
Abstract
Systemic inflammation has been associated with aggressive tumor growth, invasion, and metastasis. Here we performed a comprehensive analysis of 26 kinds of inflammatory cytokine expression patterns among 185 patients with breast cancer and 54 healthy volunteers followed by chemometric analysis. We identified the specific cytokine expression patterns of breast cancer patients compared to healthy volunteers with (1) VEGF, IL-9, GM-CSF, IL-13, IL-4, and IFNγ, (2) IL-8, IL-10, IL-12, IL-5, IL-7, IL-1α, GCSF, IL-1β, and TNFα and (3) IL-2, Eotaxin, MIP1β, MIP1α, IL-17, and bFGF. Among the patients with breast cancer, we identified the specific cytokine signature of metastatic patients compared to non-metastatic patients. We also established a mathematical model for distinguishing patients with breast cancer from healthy volunteers and metastatic patients from non-metastatic patients. This cytokine network analysis could provide new insights into early intervention and effective therapeutic strategy for patients with breast cancer.
Similar content being viewed by others

Introduction
Inflammation plays a crucial role in the immune system and defense against several pathogens, including viruses and bacteria, and has been proposed to mediate the initiation and promotion of tumors, angiogenesis and metastasis1. Inflammatory cells are attracted by oncogenic changes, hypoxia, cytokines, and chemokines, among other factors. Inflammation of a tumor microenvironment comprises infiltrating immune cells and activated fibroblasts, which secrete cytokines, chemokines, and growth factors to which the tumor responds2. Moreover, a recent study has shown that inflammation signaling, especially involving IL-6/JAK2/Stat3, plays a crucial role in the stem cell-like characteristics of breast cancer (BC)3.
Measurement of cytokines in serum involves well-established methods in clinical practice. IL-6 may stimulate cancer cell growth and contribute to recurrence and metastasis in BC4, with GCSF, IL-6, and IL-17 able to distinguish between BC and no-cancer groups5. While most studies have found elevated levels of cytokines in patients with BC, a study of 90 patients with BC and 15 healthy volunteers based on univariate analysis found no differences in baseline cytokine levels between the cancer patients and the healthy volunteers, as evidenced by plasma levels of IL-1β, IL-6, IL-8, IL-10, IL-12 and TNF-α6. However, the direct correlation between inflammatory cytokine levels and clinical outcomes has not been evident in patients with BC.
Chemometrics-driven evaluations, especially principal component analysis (PCA), are among the data analysis methods used for statistical inference of low-dimensional parameters with high-dimensional data7; furthermore, many valuable diagnostic data have been revealed by PCA, in particular, in comprehensive gene analysis8. Recently, we reported that mRNA expressions of PD-L1, FOXP3, CD80, CD40 and CD14 in peripheral blood mononuclear cells are affected by disease development and progression9. These data revealed that circulating immune cells were affected by BC development and progression.
Here we performed a comprehensive analysis of inflammatory cytokine in serum derived from 185 patients with BC and 54 healthy volunteers. Our study showed the patients with BC had three different cytokine expression patterns: (1) VEGF, IL-9, GM-CSF, IL-13, IL-4, and IFNγ; (2) IL-8, IL-10, IL-12, IL-5, IL-7, IL-1α, GCSF, IL-1β, and TNFα; (3) IL-2, eotaxin, MIP1β, MIP1α, IL-17, and bFGF. Our data showed that BC patients were distinguishable from healthy volunteers. In the patients with BC, metastatic human epidermal growth factor receptor (HER2)-positive BC patients and triple-negative BC (TNBC) patients showed the specific signature plotting pattern. Furthermore, these cytokine profiles correlated with clinical outcomes in BC.
Results
Patient characteristics
Data on 185 BC patients and 54 women healthy volunteers were available. All of the samples were collected at the time of diagnosis. One-quarter of patients had metastatic BC. Among the BC patients, 62.2% were estrogen receptor-positive and HER2-negative with luminal-type BC, 24.3% had HER2-type BC, and 13.5% had TNBC. Details of patient characteristics are provided in Table 1.
Expression pattern of cytokines in BC patients was distinct from healthy volunteers
PCA of 185 BC patients and 54 healthy volunteers showed that the former were clearly distinguishable from the latter (Fig. 1a). Almost all healthy volunteers were located in Area 1; there was only one healthy volunteer in Area 4. In contrast, BC patients were located in broader zones. A small overlap area between healthy volunteers and BC patients can be observed. Figure 1b shows the contribution of each cytokine to Primary Component 1 (PC1) and PC2. Cytokines, which existed in Area 2 (see Fig. 1b), contributed to Areas 1 and 2 (see Fig. 1a), such as in the form of IFN-γ and IL-13, and also existed in Area 4 (see Fig. 1b) and contributed to Areas 2 and 4 (see Fig. 1a), such as in the form of IL-17 and bFGF.

PCA score plot and corresponding loading plot for subjects. PCA score plot (a) and corresponding loading plot (b) of measured serum cytokines for healthy volunteers (blue) and BC patients (red). Area 1: PC1 > 0, PC2 < 0, Area 2: PC1 < 0, PC2 < 0, Area 3: PC1 > 0, PC2 > 0, Area 4: PC1 < 0, PC2 > 0.
Expression pattern of cytokines in cancer progression and phenotypes
Next, we investigated the expression pattern in BC patients by subgroup plotting. Figure 2a depicts the PCA of the plot according to tumor staging. The patients with Stages 1, 2 and 3 (non-metastatic patients) were primarily located in Areas 3 and 4. In contrast, the patients with Stage 4 were primarily located in Areas 1 and 2. Figure 2b depicts the PCA of the plot of the BC phenotype. There was no signature for the luminal type, whereas the HER2 type tended to exist in the upper area (Areas 1 and 2) and the TNBC type tended to exist in the lower area (Areas 3 and 4). There was no significant pattern analyzed according to Ki67 and tumor grade (Fig. 2c,d).

Correlation between PCA score and BC characteristics. PCA score plot with BC characteristics. (a) cancer stage, (b) cancer subtype, (c) % expression of Ki67 in the tumor, (d) grade (Elston-Ellis modification of Scarff-Bloom-Richardson grading system).
Correlation mapping of cytokines in BC patients and healthy volunteers
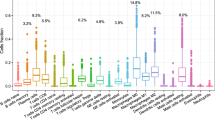
Next, we investigated the correlation pattern of cytokine expression BC patients and healthy volunteers. Figures 3a,b show the top 20 strong correlation combinations of cytokines. Figure 3c shows the heat map of the cytokines’ network with cluster analysis in BC patients. In BC patients, there were three clusters: (1) VEGF, IL-9, GM-CSF, IL-13, IL-4, and IFNγ; (2) IL-8, IL-10, IL-12, IL-5, IL-7, IL-1α, GCSF, IL-1β, and TNFα; (3) IL-2, eotaxin, MIP1β, MIP1α, IL-17, and bFGF. These results indicate that there were specific correlation patterns in BC patients. We also checked the correlation between these cytokines and TGFβ, which has been established as essential for cancer progression, because of its prominent role in the regulation of cell growth, differentiation and migration10. Moreover, there was no significant correlation with another 26 cytokines (Supplementary Fig. S1).

Correlation mapping of cytokines in BC patients and healthy volunteers. (a) Individual top 20 high correlation coefficient scatterplots. (b) The value of the correlation coefficient and the p-value of the top 20 high correlation coefficients. Statistical analysis was performed by the Pearson’s correlation test. (c) Heart map of cytokines’ network with cluster analysis in BC patients. Dark blue means high positive correlation and dark red mean high negative correlation.
Prediction of BC prognosis and therapeutic effect by PCA and IL-17 expression pattern
We investigated the correlation between PCA expression patterns and BC prognosis. We followed up Stage 1–3 patients, with distant metastasis occurring in 14 out of 139 patients (Fig. 4a). Interestingly, these metastatic patients have distributed in the PC1 < 0 areas. Kaplan Mayer analysis showed that disease-free survival (DFS) was significantly shorter in patients in PC1 < 0 (Areas 2 and 4) compared to PC1 > 0 (Areas 1 and 3) (hazard ratio: 0.21; 95% confidence interval [CI], 0.075 to 0.681; P = 0.009 with the use of the log-rank test) (Fig. 4b). In subgroup analysis, the only grade was involved in DFS. Higher stage and HER2 and TNBC subtypes had also trend, but there was not significant due to small sample size (Supplementary Fig. S2). We also investigated the correlation between IL-17 and BC prognosis due to IL-17 being the strongest effector about PC1. There was significantly poor prognosis in the high IL-17 group, which was defined by median levels of IL-17 (hazard ratio: 0.23; 95% CI, 0.078 to 0.662; P = 0.006 with the use of the log-rank test) (Fig. 4c). Next, we investigated the correlation between PCA and IL-17 expression patterns and therapeutic effects among BC patients who received neoadjuvant chemotherapy (Tables 2 and 3). A pathological complete response (pCR) was achieved in 36.6% of all cases (30/82), 25.0% of PC1 < 0 cases (11/44), 50.0% of PC1 > 0 cases (19/38) (Fig. 4d), 24.4% of high IL-17 cases (10/41) and 48.8% of low IL-17 cases (20/41) (Fig. 4e). We checked alteration between cytokine profile at BC diagnosis and after neoadjuvant therapy using eight patient’s samples (Supplementary Fig. S3). Our findings indicate that there were significant alteration patterns in non-pCR with recurrence case. These results suggest that PCA based on serum cytokine levels could predict BC prognosis and therapeutic effects.

Prediction of BC prognosis and therapeutic effect by PCA and IL-17 expression pattern. (a) PCA score plots of the patients with Stage 1–3 operable BC. The blue circles plot patients in whom metastatic disease occurred, along with the score for PC1 (X-axis) and PC2 (Y-axis). (b,c) Kaplan-Meier estimate of overall survival in Stage 1–3 operable BC patients by PC value and IL-17 expression level. B: In the PC1 < 0 areas, there was significantly poor prognosis compared to patients who were in the PC1 > 0 area. Hazard ratio: 0.21; 95% CI, 0.075 to 0.681; P = 0.009 with the use of the log-rank test. (c) There was significantly poor prognosis in the high IL-17 group. Hazard ratio: 0.23; 95% CI, 0.078 to 0.662; P = 0.006 with the use of the log-rank test. (d,e) Correlation between PCA and IL-17 expression patterns and BC therapeutic effects among patients who received neoadjuvant chemotherapy. (d) A pCR was achieved in 36.6% of all cases (30/82), 25.0% of PC1 < 0 cases (11/44) and 50.0% of PC1 > 0 cases (19/38); p = 0.0231. (e) 24.4% of high IL-17 cases (10/41) and 48.8% of low IL-17 cases (20/41); p = 0.0382. Statically analysis was conducted using Fisher’s exact test.
Modeling of orthogonal projections to latent structures (OPLS) based on cytokine array provides information on patients with BC
Our data based on PCA and correlation analysis suggested the existence of three different types of cytokine patterns in the patients with BC. Based on the cytokine pattern, we performed OPLS-discriminant analysis (OPLS-DA) to predict the patients’ status and classification. In this analysis, healthy volunteers, patients with BC, operable patients with BC (Stages 1–3), metastatic patients with BC (Stage 4), TNBC and other types (luminal and HER2) are used as classification variants.
As shown in Fig. 5a–c, we showed the scatterplot for each variant according to the trained model based on all sample data. The red and blue plot indicates each sample and the ellipse line represents the variance in each category. Intuitively, the smaller overlapped area of variance ellipses indicates the more precise prediction of classification. Our data show that the OPLS-DA model could distinguish BC patients from healthy volunteers (Fig. 5a). In the analysis on operable and metastatic BC, even the overlap of variance ellipses is slightly larger than in the previous plot, while the data also suggest that our OPLS-DA model may predict both operable and metastatic BC (Fig. 5b).

OPLS modeling based on cytokine array provides information on patients with BC. (a–c) OPLS-DA score plots of healthy volunteers and patients with BC, operable BC/metastatic BC, and TNBC/other types. The distributions of each sample are plotted by the red and blue circles, along with the score of the predictive component (X-axis) and the orthogonal component (Y-axis). The ellipse lines on the plots indicate the variance of the samples, which is drawn according to the Mahalanobis distance. (d) Summary of classification results (SD) calculated by k-fold cross-varidation (k = 5). Precision and recall refer to the relevance of the classification. See the main text for definitions.
In contrast, in the analysis on TNBC and other types, a large part of each ellipse line overlap, indicating that our OPLDS-DA model makes it difficult to distinguish TNBC from other types (Fig. 5c). To validate our OPLS-DA models, we performed k-fold cross-validation and predicted classification performance, here we used k = 5. The analysis of TNBC and other types could not be performed because of the insufficient sample size. Precision was calculated by using the following formula: precision = (true positive)/(true positive + false positive). The recall was also calculated using the following formula: recall = (true positive)/(true positive + false negative). As shown in Fig. 5d, the OPLDS-DA model for predicting BC patients and healthy volunteers shows satisfactory precision and recall values.
Moreover, the OPLDS-DA model for predicting both operable and metastatic BC shows potent precision and recall values. These results indicate that OPLS-DA analysis based on serum cytokine levels can precisely predict patients with BC. More importantly, our data showed that OPLS-DA analysis based on serum cytokine levels could predict operable or metastatic BC with a 90% probability.
Correlation between serum cytokine expression and immune profile on BC tissues
The previous study revealed that immune profile, such as tumor infiltrating lymphocytes (TILs) and FOXP3, on BC tissues has both predictive and prognostic values in BC11,12. However, the correlation between serum cytokine expression and immune profile in BC tissues is still unclear. We analyzed this correlation by evaluating TILs and FOXP3 in breast cancer tissues to uncover the immune response in breast cancer tumor microenvironment. We evaluate 83 paired samples in this study and characteristic of patients is in Supplementary Table S1. Interestingly, the majority of cytokines have a negative correlation with TILs and have a positive correlation with FOXP3 (Fig. 6a–c). These results suggest that high TILs correlates with low pro-inflammatory cytokine expression status and high FOXP3 correlates with high pro-inflammatory cytokine expression status in BC.

Correlation between serum cytokine expression and immune profile on BC tissues. (a) The value of the correlation coefficient between serum cytokine expressions and immune profile on BC tissues. The immune profile was evaluated TILs and FOXP3 on FFPE samples. Statistical analysis was performed by the Pearson’s correlation test. (b,c) PCA score plots of the patients with Stage 1–3 operable BC. (b) TILs (% stromal area), (c) FOXP3 (% TILs).
Discussion
Tumor tissue is the gold standard for clinical and investigational sequencing. However, major barriers exist regarding acquisition and utility, such as inconvenience from a scheduling perspective, the cost of patient care, and invasive procedures for patients. The primary limitation of tissue biopsy is heterogeneity, which characterizes most advanced cancers13, with heterogeneity existing between metastases within the same patient. To overcome the limitations of tissue biopsy, less invasive techniques capable of capturing tumor heterogeneity and the molecular changes that cancer cells undergo when they are exposed to therapy are needed14. The blood test, which is the appropriate and most straightforward measure for mass screening, is widely used in the testing of several diseases including metabolic syndrome.
In this study, we presented a novel approach of cytokine networks based on the comprehensive analysis of 26 kinds of expression inflammatory cytokine expression patterns, followed by chemometric analysis. We revealed the specific cytokine expression patterns between patients with BC and healthy volunteers and the specific cytokine signature in metastatic patients with BC.
Recent studies have suggested the existence of complex crosstalk between the tumor and host, which plays a crucial role in tumor initiation, growth, metastasis, and drug resistance. The inflammatory cytokine is the main component of this crosstalk. For instance, several inflammatory cytokines are crucial in the pre-metastatic niche in several animal models. There were several reports, which described cytokines and BC progression. Wang et al. reported that serum IL-6, IL-8, IL-10, SCC-Ag, and CYFRA 21-1 may serve as potential markers for predicting metastasis and prognosis of BC15. Circulating tumor cells (CTCs), which is increased with BC progression and metastasis, involved in cytokine expression in BC. Vilsmaier et al. reported that IL-1α is a candidate marker for the release of tumor cells and IL-1β, IL-12, sFlt1 and PlGF appears to be related to CTCs release in patients with BC16,17. Another group showed that pro-inflammatory cytokines TNFα, IL-6, CSF-1, and IFNγ correlated with disseminated tumor cells in BC18. We demonstrate that cytokine expression pattern correlated with both immune profiles on BC tissues (Fig. 6a). Inflammation in a tumor microenvironment comprises infiltrating immune cells that secrete cytokines, chemokines, and growth factors to which the tumor responds1,19. Previously, we revealed that BC progression alters immune profile in peripheral blood mononuclear cells (PBMCs)9. FOXP3 expression in PBMCs is one of the genes correlated with BC progression, and we discovered that FOXP3 in BC tissues also is correlated with serum cytokine expression pattern. Overall, our results may uncover significant immune response in BC tumor microenvironment.
Consistent with these findings, clinical studies have shown the upregulation of several inflammation cytokines including G-CSF, IL-6, and IL-17 in patients with BC5. Meanwhile, recent reports have shown that IL-17-producing cells increased in tumor tissues and peripheral blood from different cancer patients20 {Numasaki, 2004 #707. In contrast, a blood test to measure IL-17 levels is the more feasible way to evaluate the significance of IL-17 in tumor microenvironments, compared with measuring IL-17-producing cells. In non-small-cell lung cancer and hepatocellular carcinoma, serum IL-17 levels were correlated with poor prognosis21,22. Here, we are the first to show that serum IL-17 is up-regulated in BC patients and that high levels of IL-17 are also correlated with poor clinical outcomes.
Recently, preclinical models have shown that IL-17 mediates cancer progress via various mechanisms23,24,25,26,27,28. Coffelt et al. reported that increasing systemic IL-17 levels leads to the up-regulation of G-CSF, which subsequently causes neutrophil expansion and alteration of the neutrophil phenotype. Another study reported the effects of IL-17 and bFGF on mesenchymal stem cell (MSC) growth and elucidated the signaling pathways involved. These results indicated that IL-17 increased the frequency of colony-forming unit fibroblast (CFU-F), as well as MSC proliferation in a dose-dependent manner, while bFGF supplementation induced an increase in cell proliferation27. Consistent with these findings, our data indicated that the interaction of serum IL-17 levels with an increased level of both bFGF and G-CSF are correlated with poor DFS among BC patients. While IL-17- and IL-17-producing cells are significantly insensitive towards chemotherapy in experimental settings29, little is known about the correlation between systemic IL-17 levels and sensitivity towards chemotherapy in clinical settings, especially concerning BC. Although there are limitations to our study, given that patient characteristics include all subtypes and involve various chemotherapy regimens, our data indicate that systemic IL-17 levels are correlated with pathological complete response rates in BC patients. To overcome such limitations, we need to further investigate the correlation between serum IL-17 levels and clinical outcomes in larger-volume clinical trials.
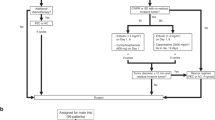
We acknowledge that this study has several other limitations. Notably, this study is retrospective, meaning that it is difficult to evaluate correlations between cytokine diversity and clinical outcome due to treatment and phenotype bias. We should validate using individual cohort to enhance our conclusion. To overcome this limitation, we are planning to validate using two ongoing clinical trial data set. The first one is to investigate the efficacy and safety of dual-HER2 blockage therapy in HER2-positive breast cancer (Clinical trial information: UMIN000007576). The other one is to evaluate the safety, antitumor effect and improved prognosis of Nivolumab with radiation therapy in patients with HER-2-negative metastatic breast cancer have bone metastasis that possible to irradiate (Clinical trial information: UMIN000026046). These clinical trials will cover all phenotypes. Additionally, we will investigate not only cytokine expression pattern but also tumor immune microenvironment status using CyTOF analysis and RNA-seq analysis of PBMCs. Then, we will confirm the correlation between cytokine expression pattern and tumor microenvironment status.
In this study, at least in the evaluations of BC development and progression, our analysis could be potentially relevant as we revealed them by OPLS-DA (Fig. 5). To further strengthen our model, we performed k-cross-validation as it is used for the development of biomarker classifiers from high dimensional data set30. Interestingly, results of k-fold cross-validation showed high accuracy to distinguish BC from HV and stage IV patients from stage I-III patients. Additionally, the standard deviation value is less than 5% both recall and precision rate. Therefore, we think the risk of over-learning is very low. Considering the application, our data are crucial because our results suggest that serum analysis is a useful approach to provide information, for example, on the subtype of cancer, inflammation status and prognosis by a 12.5-µl serum sample. Regarding accessibility, for example, in terms of low invasion, established method and low cost, the comprehensive analysis of inflammatory cytokines in serum could be useful for monitoring inflammation status in the use of antagonizing/neutralizing antibodies to address inflammatory cytokine signaling.
Methods
Serum samples
Serum from healthy volunteers, early-stage BC patients, and metastatic BC patients was collected by the Department of Breast Surgery, Kyoto University Hospital, and the Resource Center for Health Science, Kyoto, Japan. All the BC patient’s samples were collected at the BC diagnosis between April 2011 and March 2015. Eight patients had two-point samples, both at diagnosis and after neoadjuvant therapy. Written informed consent was given by all patients before collection. All study protocols were approved by the Ethics Committee for Clinical Research, Kyoto University Hospital (Authorization Number G424) and performed according to the Declaration of Helsinki and the Ethical Guidelines for Epidemiological Research of the Ministry of Education, Culture, Sports, Science, and Technology and the Ministry of Health, Labour, and Welfare of Japan. Samples were frozen in liquid nitrogen and stored at −80 °C within 2 hours from sample collection. We checked if sample storage period effects on cytokine expression in this study (Supplementary Fig. S4). All of the value of correlation coefficient were within 0.2, and there was no significant distribution in the characteristic of patients.
Cytokine and chemokine measurement
The cytokines in serum samples, IL-1β, IL-1γα, IL-2, IL-4, IL-5, IL-6, IL-7, IL-8, IL-9, IL-10, IL-12 (p70), IL-13, IL-15, IL-17, granulocyte-macrophage-colony-stimulating factor, granulocyte colony-stimulating factor, interferon gamma (IFN-γ), monocyte chemoattractant protein-1, macrophage inflammatory protein-1α (MIP-1α), macrophage inflammatory protein-1β (MIP-1β), PDGF-BB, RANTES, VEGF, bFGF and TNF-α were measured with a Bio-Plex multiplex assay system (Bio-Rad, Hercules, CA) according to the manufacturer’s instructions. This analysis was conducted on 12.5-µl serum sample from each patient.
Analysis of the immune profile on BC tissues
The paraffin sections were rehydrated and immersed in 3% hydrogen peroxide for 10 min to quench endogenous peroxidase activity. Epitope retrieval was performed by heating the sections at 95 °C in Target Retrieval Solution (pH 9, S2375; Dako) for 30 min in an electric pressure cooker (SR-P37; Panasonic, Tokyo, Japan). All incubations after the blocking step were performed at room temperature. The wash buffer was 0.05 M Tris-buffered saline with 0.05% Tween 20 (pH 7.6). Following blocking with 5% normal goat serum (Abcam) in PBS for 10 min, the sections were incubated with anti-FOXP3 antibodies (236 A/E7; Abcam) for 1 h.
Histopathologic assessment of the percentage of TILs and FOXP3 was performed on one representative immunohistochemical section of a tumor using methods recommended by the International TILs Working Group 201418. % TILs was defined as the percentage of lymphocyte area per tumor area in vivo samples. Areas of in situ carcinomas, normal lobules, necrosis, hyalinization, and crush artifacts were not included. Histopathologic evaluation of TILs was performed by two breast pathologists who scored each case independently in a blind manner. The mean values of both observers were obtained as the final scores for each case.
Statistics and data analysis
Multivariate statistical analysis (PCA and OPLS-DA) was performed in order to evaluate the measured cytokine data using R version 3.3.1 (R Foundation for Statistical Computing, 2016) and the R ropls package version 1.8.0. PCA can project higher-dimension data into lower-dimensional space in order to visualize the distribution of complex data. Typically two-dimension is used as the lower-dimensional space. Usually, PCA results are represented by a score plot and a loading plot. In a score plot, samples expressing similar cytokine values are plotted in the near position, while the spatial groups of similar samples are recognized as a pattern. In a loading plot, the positions of each point corresponding to the cytokine variables describe the correlation with the PCs, such as PC1 and PC2. The loading plot implies which cytokines mainly contribute to forming the pattern in the score plot. In our PCA calculation, a few outlier samples, which were more than 10–100 times larger than the average of the distribution, were omitted because substantial outlier values collapse the pattern. OPLS-DA is a potent statistical tool, which provides insights into distinguishing between groups of high-dimensional spectral data31. The score axis is the predictive component, which is the variation correlated to the factor of interest. The orthogonal score axis is the first component of the uncorrelated variations. A χ2 test (two-sided, α = 0.05) was used to compare the populations between groups in the score plot, using SPSS 17.0 (Chicago, IL, USA).
k-fold-cross-validation: The dataset was randomly partitioned into k = 5 disjoint subsets to be used as a training and testing sets to validate the Delphi exercise-approved diagnostic criteria. Four subsets were used as the training set to build a diagnostic model, and the remaining subset was used as the testing set to test the model. This process is repeated five times for each dataset, each round with a different training set and complementary testing set. Model performance was estimated by calculating precision and recall which definitions were described at the results section. The averages and standard deviations over the 5 datasets were calculated.
Data Availability
The datasets generated during and analyzed during the current study are not publicly available due to protecting participant confidentiality but are available from the corresponding author on reasonable request.
References
Grivennikov, S. I., Greten, F. R. & Karin, M. Immunity, inflammation, and cancer. Cell 140, 883–899, https://doi.org/10.1016/j.cell.2010.01.025 (2010).
Baumgarten, S. C. & Frasor, J. Minireview: Inflammation: an instigator of more aggressive estrogen receptor (ER) positive breast cancers. Mol Endocrinol 26, 360–371, https://doi.org/10.1210/me.2011-1302 (2012).
Marotta, L. L. & Polyak, K. Unraveling the complexity of basal-like breast cancer. Oncotarget 2, 588–589, https://doi.org/10.18632/oncotarget.314 (2011).
Leek, R. D. & Harris, A. L. Tumor-associated macrophages in breast cancer. J Mammary Gland Biol Neoplasia 7, 177–189 (2002).
Lyon, D. E., McCain, N. L., Walter, J. & Schubert, C. Cytokine comparisons between women with breast cancer and women with a negative breast biopsy. Nursing research 57, 51–58, https://doi.org/10.1097/01.NNR.0000280655.58266.6c (2008).
Pusztai, L. et al. Changes in plasma levels of inflammatory cytokines in response to paclitaxel chemotherapy. Cytokine 25, 94–102 (2004).
Nikas, J. B. & Low, W. C. ROC-supervised principal component analysis in connection with the diagnosis of diseases. Am J Transl Res 3, 180–196 (2011).
Hunter, D. J. et al. A genome-wide association study identifies alleles in FGFR2 associated with risk of sporadic postmenopausal breast cancer. Nat Genet 39, 870–874, https://doi.org/10.1038/ng2075 (2007).
Kawaguchi, K. et al. Altered expression of major immune regulatory molecules in peripheral blood immune cells associated with breast cancer. Breast Cancer. https://doi.org/10.1007/s12282-016-0682-7 (2016).
Pickup, M., Novitskiy, S. & Moses, H. L. The roles of TGFbeta in the tumor microenvironment. Nature reviews. Cancer 13, 788–799, https://doi.org/10.1038/nrc3603 (2013).
Denkert, C. et al. Tumor-associated lymphocytes as an independent predictor of response to neoadjuvant chemotherapy in breast cancer. Journal of clinical oncology: official journal of the American Society of Clinical Oncology 28, 105–113, https://doi.org/10.1200/JCO.2009.23.7370 (2010).
Denkert, C. et al. Tumour-infiltrating lymphocytes and prognosis in different subtypes of breast cancer: a pooled analysis of 3771 patients treated with neoadjuvant therapy. The lancet oncology 19, 40–50, https://doi.org/10.1016/S1470-2045(17)30904-X (2018).
Gerlinger, M. et al. Intratumor heterogeneity and branched evolution revealed by multiregion sequencing. The New England journal of medicine 366, 883–892, https://doi.org/10.1056/NEJMoa1113205 (2012).
Murtaza, M. et al. Non-invasive analysis of acquired resistance to cancer therapy by sequencing of plasma DNA. Nature 497, 108–112, https://doi.org/10.1038/nature12065 (2013).
Wang, H. & Yang, X. Association between serum cytokines and progression of breast cancer in Chinese population. Medicine (Baltimore) 96, e8840, https://doi.org/10.1097/MD.0000000000008840 (2017).
Vilsmaier, T. et al. Influence of Circulating Tumour Cells on Production of IL-1alpha, IL-1beta and IL-12 in Sera of Patients with Primary Diagnosis of Breast Cancer Before Treatment. Anticancer research 36, 5227–5236, https://doi.org/10.21873/anticanres.11093 (2016).
Vilsmaier, T. et al. Angiogenic cytokines and their influence on circulating tumour cells in sera of patients with the primary diagnosis of breast cancer before treatment. BMC cancer 16, 547, https://doi.org/10.1186/s12885-016-2612-7 (2016).
Semesiuk, N. I. et al. Disseminated tumor cells and enhanced level of some cytokines in bone marrow and peripheral blood of breast cancer patients as predictive factors of tumor progression. Exp Oncol 35, 295–302 (2013).
Coussens, L. M. & Werb, Z. Inflammation and cancer. Nature 420, 860–867, https://doi.org/10.1038/nature01322 (2002).
Chen, W. C. et al. Interleukin-17-producing cell infiltration in the breast cancer tumour microenvironment is a poor prognostic factor. Histopathology 63, 225–233, https://doi.org/10.1111/his.12156 (2013).
Chen, X. et al. Increased IL-17-producing cells correlate with poor survival and lymphangiogenesis in NSCLC patients. Lung Cancer 69, 348–354, https://doi.org/10.1016/j.lungcan.2009.11.013 (2010).
Zhang, J. P. et al. Increased intratumoral IL-17-producing cells correlate with poor survival in hepatocellular carcinoma patients. J Hepatol 50, 980–989, https://doi.org/10.1016/j.jhep.2008.12.033 (2009).
Coffelt, S. B. et al. IL-17-producing gammadelta T cells and neutrophils conspire to promote breast cancer metastasis. Nature 522, 345–348, https://doi.org/10.1038/nature14282 (2015).
Du, J. W., Xu, K. Y., Fang, L. Y. & Qi, X. L. Interleukin-17, produced by lymphocytes, promotes tumor growth and angiogenesis in a mouse model of breast cancer. Molecular medicine reports 6, 1099–1102, https://doi.org/10.3892/mmr.2012.1036 (2012).
He, D. et al. IL-17 promote tumor development through the induction of tumor promoting microenvironments at tumor sites and myeloid-derived suppressor cells. J Immunol 184, 2281–2288, https://doi.org/10.4049/jimmunol.0902574 (2010).
Liu, J. et al. IL-17 is associated with poor prognosis and promotes angiogenesis via stimulating VEGF production of cancer cells in colorectal carcinoma. Biochem Biophys Res Commun 407, 348–354, https://doi.org/10.1016/j.bbrc.2011.03.021 (2011).
Mojsilovic, S. et al. IL-17 and FGF signaling involved in mouse mesenchymal stem cell proliferation. Cell and tissue research 346, 305–316, https://doi.org/10.1007/s00441-011-1284-5 (2011).
Zhu, X. et al. IL-17 expression by breast-cancer-associated macrophages: IL-17 promotes invasiveness of breast cancer cell lines. Breast cancer research: BCR 10, R95, https://doi.org/10.1186/bcr2195 (2008).
Ma, Y. et al. Contribution of IL-17-producing gamma delta T cells to the efficacy of anticancer chemotherapy. The Journal of experimental medicine 208, 491–503, https://doi.org/10.1084/jem.20100269 (2011).
Baek, S., Tsai, C. A. & Chen, J. J. Development of biomarker classifiers from high-dimensional data. Brief Bioinform 10, 537–546, https://doi.org/10.1093/bib/bbp016 (2009).
Bylesjo, M. et al. Orthogonal projections to latent structures as a strategy for microarray data normalization. BMC Bioinformatics 8, 207, https://doi.org/10.1186/1471-2105-8-207 (2007).
Acknowledgements
We would like to thank the medical staff of the Department of Breast Surgery, Kyoto University Hospital, for their help in the recruitment of patients and the collection of samples.
Author information
Authors and Affiliations
Contributions
Kosuke Kawaguchi and Eiji Suzuki planned the studies. Kosuke Kawaguchi, Masashi Sakurai, Yasuko Yamamoto, Eiji Suzuki, Moe Tsuda, Tatsuki R. Kataoka, Masahiro Hirata, Mariko Nishie, Takashi Nojiri and Motofumi Kumazoe, performed the experiments. Kosuke Kawaguchi had responsibility for all data integrity and data analysis. Kosuke Kawaguchi, Masashi Sakurai, Yasuko Yamamoto, Eiji Suzuki, Moe Tsuda, Tatsuki R. Kataoka, Masahiro Hirata, Mariko Nishie, Takashi Nojiri, Motofumi Kumazoe, Kuniaki Saito and Masakazu Toi discussed the results. Kosuke Kawaguchi conducted all the research. Kosuke Kawaguchi had primary responsibility for the final content. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kawaguchi, K., Sakurai, M., Yamamoto, Y. et al. Alteration of specific cytokine expression patterns in patients with breast cancer. Sci Rep 9, 2924 (2019). https://doi.org/10.1038/s41598-019-39476-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-019-39476-9
This article is cited by
-
Time-series blood cytokine profiles correlate with treatment responses in triple-negative breast cancer patients
British Journal of Cancer (2024)
-
A breast cancer classification and immune landscape analysis based on cancer stem-cell-related risk panel
npj Precision Oncology (2023)
-
TGFß1 Stimulates Lymphatic Endothelial Cells to Produce IL7 and IL15, Which Act as Chemotactic Factors for Breast Cancer Cells with Mesenchymal Properties
Journal of Mammary Gland Biology and Neoplasia (2023)
-
Alteration of the immunophenotype and cytokine profiles in patients affected by neuroendocrine neoplasms
Endocrine (2023)
-
Definition of a novel breast tumor-specific classifier based on secretome analysis
Breast Cancer Research (2022)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
