
Abstract
Multidrug therapy for Mycobacterium avium complex pulmonary disease (MAC-PD) results in negative sputum cultures. However, the prognostic value of this treatment approach remains unclear. This study aimed to clarify whether multidrug therapy reduces the incidence of events related to MAC-PD and improves the mortality rate. Patients who met the diagnostic criteria for MAC-PD at our hospital between 2003 and 2019 were retrospectively evaluated using medical records. Events related to MAC-PD were defined as hospitalisation for haemoptysis or respiratory infection and the development of chronic respiratory failure. There were 90 and 108 patients in the multidrug and observation groups, respectively. The median observation period was 86 months. Intergroup differences in body mass index, proportion of patients with cavities, and erythrocyte sedimentation rate were not significant. However, the observation group was older with a higher mean age (multidrug group: 62 years, observation group: 69 years; P < 0.001) and had a higher proportion of male patients (multidrug group: 13/90 [14.4%], observation group: 35/108 [32.4%]; P < 0.01). Furthermore, intergroup differences in the incidence of events related to MAC-PD (multidrug group: 26.69/1000 person-years, observation group: 25.49/1000 person-years), MAC-PD-associated mortality rate (multidrug group: 12.13/1000 person-years, observation group: 12.74/1000 person-years), and total mortality (multidrug group: 24.26/1000 person-years, observation group: 29.50/1000 person-years) were not significant. Many patients relapse even after multidrug therapy, and our findings suggest that multidrug therapy has no effect in preventing the onset of respiratory events or prolonging life expectancy.
Similar content being viewed by others
Introduction
Non-tuberculous mycobacteria are environmentally ubiquitous. Pulmonary non-tuberculous mycobacterial disease can be caused by inhaling mycobacteria from the environment. In recent years, an increasing number of cases of pulmonary non-tuberculous mycobacterial disease have been reported worldwide1,2,3. There are over 190 species of non-tuberculous mycobacteria4; however, most pulmonary non-tuberculous mycobacterial disease cases are attributable to the Mycobacterium avium complex (MAC)3,5,6.
The 5-year and 10-year all-cause mortality rates in patients with MAC pulmonary disease (MAC-PD) have been reported as 23.9% and 46.5%, respectively, and the corresponding MAC-specific mortality rates were 5.4% and 15.7%7. Multidrug therapies, including clarithromycin, can yield bacteriological sputum culture conversion in patients with MAC-PD8,9. However, few studies have examined whether it can reduce hospitalisation and respiratory failure related to MAC-PD or mortality. Therefore, this study examined whether multidrug therapy reduces the incidence of events related to MAC-PD and improves the prognosis of the affected patients.
Methods
Study design and patients
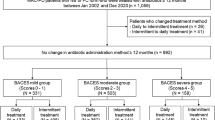
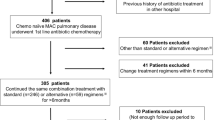
This retrospective study was conducted by evaluating patients’ medical records. Patients who were admitted to our hospital between 2003 and 2019, who met the 2020 diagnostic criteria established by the American Thoracic Society/European Respiratory Society/European Society of Clinical Microbiology and Infectious Diseases/Infectious Diseases Society of America, and for whom cultures were positive for MAC were included in the study10. The exclusion criteria were as follows: patients who had undergone surgery for MAC-PD, those with additional microbial infections other than MAC disease, and those with missing data required for the score assessment, which is a scoring system involving calculations based on the body mass index, age, presence of cavities, an elevated erythrocyte sedimentation rate, and sex, and reflects disease progression and mortality11,12. The included patients were divided into two groups. The multidrug therapy group included patients who received clarithromycin, ethambutol, and rifampicin for at least 1 year (including patients concomitantly treated with quinolones or aminoglycosides). The observation group included all the remaining patients.
The following three outcomes were analysed:
-
(1)
MAC-associated events, defined as hospitalisation for haemoptysis or respiratory infection and the onset of chronic respiratory failure;
-
(2)
MAC-specific mortality, defined as death due to haemoptysis, respiratory infection, or respiratory failure;
-
(3)
all-cause mortality.
We also conducted a prognosis analysis of patients who underwent multiple courses of treatment, classifying them according to the initial treatment.
Statistical analysis
Continuous and ordinal variables were expressed as medians and interquartile ranges, and groups were compared using Mann − Whitney U tests. Categorical variables were expressed as frequencies and percentages, and groups were compared using χ2 tests or Fisher's exact probability test. The incidence of MAC-PD-associated events, MAC-specific mortality, and all-cause mortality were expressed as the number of patients per 1000 person-years. Risk ratios and 95% confidence intervals (CI) were calculated. Kaplan–Meier curves were used to assess survival. The median values (95% CI) were presented, and the Gray test was used to compare MAC-PD-associated events and MAC-specific mortality between groups. The log-rank test was used to compare all-cause mortality. Factors predicting MAC-PD-associated events, MAC-specific mortality, and all-cause mortality were examined using single variable and multivariable Cox regression analyses. P-values < 0.05 were considered statistically significant. All statistical analyses were performed using EZR13, a modified version of the R commander designed to add statistical functions frequently used in biostatistics.
Ethical considerations
This study was approved by the medical ethics committee of Shinshu University School of Medicine (approval No. 4575). All methods were performed in accordance with the relevant guidelines and regulations. Informed consent was obtained from all patients through an opt-out process.
Results
Overall, 198 patients were included in this study, of whom 90 were included in the multidrug therapy group and 108 in the observation group. Among the patients in the multidrug therapy group, 23 were treated concurrently with aminoglycosides, 6 were treated concurrently with quinolones, and 3 were treated concurrently with both aminoglycosides and quinolones. Among the patients in the multidrug therapy group, 86 received one course of treatment and 4 underwent two courses of treatment. Of the 108 patients in the observation group, 20 had a treatment duration of less than 1 year, with 19 discontinuing treatment due to adverse events, and 1 discontinuing treatment due to interruption of outpatient visits. The median treatment duration for these 20 patients was 35.5 days (interquartile range, 19–90.75). The patient characteristics are shown in Table 1. The observation group was significantly older than the multidrug therapy group, and the total protein level in the observation group was significantly lower than that in the multidrug therapy group. The two groups had no significant differences in the mycobacterial species, diagnostic specimens, and sputum smear positivity for acid-fast bacillus. The body mass index, age, cavitary erythrocyte sedimentation rate, and sex (BACES) score in the observation group was 2 (range, 1–3), which was significantly higher than the score of 1 (range, 1–2.75) in the multidrug therapy group. The observation group had significantly higher proportions of patients aged 65 years and older and male patients, which contributed to the higher BACES score. Table 2 shows the incidence of MAC-associated events and MAC-specific mortality and all-cause mortality rates per 1000 person-years in the two groups. There were no significant differences in any of the outcomes between the groups.
Figure 1 shows the Kaplan–Meier curves for the cumulative incidence of MAC-PD-associated events and cumulative MAC-specific mortality, and all-cause mortality. The median time to MAC-PD-associated events in the multidrug therapy and observation groups was 278 and 244 months, respectively. The corresponding median times to MAC-specific death were 281 months and not available (NA). The median time to all-cause death was 281 and 251 months in the multidrug therapy and observation groups, respectively. There were no significant differences in any of the outcomes between the two groups.

(A) MAC-associated events. The median time to MAC-associated events was 278 months in the multidrug therapy group and 244 months in the observation group, with no significant intergroup differences. (B) MAC-specific mortality. The median time to MAC-specific death was 281 months in the multidrug therapy group and NA in the observation group, with no significant intergroup difference. (C) All-cause mortality. The median time to all-cause death was 281 months in the multidrug therapy group and 251 months in the observation group, with no significant intergroup difference. MAC Mycobacterium avium complex, NA not available.
Table 3 shows the results of the unadjusted and adjusted Cox regression analyses. Considering the number of patients, events, and deaths, two explanatory variables were selected: BACES score and multidrug therapy. The two explanatory variables were analysed using the forced entry method for the multivariable analysis. The BACES score significantly predicted all outcome measures, including MAC-associated events, MAC-specific mortality, and all-cause mortality. However, multidrug therapy was not associated with any of the outcomes.
Discussion
Multidrug therapy has been shown to reduce all-cause mortality in cases of pulmonary non-tuberculous mycobacterial disease14,15,16. However, these studies included MAC-PD and other pulmonary non-tuberculous mycobacterial diseases. For example, in studies that include infection due to bacterial species with relatively favourable treatment responses, such as Mycobacterium kansasii17, or relatively poor treatment responses, such as Mycobacterium abscessus18, the potential improvement in mortality rates through therapeutic interventions may differ from those in studies of MAC-PD alone. In this study which focused specifically on MAC-PD, multidrug therapy was not associated with decreased all-cause mortality. When comparing the two bacterial species within the MAC, M. intracellulare infections have been reported to have a worse prognosis than M. avium infections14,19. In this study, the number of patients with M. intracellulare infection was relatively small; therefore, the two bacterial species were not compared. However, there were no differences in the proportions of the two bacterial species between the multidrug therapy and observation groups. Furthermore, previous studies have also included patients who did not receive adequate treatment according to the current guidelines10, which involve administering a combination of three or more drugs, including macrolides and ethambutol, for at least 1 year after achieving negative sputum cultures.
In this study, multidrug therapy involved a treatment regimen containing clarithromycin, ethambutol, and rifampicin. Azithromycin is considered to have better tolerability than clarithromycin; however, there is no significant difference in efficacy between the two drugs10. In Japan, owing to medical regulations, azithromycin must be administered after clarithromycin treatment. Therefore, in this study, patients receiving macrolide therapy were specifically those who were administered clarithromycin.
The guidelines recommend a treatment duration of 1 year or more after sputum culture conversion to negative. However, in this study, over 50% of the cases were diagnosed using bronchial lavage fluid, as there was no expectoration of sputum. These cases without sputum expectoration could not be assessed for sputum culture conversion to negative, and as a result, the treatment duration is not specified in the guidelines. Therefore, this study defined the total treatment period as 1 year for the multidrug therapy group. To standardise the treatment duration, patients diagnosed based on sputum were also included in the multidrug therapy group, regardless of sputum culture conversion, if they received treatment for 1 year.
In this study, multidrug therapy was not associated with reduced overall mortality, MAC-associated events, or MAC-specific mortality. To our knowledge, no previous studies have investigated the effects of multidrug therapy on MAC-associated events or MAC-specific mortality. Furthermore, the BACES score is associated with all-cause mortality and death related to respiratory diseases and infections, treatment responsiveness, and disease progression11,12. In our study, patients in the observation group had a higher BACES score than those in the multidrug therapy group; however, the event and mortality rates did not differ between the two groups. These results suggest that multidrug therapy does not decrease the incidence of MAC-associated events or mortality.
Contrary to the findings of our study, a study by Kim et al.20 found that prognosis of MAC-PD was better in patients who received multidrug therapy. The results of the two studies may have differed because of differences in disease severity, such as the extent of bronchiectasis and systemic manifestations. Our study included a higher proportion of patients with lower BACES scores and relatively mild disease, such as those with negative sputum smears. Even without treatment, many of these patients are likely to have had a favourable prognosis.
The rate of negative conversion of sputum culture achieved with combination therapy is only 60–90%, which is suboptimal8,9. Relapse and reinfection are rare after achieving negative sputum culture20,21, which may have contributed to the findings of our study. A previous study demonstrated improved quality of life associated with treating pulmonary non-tuberculous mycobacterial disease22. A recent study evaluating the effectiveness of multidrug therapy has emphasised the importance of microbiological assessments and considering the quality of life23. Major symptoms such as severe fatigue are associated with markedly decreased quality of life and can also be key factors in starting multidrug therapy10. Therefore, the use of multidrug therapy to improve quality of life should be considered. When evaluating the improvement in the quality of life of patients with MAC-PD, it is essential to use established assessment tools24, such as St. George’s Respiratory Questionnaire, which has been validated for assessing the quality of life of patients with MAC-PD25.
Our study has some limitations. First, the treatments were not fully compliant with the guidelines because some patients did not receive treatment for 12 months after sputum culture conversion, and the recommended dose of antimicrobial agents was not consistently maintained. Second, susceptibility to clarithromycin was not confirmed in some cases, raising the possibility of MAC-PD caused by clarithromycin-resistant strains. Third, many cases were lost to follow-up within 5–10 years of the start of observation, leading to premature termination of the study. Fourth, the number of patients is relatively small, and this is also a single-centre study, so the generalisability may be limited.
Our study showed that multidrug therapy with clarithromycin, ethambutol, and rifampicin for MAC-PD may not reduce the incidence of hospitalisation events, respiratory failure related to MAC-PD, or mortality.
Data availability
The datasets generated during and/or analysed during the current study are not publicly available due to ethical restrictions but are available from the corresponding author on reasonable request.
References
Thomson, R. M., NTM Working Group at Queensland TB Control Centre and Queensland Mycobacterial Reference Laboratory. Changing epidemiology of pulmonary nontuberculous mycobacteria infections. Emerg. Infect. Dis. 16, 1576–1583. https://doi.org/10.3201/eid1610.091201 (2010).
Henkle, E., Hedberg, K., Schafer, S., Novosad, S. & Winthrop, K. L. Population-based incidence of pulmonary non-tuberculous mycobacterial disease in Oregon 2007 to 2012. Ann. Am. Thorac. Soc. 12, 642–647. https://doi.org/10.1513/AnnalsATS.201412-559OC (2015).
Namkoong, H. et al. Epidemiology of pulmonary non-tuberculous mycobacterial disease, Japan. Emerg. Infect. Dis. 22, 1116–1117. https://doi.org/10.3201/eid2206.151086 (2016).
Forbes, B. A. Mycobacterial taxonomy. J. Clin. Microbiol. 55, 380–383. https://doi.org/10.1128/JCM.01287-16 (2017).
Marras, T. K. & Daley, C. L. Epidemiology of human pulmonary infection with non-tuberculous mycobacteria. Clin. Chest Med. 23, 553–567. https://doi.org/10.1016/S0272-5231(02)00019-9 (2002).
Simons, S. et al. Non-tuberculous mycobacteria in respiratory tract infections, eastern Asia. Emerg. Infect. Dis. 17, 343–349. https://doi.org/10.3201/eid1703.100604 (2011).
Hayashi, M. et al. Prognostic factors of 634 HIV-negative patients with Mycobacterium avium complex lung disease. Am. J. Respir. Crit. Care Med. 185, 575–583. https://doi.org/10.1164/rccm.201107-1203OC (2012).
Pasipanodya, J. G., Ogbonna, D., Deshpande, D., Srivastava, S. & Gumbo, T. Meta-analyses and the evidence base for microbial outcomes in the treatment of pulmonary Mycobacterium avium-intracellulare complex disease. J. Antimicrob. Chemother. 72(Suppl 2), i3–i19. https://doi.org/10.1093/jac/dkx311 (2017).
Kadota, J. I., Kurashima, A. & Suzuki, K. The clinical efficacy of a clarithromycin-based regimen for Mycobacterium avium complex disease: A nationwide post-marketing study. J. Infect. Chemother. 23, 293–300. https://doi.org/10.1016/j.jiac.2017.01.007 (2017).
Daley, C. L. et al. Treatment of non-tuberculous mycobacterial pulmonary disease: An official ATS/ERS/ESCMID/IDSA clinical practice guideline. Clin. Infect. Dis. 71, e1–e36. https://doi.org/10.1093/cid/ciaa241 (2020).
Kim, H. J. et al. BACES score for predicting mortality in non-tuberculous mycobacterial pulmonary disease. Am. J. Respir. Crit. Care Med. 203, 230–236. https://doi.org/10.1164/rccm.202004-1418OC (2021).
Kim, H. J. et al. Usefulness of the BACES score in non-tuberculous mycobacterial pulmonary disease for various clinical outcomes. Sci. Rep. 13, 7495. https://doi.org/10.1038/s41598-023-33782-z (2023).
Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 48, 452–458. https://doi.org/10.1038/bmt.2012.244 (2013).
Jhun, B. W. et al. Prognostic factors associated with long-term mortality in 1445 patients with non-tuberculous mycobacterial pulmonary disease: A 15-year follow-up study. Eur. Respir. J. 55, 1900798. https://doi.org/10.1183/13993003.00798-2019 (2020).
Bemer, P. et al. Management of patients with pulmonary mycobacteriosis in France: A multicenter retrospective cohort study. BMC Pulm. Med. 21, 333. https://doi.org/10.1186/s12890-021-01701-5 (2021).
Im, Y. et al. Impact of time between diagnosis and treatment for non-tuberculous mycobacterial pulmonary disease on culture conversion and all-cause mortality. Chest 161, 1192–1200. https://doi.org/10.1016/j.chest.2021.10.048 (2022).
Yan, M., Brode, S. K. & Marras, T. K. The other non-tuberculous mycobacteria: Clinical aspects of lung disease caused by less common slowly growing non-tuberculous mycobacteria species. Chest 163, 281–291. https://doi.org/10.1016/j.chest.2022.09.025 (2023).
Broncano-Lavado, A., Senhaji-Kacha, A., Santamaría-Corral, G., Esteban, J. & García-Quintanilla, M. Alternatives to antibiotics against Mycobacterium abscessus. Antibiotics (Basel) 11, 1322. https://doi.org/10.3390/antibiotics11101322 (2022).
Pan, S. W. et al. Impact of different subspecies on disease progression in initially untreated patients with Mycobacterium avium complex lung disease. Clin. Microbiol. Infect. 27(467), e9-467.e14. https://doi.org/10.1016/j.cmi.2020.04.020 (2021).
Kim, J. Y. et al. Impact of treatment on long-term survival of patients with Mycobacterium avium complex pulmonary disease. Clin. Infect. Dis. 77, 120–126. https://doi.org/10.1093/cid/ciad108 (2023).
Theuretzbacher, U. et al. In memoriam: William A. Craig. Antimicrob. Agents Chemother. 59, 2971. https://doi.org/10.1128/AAC.00849-15 (2015).
Koh, W. J. et al. Outcomes of Mycobacterium avium complex lung disease based on clinical phenotype. Eur. Respir. J. 50, 1602503. https://doi.org/10.1183/13993003.02503-2016 (2017).
Czaja, C. A. et al. Improvement in quality of life after therapy for Mycobacterium abscessus group lung infection. A prospective cohort study. Ann. Am. Thorac. Soc. 13, 40–48. https://doi.org/10.1513/AnnalsATS.201508-529OC (2016).
Henkle, E. et al. Patient-centered research priorities for pulmonary non-tuberculous mycobacteria (NTM) infection. An NTM research consortium workshop report. Ann. Am. Thorac. Soc 13, S379–S384. https://doi.org/10.1513/AnnalsATS.201605-387WS (2016).
Hama, M. et al. Health-related quality of life in patients with pulmonary non-tuberculous mycobacteria infection. Int. J. Tuberc. Lung Dis. 20, 747–752. https://doi.org/10.5588/ijtld.15.0460 (2016).
Author information
Authors and Affiliations
Contributions
A.U. conceived the study. A.U., M.Y., J.A., and Y.I. developed the statistical analysis plan and conducted statistical analyses. All authors contributed to the interpretation of the results. A.U. drafted the manuscript. M.H. supervised the study. All the authors reviewed the manuscript draft and critically revised it for intellectual content. All authors have approved the final version of the manuscript for publication.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ushiki, A., Tanaka, S., Yamanaka, M. et al. Effect of multidrug therapy on the prognosis of Mycobacterium avium complex pulmonary disease. Sci Rep 14, 4438 (2024). https://doi.org/10.1038/s41598-024-55135-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-55135-0
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
