
Abstract
Both obesity and diabetes mellitus are well-known risk factors for tendinopathies. We retrospectively compared the efficacy of single corticosteroid injections in treating lateral epicondylitis in patients with and without metabolic syndrome (MetS). Fifty-one patients with lateral epicondylitis and MetS were age- and sex-matched with 51 controls without MetS. Pain severity, Disability of the Arm, Shoulder, and Hand score, and grip strength were assessed at base line and at 6, 12 and 24 weeks post-injection. The pain scores in the MetS group were greater than those in the control group at 6 and 12 weeks. The disability scores and grip strength in the MetS group were significantly worse than those of the control group at 6 weeks. However, there were no significant differences at 24 weeks between the groups in terms of pain, disability scores and grip strengths. After 24 weeks, three patients (6%) in the control group and five patients (10%) in the MetS group had surgical decompression (p = 0.46). Patients with MetS are at risk for poor functional outcome after corticosteroid injection for lateral epicondylitis in the short term, but in the long term there was no difference in outcomes of steroid injection in patients with and without MetS.
Similar content being viewed by others

Introduction
Lateral epicondylitis (LE) is the most common cause of elbow and forearm pain in adults, and it has an annual incidence of 1% to 3% in the general population1, 2. Although some patients with symptoms of a shorter duration may resolve spontaneously3, the average duration of symptoms for patients with LE is reportedly 44 months1 and no difference has been observed in the severity of symptoms in patients that had pain greater or less than 12 months4. Despite the high incidence of LE, optimal management for LE has not been established, and numerous treatment options, including bracing, therapeutic exercise, shock wave or ultrasound therapy, corticosteroid injection, and surgical decompression have been used to treat this condition5,6,7,8,9. Of these treatment choices, local corticosteroid injections are extensively administered as easy, cost-effective short- to mid-term treatment for patients with LE10,11,12. However, there is limited evidence on the long-term success of corticosteroid injection to treat LE13,14,15, and the case for corticosteroid being superior to wait and see at longer-term follow-up is not solid13, 14. The long-term improvement after a corticosteroid injection for LE might in fact be explained by the natural course of the condition2, 3. However, some patients need surgical treatment because conservative treatments fail to adequately alleviate the symptoms. The differences in treatment outcomes may, in part, be due to differences in patient characteristics, such as combined medical conditions affecting the individual.
Metabolic syndrome (MetS) is a constellation of medical conditions arising from insulin resistance and abnormal adipose deposition and function16. The prevalence of MetS has increased due to the aging population and the obesity epidemic in industrialized countries, resulting in this condition posing a major public health challenge17, 18. Both obesity and diabetes are well-known risk factors for tendinopathies19, and the prevailing hypotheses of tendon damage in obese subjects indicate two mechanisms: (i) an increased force on load-bearing tendons and (ii) biochemical alterations attributed to systemic bioactive factors19, 20. Obesity and diabetes share common pathologic pathways characterized by an increase in cross-linking between collagen fibrils mediated by advanced glycation end products (AGEs) and low-grade inflammation, which amplify the deleterious effect of tendon overuse21. The deposit of fat or cholesterol byproducts in tendon tissues can weaken the mechanical strength of the tendon and can further impair healing22, 23. Thus, the co-occurrence of MetS with these diseases might affect treatment outcomes of local corticosteroid injections in LE.
Due to the increased prevalence of MetS and the higher incidence of LE, it is important to assess the outcomes of a corticosteroid injection for LE in patients with MetS. Therefore, the aim of this study was to compare the outcome of a corticosteroid injection in patients with or without MetS. We hypothesized that patients with LE and MetS would show decreased functional scores for both objective and subjective measures of function compared to patients without MetS for 24 weeks after corticosteroid injection.
Materials and Methods
Patients diagnosed with LE and treated with corticosteroid injection between June 2013 and May 2015 were retrospectively enrolled in this study. The inclusion criteria were LE symptoms for more than 3 months, with LE defined as pain on the lateral side of the elbow, pain at the lateral epicondyle region on resisted extension of the wrist, and tenderness at the lateral epicondyle on direct palpation. The exclusion criteria were age younger than 18 years, corticosteroid injection within the past 6 months, previous surgery on the involved elbow, inflammatory diseases (e.g., rheumatoid arthritis or psoriatic arthritis), neck or shoulder pain on the ipsilateral side, and inability to complete a self-reported questionnaire. Among patients without these factors, we identified 51 patients with LE and MetS who were matched for age and sex with 51 controls without MetS. Controls were selected by cumulative sampling method at the end of the follow-up period according to matching variables in a stepwise fashion, first attempting to match on age and then sex. The diagnosis of MetS was made according to the National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III definition16, which has been widely used because of its simplicity as its components are easily and routinely measured in most clinical and research settings24. MetS was defined by the presence of at least three of the following five criteria: (1) a clinical diagnosis of diabetes treated with oral hypoglycemic medication or insulin or a fasting serum glucose level of 110 mg/dL or higher ; (2) arterial blood pressure of 130/85 mm Hg or higher or current use of antihypertensive medication ; (3) plasma triglyceride level of 150 mg/dL or higher ; (4) high-density lipoprotein cholesterol level of less than 50 mg/dL for females or less than 40 mg/dL for males ; or (5) a waist size greater than 88 cm for females or 102 cm for males. The modified NCEP ATP III criteria suggested that the cut-off points for the waist circumference should be specific according to ethnicity. In individuals of Asian origin, a cut-off of 90 cm in men and 80 cm in women is used25. For the NCEP criteria, abdominal obesity is a component of the syndrome, but not a prerequisite for its diagnosis. This study was approved by the institutional review boards of Gil Medical Center, and all participants provided written informed consent. This study did not require any deviation of the current clinical practice and was conducted in accordance with the principles of research involving human subjects as expressed in the Declaration of Helsinki (64th, 2013) and with Good Clinical Practice standard. This study was registered (30th June 2017) at the Clinical Research Information Service (CRiS), Republic of Korea (KCT0002367).
The corticosteroid injection was made with a 23-gauge needle by placing the needle under the extensor origin and injecting with multiple passes of the needle in a fanlike fashion in the area. The content was injected in the deepest aspects of the common tendon origin to limit the risk of skin atrophy. The corticosteroid injection treatment was carried out with a single 2 mL injection, containing 1 mL of lidocaine (10 mg/mL) and 1 mL of triamcinolone acetonide (40 mg/mL). After the injection, the patient was instructed to resume activity as tolerated. No further physical therapy or splinting was recommended, and no patients were injected a second time. The decision to undergo surgery was a mutual decision between the patient and the surgeon.
Patients returned for their functional assessments at 6 (range, 5–8), 12 (11–14) and 24 (22–26) weeks after the corticosteroid injection. The maximum pain-free grip strength was measured in kilogram-force using a Jamar dynamometer (Asimow Engineering, Los Angeles, CA) with the shoulder and forearm in neutral rotation. The mean value of 3 efforts was calculated and included in the analysis, and the dynamometer was calibrated according to a standard procedure by using standardized test weights. The severity of pain during daily activity was evaluated using an 11-point numeric rating scale (NRS), with ‘0’ indicating that the patient experiences no pain and ‘10’ indicating the highest imaginable pain. The patient-reported outcome was evaluated using the Disabilities of the Arm, Shoulder and Hand (DASH) score, which is a self-administered, upper-extremity specific questionnaire that consists of 30 questions26. It includes physical functions, symptoms, and social-role function, work, sleep, and confidence items. Five responses are provided per question and are scored from ‘1’ (without difficulty or no symptom) to ‘5’ (unable to engage in activity or very severe symptoms). Thus, the DASH score provides a best possible score of ‘0’ and a worst possible score of ‘100’. The DASH evaluation is user-friendly, reliable, and valid for a range of upper-extremity disorders27, 28. The investigators (trained nurse) checked all returned questionnaires for completion, and the participants were assisted in completing the missing items.
Statistical analysis
A post hoc power analysis was performed on the DASH scores to determine the minimum number of subjects needed to detect a 10-point difference between the two groups, which would be considered clinically relevant (minimal clinically important difference)29. Based on this study’s data, the inclusion of 81 patients with an allocation ratio of 40/41 would provide 84% power and a 2-sided level of 0.05 to detect the clinical relevant differences between the two groups.
Descriptive statistics were used to represent the demographics and clinical characteristics of the patients. The Kolmogorov-Smirnov test was used to identify the normality of the variable distributions, and a t-test was used to determine any significant differences between the two groups in terms of continuous variables, and the Chi-squared or Fisher exact tests were used to determine any significant differences in the categorical variables. The outcomes at the follow-up visits were compared with use of two-way ANOVA with repeated measures for time with adjustment of p values by the Greenhouse-Geisser epsilon. Statistical significance was accepted when p < 0.05.
Ethical approval
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This study was registered (30th June 2017) at the Clinical Research Information Service (CRiS), Republic of Korea (KCT0002367).
Results
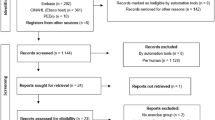
The age and sex of the MetS group were similar to those of the control group, and there was no significant difference in the duration of symptoms and affected side between the two groups. However, the BMI of the patients in the MetS group was significantly greater than that for patients without MetS (Table 1). There were five cases of steroid flare (three in the MetS group and two in the control group) and five cases of skin discoloration/subcutaneous fat atrophy (three in the MetS group and two in the control group), but there were no other serious complications after the injection therapy. Before the 24-week evaluation, 5 patients in the MetS group and 8 in the control group were lost to follow-up (Fig. 1). Missing data were not imputed so as to avoid biasing estimates of the missing outcomes30.

Flow chart of the study population, showing the number of patients with lateral epicondyllitis that were enrolled in the metabolic syndrome group and the control group, and their status at the follow-up visit.
Patients with MetS had similar pre-injection mean grip strengths, pain NRS and DASH scores compared to the control group. Repeated-measures analysis of variance was used to test for a treatment effect, that is, for any average difference between groups in the pattern of change over time. Analysis of pain NRS score showed significant group effect [F(1,79) = 9.37, p = 0.003] and a significant group by time interaction [F(2.19, 203.27) = 3.64, p = 0.028]. The pain NRS scores in the MetS group were greater than those in the control group at 6 and 12 weeks of follow-up (p = 0.02 and 0.04, respectively, Fig. 2). Similarly, analysis of pain DASH scores showed significant group effect [F(1,79) = 10.73, p = 0.002] and a significant group by time interaction [F(2.48, 195.21) = 3.71, p = 0.026]. The DASH scores in the MetS group were significantly greater (with more severe symptoms) than those of the control group at 6 weeks of follow-up (p = 0.01, Fig. 3). Analysis of grip strength showed no group effect [F(1,79) = 2.82, p = 0.097], but a significant group by time interaction [F(2.29, 179.21) = 3.25, p = 0.041]. The grip strength was weaker in patients with MetS than in the control group at 6 weeks of follow-up (p = 0.04, Fig. 4). However, there were no significant differences at the final follow-up between the MetS and control group in terms of the pain NRS scores, DASH scores and grip strengths. After 24 weeks of follow-up, three patients (6%) in the control group and five patients (10%) in the MetS group had surgical decompression due to persistent or recurrent symptoms after the injection (p = 0.46).

Comparison of pain NRS scores. LE = lateral epicondylitis, MetS = metabolic syndrome, *P < 0.05 vs. the control group at the same time point, error bars = 1 SD. Two-way ANOVA with repeated measures for time with adjustment of p values by the Greenhouse-Geisser epsilon showed significant group effect [F(1,79) = 9.37, p = 0.003] and a significant group by time interaction [F(2.19, 203.27) = 3.64, p = 0.028].

Comparison of DASH scores. LE = lateral epicondylitis, MetS = metabolic syndrome, *P < 0.05 vs. the control group at the same time point, error bars = 1 SD. Two-way ANOVA with repeated measures for time with adjustment of p values by the Greenhouse-Geisser epsilon showed significant group effect [F(1,79) = 10.73, p = 0.002] and a significant group by time interaction [F(2.48, 195.21) = 3.71, p = 0.026].

Comparison of grip strength. LE = lateral epicondylitis, MetS = metabolic syndrome, *P < 0.05 vs. the control group at the same time point, error bars = 1 SD. Two-way ANOVA with repeated measures for time with adjustment of p values by the Greenhouse-Geisser epsilon showed no group effect [F(1,79) = 2.82, p = 0.097], but a significant group by time interaction [F(2.29, 179.21) = 3.25, p = 0.041].
Discussion
The most important finding of the present study was that corticosteroid injections in MetS patients were not as effective in the short-term with regard to subjective pain perception and functional recovery. However, there were no significant differences in pain, grip strength, and functional score between the two groups at the end of the study (24-week follow-up). At 6 and 12 weeks, the pain improvement was better in the control group, while at 6-week follow-up the DASH and grip strength was better in the control group.
MetS comprises a cluster of risk factors for large-vessel artherosclerotic disease16, and diabetes is a well-known risk factor for tendinopathies31, 32. Hyperglycaemia associated with diabetes alters tendon homeostasis33, 34, affects collagen cross-linking in tendons35 and reduces proteoglycan content36. Advanced glycation end-products (AGEs) also diminish tendon collagen fiber sliding19, 37. Obesity has also been recognized as a risk factor for tendinopathy in non-load-bearing as well as load-bearing tendons38, 39. The probability of tendon abnormalities is higher in males with an increased waist circumference, and asymptomatic Achilles tendon pathology is reportedly associated with central fat distribution in males21, 40. Hypercholesterolemia results in fatty deposits in muscle and tendon tissues as well as vascular endothelial cells or liver cells41, 42, and microscopic cholesterol deposition inside the tendons could initiate and maintain low-grade persistent inflammation, which may be responsible for chronic tendon degeneration43.
Lateral epicondylitis is thought to be related to the overuse of the extensor carpi radialis brevis muscle, producing pain in the lateral elbow and forearm region2. Although the role of inflammation in the pathophysiology of this condition is questionable, lateral epicondylitis is postulated to involve degenerative changes in the epicondylar enthesis of the extensor carpi radialis brevis and perhaps also the supporting collateral ligamentous complex and joint capsule44. Uncertainty regarding the pathologic basis of lateral epicondylitis underlies, in part, the lack of consensus on its optimal management13,14,15. Some authors have supported corticosteroid injection as an effective non-operative treatment for LE10,11,12, while others have considered the injection provides only temporary relief while waiting for spontaneous recovery13, 14. Interestingly, earlier randomized trials were more likely to show significant symptom relief after a steroid injection for LE whereas recent trials tend not to show a significant effect resulting from the steroid injection2, 45. A long-term improvement after a corticosteroid injection for LE might be considered as the natural course of the condition because spontaneous resolution has been reported at up to 80% of patients within 1 year2, 3. The systematic review from Coombes et al.15 showed that corticosteroid injection was effective in the short-term, yet produced negative outcomes at 6-months and 12-months.
Even when a corticosteroid injection does not improve long-term outcomes, some patients and clinicians may be unwilling to wait several months to achieve pain resolution and functional improvement, particularly when a timely return to physically demanding work or sport is needed. An observation-only approach may lead to short-term disability and pain, with the corresponding economic cost and lost productivity46, 47. Thus, we believe that the use of a corticosteroid injection may depend on the severity and duration of the symptoms.
The variation in treatment outcomes in previous studies might be attributed to differences inherent to the studies, such as severity of the disease, occupational state, and concurrent medical condition of the participants. Female gender, high baseline pain and disability, and long symptom duration have been associated with poor treatment outcomes for LE48, 49. Previous studies have demonstrated that the presence of diabetes mellitus is associated with a worse response to corticosteroid injections50,51,52, but studies of patients with medical comorbidities other than diabetes mellitus are lacking. In this study, although significant improvements in symptom severity and hand function similar to those of LE patients without MetS occurred at 24 weeks after corticosteroid injection, the MetS group had worse functional outcomes than those without MetS in terms of pain NRS scores, DASH scores, and grip strength in the early post-injection period (up to 12 weeks).
There were several limitations to our study. First, the assessment included short-term results, which stand in contrast with the chronic nature of LE, and this impedes having a better understanding of the natural course of the pain and function of LE. On the other hand, LE is a self-limiting condition, and functional improvements may be partially attributable to the natural history of the condition. Thus, the main purpose of treatment may be to shorten the duration of the symptoms and disability. Moreover, a 24-week follow-up is believed to be sufficient to evaluate the effect15. Second, the pharmacokinetics and effective dosage of locally administered corticosteroid have not been properly established, and the regimen in this study may not be optimal in its effectiveness and safety, even though its administration was determined in previous studies. Third, only one type of questionnaire was used to assess the functional outcomes of the patients. The minimal clinically important differences or responsiveness of the questionnaires after corticosteroid injection may differ between functional assessments, and another type of functional assessment might result in different conclusions. Third, 13 (13%) patients were lost to follow-up before the 6-month evaluation, and there were some missing questions and questionnaires in our cohort. Finally, the patients were limited to one ethnic population drawn from an urban area. Therefore, their characteristics and the study results may not be generalizable to other populations.
Conclusion
The results of this study suggest that patients with LE and MetS are at risk for higher pain scores and lower functional outcomes after the corticosteroid injection for LE in the short term, but in the long term there was no difference in outcomes of steroid injection in the MetS and non-MetS group.
References
Verhaar, J. A. Tennis elbow. Anatomical, epidemiological and therapeutic aspects. Int Orthop 18, 263–267 (1994).
Sayegh, E. T. & Strauch, R. J. Does nonsurgical treatment improve longitudinal outcomes of lateral epicondylitis over no treatment? A meta-analysis. Clin Orthop Relat Res 473, 1093–1107 (2015).
Hong, Q. N., Durand, M. J. & Loisel, P. Treatment of lateral epicondylitis: where is the evidence? Joint Bone Spine 71, 369–373 (2004).
Svernlov, B. & Adolfsson, L. Non-operative treatment regime including eccentric training for lateral humeral epicondylalgia. Scand J Med Sci Sports 11, 328–334 (2001).
Melikyan, E. Y., Shahin, E., Miles, J. & Bainbridge, L. C. Extracorporeal shock-wave treatment for tennis elbow. A randomised double-blind study. J Bone Joint Surg Br 85, 852–855 (2003).
Kachooei, A. R., Talaei-Khoei, M., Faghfouri, A. & Ring, D. Factors associated with operative treatment of enthesopathy of the extensor carpi radialis brevis origin. J Shoulder Elbow Surg 25, 666–670 (2016).
Smidt, N. et al. Corticosteroid injections, physiotherapy, or a wait-and-see policy for lateral epicondylitis: a randomised controlled trial. Lancet 359, 657–662 (2002).
Bisset, L. et al. Mobilisation with movement and exercise, corticosteroid injection, or wait and see for tennis elbow: randomised trial. BMJ 333, 939 (2006).
Coombes, B. K., Bisset, L., Brooks, P., Khan, A. & Vicenzino, B. Effect of corticosteroid injection, physiotherapy, or both on clinical outcomes in patients with unilateral lateral epicondylalgia: a randomized controlled trial. JAMA 309, 461–469 (2013).
Stefanou, A., Marshall, N., Holdan, W. & Siddiqui, A. A randomized study comparing corticosteroid injection to corticosteroid iontophoresis for lateral epicondylitis. J Hand Surg Am 37, 104–109 (2012).
Mardani-Kivi, M. et al. The effects of corticosteroid injection versus local anesthetic injection in the treatment of lateral epicondylitis: a randomized single-blinded clinical trial. Arch Orthop Trauma Surg 133, 757–763 (2013).
Verhaar, J. A., Walenkamp, G. H., van Mameren, H., Kester, A. D. & van der Linden, A. J. Local corticosteroid injection versus Cyriax-type physiotherapy for tennis elbow. J Bone Joint Surg Br 78, 128–132 (1996).
Wolf, J. M., Ozer, K., Scott, F., Gordon, M. J. & Williams, A. E. Comparison of autologous blood, corticosteroid, and saline injection in the treatment of lateral epicondylitis: a prospective, randomized, controlled multicenter study. J Hand Surg Am 36, 1269–1272 (2011).
Krogh, T. P. et al. Treatment of lateral epicondylitis with platelet-rich plasma, glucocorticoid, or saline: a randomized, double-blind, placebo-controlled trial. Am J Sports Med 41, 625–635 (2013).
Coombes, B. K., Bisset, L. & Vicenzino, B. Efficacy and safety of corticosteroid injections and other injections for management of tendinopathy: a systematic review of randomised controlled trials. Lancet 376, 1751–1767 (2010).
Expert Panel on Detection, E. & Treatment of High Blood Cholesterol in, A. Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA 285, 2486-2497 (2001).
Bloomgarden, Z. T. American Association of Clinical Endocrinologists (AACE) consensus conference on the insulin resistance syndrome: 25–26 August 2002, Washington, DC. Diabetes Care 26, 933–939 (2003).
Ford, E. S., Giles, W. H. & Dietz, W. H. Prevalence of the metabolic syndrome among US adults: findings from the third National Health and Nutrition Examination Survey. JAMA 287, 356–359 (2002).
Abate, M., Schiavone, C., Salini, V. & Andia, I. Occurrence of tendon pathologies in metabolic disorders. Rheumatology (Oxford) 52, 599–608 (2013).
Gaida, J. E., Ashe, M. C., Bass, S. L. & Cook, J. L. Is adiposity an under-recognized risk factor for tendinopathy? A systematic review. Arthritis Rheum 61, 840–849 (2009).
Gaida, J. E., Alfredson, H., Kiss, Z. S., Bass, S. L. & Cook, J. L. Asymptomatic Achilles tendon pathology is associated with a central fat distribution in men and a peripheral fat distribution in women: a cross sectional study of 298 individuals. BMC Musculoskelet Disord 11, 41 (2010).
von Bahr, S. et al. Mechanism of accumulation of cholesterol and cholestanol in tendons and the role of sterol 27-hydroxylase (CYP27A1). Arterioscler Thromb Vasc Biol 22, 1129–1135 (2002).
Tilley, B. J., Cook, J. L., Docking, S. I. & Gaida, J. E. Is higher serum cholesterol associated with altered tendon structure or tendon pain? A systematic review. Br J Sports Med 49, 1504–1509 (2015).
Zimmet, P. Z., Alberti, K. G. & Shaw, J. E. Mainstreaming the metabolic syndrome: a definitive definition. Med J Aust 183, 175–176 (2005).
Moy, F. M. & Bulgiba, A. The modified NCEP ATP III criteria maybe better than the IDF criteria in diagnosing Metabolic Syndrome among Malays in Kuala Lumpur. BMC Public Health 10, 678 (2010).
Hudak, P. L., Amadio, P. C. & Bombardier, C. Development of an upper extremity outcome measure: the DASH (disabilities of the arm, shoulder and hand) [corrected]. The Upper Extremity Collaborative Group (UECG). Am J Ind Med 29, 602–608 (1996).
Szabo, R. M. Outcomes assessment in hand surgery: when are they meaningful? J Hand Surg Am 26, 993–1002 (2001).
Gummesson, C., Atroshi, I. & Ekdahl, C. The disabilities of the arm, shoulder and hand (DASH) outcome questionnaire: longitudinal construct validity and measuring self-rated health change after surgery. BMC Musculoskelet Disord 4, 11 (2003).
Franchignoni, F. et al. Minimal clinically important difference of the disabilities of the arm, shoulder and hand outcome measure (DASH) and its shortened version (QuickDASH). J Orthop Sports Phys Ther 44, 30–39 (2014).
Schafer, J. L. Multiple imputation: a primer. Stat Methods Med Res 8, 3–15 (1999).
Huang, H. K. et al. Outcomes and complications after percutaneous release for trigger digits in diabetic and non-diabetic patients. J Hand Surg Eur Vol 40, 735–739 (2015).
Ranger, T. A., Wong, A. M., Cook, J. L. & Gaida, J. E. Is there an association between tendinopathy and diabetes mellitus? A systematic review with meta-analysis. Br J Sports Med 50, 982–989 (2016).
Wu, Y. F. et al. High glucose alters tendon homeostasis through downregulation of the AMPK/Egr1 pathway. Sci Rep 7, 44199 (2017).
Tsai, W. C. et al. High glucose concentration up-regulates the expression of matrix metalloproteinase-9 and -13 in tendon cells. BMC Musculoskelet Disord 14, 255 (2013).
Reddy, G. K. Glucose-mediated in vitro glycation modulates biomechanical integrity of the soft tissues but not hard tissues. J Orthop Res 21, 738–743 (2003).
Burner, T., Gohr, C., Mitton-Fitzgerald, E. & Rosenthal, A. K. Hyperglycemia reduces proteoglycan levels in tendons. Connect Tissue Res 53, 535–541 (2012).
Li, Y., Fessel, G., Georgiadis, M. & Snedeker, J. G. Advanced glycation end-products diminish tendon collagen fiber sliding. Matrix Biol 32, 169–177 (2013).
Ames, J. B., Horan, M. P., Van der Meijden, O. A., Leake, M. J. & Millett, P. J. Association between acromial index and outcomes following arthroscopic repair of full-thickness rotator cuff tears. J Bone Joint Surg Am 94, 1862–1869 (2012).
Frey, C. & Zamora, J. The effects of obesity on orthopaedic foot and ankle pathology. Foot Ankle Int 28, 996–999 (2007).
Gaida, J. E. et al. Dyslipidemia in Achilles tendinopathy is characteristic of insulin resistance. Med Sci Sports Exerc 41, 1194–1197 (2009).
Jozsa, L., Reffy, A. & Balint, J. B. The pathogenesis of tendolipomatosis ; an electron microscopical study. Int Orthop 7, 251–255 (1984).
Finlayson, R. & Woods, S. J. Lipid in the Achilles tendon. A comparative study. Atherosclerosis 21, 371–389 (1975).
Beason, D. P., Abboud, J. A., Kuntz, A. F., Bassora, R. & Soslowsky, L. J. Cumulative effects of hypercholesterolemia on tendon biomechanics in a mouse model. J Orthop Res 29, 380–383 (2011).
Calfee, R. P., Patel, A., DaSilva, M. F. & Akelman, E. Management of lateral epicondylitis: current concepts. J Am Acad Orthop Surg 16, 19–29 (2008).
Claessen, F. M., Heesters, B. A., Chan, J. J., Kachooei, A. R. & Ring, D. A Meta-Analysis of the Effect of Corticosteroid Injection for Enthesopathy of the Extensor Carpi Radialis Brevis Origin. J Hand Surg Am2016).
Korthals-de Bos, I. B. et al. Cost effectiveness of interventions for lateral epicondylitis: results from a randomised controlled trial in primary care. Pharmacoeconomics 22, 185–195 (2004).
Sanders, T. L., Maradit Kremers, H., Bryan, A. J., Ransom, J. E. & Morrey, B. F. Health Care Utilization and Direct Medical Costs of Tennis Elbow: A Population-Based Study. Sports Health 8, 355–358 (2016).
Solheim, E., Hegna, J. & Oyen, J. Extensor tendon release in tennis elbow: results and prognostic factors in 80 elbows. Knee Surg Sports Traumatol Arthrosc 19, 1023–1027 (2011).
Waugh, E. J., Jaglal, S. B., Davis, A. M., Tomlinson, G. & Verrier, M. C. Factors associated with prognosis of lateral epicondylitis after 8 weeks of physical therapy. Arch Phys Med Rehabil 85, 308–318 (2004).
Baumgarten, K. M., Gerlach, D. & Boyer, M. I. Corticosteroid injection in diabetic patients with trigger finger. A prospective, randomized, controlled double-blinded study. J Bone Joint Surg Am 89, 2604–2611 (2007).
Rozental, T. D., Zurakowski, D. & Blazar, P. E. Trigger finger: prognostic indicators of recurrence following corticosteroid injection. J Bone Joint Surg Am 90, 1665–1672 (2008).
Kameyama, M., Funae, O., Meguro, S. & Atsumi, Y. HbA1c values determine the outcome of intrasheath injection of triamcinolone for diabetic flexor tenosynovitis. Diabetes Care 29, 2512–2514 (2006).
Author information
Authors and Affiliations
Contributions
Y.H.R. and J.H.N. designed the experiments, wrote the protocol, collected the data and took responsibility for the integrity of the data. Y.H.R. and M.O. performed data analysis and wrote the manuscript. H.S.G. and G.H.B. reviewed the manuscript. All authors have approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing Interests
The authors declare that they have no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Roh, Y.H., Oh, M., Noh, J.H. et al. Effect of Metabolic Syndrome on the Functional Outcome of Corticosteroid Injection for Lateral Epicondylitis: Retrospective Matched Case-Control Study. Sci Rep 7, 10845 (2017). https://doi.org/10.1038/s41598-017-11179-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-017-11179-z
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
