8 and the aberrant gene products are currently being targeted by specific antagonists or monoclonal antibodies.9 Oncologists are now able to stratify subsets of cancer and make informed therapeutic decisions. Consequently, targeted therapy has gained credibility in reinforcing and/or replacing conventional cytotoxic chemotherapy. Several targeted agents are presently approved by the FDA and are being used clinically against several types of cancer.
Here, we categorize the work flow of precision oncology into two segments, precision diagnosis and precision therapy, and provide milestones and important aspects characterizing each segment. By reviewing targeted therapies clinically approved against breast cancer, lung cancer and melanoma, we reveal the current status and expose possible challenges in precision oncology. Two of the most effective state-of-the-art tools for the success of precision oncology are also described.
Precision oncology for patients—from precision diagnosis to precision therapy
In order to better understand and utilize precision oncology (i.e., precision medicine as it applies to cancer), analyzing the procedures step by step is crucial. Precision oncology comprises precision diagnosis and precision therapy. Precision diagnosis begins with an accurate diagnosis of each individual cancer patient and ideally classifies subjects into cancer patients and individuals at high risk for specific cancers.10 By detecting biomarkers that are associated with specific cancer types such as BRCA1/2 mutations in breast cancer,11, 12 we can diagnose the current or potential risks of each individual. Accumulating evidence shows that multiple biomarkers (so called “signature”) can help in creating more precise and evidence-based therapeutic strategies to modulate cancer.13, 14 Establishing molecular subtypes and categorizing tumors into one of the subtypes enhances the accuracy of therapeutic options.15 The information derived from precision diagnosis reveals the precise medical measures, including surgery, radiation, chemotherapy, adjuvant therapy, supplements, and/or vaccines,16 that are needed for each individual.
Precision therapy matches the most effective treatment to the individual cancer patient based on the genetic profile of the specific cancer, and can be divided into two categories that include precision chemotherapy and precise therapeutic procedures. Precision chemotherapy is the use of the correct drugs prescribed that assures maximum benefit with minimum risk or toxicity for the patient. Therapeutic measures could include surgery and radiation therapy tailored to the patient’s needs.
Precision diagnosis
Information-based diagnosis can assist clinicians not only in identifying tumor type and stage, but also in revealing important genetic mutations that drive carcinogenesis. Advances in technology have clearly resulted in more effective therapeutic decisions. Final goals include optimization of clinical outcomes, avoidance of unnecessary therapies, minimized side effects, and overcoming or avoiding drug resistance.
BRCA1/2 are a milestone for precision diagnosis
The discovery of the breast cancer susceptibility genes, BRCA1/2, was traced from a family with a history of breast cancer, and indicated the association between genetic features and the early onset of the disease.11, 12 In addition to other breast cancer susceptibility genes, the BRCA1/2 mutation test is one of the most well-established models in precision oncology. It has become a guideline that aids clinicians in creating prevention strategies and targeted therapies. More than one million individuals have been tested for BRCA1/2 mutations worldwide.17
The landscape of mutations in the BRCA1/2 genes has been extensively studied and the relationship between the mutations and breast cancer risk is also well-defined. More than 1800 different variants (i.e., intronic changes, insertions, deletions and missense mutations) have been observed in BRCA1 and 2000 different variants have been reported to occur in BRCA2.17 BRCA1/2 mutations are currently the most significant gene variations in breast cancer surpassing tumor protein p53 (TP53), phosphatase and tensin homolog (PTEN), liver kinase B1 (LKB1), and cadherin1 (CDH1) mutations.17,18,19 BRCA1/2 mutations are estimated to account for ~15% of the relative familial risk of breast cancer.17 Mutations in BRCA1 and BRCA2 reportedly contribute equally to early-onset breast cancer.20
Development and improvement of genetic tests
Recent progress in immunohistochemistry (IHC) has helped clinicians to identify the presence of specific biomarkers and to categorize patients in pathology.21, 22 Detection of human epidermal growth factor receptor 2 (HER2)23 in breast cancer and PD-L124 in lung cancer based on IHC aided the prescription of suitable drugs for the patients. However, many other techniques are currently available to quantify changes in gene expression, and include reverse transcriptase-polymerase chain reaction,25 DNA arrays,26 NanoString technology,27 comparative genomic hybridization arrays, and single-nucleotide polymorphism analysis.28 Genetic tests have been developed for diagnostic, predictive and prognostic purposes and some have been approved by the FDA, whereas others are still under development for breast cancer,29,30,31,32,33,34,35,36,37 lung cancer,38,39,40,41,42,43,44 and melanoma45,46,47,48,49 (Table 1). Although the most significant genes, such as BRCA1/2, can only predict or explain a portion of disease susceptibility, the number of genes examined in a single test has continually increased to improve accuracy.14, 50 Of particular note (Table 1), the 70-gene signature test for breast cancer (MammaPrint by Agendia)29 showed the most efficacy in a clinical trial.51 The study in 6693 women with early-stage breast cancer was conducted to examine whether the gene signature test could reduce the use of chemotherapy. For patients who had high clinical risk and low genomic risk for recurrence, the difference in the 5-year survival rates between chemotherapy (98.8%) and no-chemotherapy (97.3%) was only 1.5%.51 The result shows that approximately 46% of women with breast cancer who are at high clinical risk might not require chemotherapy and that the 70-gene signature could aid in treatment decisions.51 The Oncotype Dx test by Genomic Health also helps clinicians in selecting proper treatment options for patients with invasive breast cancer.34, 52 The Oncotype Dx test generates a recurrence score (0–100) by analyzing the expression of 21 genes.53, 54 Survival rates of patients with high recurrence scores (31 and higher) have been improved by adjuvant chemotherapy, whereas patients with low recurrence scores (less than 17) are unlikely to get benefits from the chemotherapy.52
Precision therapy
Precision therapies have been applied in breast cancer, lung cancer and melanoma, but many challenges still need to be addressed.
Breast cancer and targeted therapy
The most well-known target-based treatment against breast cancer is directed at the estrogen receptor (ER) and the HER2 (Table 2).55 The discovery of these two protein receptors opened a new avenue for targeted therapy that showed improved efficacy compared to aromatase inhibitors, which suppress plasma estrogen levels in postmenopausal women.56 Tamoxifen, a pro-drug targeting the ER, is metabolized in the liver into active metabolites that have a higher affinity for the ER compared to the parental tamoxifen.57 Trastuzumab is a monoclonal antibody targeting HER2 and is used in patients with breast cancers overexpressing this receptor (Table 2).58, 59 Trastuzumab inhibits the activity of HER2, which forms heterodimers with other tyrosine kinase receptors (i.e., EGFR, HER3 and HER4) and promotes tumorigenesis.60 From a clinical trial of 469 women with metastatic breast cancer overexpressing HER2, combinational treatment with trastuzumab and standard chemotherapy attenuated disease progression compared to standard chemoptherapy alone (i.e., median, 4.6 vs. 7.4 months).61 The objective response rate (i.e., 32 vs. 50%) and survival time (i.e., median, 20.3 vs. 25.1 months) were also improved by the addition of trastuzumab to the chemotherapy.61 A combination of pertuzumab, trastuzumab, and chemotherapy (i.e., docetaxel) improved the median overall survival time (i.e., 40.8 vs. 56.5 months) compared to trastuzumab-only plus chemotherapy.62 A conjugate drug of a HER2 monoclonal antibody and a cytotoxic drug, ado-trastuzumab emtansine, prolonged progression-free survival and overall survival with lower adverse effects compared with a combination of lapatinib and chemotherapy (Table 2).63
Challenges of targeted breast cancer therapies
The identification of driver genes in breast cancer increases the likelihood of matching the correct, most effective drug to the right patient. Only a few genes, however, have been validated to act as driver genes. BRCA1/2, estrogen receptor alpha (ESR1), HER2, PI3-K/Akt/mTOR, Egfr, cyclin dependent kinase 4 (CDK4)/Rb, Ras/Raf/mitogen-activated protein kinase (MEK) are known to be critical in breast cancer therapy (Table 2).64, 65 For instance, somatic mutations of PI3-K occur in more than 10% of all breast cancers65 and Akt1 and Akt3 mutations and PTEN deletion contribute to the activation of the PI3-K pathway.28, 66 Nevertheless, approximately 50% of the familial relative risk (the ratio of the risk of disease for a relative of an affected individual to that for the general population) of breast cancer is still unexplained.17 Couch et al. estimated that contributions of genes including BRCA1/2, TP53, PTEN, LKB1, CDH1, and known/predicted single-nucleotide polymorphisms in breast cancer, and the current knowledge of genetic variations, only covered half of the breast cancer risk.17
Variants of uncertain significance (VUS) add another layer of complication in breast cancer treatment. VUS refers to changes in a normal gene sequence for which the clinical association with disease is unclear.67 Although many efforts have been made to evaluate and classify genetic variants, including missense, intronic, and small in-frame insertions and deletions,68,69,70 the rarity of the individual VUS makes interpretation difficult because of insufficient statistical power.
Furthermore, some breast cancer patients lack good target proteins for therapy. Triple-negative breast cancer (TNBC), for example, is negative for ER and progesterone receptor (PgR) and lacks HER2 amplification and therefore cannot be treated with classic endocrine therapy or HER2-targeted therapy.71, 72 The loss of HER2 expression in metastatic tumors compared with HER2-amplified primary breast cancers is frequently observed, and ER-positive/PgR-positive/HER2-amplified tumors become TNBC after chemotherapy.55, 73, 74 Although alternative molecular targets, such as EGFR, which is frequently amplified and is related to poor prognosis,75, 76 are being elucidated (Table 2), TNBC has only a small number of therapeutic options, and remains a difficult type of cancer in the field of breast cancer therapy.77
Lung cancer and targeted therapies
FDA approval of gefitinib, an epidermal growth factor receptor (EGFR) inhibitor,78 accelerated target-based therapy in lung cancer patients replacing cytotoxic chemotherapy for first-line therapy.79, 80 For patients with EGFR-activating mutations (exon19del or L858R), erlotinib81, 82 also performed better than conventional chemotherapies, such as cisplatin. EGFR-targeted therapy was combined with cytotoxic drugs as a combination therapy that showed improved progression-free survival.83, 84 However, almost all patients treated with the EGFR inhibitors acquired resistance to the drugs due to secondary EGFR mutations such as T790M.85, 86 Second-generation EGFR inhibitors (e.g., afatinib87, 88) were designed to target mutant EGFR better than the wild-type receptor. Third-generation EGFR inhibitors, including osimertinib and olmutinib, irreversibly bind to EGFR T790M and have been approved for use in the U.S. and South Korea, respectively (Table 3).89,90,91
Crizotinib is an FDA-approved inhibitor of anaplastic lymphoma kinase (ALK), Ros proto-oncogene 1 (ROS1), and Met proto-oncogene (MET; Table 3). ALK is a cell surface protein that stimulates signaling pathways, such as the Ras/Raf/MEK, PI3-K/mTOR, and Janus kinase (JAK)/signal transducer and activator of transcription (STAT) pathways,92 and is activated by gene translocation and fusion with other genes.93,94,95,96,97,98 ROS1 is an orphan receptor tyrosine kinse (RTK) activated by chromosomal rearrangement and fusion with other genes.99 MET, another type of RTK, is overexpressed/amplified or exhibits an exon 14 skip-mutation in non-small-cell lung cancer (NSCLC) patients.100 Crizotinib has shown its superiority over standard chemotherapy in ALK-positive lung cancer patients101, 102 and ROS1-rearranged NSCLC patients.103 Lung adenocarcinoma patients harboring the MET exon 14 splice site mutation also responded to crizotinib.104 However, ALK mutations, such as R1174L, L1196M, and R1275Q, conferred resistance to crizotinib and led to the development of second-generation ALK inhibitors. FDA has approved the use of ceritinib,105 which targets the L1196M gatekeeper mutation, and alectinib,106 which targets the R1174L, L1196M, and R1275Q mutations.
BRAF is a signaling protein activated by various RTKs. In NSCLC, 2–4% of patients possess BRAF V600 mutations.100 Although BRAF inhibitors (vemurafenib and dabrafenib) were originally developed for the treatment of melanoma, recent clinical trials with the inhibitors showed potential in BRAF V600 mutant NSCLC patients (Table 3). Vemurafenib resulted in tumor regression in the majority (14 of 19) of NSCLC patients, and the objective response rate was 42%.107 In a phase 2 trial, dabrafenib treatment with trametinib, a MEK inhibitor, reached 63% overall response in BRAF V600E-mutant NSCLC patients, who had documented tumor progression after previous platinum-based chemotherapy.108
Immunotherapy has received substantial attention recently as a cancer therapy. Unlike other therapies, the goal of immunotherapy is to boost or restore the ability of immune cells to kill tumor cells.109 Tumor cells suppress and evade the immune system through interactions between the programmed cell death protein 1 (PD-1) of T-cells and the PD ligand 1 (PD-L1) of tumor cells.110 Two monoclonal antibodies against PD-1 (Table 3), including nivolumab111,112,113,114 and pembrolizumab,115, 116 have received FDA approval for second-line treatment against NSCLC that express PD-L1.
Challenges of targeted lung cancer therapies
The war against drug resistance is probably the most difficult challenge in lung cancer treatment. Clonal evolution, the accumulation of genetic and epigenetic changes over time in individual cells,117, 118 is now believed to be the root of drug resistance.119, 120 Biopsies that were taken after the failure of rociletinib targeting EGFR mutant (T790M)-expressing lung cancer121 showed that at least a portion of the resistant tumor still expressed the T790-wild-type protein.120 The wild-type clones existed before treatment with rociletinib. Piotrowska et al. concluded that combination treatment using rociletinib targeting mutant EGFR T790M clones and other drugs targeting wild-type EGFR T790 are required to further improve the drug response rate and final outcomes.120 However, when first-generation EGFR inhibitors (gefitinib and erlotinib) and third-generation EGFR inhibitors (rociletinib/CO-1686, osimertinib/AZD9291, olmutinib/HM61713 and WZ4002) were used in combination, a new mutation of C797S emerged and complicated the therapeutic options.122 Studies showed that if the C797S mutation was on a different allele of T790M, combination treatment with gefitinib and WZ4002 inhibited EGFR signaling. In contrast, if C797S and T790M were on the same EGFR allele, the combination of gefitinib and WZ4002 was not effective.122 Monitoring changes in cancer cells at the molecular level will be helpful in preventing and resolving drug resistance in lung cancer.
Melanoma and targeted therapies
BRAF in the mitogen-activated protein kinase (MAPK) pathway (Ras-Raf-MEK-ERK) is constitutively activated by mutations in 40% of melanomas.123 The most common mutations are V600E and V600K, representing 73 and 19%, respectively.124 The growth of BRAF V600E-expressing melanoma can be inhibited directly by vemurafenib125 or dabrafenib (Table 4).126 Drug resistance, also called “bypass tracks”, is increasingly relevant as targeted therapy emerges.127 Patients with BRAF mutations acquired resistance due to increased expression and phosphorylation of platelet-derived growth factor receptor beta (PDGFβ) and N-Ras.128 The MEK inhibitor, trametinib, also suppresses BRAF V600E-expressing or V600K-expressing melanomas by targeting the BRAF downstream MAPK pathway (Table 4).129 Because drug monotherapies commonly result in resistance,128, 130 combination treatment with a BRAF inhibitor and a MEK inhibitor has been prescribed to increase the patient’s response rate and also lengthen their survival time.131 Especially, combination therapy as a first-line approach increased overall survival rates in a clinical trial.132 In patients with BRAF V600 mutations, a combination of cobimetinib (MEK inhibitor) and vemurafenib treatment showed median overall survival of 22.3 months, compared with 17.4 months by placebo and vemurafenib treatment.132
Melanoma cells express the CTLA-4 and PD-1 immune receptor proteins that are normally expressed in T-cells. Because each of these two proteins can inhibit activation of T-cells and down-regulate the immune response, the abnormal expression of CTLA-4 and PD-1 in tumor cells is suggested as a molecular mechanism of immune evasion in tumors.133 Ipilimumab, a CTLA-4 monoclonal antibody, was approved by the FDA for treatment of patients with metastatic melanoma (Table 4).134, 135 The PD-1 monoclonal antibodies, nivolumab136,137,138 and pembrolizumab,139 were also effective against metastatic melanoma (Table 4). Ipilimumab and nivolumab are also used in combination to treat melanoma.140
Challenges of targeted melanoma therapies
Similar to other types of cancer, one of the greatest challenges in melanoma treatment is the relapse and development of resistant disease after therapy. Recently, even patients who have undergone immunotherapy were shown to acquire resistance to PD-1 blockade in melanoma.141 Zaretsky et al. reported a delayed relapse of patients who had had initial tumor regression induced by continuous pembrolizumab treatment. The analyses of biopsies showed that JAK1/2 truncating mutations resulted in loss of PD-L1 expression and changed the molecular profile of the melanoma.141, 142 Overall, although immunotherapy has become a promising and unique strategy for cancer treatment, an integrative strategy should be prepared to prevent drug resistance.
Tools for precision oncology
The demand for new diagnostic and treatment tools has been driven by precision oncology. In particular, the use of liquid biopsies and patient-derived xenograft (PDX) models has received considerable attention from researchers and clinicians. For precision diagnosis, having new diagnostic platforms like liquid biopsies is crucial because this type of assay can gather information from patients in a manner that is minimally invasive. For precision therapy, testing drugs in a paradigm like the PDX model is beneficial because this model can be used to represent tumors of patients before drugs are prescribed.
Liquid biopsies
A biopsy is an examination of tissue obtained from a living body to discover the presence, cause, or extent of a disease. Although biopsies have become more important as the field of precision oncology continues to expand, sampling some types of tumors is still difficult and can result in diagnostic errors. To address this problem, biofluid samples, including serum, plasma, saliva, urine, and cerebrospinal fluid, are now being used to screen for tumors, characterize molecular features, and analyze tumor types.143,144,145,146 Liquid biopsies can provide clear information regarding the genetic makeup of each tumor. Because liquid biopsies are relatively non-invasive, clinicians can repeat sampling and monitor disease progression over time without performing solid-tissue biopsies. Circulating tumor cells (CTCs) and cell-free DNA (cfDNA) are promising components of liquid biopsies.
CTCs are cancer cells that are shed into the vascular system from the primary tumor and are circulating around the body in the blood.147 CTCs have been detected in patients with metastatic tumors at an average concentration of 1–10 cells/ml, but are extremely rare in individuals without tumors or with non-malignant tumors.143, 148,149,150 Circulating non-tumor epithelial cells in the blood of patients undergoing surgery and the difficulty in identifying markers of CTCs pose challenges to this technology. However, because dynamic changes occur in surface markers of CTCs, analysis of DNA/RNA from CTCs can enable clinicians to predict tumor progression and drug susceptibility of the patient.146, 151,152,153,154 A clinical trial with CTCs showed its promise as a prognostic marker and limitation as an indicator of changing chemotherapy.155 The trial divided patients with metastatic breast cancer into four groups. Patients whose CTC number was not increased at baseline remained on initial therapy (arm A), and patients whose CTC numbers had been increased, but later decreased after 21 days of therapy, also remained on the initial therapy (arm B). Patients whose CTC numbers were consistently increased were randomly assigned to maintain initial therapy (arm C1) or changed to an alternative therapy (arm C2). Overall survival rates between arms A, B, and C (sum of C1 and C2) showed significant differences between groups (i.e., 35 vs. 23 vs. 13 months, respectively). However, no difference was observed between the overall survival rates of arms C1 and C2. This result indicates that CTC is a strong prognostic marker of overall survival in patients with metastatic breast cancer, although changing chemotherapy options based on CTC does not prolong the overall survival rate.155 In summary, monitoring the efficacy of adjuvant therapies is feasible with CTC-based liquid biopsies, analyses of CTCs will be one of the key players in precision diagnosis.
cfDNA refers to tumor DNA released from primary cancers into the biofluids of cancer patients.146 The majority of cfDNA is derived from cells that have undergone apoptosis or necrosis and then release fragments of DNA of approximately 150–180 bp in length.144, 146 Similar to acquiring CTC, tumor cell-derived cfDNA is difficult to obtain because of the extensive amount of cfDNA that is also released from non-malignant cells.156 Nevertheless, cfDNA could provide a better diagnostic tool than CTCs from the same patient to detect mutations.157 Because cfDNA could be used to monitor clonal evolution and emergence of drug resistance,158 this type of analysis might assist clinicians in making tailored therapeutic decisions for cancer patients in the future.
PDX models
The PDX model uses actual patient tumor fragments that have been sectioned from the cancer patient and implanted into immunodeficient mice.159 By treating mice harboring the PDX tumor fragment, the efficacy of a drug can be predicted before being prescribed to the actual patient. Thus PDX is a platform that provides evidence-based guidelines in choosing the correct and most effective drug to prescribe to a patient. For preclinical drug development, the PDX model overcomes the important limitation of using conventional cancer cell lines, which have developed characteristics that do not accurately reflect the actual cancer patient tumor. Conventional cell line-based xenografts lack the broad diversity and heterogeneity of cancer.160 In contrast, the PDX model preserves the heterogeneity and microenvironment of the original tumor after being passaged in mice.159, 160 In 1985 the PDX model was confirmed to have good predictive value in showing that drug responses from PDX models corresponded very well with the response from patients.161 The tumor heterogeneity of the PDX was shown to be well preserved in patient-derived tumor cells (PDTC).162 These results support the potential of the PDTC-PDX pipeline for drug development. Although the lack of functional immune reactions in this model is a limitation, humanized mice that mimic the human immune system and resultant microenvironment allow researchers to better understand translational oncology.163 Overall, this clinically relevant mouse model should be beneficial in drug development and precision therapy for cancer patients.
Establishing PDX models worldwide reflects the high expectations of translating preclinical research to the clinic. Novartis, a large pharmaceutical company (Switzerland), has established about 1000 PDX models expressing a diverse pool of driver mutations in cancer.164 EurOPDX, a European consortium for PDX, has established more than 1500 subcutaneous and orthotopic PDX models165 and the Jackson Laboratory (ME, USA) has created about 550 PDX models.165 The US–China (Henan) Hormel Cancer Institute (Zhengzhou, China) has established unique PDX models that include Wilms’ tumor and esophageal cancer models. Dana-Farber Cancer Institute (MA, USA) established a Public Repository of Xenografts (PRoXe), which includes PDXs of leukemia and lymphoma.166 Of particular note, EurOPDX launched cBioPortal, where information on models and their molecular annotation have been opened to the public to provide a platform of PDX studies.167
Limitations and prospects of precision oncology
Despite the growing enthusiasm and enormous investment in precision oncology, empirical evidence and verification is still critically needed showing that precision therapy is significantly better than conventional treatments.168, 169 Results from one of the first clinical trials based on precision oncology were not promising.170 In this trial, the genomic information of patients was analyzed and patients who had targetable driver mutations were subjected to precision therapy. Unfortunately, the use of molecular-targeted drugs did not result in improved progression-free survival compared to treatments based on the clinicians’ choice (i.e., randomized trial). Another study that enrolled patients with different types of tumors, including colon, thyroid and ovarian cancer expressing the BRAF V600 mutation, showed similar results.107 In this study, vemurafenib, an FDA-approved drug against melanoma, was only effective in some of the non-melanoma patients. These results suggest that prescription of drugs against a certain type of cancer does not guarantee success in treatment of other types of cancers although they harbor the same mutation/alteration on the target protein.
Several factors could have led to the lack of success of the current precision oncology-based trials.171 One factor could be the lack of specific molecular-targeted drugs. Drugs are not yet available for many drivers in carcinogenesis at least partly due to the tremendous cost in money and time. Furthermore, many drugs are so toxic that clinicians are forced to reduce the dose, which results in only a partial inhibition of the targeted pathway giving the tumor the opportunity to develop resistance to the drugs. Other factors include tumor heterogeneity and constant evolution.119, 172,173,174 In addition, the genomic signature from one part of the tumor measured at a certain time point likely does not represent other parts or different time points of tumor development. These features pose a huge hurdle to precision oncology.
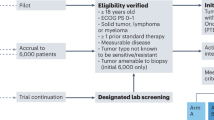
To address tumor heterogeneity and evolution, the National Cancer Institute recently revealed a new trial design of genomically informed precision therapy, referred to as the NCI-MATCH (Molecular Analysis for Therapy Choice) Trial.175, 176 NCI-MATCH aims to identify ‘actionable mutations’ and test whether a drug or drug combinations are active against specific molecular abnormalities.176 The multi-arm phase 2 trial initially aimed to screen 3000 patients and enroll 1000 adults with advanced solid tumors for which standard therapy has not yet been developed. The initial trial with 10 treatment arms has completed accrual and patient recruitment was closed in November 2015 for planned interim analysis. Based on the low number of actionable mutations and the enrollment number exceeding expectations from the interim analysis, the trial reopened on May 31, 2016, extending treatment arms to 24 and aiming to screen 6000 patients.177 Genetic variants of the patients will be analyzed for 143 genes and the patients assigned to one of several different treatment groups.175 The hope is that this new design will increase the flexibility of clinical decisions and improve the overall outcome of the patients.
One of the most promising and successful examples of precision oncology is the treatment of chronic myeloid leukemia (CML) with imatinib.10 The high proportion of the clonal BCR–ABL translocation in CML enabled almost all CML patients to benefit from imatinib.178 Likewise, finding concurrent driver mutations or clonal markers will benefit a large group of people. The hope is that predicting/monitoring changes in cells and dividing patients with subgroups before or at the point of cancer relapse will improve clinical outcomes.
Pan-cancer precision diagnosis and therapy are emerging. For instance, pembrolizumab, a PD-1 inhibitor, is approved by the FDA for treatment of metastatic melanoma,179 metastatic NSCLC,180 Hodgkin’s lymphoma,181 and metastatic head and neck squamous cell carcinomas.182 Although the proportion of patients who are eligible for the treatment is lower than that of imatinib-CML cases, this target-based approach provided a better treatment option compared to adjuvant chemotherapy. Furthermore, RTK inhibitors also aim to cover patients across various cancer types. One of the newest approaches is a fibroblast growth factor receptor (FGFR) inhibitor that directly targets its genetic alterations. BGJ398, a FGFR1-3 inhibitor, was tested in patients with advanced solid tumors including lung, breast, bladder, colon, and liver.183 The phase 1 trial showed that BGJ398 exhibits anti-tumor activity against FGFR1-amplified NSCLC and FGFR3-mutant bladder cancer.183 For precision diagnosis, eligible patients for targeted therapies will be screened and for precision therapy, the targeted drug(s) will be administered at a correct dose to benefit each individual.
The advances in lipidomics, proteomics, and metabolomics will aid in the implementation of precision oncology. In the field of lipidomics, arachidonic acid is a signaling precursor that has attracted interest for anti-cancer therapy.184, 185 A recent study of lipidomic profiling showed that lung tumors possess higher levels of arachidonic acid-containing phospholipids and phosphatidylinositols compared to normal tissue.185 Myc inactivation caused a significant decrease in arachidonic acid and its lipid metabolites.185 These results suggest that arachinonic acid and its metabolites can serve as biomarkers in precision diagnosis. In the field of proteomics, cryo-electron microscopy (cryo-EM) has received considerable attention as a tool for “visual proteomics”.10, 186 For example, the structure of the ATP-binding cassette subfamily G2 (ABCG2), a human multidrug transporter, revealed that two cholesterol molecules are bound to a hydrophobic pocket between the transmembrane domains.187 The cryo-EM structure provides structural insights of cholesterol recognition and pharmacokinetics of ABCG2 in precision therapy. In the field of metabolomics, gut microbiota possess a large repertoire of metabolizing xenobiotics, small molecules that are foreign to the human body.188 For example, irinotecan becomes SN-38, an active topoisomerase inhibitor in the body.189 SN-38 is glucuronidated by host liver enzymes and loses its activity (SN-38G). However, bacterial β-glucuronidase hydrolyzes and reactivates SN-38G in the large intestine, causing intestinal damage and diarrhea.189 Accumulative knowledge of microbiota in each patient could enhance the efficacy of precision therapy and lower adverse side effects.
To summarize, precision oncology has emerged to improve efficacy, minimize side effects of drugs and avoid drug resistance in cancer therapy. Precision oncology is categorized into two segments, precision diagnosis and precision therapy. In precision diagnosis, mutations of important genes such as BRCA1/2 have led clinicians to tailor treatment options to individuals. Improvement on genetic tests facilitated molecular target-based precision therapy. In breast cancer, lung cancer, and melanoma, drugs that inhibit important target proteins prolonged progression-free survival and overall survival of the patients compared to genotoxic chemotherapy. Although difficulties due to clonal evolution and cancer heterogeneity still exist, state-of-the-art tools such as liquid biopsies and PDX models will enhance the efficacy of precision diagnosis and precision therapy, respectively. Supported by government-driven projects worldwide, precision oncology will be the standard pipeline of cancer therapy.
References
Fox, A. L. The relationship between chemical constitution and taste. Proc. Natl. Acad. Sci. USA 18, 115–120 (1932).
Dance, A. Medical histories. Nature 537, S52–53 (2016).
Hamburg, M. A. & Collins, F. S. The path to personalized medicine. N. Engl. J. Med. 363, 301–304 (2010).
Collins, F. S. & Varmus, H. A new initiative on precision medicine. N. Engl. J. Med. 372, 793–795 (2015).
Aelion, C. M. et al. The US Cancer Moonshot initiative. Lancet Oncol. 17, e178–180 (2016).
Janda, M. & Soyer, P. Greater precision in melanoma prevention. JAMA Dermatol. 153, 18–19 (2016).
Scott, A. R. Technology: read the instructions. Nature 537, S54–56 (2016).
Zhang, W. et al. Network-based machine learning and graph theory algorithms for precision oncology. npj Precision Oncology. doi:10.1038/s41698-017-0029-7 (2017).
Bode, A. M. & Dong, Z. Precision oncology-the future of personalized cancer medicine? npj Precision Oncology. doi:10.1038/s41698-017-0010-5 (2017).
Shin, S. H., Bode, A. M. & Dong, Z. Precision medicine: the foundation of future cancer therapeutics. npj Precision Oncology. doi:10.1038/s41698-017-0016-z (2017).
Miki, Y. et al. A strong candidate for the breast and ovarian cancer susceptibility gene BRCA1. Science 266, 66–71 (1994).
Wooster, R. et al. Identification of the breast cancer susceptibility gene BRCA2. Nature 378, 789–792 (1995).
Friedman, A. A., Letai, A., Fisher, D. E. & Flaherty, K. T. Precision medicine for cancer with next-generation functional diagnostics. Nat. Rev. Cancer 15, 747–756 (2015).
Borrebaeck, C. A. Precision diagnostics: moving towards protein biomarker signatures of clinical utility in cancer. Nat. Rev. Cancer 17, 199–204 (2017).
Dienstmann, R. et al. Consensus molecular subtypes and the evolution of precision medicine in colorectal cancer. Nat. Rev. Cancer 17, 79–92 (2017).
Cao, Y. EBV based cancer prevention and therapy in nasopharyngeal carcinoma. npj Precision Oncology. doi:10.1038/s41698-017-0018-x (2017)
Couch, F. J., Nathanson, K. L. & Offit, K. Two decades after BRCA: setting paradigms in personalized cancer care and prevention. Science 343, 1466–1470 (2014).
Michailidou, K. et al. Large-scale genotyping identifies 41 new loci associated with breast cancer risk. Nat. Genet. 45, 353–361 (2013). 361e351–361e352.
Bahcall, O. G. iCOGS collection provides a collaborative model. Foreword. Nat. Genet. 45, 343 (2013).
Peto, J. et al. Prevalence of BRCA1 and BRCA2 gene mutations in patients with early-onset breast cancer. J. Natl. Cancer Inst. 91, 943–949 (1999).
Osin, P. P. & Lakhani, S. R. The pathology of familial breast cancer: Immunohistochemistry and molecular analysis. Breast Cancer Res. 1, 36–40 (1999).
Djuric, U. et al. Precision histology: how deep learning is poised to revitalize histomorphology for personalized cancer care. npj Precision Oncology. doi:10.1038/s41698-017-0022-1 (2017).
Moelans, C. B. et al. Validation of a fully automated HER2 staining kit in breast cancer. Cell. Oncol. 32, 149–155 (2010).
Rangachari, D. et al. Correlation between classic driver oncogene mutations in EGFR, ALK, or ROS1 and 22C3-PD-L1 > / = 50% Expression in lung adenocarcinoma. J. Thorac. Oncol. 12, 878–883 (2017).
Paik, S. et al. A multigene assay to predict recurrence of tamoxifen-treated, node-negative breast cancer. N. Engl. J. Med. 351, 2817–2826 (2004).
van de Vijver, M. J. et al. A gene-expression signature as a predictor of survival in breast cancer. N. Engl. J. Med. 347, 1999–2009 (2002).
Sorlie, T. et al. Repeated observation of breast tumor subtypes in independent gene expression data sets. Proc. Natl. Acad. Sci. USA 100, 8418–8423 (2003).
Andre, F. et al. Comparative genomic hybridisation array and DNA sequencing to direct treatment of metastatic breast cancer: a multicentre, prospective trial (SAFIR01/UNICANCER). Lancet Oncol. 15, 267–274 (2014).
Glas, A. M. et al. Converting a breast cancer microarray signature into a high-throughput diagnostic test. BMC Genom. 7, 278 (2006).
Blumencranz, P. et al. Scientific Impact Recognition Award. Sentinel node staging for breast cancer: intraoperative molecular pathology overcomes conventional histologic sampling errors. Am. J. Surg. 194, 426–432 (2007).
Foged, N. T., Brugmann, A. & Jorgensen, J. T. The HER2 CISH pharmDx(TM) Kit in the assessment of breast cancer patients for anti-HER2 treatment. Expert Rev. Mol. Diagn. 13, 233–242 (2013).
Lim, S. J., Cantillep, A. & Carpenter, P. M. Validation and workflow optimization of human epidermal growth factor receptor 2 testing using INFORM HER2 dual-color in situ hybridization. Hum. Pathol. 44, 2590–2596 (2013).
Nielsen, T. et al. Analytical validation of the PAM50-based prosigna breast cancer prognostic gene signature assay and ncounter analysis system using formalin-fixed paraffin-embedded breast tumor specimens. BMC Cancer 14, 177 (2014).
Cobleigh, M. A. et al. Tumor gene expression and prognosis in breast cancer patients with 10 or more positive lymph nodes. Clin. Cancer Res. 11, 8623–8631 (2005).
Filipits, M. et al. A new molecular predictor of distant recurrence in ER-positive, HER2-negative breast cancer adds independent information to conventional clinical risk factors. Clin. Cancer Res. 17, 6012–6020 (2011).
Zhang, Y. et al. Breast cancer index identifies early-stage estrogen receptor-positive breast cancer patients at risk for early- and late-distant recurrence. Clin. Cancer Res. 19, 4196–4205 (2013).
Harms, W. et al. Clinical significance of urokinase-type plasminogen activator (uPA) and its type-1 inhibitor (PAI-1) for metastatic sentinel lymph node involvement in breast cancer. Anticancer Res. 34, 4457–4462 (2014).
Kimura, H. et al. Analytical performance of the cobas EGFR mutation assay for Japanese non-small-cell lung cancer. Lung Cancer 83, 329–333 (2014).
Malik, S. M. et al. U.S. food and drug administration approval: crizotinib for treatment of advanced or metastatic non-small cell lung cancer that is anaplastic lymphoma kinase positive. Clin. Cancer Res. 20, 2029–2034 (2014).
Vallee, A., Le Loupp, A. G. & Denis, M. G. Efficiency of the Therascreen(R) RGQ PCR kit for the detection of EGFR mutations in non-small cell lung carcinomas. Clin. Chim. Acta 429, 8–11 (2014).
Conde, E., Hernandez, S., Prieto, M., Martinez, R. & Lopez-Rios, F. Profile of Ventana ALK (D5F3) companion diagnostic assay for non-small-cell lung carcinomas. Expert Rev. Mol. Diagn. 16, 707–713 (2016).
Sanders, H. et al. Mutation yield of a 34-gene solid tumor panel in community-based tumor samples. Mol. Diagn. Ther. 20, 241–253 (2016).
Abel, H. J. et al. Detection of gene rearrangements in targeted clinical next-generation sequencing. J. Mol. Diagn. 16, 405–417 (2014).
Di Cristofaro, J., Silvy, M., Chiaroni, J. & Bailly, P. Single PCR multiplex SNaPshot reaction for detection of eleven blood group nucleotide polymorphisms: optimization, validation, and one year of routine clinical use. J. Mol. Diagn. 12, 453–460 (2010).
Halait, H. et al. Analytical performance of a real-time PCR-based assay for V600 mutations in the BRAF gene, used as the companion diagnostic test for the novel BRAF inhibitor vemurafenib in metastatic melanoma. Diagn. Mol. Pathol. 21, 1–8 (2012).
Marchant, J., Mange, A., Larrieux, M., Costes, V. & Solassol, J. Comparative evaluation of the new FDA approved THxID-BRAF test with High Resolution Melting and Sanger sequencing. BMC Cancer 14, 519 (2014).
Sivendran, S. et al. Dissection of immune gene networks in primary melanoma tumors critical for antitumor surveillance of patients with stage II-III resectable disease. J. Invest. Dermatol. 134, 2202–2211 (2014).
Minca, E. C. et al. Comparison between melanoma gene expression score and fluorescence in situ hybridization for the classification of melanocytic lesions. Mod. Pathol. 29, 832–843 (2016).
Chan, M., Lee, C. W. & Wu, M. Integrating next-generation sequencing into clinical cancer diagnostics. Expert Rev. Mol. Diagn. 13, 647–650 (2013).
Lyons, Y. A. et al. Immune cell profiling in cancer: molecular approaches to cell-specific identification. npj Precision Oncology. doi:10.1038/s41698-017-0031-0 (2017).
Cardoso, F. et al. 70-Gene signature as an aid to treatment decisions in early-stage breast cancer. N. Engl. J. Med. 375, 717–729 (2016).
McVeigh, T. P. & Kerin, M. J. Clinical use of the oncotype DX genomic test to guide treatment decisions for patients with invasive breast cancer. Breast Cancer 9, 393–400 (2017).
Cronin, M. et al. Analytical validation of the oncotype DX genomic diagnostic test for recurrence prognosis and therapeutic response prediction in node-negative, estrogen receptor-positive breast cancer. Clin. Chem. 53, 1084–1091 (2007).
Sparano, J. A. & Paik, S. Development of the 21-gene assay and its application in clinical practice and clinical trials. J. Clin. Oncol. 26, 721–728 (2008).
Arnedos, M. et al. Precision medicine for metastatic breast cancer--limitations and solutions. Nat. Rev. Clin. Oncol. 12, 693–704 (2015).
Smith, I. E. & Dowsett, M. Aromatase inhibitors in breast cancer. N. Engl. J. Med. 348, 2431–2442 (2003).
Desta, Z., Ward, B. A., Soukhova, N. V. & Flockhart, D. A. Comprehensive evaluation of tamoxifen sequential biotransformation by the human cytochrome P450 system in vitro: prominent roles for CYP3A and CYP2D6. J. Pharmacol. Exp. Ther. 310, 1062–1075 (2004).
Mates, M. et al. Systemic targeted therapy for her2-positive early female breast cancer: a systematic review of the evidence for the 2014 Cancer Care Ontario systemic therapy guideline. Curr. Oncol. 22, S114–122 (2015).
Cobleigh, M. A. et al. Multinational study of the efficacy and safety of humanized anti-HER2 monoclonal antibody in women who have HER2-overexpressing metastatic breast cancer that has progressed after chemotherapy for metastatic disease. J. Clin. Oncol. 17, 2639–2648 (1999).
Citri, A. & Yarden, Y. EGF-ERBB signalling: towards the systems level. Nat. Rev. Mol. Cell Biol. 7, 505–516 (2006).
Slamon, D. J. et al. Use of chemotherapy plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2. N. Engl. J. Med. 344, 783–792 (2001).
Swain, S. M. et al. Pertuzumab, trastuzumab, and docetaxel in HER2-positive metastatic breast cancer. N. Engl. J. Med. 372, 724–734 (2015).
Verma, S. et al. Trastuzumab emtansine for HER2-positive advanced breast cancer. N. Engl. J. Med. 367, 1783–1791 (2012).
Stephens, P. J. et al. The landscape of cancer genes and mutational processes in breast cancer. Nature 486, 400–404 (2012).
Cancer Genome Atlas Network. Comprehensive molecular portraits of human breast tumours. Nature 490, 61–70 (2012).
Loi, S. et al. PIK3CA genotype and a PIK3CA mutation-related gene signature and response to everolimus and letrozole in estrogen receptor positive breast cancer. PLoS One 8, e53292 (2013).
Richards, S. et al. Standards and guidelines for the interpretation of sequence variants: a joint consensus recommendation of the american college of medical genetics and genomics and the association for molecular pathology. Genet. Med. 17, 405–424 (2015).
Spurdle, A. B. et al. ENIGMA--evidence-based network for the interpretation of germline mutant alleles: an international initiative to evaluate risk and clinical significance associated with sequence variation in BRCA1 and BRCA2 genes. Hum. Mutat. 33, 2–7 (2012).
Tavtigian, S. V., Greenblatt, M. S., Lesueur, F. & Byrnes, G. B. In silico analysis of missense substitutions using sequence-alignment based methods. Hum. Mutat. 29, 1327–1336 (2008).
Lindor, N. M. et al. A review of a multifactorial probability-based model for classification of BRCA1 and BRCA2 variants of uncertain significance (VUS). Hum. Mutat. 33, 8–21 (2012).
Collett, K. et al. A basal epithelial phenotype is more frequent in interval breast cancers compared with screen detected tumors. Cancer Epidemiol. Biomark. Prev. 14, 1108–1112 (2005).
Stockmans, G., Deraedt, K., Wildiers, H., Moerman, P. & Paridaens, R. Triple-negative breast cancer. Curr. Opin. Oncol. 20, 614–620 (2008).
Amir, E. et al. Prospective study evaluating the impact of tissue confirmation of metastatic disease in patients with breast cancer. J. Clin. Oncol. 30, 587–592 (2012).
Niikura, N. et al. Loss of human epidermal growth factor receptor 2 (HER2) expression in metastatic sites of HER2-overexpressing primary breast tumors. J. Clin. Oncol. 30, 593–599 (2012).
Nakai, K., Hung, M. C. & Yamaguchi, H. A perspective on anti-EGFR therapies targeting triple-negative breast cancer. Am. J. Cancer Res. 6, 1609–1623 (2016).
Reis-Filho, J. S. & Tutt, A. N. Triple negative tumours: a critical review. Histopathology 52, 108–118 (2008).
Bianchini, G., Balko, J. M., Mayer, I. A., Sanders, M. E. & Gianni, L. Triple-negative breast cancer: challenges and opportunities of a heterogeneous disease. Nat. Rev. Clin. Oncol. 13, 674–690 (2016).
Ciardiello, F. & Tortora, G. A novel approach in the treatment of cancer: targeting the epidermal growth factor receptor. Clin. Cancer Res. 7, 2958–2970 (2001).
Maemondo, M. et al. Gefitinib or chemotherapy for non-small-cell lung cancer with mutated EGFR. N. Engl. J. Med. 362, 2380–2388 (2010).
Mitsudomi, T. et al. Gefitinib versus cisplatin plus docetaxel in patients with non-small-cell lung cancer harbouring mutations of the epidermal growth factor receptor (WJTOG3405): an open label, randomised phase 3 trial. Lancet Oncol. 11, 121–128 (2010).
Zhou, C. et al. Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): a multicentre, open-label, randomised, phase 3 study. Lancet Oncol. 12, 735–742 (2011).
Rosell, R. et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): a multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 13, 239–246 (2012).
Wu, Y. L. et al. Intercalated combination of chemotherapy and erlotinib for patients with advanced stage non-small-cell lung cancer (FASTACT-2): a randomised, double-blind trial. Lancet Oncol. 14, 777–786 (2013).
Seto, T. et al. Erlotinib alone or with bevacizumab as first-line therapy in patients with advanced non-squamous non-small-cell lung cancer harbouring EGFR mutations (JO25567): an open-label, randomised, multicentre, phase 2 study. Lancet Oncol. 15, 1236–1244 (2014).
Kobayashi, S. et al. EGFR mutation and resistance of non-small-cell lung cancer to gefitinib. N. Engl. J. Med. 352, 786–792 (2005).
Yu, H. A. et al. Analysis of tumor specimens at the time of acquired resistance to EGFR-TKI therapy in 155 patients with EGFR-mutant lung cancers. Clin. Cancer Res. 19, 2240–2247 (2013).
Sequist, L. V. et al. Phase III study of afatinib or cisplatin plus pemetrexed in patients with metastatic lung adenocarcinoma with EGFR mutations. J. Clin. Oncol. 31, 3327–3334 (2013).
Wu, Y. L. et al. Afatinib versus cisplatin plus gemcitabine for first-line treatment of Asian patients with advanced non-small-cell lung cancer harbouring EGFR mutations (LUX-Lung 6): an open-label, randomised phase 3 trial. Lancet Oncol. 15, 213–222 (2014).
Janne, P. A. et al. AZD9291 in EGFR inhibitor-resistant non-small-cell lung cancer. N. Engl. J. Med. 372, 1689–1699 (2015).
Sequist, L. V., Rolfe, L. & Allen, A. R. Rociletinib in EGFR-mutated non-small-cell lung cancer. N. Engl. J. Med. 373, 578–579 (2015).
Greig, S. L. Osimertinib: first global approval. Drugs 76, 263–273 (2016).
Hallberg, B. & Palmer, R. H. Mechanistic insight into ALK receptor tyrosine kinase in human cancer biology. Nat. Rev. Cancer 13, 685–700 (2013).
Soda, M. et al. Identification of the transforming EML4-ALK fusion gene in non-small-cell lung cancer. Nature 448, 561–566 (2007).
Rikova, K. et al. Global survey of phosphotyrosine signaling identifies oncogenic kinases in lung cancer. Cell 131, 1190–1203 (2007).
Takeuchi, K. et al. KIF5B-ALK, a novel fusion oncokinase identified by an immunohistochemistry-based diagnostic system for ALK-positive lung cancer. Clin. Cancer Res. 15, 3143–3149 (2009).
Heuckmann, J. M. et al. Differential protein stability and ALK inhibitor sensitivity of EML4-ALK fusion variants. Clin. Cancer Res. 18, 4682–4690 (2012).
Togashi, Y. et al. KLC1-ALK: a novel fusion in lung cancer identified using a formalin-fixed paraffin-embedded tissue only. PLoS One 7, e31323 (2012).
Kim, H. R. et al. Distinct clinical features and outcomes in never-smokers with nonsmall cell lung cancer who harbor EGFR or KRAS mutations or ALK rearrangement. Cancer 118, 729–739 (2012).
Davies, K. D. & Doebele, R. C. Molecular pathways: ROS1 fusion proteins in cancer. Clin. Cancer Res. 19, 4040–4045 (2013).
Michels, S. & Wolf, J. Stratified treatment in lung cancer. Oncol. Res. Treat. 39, 760–766 (2016).
Shaw, A. T. et al. Crizotinib versus chemotherapy in advanced ALK-positive lung cancer. N. Engl. J. Med. 368, 2385–2394 (2013).
Solomon, B. J. et al. First-line crizotinib versus chemotherapy in ALK-positive lung cancer. N. Engl. J. Med. 371, 2167–2177 (2014).
Shaw, A. T. et al. Crizotinib in ROS1-rearranged non-small-cell lung cancer. N. Engl. J. Med. 371, 1963–1971 (2014).
Paik, P. K. et al. Response to MET inhibitors in patients with stage IV lung adenocarcinomas harboring MET mutations causing exon 14 skipping. Cancer Discov. 5, 842–849 (2015).
Shaw, A. T. et al. Ceritinib in ALK-rearranged non-small-cell lung cancer. N. Engl. J. Med. 370, 1189–1197 (2014).
Sakamoto, H. et al. CH5424802, a selective ALK inhibitor capable of blocking the resistant gatekeeper mutant. Cancer Cell 19, 679–690 (2011).
Hyman, D. M. et al. Vemurafenib in multiple nonmelanoma cancers with BRAF V600 mutations. N. Engl. J. Med. 373, 726–736 (2015).
Planchard, D. et al. Dabrafenib plus trametinib in patients with previously treated BRAF(V600E)-mutant metastatic non-small cell lung cancer: an open-label, multicentre phase 2 trial. Lancet Oncol. 17, 984–993 (2016).
Lee, L., Gupta, M. & Sahasranaman, S. Immune checkpoint inhibitors: an introduction to the next-generation cancer immunotherapy. J. Clin. Pharmacol. 56, 157–169 (2016).
Chen, Y. M. Immune checkpoint inhibitors for nonsmall cell lung cancer treatment. J. Chin. Med. Assoc. 80, 7–14 (2017).
Rizvi, N. A. et al. Activity and safety of nivolumab, an anti-PD-1 immune checkpoint inhibitor, for patients with advanced, refractory squamous non-small-cell lung cancer (CheckMate 063): a phase 2, single-arm trial. Lancet Oncol. 16, 257–265 (2015).
Gettinger, S. N. et al. Overall survival and long-term safety of nivolumab (anti-programmed death 1 antibody, BMS-936558, ONO-4538) in patients with previously treated advanced non-small-cell lung cancer. J. Clin. Oncol. 33, 2004–2012 (2015).
Brahmer, J. et al. Nivolumab versus docetaxel in advanced squamous-cell non-small-cell lung cancer. N. Engl. J. Med. 373, 123–135 (2015).
Borghaei, H. et al. Nivolumab versus docetaxel in advanced nonsquamous non-small-cell lung cancer. N. Engl. J. Med. 373, 1627–1639 (2015).
Garon, E. B. et al. Pembrolizumab for the treatment of non-small-cell lung cancer. N. Engl. J. Med. 372, 2018–2028 (2015).
Hirsch, F. R. et al. Lung cancer: current therapies and new targeted treatments. Lancet 389, 299–311 (2017).
Greaves, M. & Maley, C. C. Clonal evolution in cancer. Nature 481, 306–313 (2012).
Nowell, P. C. The clonal evolution of tumor cell populations. Science 194, 23–28 (1976).
Lipinski, K. A. et al. Cancer evolution and the limits of predictability in precision cancer medicine. Trends Cancer 2, 49–63 (2016).
Piotrowska, Z. et al. Heterogeneity underlies the emergence of EGFRT790 wild-type clones following treatment of T790M-positive cancers with a third-generation EGFR Inhibitor. Cancer Discov. 5, 713–722 (2015).
Sequist, L. V. et al. Rociletinib in EGFR-mutated non-small-cell lung cancer. N. Engl. J. Med. 372, 1700–1709 (2015).
Niederst, M. J. et al. The allelic context of the C797S mutation acquired upon treatment with third-generation EGFR inhibitors impacts sensitivity to subsequent treatment strategies. Clin. Cancer Res. 21, 3924–3933 (2015).
Davies, H. et al Mutations of the BRAF gene in human cancer. Nature 417, 949–954 (2002).
Menzies, A. M. et al. Distinguishing clinicopathologic features of patients with V600E and V600K BRAF-mutant metastatic melanoma. Clin. Cancer Res. 18, 3242–3249 (2012).
Chapman, P. B. et al. Improved survival with vemurafenib in melanoma with BRAF V600E mutation. N. Engl. J. Med. 364, 2507–2516 (2011).
Hauschild, A. et al. Dabrafenib in BRAF-mutated metastatic melanoma: a multicentre, open-label, phase 3 randomised controlled trial. Lancet 380, 358–365 (2012).
Lovly, C. M. & Shaw, A. T. Molecular pathways: resistance to kinase inhibitors and implications for therapeutic strategies. Clin. Cancer Res. 20, 2249–2256 (2014).
Nazarian, R. et al. Melanomas acquire resistance to B-RAF(V600E) inhibition by RTK or N-RAS upregulation. Nature 468, 973–977 (2010).
Flaherty, K. T. et al. Improved survival with MEK inhibition in BRAF-mutated melanoma. N. Engl. J. Med. 367, 107–114 (2012).
Johannessen, C. M. et al. COT drives resistance to RAF inhibition through MAP kinase pathway reactivation. Nature 468, 968–972 (2010).
Flaherty, K. T. et al. Combined BRAF and MEK inhibition in melanoma with BRAF V600 mutations. N. Engl. J. Med. 367, 1694–1703 (2012).
Ascierto, P. A. et al. Cobimetinib combined with vemurafenib in advanced BRAF(V600)-mutant melanoma (coBRIM): updated efficacy results from a randomised, double-blind, phase 3 trial. Lancet Oncol. 17, 1248–1260 (2016).
Chapon, M. et al. Progressive upregulation of PD-1 in primary and metastatic melanomas associated with blunted TCR signaling in infiltrating T lymphocytes. J. Invest. Dermatol. 131, 1300–1307 (2011).
Hodi, F. S. et al. Improved survival with ipilimumab in patients with metastatic melanoma. N. Engl. J. Med. 363, 711–723 (2010).
O’Day, S. J. et al. Efficacy and safety of ipilimumab monotherapy in patients with pretreated advanced melanoma: a multicenter single-arm phase II study. Ann. Oncol. 21, 1712–1717 (2010).
Topalian, S. L. et al. Safety, activity, and immune correlates of anti-PD-1 antibody in cancer. N. Engl. J. Med. 366, 2443–2454 (2012).
Topalian, S. L. et al. Survival, durable tumor remission, and long-term safety in patients with advanced melanoma receiving nivolumab. J. Clin. Oncol. 32, 1020–1030 (2014).
Robert, C. et al. Nivolumab in previously untreated melanoma without BRAF mutation. N. Engl. J. Med. 372, 320–330 (2015).
Robert, C. et al. Pembrolizumab versus Ipilimumab in advanced melanoma. N. Engl. J. Med. 372, 2521–2532 (2015).
Larkin, J. et al. Combined Nivolumab and Ipilimumab or monotherapy in untreated melanoma. N. Engl. J. Med. 373, 23–34 (2015).
Zaretsky, J. M. et al. Mutations associated with acquired resistance to PD-1 blockade in melanoma. N. Engl. J. Med. 375, 819–829 (2016).
Shin, D. S. et al. Primary resistance to PD-1 blockade mediated by JAK1/2 mutations. Cancer Discov. 7, 188–201 (2017).
Allard, W. J. et al. Tumor cells circulate in the peripheral blood of all major carcinomas but not in healthy subjects or patients with nonmalignant diseases. Clin. Cancer Res. 10, 6897–6904 (2004).
Jiang, P. et al. Lengthening and shortening of plasma DNA in hepatocellular carcinoma patients. Proc. Natl. Acad. Sci. USA 112, E1317–1325 (2015).
Schwarzenbach, H., Hoon, D. S. & Pantel, K. Cell-free nucleic acids as biomarkers in cancer patients. Nat. Rev. Cancer 11, 426–437 (2011).
Alix-Panabieres, C. & Pantel, K. Clinical applications of circulating tumor cells and circulating tumor DNA as liquid biopsy. Cancer Discov. 6, 479–491 (2016).
Mavroudis, D. Circulating cancer cells. Ann. Oncol. 21(Suppl. 7), vii95–vii100 (2010).
Miller, M. C., Doyle, G. V. & Terstappen, L. W. Significance of circulating tumor cells detected by the cellsearch system in patients with metastatic breast colorectal and prostate cancer. J. Oncol. 2010, 617421 (2010).
Alix-Panabieres, C. & Pantel, K. Circulating tumor cells: liquid biopsy of cancer. Clin. Chem. 59, 110–118 (2013).
Morris, R. J. Circulating tumor cells: quintessential precision oncology presenting challenges for biology. npj Precision Oncology. doi:10.1038/s41698-017-0019-9 (2017).
Scher, H. I. et al. Circulating tumor cell biomarker panel as an individual-level surrogate for survival in metastatic castration-resistant prostate cancer. J. Clin. Oncol. 33, 1348–1355 (2015).
Witek, M. A. et al. Discrete microfluidics for the isolation of circulating tumor cell subpopulations targeting fibroblast activation protein alpha and epithelial cell adhesion molecule. npj Precision Oncology. doi:10.1038/s41698-017-0028-8 (2017).
Renier, C. et al. Label-free isolation of prostate circulating tumor cells using Vortex microfluidic technology. npj Precision Oncology. doi:10.1038/s41698-017-0015-0 (2017).
Tanaka, S. et al. The lack of increases in circulating endothelial progenitor cell as a negative predictor for pathological response to neoadjuvant chemotherapy in breast cancer patients. npj Precision Oncology. doi:10.1038/s41698-017-0006-1 (2017).
Smerage, J. B. et al. Circulating tumor cells and response to chemotherapy in metastatic breast cancer: SWOG S0500. J. Clin. Oncol. 32, 3483–3489 (2014).
Diehl, F. et al. Detection and quantification of mutations in the plasma of patients with colorectal tumors. Proc. Natl. Acad. Sci. USA 102, 16368–16373 (2005).
Bettegowda, C. et al. Detection of circulating tumor DNA in early- and late-stage human malignancies. Sci. Transl. Med. 6, 224ra224 (2014).
Siravegna, G. et al. Clonal evolution and resistance to EGFR blockade in the blood of colorectal cancer patients. Nat. Med. 21, 827 (2015).
Hidalgo, M. et al. Patient-derived xenograft models: an emerging platform for translational cancer research. Cancer Discov. 4, 998–1013 (2014).
Aparicio, S., Hidalgo, M. & Kung, A. L. Examining the utility of patient-derived xenograft mouse models. Nat. Rev. Cancer 15, 311–316 (2015).
Fiebig, H. H. et al. Development of three human small cell lung cancer models in nude mice. Recent Results Cancer Res. 97, 77–86 (1985).
Bruna, A. et al. A biobank of breast cancer explants with preserved intra-tumor heterogeneity to screen anticancer compounds. Cell 167, 260–274, e222 (2016).
Morton, J. J., Bird, G., Refaeli, Y. & Jimeno, A. Humanized mouse xenograft models: narrowing the tumor-microenvironment gap. Cancer Res. 76, 6153–6158 (2016).
Gao, H. et al. High-throughput screening using patient-derived tumor xenografts to predict clinical trial drug response. Nat. Med. 21, 1318–1325 (2015).
Ledford, H. US cancer institute to overhaul tumour cell lines. Nature 530, 391 (2016).
Townsend, E. C. et al. The public repository of xenografts enables discovery and randomized phase II-like trials in mice. Cancer Cell 29, 574–586 (2016).
Byrne, A. T. et al. Interrogating open issues in cancer precision medicine with patient-derived xenografts. Nat. Rev. Cancer 17, 254–268 (2017).
Prasad, V. Perspective: the precision-oncology illusion. Nature 537, S63 (2016).
Prasad, V., Fojo, T. & Brada, M. Precision oncology: origins, optimism, and potential. Lancet Oncol. 17, e81–86 (2016).
Le Tourneau, C. et al. Molecularly targeted therapy based on tumour molecular profiling versus conventional therapy for advanced cancer (SHIVA): a multicentre, open-label, proof-of-concept, randomised, controlled phase 2 trial. Lancet Oncol. 16, 1324–1334 (2015).
Tannock, I. F. & Hickman, J. A. Limits to personalized cancer medicine. N. Engl. J. Med. 375, 1289–1294 (2016).
Gerlinger, M. et al. Intratumor heterogeneity and branched evolution revealed by multiregion sequencing. N. Engl. J. Med. 366, 883–892 (2012).
Arbiser, J. L. et al. Targeting the duality of cancer. npj Precision Oncology. doi:10.1038/s41698-017-0026-x (2017).
Liu, F., Mischel, P. S. & Cavenee, W. K. Precision cancer therapy is impacted by oncogene-dependent epigenome remodeling. npj Precision Oncology. doi:10.1038/s41698-017-0005-2 (2017).
Mullard, A. NCI-MATCH trial pushes cancer umbrella trial paradigm. Nat. Rev. Drug. Discov. 14, 513–515 (2015).
Brower, V. NCI-MATCH pairs tumor mutations with matching drugs. Nat. Biotechnol. 33, 790–791 (2015).
Coyne, G. O., Takebe, N. & Chen, A. P. Defining precision: the precision medicine initiative trials NCI-MPACT and NCI-MATCH. Curr. Probl. Cancer 41, 182–193 (2017).
O’Brien, S. G. et al. Imatinib compared with interferon and low-dose cytarabine for newly diagnosed chronic-phase chronic myeloid leukemia. N. Engl. J. Med. 348, 994–1004 (2003).
Barone, A. et al. FDA approval summary: pembrolizumab for the treatment of patients with unresectable or metastatic melanoma. Clin. Cancer Res. doi:10.1158/1078-0432.CCR-16-0664 (2017).
Sul, J. et al. FDA approval summary: pembrolizumab for the treatment of patients with metastatic non-small cell lung cancer whose tumors express programmed death-ligand 1. Oncologist 21, 643–650 (2016).
Colwell, J. Pembrolizumab approved for Hodgkin lymphoma. Cancer Discov. doi:10.1158/2159-8290.CD-NB2017-044 (2017).
Larkins, E. et al. U.S. food and drug administration approval summary: pembrolizumab for the treatment of recurrent or metastatic head and neck squamous cell carcinoma with disease progression on or after platinum-containing chemotherapy. Oncologist 22, 873–878 (2017).
Nogova, L. et al. Evaluation of BGJ398, a fibroblast growth factor receptor 1-3 kinase inhibitor, in patients with advanced solid tumors harboring genetic alterations in fibroblast growth factor receptors: results of a global phase I, dose-escalation and dose-expansion study. J. Clin. Oncol. 35, 157–165 (2017).
Wenk, M. R. The emerging field of lipidomics. Nat. Rev. Drug Discov. 4, 594–610 (2005).
Hall, Z. et al. Myc expression drives aberrant lipid metabolism in lung cancer. Cancer Res. 76, 4608–4618 (2016).
Nickell, S., Kofler, C., Leis, A. P. & Baumeister, W. A visual approach to proteomics. Nat. Rev. Mol. Cell Biol. 7, 225–230 (2006).
Taylor, N. M. I. et al. Structure of the human multidrug transporter ABCG2. Nature 546, 504–509 (2017).
Koppel, N., Maini Rekdal, V. & Balskus, E. P. Chemical transformation of xenobiotics by the human gut microbiota. Science, doi:10.1126/science.aag2770 (2017).
Wallace, B. D. et al. Alleviating cancer drug toxicity by inhibiting a bacterial enzyme. Science 330, 831–835 (2010).
Acknowledgements
This work was supported by The Hormel Foundation. S.H.S. was supported by a Bioinformatics and Computational Biology fellowship and a Doctoral Dissertation Fellowship from the University of Minnesota. We also thank Dr. Tia Rai for assistance in submitting this manuscript.
Author information
Authors and Affiliations
Contributions
Z.D. supervised the conception of the work and revised it critically. S.H.S. and A.M.B. wrote the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Shin, S., Bode, A.M. & Dong, Z. Addressing the challenges of applying precision oncology. npj Precision Onc 1, 28 (2017). https://doi.org/10.1038/s41698-017-0032-z
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41698-017-0032-z
This article is cited by
-
Revolutionizing personalized medicine with generative AI: a systematic review
Artificial Intelligence Review (2024)
-
Modelling acute myeloid leukemia (AML): What’s new? A transition from the classical to the modern
Drug Delivery and Translational Research (2023)
-
Precision gynecologic oncology: circulating cell free DNA epigenomic analysis, artificial intelligence and the accurate detection of ovarian cancer
Scientific Reports (2022)
-
Molecular profile of KRAS G12C-mutant colorectal and non-small-cell lung cancer
BMC Cancer (2021)
-
Cancer prevention and screening: the next step in the era of precision medicine
npj Precision Oncology (2019)
