
Abstract
The aim of this study was to examine the effectiveness of a stress management educational intervention programme based on the Transactional Model of Stress and Coping (TMSC) among industrial workers. Participants were 106 employees of a power plant in Iran, randomly assigned into an intervention group and a control group. The intervention comprised active and participatory methods to enhance employees coping skills and it was delivered in six face-to-face sessions. Data was collected using the Ways of Coping Questionnaire, the Multidimensional Scale of Perceived Social Support, the Perceived Stress Scale, and the Spiritual Well-Being Scale at baseline and three months after the intervention. We found mean scores of distancing, self-controlling, seeking social support, escape-avoidance, planned problem-solving, positive reappraisal, total coping skills, perceived social support, and spiritual well-being significantly differed at follow-up compared to baseline in the intervention group, but not in the control group. There was also a significant difference in the mean score of perceived stress between the two groups. We conclude that the educational intervention based on the TMSC was effective in improving coping skills and reducing perceived stress. We suggest that interventions based on the TMSC model can be supportive in workplaces where job stress is common.
Similar content being viewed by others


Introduction
Employees are exposed to a range of physical and psychosocial risks at their workplaces according to occupation1. Job stress is associated with various negative outcomes at both individual and organizational levels. There is consensus in the literature that occupational stress can be described as a perceived imbalance of the demands of a job and the individual’s resources to meet those requirements2,3. Similarly, adequate management of a potential gap between the one’s capabilities and the demands of the job is an ability to cope3, and failing to cope with one’s work demands has the potential for harmful physical and emotional outcomes as a result of chronic triggering of the stress response2. There is a significant accumulation of evidence of the physiological processes that show how stress mediates the onset and impact of various disease states, and similarly, there is evidence of a connection of psychosocial stressors supporting negative health outcomes, and dysfunction in the workplace4. These problems, in turn, increase the rates of absenteeism and presenteeism, poor work performance, accident and injury, and low productivity5.
Stress management is a poorly defined concept6 and thus a variety of practical techniques have been used to cope with occupational and life stressors to prevent or ameliorate negative physical and psychological consequences7. In practice, stress management interventions can be used at the organisational level, at the individual level, and the interface of individual and organisation8. Similarly, distinctions have been made regarding primary, secondary and tertiary interventions7, with a strong argument that a risk assessment approach to manage stressors in the workplace is a legal duty for employers, and thus has to be a part of the stress management actions4. Nevertheless, although organisational changes can be made to ameliorate stressors in some workplaces9, there are also inherent stressors in some occupations, and there are differences in how individuals perceive events as stressful3,10. That is, subjective factors are critical to the experience of stress. Factors such as self-efficacy, optimism, social support from co-workers, supervisors and family, and participation in decision-making have positive effects on coping with stressors in the workplace11. Critically, there are substantial benefits for an organisation through empowering employees with skills to cope with inherent stressors from both work and life. Whilst it is not appropriate to establish training programmes that simply serve to adapt workers to poorly designed job2, equally, stress management methods should not be abandoned when they seek to tackle secondary, individual aspects of coping with stressors on a job in a dynamic workplace7,12. Following from this, we discerned a need to develop an effective education programme for industrial workers through reference to established scientific research in the area of stress and coping. There is a strong business case for promoting mental health in the workplace, and providing coping skills training can be considered a practical and cost-effective method to reduce job stress and increase the psychological well-being of employees, ultimately increasing their physical and mental health5.
The conceptualisation of coping in the context of stress has for many years revolved around the work of Lazarus and Folkman. Their Transactional Model of Stress and Coping (TMSC) illustrates how stress and coping is a process based on changing cognitive appraisals of a given situation and one’s resources3. Appraisals (primary and secondary) and coping efforts are the two main components of a dynamic transactional process between the person and their environment. If their situation is perceived as threatening, then the person appraises their ability to deal with that threat, and from there takes a coping strategy that is largely problem-focused or emotion-focused. Essentially then, coping has two major functions: to regulate harmful emotions, and to change the negative person-environment relationship that has produced the distress13. The appropriateness and quality of coping efforts determines outcomes, including adaptation, emotional wellness, functional status, or behaviour change, accepting that there are several variables can mediate the process of coping. In particular, social support and meaning-based thinking, like positive reappraisal and spiritual beliefs, are among the important mediating factors that should be considered when planning education programmes to support the development of stress coping skills [3. 10. 12].
There is evidence to suggest that educational health promotion programmes are effective interventions for stress management in the workplace. For example, a rational-emotive health education intervention used to coach technical college teachers’ in Nigeria, significantly decreased the stress of the intervention group compared to a control group14. Similarly, using a sample of distressed managers across several work sectors, Asplund et al.15 showed that a guided internet-based stress management intervention in a randomized controlled trial reduced stress and improved other mental-related and work-related health symptoms compared to a control group both post-test and at a six-month follow-up. Also, an evaluation of a mobile-app based stress management intervention found a reduction in perceived stress in highly stressed workers, if no improvement in anxiety, depression or work engagement16. Relatively few studies, however, have used the TMSC as a framework for managing stress in the workplace. One exception is a quasi-experimental study of healthcare workers in Iran (n = 84) in which half the sample received a transactional model-based education programme17. When compared to controls, follow-up scores of the intervention group indicated significantly improved coping strategies. A second study examined the efficacy of an education programme delivered on the internet to a sample of 26 American teachers to manage burnout18. One week after the 4-week education programme was completed, there was a significant increase in healthy coping strategies as measured by the Maslach Burnout Inventory-Educator Survey for the intervention group and no change in the control group (n = 25). The authors suggest that their study confirms that the TMSC framework provides an appropriate approach to develop interventions to increase healthy coping strategies in the teaching profession.
To our knowledge, there remains a need to provide supportive stress interventions beyond the teaching profession, including employees working in large industrial power plants. To our knowledge, no study has assessed the effect of a transactional model-based education programme on stress management and coping skills of industrial workers. Therefore, the purpose of this study was to investigate the effect of a health promotion educational intervention based on the TMSC on stress management and coping skills among industrial workers in Iran.
Method
The Scientific and Ethics Committee of Shiraz University of Medical Sciences approved the study protocol (IR.SUMS.REC.1399.372). The research was conducted in accordance with the Declaration of Helsinki, and all participants provided written informed consent.
Study design and participants
This study used a randomized controlled trial (RCT) design with a 1:1 ratio. Participants were employees of a combined cycle power plant in Iran. The company had 211 employees at the time of the study, all employees worked one of two teams, each working rotating 12-h shifts. Inclusion criteria were having more than one year of job tenure, no history of stress management education, and no history of psychiatric treatment, determined through participants’ self-report. Exclusion criteria included absence from two educational sessions, not attending the pre-test or post-test sessions, withdrawal from the study, and undergoing treatment by a psychiatrist due to mental illness during the intervention. 194 employees were eligible to participate, however some declined to participate leaving a consenting sample of 170 employees. A sample size calculation was calculated based on the effect size (0.58) provided by Faryabi et al.17 which indicated that a 1:1 group size of 48 was sufficient at an alpha set at 0.05, and a beta of 0.2 / power of 0.80. To account for potential atrophy at follow-up, we increased recruitment by 10%, and recruited 53 to the two groups in the study. To prevent or mitigate contamination and bias in this per-protocol study, we randomly selected one work shift as the intervention group and the other as the control group using a tossed coin. Random allocation of potential participants from each shift was then undertaken using an Excel spreadsheet programme that permitted sampling by shuffling the population19. Hence a random sample of 53 employees was allocated to the study from the consenting sample in each of the two shifts.
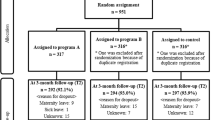
Data was collected at baseline, and three months after the 6-weeks educational intervention period had been completed. All participants completed the anonymous study questionnaires on the same day at baseline, and the same day at the follow-up, except for three participants in the intervention group who did not provide data at the three-month follow-up. This gave a final sample for data analysis of 103 participants. Figure 1 shows the flow of the participants throughout the study, based on the Consolidated Standards of Reporting Trials (CONSORT)20.

Consort flow diagram of the study. 211 employees who participants worked one of two 12-hour shifts in an industrial plant were invited into the study. 170 gave informed consented. One shift was randomly allocated as the educational intervention group the other was the control group. From potential participants 53 participants were randomly allocated into each study group. Three participants dropped out of the Intervention Group before the three-months post-intervention follow-up which was on the same day for both groups. Thus, data was analysed from 50 participants in the Intervention group and compared with 53 participants in the control group.
Measures
Demographic information
Demographic variables—age, sex, marital status, education level, job tenure, and employment status—were assessed at baseline.
Ways of coping questionnaire (WCQ)
WCQ is an established measure based on Lazarus and Folkman’s process-oriented stress and coping theory. It was originally developed with 68 items to identify the coping strategies people use in stressful situations2. Further work from this lab identified eight types of emotion- and problem-based coping, across 66 items. These are confrontive coping, distancing, self-controlling, seeking social support, accepting responsibility, escape-avoidance, planned problem-solving, and positive reappraisal13. Various versions of the questionnaire exist according to the setting in which it is being used. In this study participants were first asked about a stressful situation related to work that occurred during the previous week. Participants were then asked how extensively they used a given coping strategy in relation to that situation using a four-point scale from 0 (not used) to 3 (used a great deal) for each of the 66 items. Responses are totalled for each of the eight subscales and the total WCQ. The psychometric properties of the Persian version of this questionnaire have been confirmed22. Cronbach’s alpha coefficient was 0.89 for the total questionnaire in the study.
Multidimensional scale of perceived social support (MSPSS)
MSPSS23 is a brief questionnaire of perceived adequacy of social support. It includes 12 items that enquire after the perceived adequacy of family, friends and significant others (four items for each subscale), using a seven-point Likert scale (1 = very strongly disagree, 7 = very strongly agree). A higher score equates with higher perceived social support. The psychometric properties of the Persian version of this questionnaire have been confirmed24. Cronbach’s alpha coefficient for the questionnaire was 0.82.
Perceived stress scale (PSS-10)
PSS-1025 is a tool that measures the extent to which life events are appraised as stress provoking in terms of overload, lack of control and poor predictability. It is widely used in many settings including general population and occupational investigations. Each of the ten items asks how often in the past month participants have been stressed by a situation. For example, upset about an unexpected event, or confident about their ability to hand a personal problem. All items were scored using a five-point Likert scale (0 = never, 4 = very often) and the four positively worded items were reverse scored, such that higher scores indicate higher stress. The psychometric properties of the Persian version of PSS-10 were confirmed26. In this study Cronbach’s alpha coefficient was 0.91.
Spiritual well-being scale (SWBS)
SWBS27 is a 20-item indicator of the quality of life in the sphere of spiritual well-being. It includes 10 items associated with religious well-being, and one’s relationship with God, and 10 items measuring existential well-being, and a one’s understanding of the purpose of life. The SWBS uses a six-point Likert-type scale (1 = strongly agree, 6 = strongly disagree), with some items reversed so that high scores indicate more well-being. The SWBS provides three scores; in this study only the total SWBS score was used. The psychometric properties of the Persian version of the scale were confirmed28. Cronbach’s alpha coefficient was 0.78 for the total questionnaire.
Educational intervention programme
The intervention consisted of six face-to-face educational sessions held for the intervention group—which was divided into six subgroups. Each of the six weekly sessions lasted 1.5–2 h. The training programme is outlined in Table 1. A WhatsApp group was created for each subgroup to provide supplementary information and short video clips.
All the educational content was provided to the control group after the analysis of the intervention.
Data analysis
In both evaluation phases, histograms and the Kolmogorov–Smirnov test were first used to check the distribution and skewness of data. The dependent variables were all normally distributed, thus, chi-square, t-tests, and analyses of covariance (ANCOVA) were used to compare the data. All analyses were performed using SPSS version 23 software (SPSS Inc., Chicago, IL, USA). A p-value ≤ 0.05 represented statistical significance.
Results
Mean age was 35.88 (SD = 5.22) years and ranged from 27 to 50 years in the intervention group (n = 50); mean age was 36.42 (SD = 5.99) years and ranged 25 to 52 years in the control group (n = 53). Mean job tenure ranged from 1 to 27 years with an average of 8.34 (SD = 6.47) years in the intervention group and ranged from 1 to 28 years with an average of 8.92 (SD = 6.24) years in the control group. Table 2 shows the baseline demographic characteristics of the study participants. The distributions of age, marital status, education level, job tenure, and employment status did not significantly differ between the two groups at baseline. As there was a difference between the two groups regarding sex, this variable was included in subsequent analyses as a covariate.
Statistical analyses showed that mean scores of confrontive coping (t = − 0.226, p = 0.822), distancing (t = 0.438, p = 0.662), self-controlling (t = − 0.345, p = 0.730), seeking social support (t = − 0.187, p = 0.852), accepting responsibility (t = − 1.60, p = 0.113), escape-avoidance (t = 0.151, p = 0.881), planned problem-solving (t = − 0.313, p = 0.755), positive reappraisal (t = 0.510, p = 0.611), total WCQ score (t = − 0.324, p = 0.747), perceived social support (t = − 0.450, p = 0.654), and spiritual well-being (t = 0.985, p = 0.327) did not significantly differ between two groups at baseline (see Table 3). However, at the three-month follow-up, a significant change in terms of coping strategies, spiritual well-being, and perceived social support was observed in the intervention group compared to the control group. Statistical analyses showed that the mean scores of distancing (t = 6.01, p < 0.001), self-controlling (t = 2.84, p = 0.005), seeking social support (t = 5.70, p < 0.001), escape-avoidance (t = − 2.17, p = 0.032), planned problem-solving (t = 5.12, p < 0.001), positive reappraisal (t = 6.07, p < 0.001), total WCQ score (t = 5.17, p < 0.001), perceived social support (t = 2.77, p = 0.007), and spiritual well-being (t = 4.06, p < 0.001) were significantly different between the two groups at the three-month follow-up.
Paired-samples t-tests revealed that, unlike the control group, the mean score difference (MSD) of distancing (MSD = 2.88, t = − 6.60, p < 0.001), self-controlling (MSD = 2.28, t = − 4.04, p < 0.001), seeking social support (MSD = 5.30, t = − 7.10, p < 0.001), escape-avoidance (MSD = 2.28, t = 3.70, p < 0.001), planned problem-solving (MSD = 3.32, t = 6.48, p < 0.001), positive reappraisal (MSD = 5.42, t = − 7.13, p < 0.001), total WCQ (MSD = 25.12, t = − 6.43, p < 0.001), perceived social support (MSD = 10.46, t = − 5.57, p < 0.001), and spiritual well-being (MSD = 16.48, t = − 6.85, p < 0.001) at the three-month follow-up were significantly different from the mean scores at baseline in the intervention group. In both intervention and control groups the mean score of perceived stress was significantly reduced at the three-month follow-up compared to baseline. However, the MSD was 1.87 in the control group and 4.92 in the intervention group, showing a statistically significant difference (t = − 2.96, p = 0.004).
Finally, we performed ANCOVA to be sure that sex and baseline values did not significantly change the results. As can be seen in Table 3, there was no significant change in the results.
Discussion
This randomized controlled trial assessed the effect of an educational intervention based on the TMSC on stress management and coping skills among industrial workers in Iran. The results suggest that the educational intervention could significantly improve coping skills strategies, spiritual well-being, and perceived social support, and decrease perceived stress among industrial workers. This original study is the first to use an educational intervention based on the robust TMSC to help industrial workers cope with stress through the development of appropriate stress coping skills.
The significant impact of the educational programme on coping skills in the present study aligns with previous research in other working populations17,18. A review of extant literature confirmed that no study has particularly addressed educational interventions based on the TMSC to promote coping skills in industrial workers. Among the studied coping skills, the biggest improvement in the intervention group was observed in positive reappraisal. This emotion-regulation strategy essentially involves reinterpreting an experience to deliberately seek out positive meaning when a situation has previously been recognised as negative for self29. A positive reappraisal is often the first step towards re-engagement with a stressor event, and developing such coping strategies enables a person to reduce the negative impact of stressors in their life30.
Seeking social support was another coping skill that was increased in the intervention group. This problem-focused coping skill intentionally pursues practical, informational and emotional support from relevant others to relieve the particular stressor which is challenging in one’s life31. Positive perceptions of one’s social support is associated with better psychological well-being, physical health, and quality of life, and have been shown to buffer individuals against the adverse effects of stressful events31. In this regard, the results indicated a significant improvement in perceived social support in the intervention group. The educational programme designed to improve seeking social support, small group discussions, and the WhatsApp social media group may have helped improve group dynamism and promote perceived social support among the workers in the intervention group.
The present study showed a remarkable change in spiritual well-being when the measure was repeated after the intervention. Drawing upon one’s beliefs and understanding of the holistic purpose of life can be recognised as adaptive, and a positive coping strategy in the face of considerable suffering32. This underlying factor is not considered in the original TMSC model. Nevertheless, in the present study, the effect of the educational intervention on spiritual well-being was evaluated using a valid and standard tool, and was seen to make an important contribution to stress coping skills. This is in line with arguments that spiritual well-being is important, and a predictor of the levels of subsequent happiness, psychological well-being, and stress. That is, spiritual well-being has a significant impact on stress coping skills and health promotion behaviours32,33,34.
One of the most important results of the present study was that the educational programme reduced perceived stress even when measured three months after the intervention, suggesting some longevity to the principles of the TMSC programme. We acknowledge that an assertion that this programme could empower industrial workers to cope with stressors in the long term requires additional data collection, perhaps after two years, as it is well-known that there are skills decay over time, even when used regularly35. It has been suggested that a regular ‘refresher’ educational session may provide sustainability for the long-term for skills programmes36. Critically, there is evidence that this is so from a skills-based training programme for midwives which found that a two-session refresher course provided one-year after the initial training minimised the decay four months after the refresher course, compared with participants who did not have the refresher course37. Altogether, additional follow-up in future studies will further endorse the benefits of providing education programmes for enhancing stress-coping skills in industrial workers, and whether refreshers are additionally supportive.
The present study is the first to describe the effect of an educational intervention based on the comprehensive and standard method of TMSC among industrial workers. This RCT study produced causal evidence of the role stress coping skills training can contribute to industrial workers’ well-being. In this study, we measured spiritual well-being in addition to eight coping skills of the TMSC model. The simultaneous use of face-to-face and virtual education is one of the other strengths of the study.
Despite the strengths of the study, it also has some limitations. This study was conducted in one Iranian industrial company and may not generalize to other industrial work environments, or culturally diverse environments. Self-reported questionnaires were used to gather study variables, which may have been accompanied by some bias despite the full explanation provided to the participants at the beginning of the study as an attempt to gain their trust. The lack of long-term outcome assessment may also be considered another limitation of the present study. Finally, despite trying to prevent or mitigate contamination, selecting one work shift as the intervention group and the other as the control group might be contamination.
Conclusion
This study provides evidence of the effectiveness of an educational intervention based on TMSC for improving coping skills and spiritual well-being. The improvement in coping skills had a positive effect on increasing perceived social support and reducing perceived stress. Altogether, these results suggest that an educational intervention programme based on a systematic framework, such as the TMSC, and on-site interventions can effectively improve employees' quality of life. Therefore, it is suggested that educational interventions be implemented based on standard and valid models such as TMSC in other work environments given the ubiquity of job stress.
Data availability
Data associated with this study is available upon reasonable request to the corresponding author.
References
Mokarami, H., Gharibi, V., Kalteh, H. O., Faraji Kujerdi, M. & Kazemi, R. Multiple environmental and psychosocial work risk factors and sleep disturbances. Int. Arch. Occup. Environ. Health 93, 623–633 (2020).
Cox, T. Stress (Macmillan, 1978).
Lazarus, R. S. & Folkman, S. Stress, appraisal, and coping (Springer, 1984).
MacKay, C. J., Cousins, R., Kelly, P. J., Lee, S. & McCaig, R. H. “Management Standards” and work-related stress in the UK: Policy background and science. Work Stress. 18, 91–112 (2004).
Brunner, B., Igic, I., Keller, A. C. & Wieser, S. Who gains the most from improving working conditions? Health-related absenteeism and presenteeism due to stress at work. Euro J. Health Econom. 20, 1165–1180 (2019).
Ong, L., Linden, W. & Young, S. Stress management. What is it?. J. Psychosom. Res. 56, 133–137 (2004).
Murphy, L. R. Occupational stress management: A review and appraisal. J. Occup. Org. Psychol. 57, 1–15 (1984).
De Frank, R. S. & Cooper, C. L. Worksite stress management interventions: Their effectiveness and conceptualisation. J. Manag. Psychol. 2, 4–10 (1987).
Cousins, R. et al. “Management Standards” and work-related stress in the UK: Practical development. Work Stress. 18, 113–136. https://doi.org/10.1080/02678370410001734322 (2004).
Lazarus, R. S. Psychological stress and the coping process (McGraw-Hill, 1966).
Van den Brande, W., Baillien, E., De Witte, H., Vander Elst, T. & Godderis, L. The role of work stressors, coping strategies and coping resources in the process of workplace bullying: A systematic review and development of a comprehensive model. Aggress. Violent Behav. 29, 61–71 (2016).
Parkes, K. R. Coping in stressful episodes: The role of individual differences, environmental factors and situational characteristics. J. Personal Soc. Psychol. 51, 1277–1292 (1986).
Folkman, S., Lazarus, R. S., Dunkel-Schetter, C., DeLongis, A. & Gruen, R. J. Dynamics of a stressful encounter: Cognitive appraisal, coping, and encounter outcomes. J. Personal Soc. Psychol. 50, 992–1003 (1986).
Ugwoke, S. C. et al. Effects of a rational-emotive health education intervention on stress management and irrational beliefs among technical college teachers in Southeast Nigeria. Med (Baltimore). 96, e7658. https://doi.org/10.1097/MD.00000000007658 (2017).
Asplund, P. R. et al. Internet-based stress management for distressed managers: results from a randomised controlled trial. Occup. Environ. Med. 75, 105–113 (2018).
Lee, Y. J. Effects of a mobile health intervention on activities of stress self-management for workers: A randomized controlled trial. Work https://doi.org/10.3233/WOR-211406 (2022).
Faryabi, R., Mirzayi, R., Salari, E. & Javadi, A. Investigating the effect of education based on Lazarus and Folkman’s transactional stress model on coping skills of Jiroft university sciences health care workers. J. Jiroft Univ. Med. Sci. 3, 120–129 (2016).
Ansley, B. M. et al. The impact of an online stress intervention on burnout and teacher efficacy. Teaching Teacher Educ. 98, 103251. https://doi.org/10.1016/j.tate.2020.103251 (2021).
Siegel, A. F. & Wagner, M. R. Practical business statistics (Academic Press, London, 2022).
Moher, D. et al. CONSORT 2010 explanation and elaboration: Updated guidelines for reporting parallel group randomised trials. Int. J. Surg. 10, 28–55 (2012).
Folkman, S. & Lazarus, R. S. An analysis of coping in a middle-aged community sample. J. Health Soc. Behav. 21, 219–239 (1980).
Padyab, M., Ghazinour, M. & Richter, J. Factor structure of the Farsi version of the ways of coping questionnaire. J. Appl. Soc. Psychol. 42, 2006–2018 (2012).
Zimet, G. D., Dahlem, N. W., Zimet, S. G. & Farley, G. K. The miltidimensional scale of perceived social support. J. Personal Assess. 52, 30–41 (1988).
Bagherian-Sararoudi, R., Hajian, A., Ehsan, H. B., Sarafraz, M. R. & Zimet, G. D. Psychometric properties of the Persian version of the multidimensional scale of perceived social support in Iran. Int. J. Prevent. Med. 4, 1277–1281 (2013).
Cohen, S., Kamarck, T. & Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 24, 385–396 (1983).
Maroufizadeh, S., Zareiyan, A. & Sigari, N. Reliability and validity of Persian version of perceived stress scale (PSS-10) in adults with asthma. Arch. Iran Med. 17, 361–365 (2014).
Paloutzian, R. F., Ellison, C. W. (1982) Loneliness, spiritual wellbeing and quality of life. Loneliness: A sourcebook of current theory, research, and therapy, Peplau, L. A. & Perlman, D., (Eds.) pp. 224–237). (Wiley, 1982).
Nia, H. S. et al. Psychometric evaluation of the Persian version of the spiritual well-being scale (SWBS) in Iranian patients with cancer. Pall Support Care 20, 113–121 (2021).
Nowlan, J. S., Wuthrich, V. M. & Rapee, R. M. Positive reappraisal in older adults: a systematic literature review. Aging Ment. Health 19, 475–484 (2015).
Garland, E., Gaylord, S. & Park, J. The role of mindfulness in positive reappraisal. Explore 5, 37–44 (2009).
Thoits, P. A. Mechanisms linking social ties and support to physical and mental health. J. Health Soc. Behav. 52, 145–161 (2011).
Rowold, J. Effects of spiritual well-being on subsequent happiness, psychological well-being, and stress. J. Relig. Health 50, 950–963 (2011).
Chehrazi, M., Faramarzi, M., Abdollahi, S., Esfandiari, M. & EShafie rizi, S. Health promotion behaviours of pregnant women and spiritual well-being: Mediatory role of pregnancy stress, anxiety and coping ways. Nurs Open 8, 3558–3565 (2021).
Kim, J. & Kim, J. The effect of spiritual well-being on stress coping. Int. J. Adv. Culture Technol. 7, 1–9 (2019).
Kovacs, G., Bullock, G., Ackroyd-Stolarz, S., Cain, E. & Petrie, D. A randomized controlled trial on the effect of educational interventions in promoting airway management skill maintenance. Ann. Emerg Med. 36, 301–309 (2000).
Rowe, M. M. Skills training in the long-term management of stress and occupational burnout. Curr. Psychol. 19, 215–228 (2000).
Eblovi, D. et al. Retention and use of newborn resuscitation skills following a series of helping babies breathe trainings for midwives in rural Ghana. Glob. Health Act. 10, 1387985. https://doi.org/10.1080/16549716.2017.1387985 (2017).
Acknowledgements
This work was supported by Shiraz University of Medical Sciences under Grant number: 98-01-04-21905. The authors would like to thank the employees for participating in the study.
Author information
Authors and Affiliations
Contributions
M.H.K.: conceptualization, methodology, supervision, , investigation, participant management, data assessment and curation, writing: original draft review and editing of the manuscript; F.M.: methodology, investigation, validation, data assessment and curation, writing: original draft review and editing; R.C.: methodology, writing: draft review and editing of the manuscript; H.M.: conceptualization, methodology, supervision, formal analysis, validation, writing: original draft review and editing of the manuscript, project administration, funding acquisition. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kaveh, M.H., Mehrazin, F., Cousins, R. et al. Effectiveness of a transactional model-based education programme for enhancing stress-coping skills in industrial workers: a randomized controlled trial. Sci Rep 13, 5076 (2023). https://doi.org/10.1038/s41598-023-32230-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-32230-2
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
