
Abstract
One of the most promising new treatments for gonorrhoea currently in phase 3 clinical trials is zoliflodacin. Studies have found very little resistance to zoliflodacin in currently circulating N. gonorrhoeae strains, and in-vitro experiments demonstrated that it is difficult to induce resistance. However, zoliflodacin resistance may emerge in commensal Neisseria spp., which could then be transferred to N. gonorrhoeae via transformation. In this study, we investigated this commensal-resistance-pathway hypothesis for zoliflodacin. To induce zoliflodacin resistance, ten wild-type susceptible isolates belonging to 5 Neisseria species were serially passaged for up to 48 h on gonococcal agar plates containing increasing zoliflodacin concentrations. Within 7 to 10 days, all strains except N. lactamica, exhibited MICs of ≥ 4 µg/mL, resulting in MIC increase ranging from 8- to 64-fold. The last passaged strains and their baseline were sequenced. We detected mutations previously reported to cause zoliflodacin resistance in GyrB (D429N and S467N), novel mutations in the quinolone resistance determining region (QRDR) (M464R and T472P) and mutations outside the QRDR at amino acid positions 28 and 29 associated with low level resistance (MIC 2 µg/mL). Genomic DNA from the laboratory evolved zoliflodacin-resistant strains was transformed into the respective baseline wild-type strain, resulting in MICs of ≥ 8 µg/mL in most cases. WGS of transformants with decreased zoliflodacin susceptibility revealed presence of the same zoliflodacin resistance determinants as observed in the donor strains. Two inter-species transformation experiments were conducted to investigate whether zoliflodacin resistance determinants of commensal Neisseria spp. could be acquired by N. gonorrhoeae. N. gonorrhoeae strain WHO P was exposed to (i) pooled genomic DNA from the two resistant N. mucosa strains and (ii) a gyrB amplicon of the resistant N. subflava strain 45/1_8. Transformants of both experiments exhibited an MIC of 2 µg/mL and whole genome analysis revealed uptake of the mutations detected in the donor strains. This is the first in-vitro study to report that zoliflodacin resistance can be induced in commensal Neisseria spp. and subsequently transformed into N. gonorrhoeae.
Similar content being viewed by others

Introduction
The continued emergence and spread of combined gonococcal resistance to ceftriaxone and azithromycin has reinvigorated the search for alternative therapies1. One of the most promising new treatments currently in phase 3 clinical trials is zoliflodacin (NCT03959527)1. Zoliflodacin (ETX0914) belongs to a new class of antibiotics that inhibit bacterial DNA replication via interactions with DNA gyrase subunit B2. Studies have found very little resistance to zoliflodacin in currently circulating strains of Neisseria gonorrhoeae3. In addition, a number of in-vitro experiments have found that it is difficult to induce zoliflodacin resistance in N. gonorrhoeae using currently recommended treatment regimens4,5,6. Based on these findings, several authors have concluded that there is a low probability of zoliflodacin resistance emerging in N. gonorrhoeae following its introduction as a treatment for gonorrhoea3,4,6.
We and others have hypothesized that zoliflodacin resistance may emerge in commensal Neisseria spp. which could then be transferred to N. gonorrhoeae via transformation7. This hypothesis was based on the fact that transformation of resistance from commensal Neisseria spp. into N. gonorrhoeae has been instrumental in the emergence of cephalosporin, sulfonamide and macrolide resistance8,9,10,11. Transformation of gyrA has also played an important role in the genesis of fluoroquinolone resistance in N. meningitidis. A study in Shanghai, found that 99.3% of commensal Neisseria and 67.7% of N. meningitidis isolates were resistant to fluoroquinolones and that horizontal gene transfer (HGT) from commensals was responsible for fluoroquinolone resistance in over half the N. meningitidis isolates12. An in silico analysis of 20,047 Neisseria isolates from around the world found evidence that a number of strains of N. gonorrhoeae have previously taken up sections of gyrB from commensal Neisseria, including the quinolone resistance-determining region (QRDR; 1255–1488 bp) of gyrB, which is also the zoliflodacin resistance-conferring region13.
In vitro studies have demonstrated that gonococcal zoliflodacin resistance typically emerges via three substitutions in GyrB—Asp429Asn, Lys450Thr or Ser467Asn2,6. These findings provided the justification for the current paper where we investigated the commensal-resistance-pathway hypothesis as follows: Firstly, we sought to assess the zoliflodacin MICs of circulating commensal Neisseria species. Secondly, we assessed if we could induce zoliflodacin resistance in N. cinerea, N. lactamica, N. macacae, N. mucosa and N. subflava14. Thirdly, we evaluated which gyrB mutations were associated with evolved decreased susceptibility to zoliflodacin in these species. Finally, we attempted to transform zoliflodacin resistance-conferring DNA within and between Neisseria species including from N. subflava/N. mucosa into N. gonorrhoeae.
Methods
Sampling, ethical approval and bacterial isolates used in the study
Details of the isolates used for this experiment are provided in Tables 1, 2 and Suppl Table 1. The commensal Neisseria isolates were cultured from oropharyngeal swabs from asymptomatic men and women participating in three recently performed clinical studies at our centre in Belgium—the Resistogenicity, ComCom, PReGo and ResistAZM (NCT05027516) studies14,15,16. The samples were obtained between 2019 and 2022. Written informed consent was obtained from all participating patients and the studies were approved by the Institute of Tropical Medicine’s Institutional Review Board (1276/18 and 1351/20) and from the Ethics Committee of the University of Antwerp (19/06/058 and AB/ac/003). Our selection of isolates from these studies was biased towards N. mucosa and N. macacae, as in a previous phylogenetic study of 20, 047 Neisseria isolates, we found that these were the only two commensal Neisseria species which were donors of gyrB DNA into N. gonorrhoeae13. We also included a number of Neisseria isolates from reference collections (Suppl Table 1).
All methods were performed in accordance with the relevant guidelines and regulations. Briefly, suspensions from tenfold dilutions of the oropharyngeal swabs in PBS were inoculated on Neisseria commensal selective agar plates (LBVT.SNR). Species identity was confirmed via MALDI-TOF and whole genome sequencing (WGS) was carried out as detailed elsewhere17.
In vitro assays
Determination of the MIC
All the frozen isolates stored in skimmed milk at − 80 °C were revived on gonococcal base (GCB) agar (Gonococcal Medium Base, BD Difco™) supplemented with 1% IsoVitaleX (BD BBL™) and subcultured twice before starting the experiments.
Minimal inhibitory concentrations (MIC ≤ 0.015 to 16 µg/mL) for zoliflodacin (obtained from MedChemExpress) were determined on GCB agar in accordance with the CLSI methodology18. The WHO gonococcal reference strains F, P, X, Z and the ATCC strain 49,226 were included as the control isolates. The bacterial inoculum size was 104 colony-forming units. The inoculated plates were incubated at 36 °C in 5% CO2 with high humidity. MICs were read after 24 h of incubation.
Serial passage experiments
Briefly, the strains were inoculated on a GCB agar plate containing 0.015 mg/L zoliflodacin and incubated at 36 °C in an atmosphere of 5% CO2. After visible growth was attained, colonies from the GCB agar plate with 0.015 mg/L zoliflodacin were inoculated onto a GCB agar plate with a twofold higher zoliflodacin concentration compared to the previous plate (0.03 mg/L). This process was repeated for each strain until no visible growth was seen on cultured plates or growth was obtained on the plate with the final concentration of 16 µg/mL. The cultures from each time point were stored in skimmed milk (Skim Milk, BD Difco™) supplemented with 20% of glycerol and stored at − 80 °C.
Genomic DNA extraction and fragmentation
Suspensions of bacteria from overnight cultures on GC agar plates were prepared in 2 mL of phosphate buffered saline (PBS; pH 7.6). Genomic DNA extraction was carried out using the QIAamp DNA Mini kit (Qiagen, Hilden, Germany) following the manufacturer’s protocol for isolation of genomic DNA from bacterial cultures. DNA was eluted in a total volume of 300 µL Aqua SteropFlexo (Sterop group, Belgium) and stored at 4 °C for further use. The DNA concentration and purity was determined using the Nanodrop® ND-1000 spectrophotometer (Thermo Scientific, Waltham, MA, USA). A concentration of 100 ng/µL was used in subsequent experiments.
Samples of purified genomic DNA (gDNA) were sheared into short fragments using ultrasonication shearing to be used in transformation experiments19. After sonication, all samples were stored at 4 °C. The size of the gDNA fragments were assessed with the Agilent Tape station (Agilent Technologies, Waldbronn, Germany) and visualized on 1% agarose gel20.
PCR amplification of gyrB
PCR amplification of a 253 bp gyrB that included the resistance mutation at position D249 were amplified using the primer pairs gyrB-F1-1118-1353_Zoli (5ʹ-TCATCACCARCAAAATCGTC-3ʹ) and gyrB-R1-1118-1353_Zoli (5ʹ-ACCTTTGAGCGGCAAAATC-3ʹ). The primers were synthesized by Eurogentec (Seraing, Belgium). The PCR mixture consisted of 1× PE Buffer (Perkin–Elmer, Cetus, Norwalk, CT, USA), 2 mM MgCl2, 0.28 mM deoxyribonucleoside triphosphate (dNTP) (Pharmacia Biotech, St Albans, UK), 0.15 μM of primers, and 2 U of Taq polymerase (Perkin–Elmer, Cetus, Norwalk, CT, USA). 20 ng of DNA extract was added to the reaction mixture.
A one-step thermocycling protocol was carried out in a thermocycler (Perkin–Elmer, Cetus, Norwalk, CT, USA) as follows: Initial denaturation at 94 °C for 10 min, followed by 35 cycles of denaturation at 94 °C for 45 s (s), annealing at 54 °C for 45 s, and extension at 72 °C for 1 min (min). The final extension step was carried out at 72 °C for 5 min. The PCR amplicon (15 μL) was visualized via electrophoresis in a 1% agarose gel in 1× Tris–acetate-EDTA buffer (pH 8.5). The gel was stained with Gelred (0.5 mg/L; Sigma, Bornem, Belgium) and was photographed under short-UV light. The size of the amplified products was assessed by comparing with a 100 bp Smartladder marker (Eurogentec).
Intra- and inter-species transformation
Transformation of reduced zoliflodacin susceptibility isolates with fragmented genomic DNA
For intra-species transformation, the genomic DNA from the resistant strains that were generated via serial passage experiments were transformed into the susceptible wild-type strains from which the resistant strains were evolved (Table 2). For intra-species transformation, the WHO P N. gonorrhoeae recipient strain was transformed with genomic DNA from pools of two commensal strains each (Table 3). Transformations were conducted as described in Ref.8. Briefly, the strains were suspended in GCB broth (15 g/L protease peptone 3, 1 g/L soluble starch, 4 g/L dibasic K2HPO4, 1 g/L monobasic KH2PO4, 5 g/L NaCl) supplemented with 1% isovitalex, 10 µM MgSO4 and 2.5 µg of fragmented gDNA. The suspensions were incubated at 37 °C for 1h and plated on non-selective GCB agar plates overnight. The recovered transformants were then placed on selective GCB plates with 0.125, 1, 2 and 4 µg/mL of zoliflodacin for 18–24 h.
Transformation of PCR amplicon with zoliflodacin mutation
For intra- and inter-species transformation, the recipient strains were transformed with ~ 2.5 µg of PCR-purified products and the transformation was carried out as described above. The experiment was carried out for limited isolates (Table 3, Suppl Table 2).
Whole genome sequencing and analysis
The whole genome data available from the Resistogenicity, ComCom and PReGo studies were included in this study (Suppl Table 1). In addition, eight isolates, including isolates with zoliflodacin resistance determining mutations with confirmed phenotypic resistance from the serial passage (highest obtained MIC) and transformation experiments, as well as their wild-type baselines, were subjected to WGS (Table 2). WGS was outsourced to Eurofins (Konstanz, Germany). The Dneasy® Blood & Tissue Kit (Qiagen, Hilden, Germany) was used to extract genomic DNA, which was then suspended in nuclease-free water (Sigma-Aldrich, Seelze, Germany). Library preparation was carried out using Nextera XT DNA library prep kit followed by Illumina sequencing using paired-end 150-bp read sequencing chemistry (Illumina, San Diego, CA, USA). Raw reads that were generated were quality-controlled using FastQC (v0.11.9) and trimmed using Trimmomatic (v0.39)21,22. Shovill (v1.0.4, https://github.com/tseemann/shovill) was used to de novo assemble the wild-type baseline isolates, which were subsequently annotated with Prokka (v1.14.6)23. The consensus gyrB gene, encoding the DNA gyrase subunit B, was extracted, and reads of the isolates exhibiting zoliflodacin decreased susceptibility were mapped to their baseline using the Burrows-Wheeler Alignment Tool (v0.7.17-r1188) and Samtools (v1.9)24. Reference mappings were visualized using the Integrative Genomics Viewer (IGV, v2.5.3) to discover single-nucleotide polymorphisms (SNPs) compared to the baseline and to estimate the proportion of reads mutated25. Multiple sequence alignments of the gyrB were generated using MEGA software26. The raw reads are deposited at https://www.ncbi.nlm.nih.gov/sra/PRJNA926517.
The overview of the study is illustrated in Fig. 1.

Overview of the study. The figure was created using BioRender.
Statistics
Differences in MICs between groups were assessed using the Mann–Whitney test. Statistical analyses were performed using GraphPad Prism v9.
Results
Baseline MICs of Neisseria species isolates
In the absence of a breakpoint for zoliflodacin resistance, we classified a MIC of ≥ 4 µg/mL as resistantThe zoliflodacin MICs of N. cinerea (median 1 µg/mL, IQR 0.5–2 µg/Ml, n = 4; P < 0.0005), N. macacae (median 1 µg/mL, IQR 1–2 µg/mL, n = 15; P < 0.005), and N. mucosa (median 2 µg/mL, IQR 0.5–2 µg/mL, n = 30; P < 0.0005), were higher than those of N. gonorrhoeae (median 0.125 µg/mL, IQR 0.06–0.19 µg/mL, n = 5; Fig. 2; Suppl Table 1). The MICs of N. lactamica (median 0.25 µg/mL, IQR 0.125–0.5 µg/mL, n = 5) were similar to those of N. gonorrhoeae. The sample size for N. subflava was too small (n = 2) to warrant statistical testing.

Zoliflidacin MICs of 62 strains from 5 Neisseria species (**P < 0.001; ***P < 0.0001; ns non-significant).
Induction of zoliflodacin resistance
To induce zoliflodacin resistance, ten susceptible Neisseria isolates [N. lactamica (n = 1), N. cinerea (n = 1), N. macacae (n = 1), N. subflava (n = 2), N. mucosa (n = 3), and N. gonorrhoeae (n = 2)] were serially passaged on agar plates containing increasing zoliflodacin concentrations (Fig. 3). Within 7 to 10 days, all strains, except the N. lactamica strain, attained MICs of 4 µg/mL or higher, resulting in MIC increases ranging from 8- to 64-fold (Supplemental Table 1). There was only a two-fold increase in MIC for the N. lactamica strain (Fig. 3). The increase in MIC was most rapid in N. subflava 45/1, with the MIC increasing from 2 to ≥ 16 µg/mL in 3 days. The minimum time required for the emergence of zoliflodacin resistance was thus 3 days. The last passaged strains from the passage experiment and their baselines were subjected to WGS. In all strains, in vitro-induced zoliflodacin resistance was associated with mutations in the gyrB gene (Table 2). In N. subflava and N. gonorrhoeae, we detected mutations previously reported to cause zoliflodacin resistance, i.e. D429N and S467N. At position 467, we also identified a serine to glycine amino acid substitution in a N. cinerea strain, rather than the 467-asparagine resistance mutant described in the literature. Although we did not find the well-known K450N/T mutation, the consensus sequence reported an Isoleucine at position 450 in a N. cinerea strain. However, reference mapping revealed heteroresistance at this position, with 75% of the reads corresponding to K450I and 25% leading to K450N substitutions. Novel mutations, M464R and T472P, were discovered in the quinolone resistance-determining region (QRDR) of N. mucosa. Interestingly, we also observed novel mutations at amino acid positions 28 and 29 outside the QRDR in N. subflava and N. gonorrhoeae, respectively, that were the only genetic variants detected in gyrB in the resistant strains compared to their wild-type baseline. We found no evidence of multiple or multi-step mutations in gyrB.

Increase of zoliflodacin MICs during passage experiments using increasing concentrations of zoliflodacin for 10 strains from 5 Neisseria species. Zoliflodacin MICs were truncated at 16 µg/mL.
Intra-species transformation of zoliflodacin resistance determinants
The genomic DNA of the resistant strains was transformed into their own susceptible baseline strain. This procedure resulted in zoliflodacin MICs of 8 µg/mL or higher (Table 2). WGS of transformants with decreased zoliflodacin susceptibility revealed the presence of the same zoliflodacin resistance determinants as observed in the donor (Table 2). The WHO-P N. gonorrhoeae reference strain was exposed to a pool of genomic DNA of zoliflodacin-resistant N. gonorrhoeae WHO-P and ATCC strain 49226. Only the mutation found in the ATCC strain (S467N) was detected in the transformant’s sequence analysis (Table 2). Attempts to transform the PCR product of gyrB from zoliflodacin resistant N. gonorrhoeae ATCC 49226_8 and WHO-P_8 into N. gonorrhoeae WHO-P failed (Table S2).
Inter-species transformation of zoliflodacin resistance determinants
Three inter-species transformation experiments were conducted to investigate whether zoliflodacin resistance determinants of commensal Neisseria could be acquired by N. gonorrhoeae. N. gonorrhoeae reference strain WHO-P was exposed to pooled genomic DNA from the three resistant N. mucosa strains, resulting in a MIC of ≥ 16 µg/mL and uptake of the previously reported K450N mutation present in a proportion of the reads of the heteroresistant donor strain 801/1_8 (Table 3). No evidence of transformation was detected in equivalent experiments with the same donor strains but with N. gonorrhoeae, Res 18 as the recipient (Table 3).
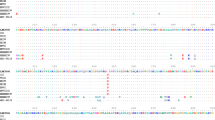
In the third experiment, the gyrB amplicon (253 bp) (Fig. 4) of the zoliflodacin resistant N. subflava strain 45/1_8 was used as the donor, and N. gonorrhoeae WHO-P as the recipient. The zoliflodacin MIC of N. gonorrhoeae WHO-P showed an increase from 0.125 to 216 µg/mL, and sequence alignment revealed that it had taken up a part of the gyrB amplicon of the resistant N. subflava strain 45/1_8 (Table 3, Fig. S1).

An image showing the PCR amplified gyrB (235 bp) in 1% agarose gel electrophoresis. GyrB was amplified from DNA of Ng (Neisseria gonorrhoeae; n = 2) and Ns (Neisseria subflava; n = 2). Milli Q. H2O was was used as a negative control.
gyrB mutations in circulating commensal Neisseria species
We found 7 mutations in gyrB that emerged in response to zoliflodacin selection pressure. We assessed if any of these mutations were present in the zoliflodacin MIC panel of commensal Neisseria species. None of these strains had any of these mutations. We did however find a different single amino acid substitution at position 472. T472P mutation that was followed by a 32-fold increase in zoliflodacin MIC, emerged in N. mucosa DSM4631. We found two strains of N. lactamica (CO000761/1, CO000771/1) and three strains of N. cinerea (CO000776/4, CO000782/1) that had T472A substitution. This single amino acid change was not associated with zoliflodacin MICs (Mann–Whitney test, P > 0.05 for both species).
Discussion
We found that the zoliflodacin MICs of N. cinerea, N. macacae and N. mucosae were higher than those of N. gonorrhoeae. Our passage experiments revealed that zoliflodacin resistance could be induced in all species assessed—an 8- to 64-fold increase within 7 to 10 days. Finally, we were able to transform zoliflodacin resistance both within and between Neisseria species. Of particular concern, transformation experiments revealed that N. gonorrhoeae could obtain zoliflodacin resistance from N. subflava—the most prevalent commensal Neisseria species.
As noted above, transformation of resistance from commensal Neisseria spp. into N. gonorrhoeae has been instrumental in the emergence of cephalosporin, sulfonamide and macrolide resistance8,9,10,11. Transformation from commensal Neisseria has also been found to be responsible for fluoroquinolone resistance in over half the N. meningitidis isolates in one study from China12. Our findings support the possibility that gonococcal resistance to zoliflodacin could emerge via resistance in commensal Neisseria. Because commensal Neisseria such as N. subflava are a key component of a healthy oropharyngeal microbiome they are present in almost all individuals14,27. This high prevalence means they are at considerably greater risk for bystander selection—the emergence of AMR in response to antimicrobials taken for other indications28. The broader the range of infections that zoliflodacin is used to treat, the higher the risk of this bystander selection. Even if the use of zoliflodacin is restricted to STIs such as N. gonorrhoeae and M. genitalium, the high prevalence of these infections in high risk groups such as HIV PrEP cohorts (around 10–15% for both infections29,30), will translate into high zoliflodacin exposure within these groups. The higher prevalence of commensal than pathogenic Neisseria in these groups will mean that the commensals are under a greater selection pressure to acquire resistance to zoliflodacin. This effect may be particularly prominent for zoliflodacin on commensal Neisseria as the penetration of zoliflodacin in the oropharynx appears to be particularly poor. Poor oropharyngeal penetration of zoliflodacin is the most plausible explanation for the lower cure rates for gonorrhoea in the pharynx (50%) than urogenital sites (96%)1.
In this study we found that the zoliflodacin MICs of N. mucosa, N. macacae and N. cinerea were higher than those in N. gonorrhoeae. These higher MICs could not be explained by established gyrB resistance associated mutations. It should also be noted that other studies have found that the known zoliflodacin resistance associated mutations are not able to fully explain differences in zoliflodacin MICs. For example, a study of 986 gonococcal isolates collected in China between 2014 and 2018 found a doubling in MIC50 and MIC90 over the time period, but no known zoliflodacin RAMs were detected31. We found that zoliflodacin resistance can emerge fairly rapidly within commensal Neisseria species and be transformed into N. gonorrhoeae. These results suggest it may be prudent to include surveillance of zoliflodacin susceptibility in commensal Neisseria in clinical trials and programmes using this agent. This suggestion would fit into calls to include surveillance of antimicrobial susceptibility of commensal Neisseria within gonococcal surveillance programmes such as Euro-GASP7,32.
There are a number of limitations to this study. Our study only used a limited number of strains from a small number of commensal species. We did not include N. meningitidis. The main gyrB mutations we found to be implicated in zoliflodacin resistance are well-established in previous studies. We did however find two additional gyrB mutations which may increase zoliflodacin MICs. However, we were unable to prove this effect experimentally. Additionally, we would like to acknowledge that several aspects were not assessed in our study. We did not determine the mutation frequency and the stability of the induced zoliflodacin resistance, assess the transformation efficacy, explore potential fitness effects associated with induced zoliflodacin resistance, or investigate cross-resistance to other antimicrobials. These are important considerations that should be addressed in future studies to gain a more comprehensive understanding of zoliflodacin resistance. Furthermore, it is crucial to acknowledge that in vitro induced mutations may not fully represent the mutations that develop in vivo. While our study provides insights into the potential mechanisms of zoliflodacin resistance, the translation of these findings to clinical settings requires further investigation.
Transformation efficacy between Neisseria spp. is heavily influenced by the similarity of the direct uptake sequences (DUS) of the recipient and donor33. Analyses have revealed the existence of eight families of DUS sequence with the Neisseriaceae family33. N. gonorrhoeae is from the same DUS family (AT-DUS) as N. meningitidis, N. lactamica, N. polysaccharea and N. cinerea33. The N. mucosa and N. subflava used in the transformation experiments are from the closely related to AG-DUS family33. Thus the fact that the donor species used in the transformation experiments were from a different DUS family to N. gonorrhoeae may be considered as further study limitation.
Notwithstanding these limitations, this is the first study to report that zoliflodacin resistance can be induced in commensal Neisseria and subsequently acquired by N. gonorrhoeae via transformation. This finding has important implications for how we introduce this novel antimicrobial and how we monitor for the emergence of zoliflodacin resistance.
Data availability
All data generated or analysed during this study are included in this published article and its Supplementary Information files. Please see: https://www.ncbi.nlm.nih.gov/sra/PRJNA926517.
References
Taylor, S. N. et al. Single-dose zoliflodacin (ETX0914) for treatment of urogenital gonorrhea. N. Engl. J. Med. 379(19), 1835–1845 (2018).
Bradford, P. A., Miller, A. A., O’Donnell, J. & Mueller, J. P. Zoliflodacin: An oral spiropyrimidinetrione antibiotic for the treatment of Neisseria gonorrheae, including multi-drug-resistant isolates. ACS Infect. Dis. 6(6), 1332–1345 (2020).
Adamson, P. C., Lin, E. Y., Ha, S.-M. & Klausner, J. D. Using a public database of Neisseria gonorrhoeae genomes to detect mutations associated with zoliflodacin resistance. J. Antimicrob. Chemother. 76, 2847 (2021).
Foerster, S. et al. In vitro antimicrobial combination testing of and evolution of resistance to the first-in-class spiropyrimidinetrione zoliflodacin combined with six therapeutically relevant antimicrobials for Neisseria gonorrhoeae. J. Antimicrob. Chemother. 74(12), 3521–3529 (2019).
Foerster, S. et al. Genetic resistance determinants, in vitro time-kill curve analysis and pharmacodynamic functions for the novel topoisomerase II inhibitor ETX0914 (AZD0914) in Neisseria gonorrhoeae. Front. Microbiol. 6, 1377 (2015).
Alm, R. A. et al. Characterization of the novel DNA gyrase inhibitor AZD0914: Low resistance potential and lack of cross-resistance in Neisseria gonorrhoeae. Antimicrob. Agents Chemother. 59(3), 1478–1486 (2015).
Kenyon, C., Laumen, J. & Manoharan-Basil, S. Choosing new therapies for Gonorrhoea: We need to consider the impact on the pan-Neisseria genome. A viewpoint. Antibiotics 10(5), 515 (2021).
Wadsworth, C. B., Arnold, B. J., Sater, M. R. A. & Grad, Y. H. Azithromycin resistance through interspecific acquisition of an epistasis-dependent efflux pump component and transcriptional regulator in Neisseria gonorrhoeae. Mbio 9(4), 18. https://doi.org/10.1128/mBio.01419-18 (2018).
Kanesaka, I., Ohno, A., Katsuse, A. K., Takahashi, H. & Kobayashi, I. The emergence of the ceftriaxone-resistant Neisseria gonorrhoeae FC428 clone by transfer of resistance from an oral Neisseria subflava reservoir of resistance. J. Antimicrob. Chemother. 77, 364 (2021).
Vigue, L. & Eyre-Walker, A. The comparative population genetics of Neisseria meningitidis and Neisseria gonorrhoeae. PeerJ 7, e7216 (2019).
Manoharan-Basil, S. S. et al. Evidence of horizontal gene transfer of 50S ribosomal genes rplB, rplD, and rplY in Neisseria gonorrhoeae. Front. Microbiol. 12, 1263 (2021).
Chen, M., Zhang, C., Zhang, X. & Chen, M. Meningococcal quinolone resistance originated from several commensal Neisseria species. Antimicrob. Agents Chemother. 64, 10 (2019).
Manoharan-Basil, S. S., Gonzalez, N., Laumen, J. & Kenyon, C. Horizontal gene transfer of fluoroquinolone resistance-conferring genes from commensal Neisseria to Neisseria gonorrhoeae: A global phylogenetic analysis of 20,047 isolates. Front. Microbiol. 13, 225 (2022).
Laumen, J. G. E. et al. Antimicrobial susceptibility of commensal Neisseria in a general population and men who have sex with men in Belgium. Sci. Rep. 12(1), 1–10 (2022).
de Block, T. et al. WGS of commensal Neisseria reveals acquisition of a new ribosomal protection protein (MsrD) as a possible explanation for high level azithromycin resistance in Belgium. Pathogens 10(3), 384. https://doi.org/10.3390/pathogens10030384 (2021).
Van Dijck, C. et al. Antibacterial mouthwash to prevent sexually transmitted infections in men who have sex with men taking HIV pre-exposure prophylaxis (PReGo): A randomised, placebo-controlled, crossover trial. Lancet Infect. Dis. 21(5), 657–667 (2021).
Laumen, J. G. E. et al. Antimicrobial susceptibility of commensal Neisseria in a general population and men who have sex with men in Belgium. Sci. Rep. 12(9), 1 (2022).
CLSI. Performance Standards for Antimicrobial Susceptibility Testing CLSI Supplement M100 30th edn. (Clinical and Laboratory Standards Institute, 2020).
Elsner, H. I. & Lindblad, E. B. Ultrasonic degradation of DNA. DNA 8(10), 697–701 (1989).
Sambrook, J. & Russell, D. W. Agarose gel electrophoresis. Cold Spring Harbor Protoc. 2006(1), 4020 (2006).
Andrews, S. FastQC: A Quality Control Tool for High Throughput Sequence Data (Babraham Bioinformatics, Babraham Institute, 2010).
Bolger, A. M., Lohse, M. & Usadel, B. Trimmomatic: A flexible trimmer for Illumina sequence data. Bioinformatics 30(15), 2114–2120 (2014).
Seemann, T. Prokka: Rapid prokaryotic genome annotation. Bioinformatics 30(14), 2068–2069 (2014).
Li, H. & Durbin, R. Fast and accurate short read alignment with Burrows–Wheeler transform. Bioinformatics 25(14), 1754–1760 (2009).
Robinson, J. T. et al. Integrative genomics viewer. Nat. Biotechnol. 29(1), 24–26 (2011).
Stecher, G., Tamura, K. & Kumar, S. Molecular evolutionary genetics analysis (MEGA) for macOS. Mol. Biol. Evol. 37(4), 1237–1239 (2020).
Caselli, E. et al. Defining the oral microbiome by whole-genome sequencing and resistome analysis: The complexity of the healthy picture. BMC Microbiol. 20(1), 120. https://doi.org/10.1186/s12866-020-01801-y (2020).
Tedijanto, C., Olesen, S. W., Grad, Y. H. & Lipsitch, M. Estimating the proportion of bystander selection for antibiotic resistance among potentially pathogenic bacterial flora. Proc. Natl. Acad. Sci. U.S.A. 115(51), E11988–E11995. https://doi.org/10.1073/pnas.1810840115 (2018).
Kenyon, C., Vanbaelen, T. & Van Dijck, C. Recent insights suggest the need for the STI field to embrace a more eco-social conceptual framework: A viewpoint. Int. J. STD AIDS 33, 404 (2022).
Tsoumanis, A., Hens, N. & Kenyon, C. R. Is screening for chlamydia and gonorrhea in men who have sex with men associated with reduction of the prevalence of these infections? A systematic review of observational studies. Sex Transm. Dis. 45(9), 615–622 (2018).
Le, W. et al. Susceptibility trends of zoliflodacin against multidrug-resistant Neisseria gonorrhoeae clinical isolates in Nanjing, China, 2014 to 2018. Antimicrob. Agents Chemother. 65(3), e00863 (2021).
Goytia, M. & Wadsworth, C. B. Canary in the coal mine: How resistance surveillance in commensals could help curb the spread of AMR in pathogenic Neisseria. Mbio 13(5), e01991 (2022).
Frye, S. A., Nilsen, M., Tønjum, T. & Ambur, O. H. Dialects of the DNA uptake sequence in Neisseriaceae. PLoS Genet. 9(4), e1003458 (2013).
Lahra, M. M., Limnios, A., Sikora, A. E., Wi, T. & Harris, S. R. The novel 2016 WHO Neisseria gonorrhoeae reference strains for global quality assurance of laboratory investigations: Phenotypic, genetic and reference genome characterization. J. Antimicrob. Chemother. 71, 3096–3108 (2016).
Author information
Authors and Affiliations
Contributions
S.A., J.L., S.M.B. and C.K. conceptualized the study. J.L. and S.A. conducted the experiments. J.L., S.A., S.M.B. and C.K. were responsible for the acquisition, analysis and interpretation of the analyses. C.K., J.L., S.A. and S.M.B. wrote the first draft, and all authors (C.K., J.L., S.A., T.D.B., C.V.D., I.D.B., D.V.D.B. and S.M.B.) read and approved the final draft.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Abdellati, S., Laumen, J.G.E., de Block, T. et al. Gonococcal resistance to zoliflodacin could emerge via transformation from commensal Neisseria species. An in-vitro transformation study. Sci Rep 14, 1179 (2024). https://doi.org/10.1038/s41598-023-49943-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-49943-z
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
