
Abstract
Remote ischemic preconditioning (RIPC) by repeated brief cycles of limb ischemia/reperfusion reduces myocardial ischemia/reperfusion injury. In left ventricular (LV) biopsies from patients undergoing coronary artery bypass grafting (CABG), only the activation of signal transducer and activator of transcription 5 was associated with RIPC’s cardioprotection. We have now used an unbiased, non-hypothesis-driven proteomics and phosphoproteomics approach to analyze LV biopsies from patients undergoing CABG and from pigs undergoing coronary occlusion/reperfusion without (sham) and with RIPC. False discovery rate-based statistics identified a higher prostaglandin reductase 2 expression at early reperfusion with RIPC than with sham in patients. In pigs, the phosphorylation of 116 proteins was different between baseline and early reperfusion with RIPC and/or with sham. The identified proteins were not identical for patients and pigs, but in-silico pathway analysis of proteins with ≥2-fold higher expression/phosphorylation at early reperfusion with RIPC in comparison to sham revealed a relation to mitochondria and cytoskeleton in both species. Apart from limitations of the proteomics analysis per se, the small cohorts, the sampling/sample processing and the number of uncharacterized/unverifiable porcine proteins may have contributed to this largely unsatisfactory result.
Similar content being viewed by others

Introduction
Remote ischemic conditioning by brief episodes of ischemia/reperfusion in parenchymal organs or limbs before (pre-) or during (per-) sustained myocardial ischemia and subsequent reperfusion protects the myocardium from ischemia/reperfusion injury. The protection by remote ischemic conditioning has been confirmed in all species tested so far, including humans1,2,3,4. The reduction of myocardial ischemia/reperfusion injury by remote ischemic conditioning has been demonstrated in patients undergoing elective interventional5 or surgical coronary revascularization6,7,8,9, and in patients with acute myocardial infarction10,11,12,13,14,15. The protection was confirmed by a reduction in cardiac biomarker release5,6,7,8,9, 14 or by cardiac imaging10, 12, 13, 15, and it was associated with improved short-8, 12 and long-term clinical outcome5, 7, 11. In contrast, two recent large-scaled randomized trials in patients undergoing cardiac surgery, ERICCA and RIPHeart, failed to confirm reduced biomarker release and improved clinical outcome with remote ischemic preconditioning (RIPC)16, 17. The use of propofol anesthesia in the majority of patients in both trials may have abrogated the cardioprotective effect of RIPC18, 19. The magnitude of myocardial ischemia/reperfusion injury may also affect the extent of RIPC’s protection. In patients undergoing coronary artery bypass grafting (CABG), greater myocardial injury by longer cross-clamp time facilitated the manifestation of cardioprotection by RIPC20. Along this line, in patients undergoing transfemoral transcatheter aortic valve implantation with only short duration of peri-interventional ischemia and with less troponin I release, RIPC did not provide protection21.
In order to fully recruit the cardioprotection by RIPC and to improve patient outcome it is necessary to understand the signal transduction of RIPC. The signaling pathways recruited by remote and local ischemic conditioning maneuvers appear to be similar22. Conceptually, the signal transduction comprises triggers which activate intracellular mediator cascades to ultimately transmit the cardioprotective signal to end-effectors, notably the mitochondria23. Numerous studies using Western blot analysis, pharmacological agonist and antagonist approaches, and genetic approaches in various experimental models identified a number of signaling proteins, which were conceptually summarized as the nitric oxide synthase/protein kinase G pathway, the reperfusion injury salvage kinase pathway, and the survival activating factor enhancement pathway24, 25. The activation and expression of 22 signaling proteins that had previously been identified in experimental models in response to ischemic conditioning maneuvers were analyzed using Western blot analysis in left ventricular (LV) biopsies taken at early reperfusion after cardioplegic ischemic arrest from patients undergoing CABG under isoflurane anesthesia26, 27. Among these 22 proteins, only the activation of the signal transducer and activator of transcription 5 (STAT5) was associated with reduced biomarker release by RIPC26. In pigs, STAT3 but not STAT5 activation is causally involved in cardioprotection by RIPC28, reflecting species-specific differences in the signal transduction of RIPC24. The up- and downstream signals of STAT5/STAT3 as well as other, not previously described pathways in signal transduction of RIPC have not been identified yet. An unbiased, non-hypothesis-driven analysis of myocardial tissue may therefore provide new insights into the signal transduction and identify novel therapeutic targets of RIPC29,30,31,32. We have therefore now analyzed and compared the proteome and phosphoproteome of LV biopsies taken at early reperfusion after cardioplegic ischemic arrest from patients undergoing CABG without (sham) and with RIPC. Whereas proteome analysis at early reperfusion most likely reflects RIPC-related differences in proteolysis by ischemia rather than protein biosynthesis, the phosphoproteome analysis was aimed to identify the potential activation of cardioprotective proteins by RIPC. Indeed, the majority of cardioprotective proteins are regulated by posttranslational modifications, mainly by phosphorylation33. For comparison, we used the translational pig model with coronary occlusion/reperfusion without (sham) or with RIPC28, to analyze the proteome and phosphoproteome of LV biopsies taken at baseline before coronary occlusion/reperfusion and at early reperfusion. This animal model has less interindividual variability than that of patients and no co-morbidities and co-medications34.
Results
Cardioprotection by RIPC
In patients, demographics, baseline and intraoperative characteristics were not different between those with RIPC and with sham (Table 1). The preoperative serum troponin I concentration (cTnI) did not differ between patients with RIPC and with sham. The cTnI release was decreased by RIPC (area under the curve (AUC) over 72 h: 218 ± 28 versus 569 ± 134 ng/ml × 72 h, p = 0.018; Fig. 1a). In pigs, the area at risk (24 ± 2 versus 23 ± 2% of the LV) was not different between RIPC (24 ± 2% of the LV) and sham (23 ± 2%). Transmural blood flow within the area at risk was reduced at 5 min ischemia from baseline (RIPC: 0.023 ± 0.004 versus 0.780 ± 0.027 ml/min/g; sham: 0.023 ± 0.004 versus 0.718 ± 0.035 ml/min/g). RIPC reduced infarct size (Fig. 1b).

Serum concentration of troponin I of patients. (a) The serum concentration of troponin I before (preop) and over 72 h after coronary artery bypass grafting (CABG) in patients undergoing remote ischemic preconditioning (RIPC; black symbols/bars) or sham (white symbols/bars). Decreased troponin I concentrations confirmed protection by RIPC. Insert: area under the curve (AUC) for serum troponin I concentrations over 72 h. (b) Infarct size of pigs after 60 min coronary occlusion and 180 min reperfusion. Protection by RIPC was confirmed by infarct size reduction. Data are mean ± standard error of the mean. The data were compared using a 2-way (group, time) ANOVA for repeated measures or using unpaired Student’s t-test (AUC, infarct size).
Comparable sample composition in the individual LV biopsies
In human LV biopsies, the expressions of proteins characterizing the different cell types, i.e. CD31, collagen 3α, hemoglobin γ, enolase 2 and tropomyosin, were comparable between RIPC and sham when lysed with Tris/sodium dodecyl sulfate (SDS) and radioimmunoprecipitation assay (RIPA) buffer, respectively (Supplemental Figs S1a and S2a and b). In porcine LV biopsies, the expressions of these proteins were also not different between baseline and early reperfusion and between RIPC and sham, respectively (Supplemental Figs S1b and S3).
Western blot analysis of STAT5 in human and STAT3 in porcine LV biopsies
Confirming our prior reports26, 27, the STAT5 phosphorylation in human LV biopsies taken at early reperfusion tended to be higher with RIPC than with sham when lysed with Tris/SDS buffer and with RIPA buffer (Fig. 2a and Supplemental Fig. S4a). Also confirming our prior report28, the STAT3 phosphorylation in porcine LV biopsies tended to be increased from baseline to early reperfusion after coronary occlusion with RIPC, and STAT3 phosphorylation during early reperfusion tended to be higher in pigs with RIPC than with sham (Fig. 2b and Supplemental Fig. S4b).

Western blot analysis of phosphorylation/expression of STAT5 in human and of STAT3 in porcine left ventricular biopsies. (a) The phosphorylation of signal transducer and activator of transcription 5 (STAT5) at tyr694 tended to be increased at early reperfusion with remote ischemic preconditioning (RIPC; black symbols) compared to that with sham (white symbols) in human left ventricular (LV) biopsies lysed in Tris/sodium dodecyl sulfate (SDS) or radioimmunoprecipitation assay (RIPA) buffer. (b) The phosphorylation of signal transducer and activator of transcription 3 (STAT3) at tyr705 tended to be increased from baseline to early reperfusion after coronary occlusion with RIPC, and tended to be greater with RIPC than with sham in porcine LV biopsies. Immunoreactivities of the phosphorylated proteins were normalized to the respective total forms and compared by unpaired (between RIPC and sham) or by paired (between baseline and early reperfusion in pigs) Student’s t-tests. The blots were cropped to display the relevant bands, full-length blots and Ponceau-S stainings are presented in Supplemental Fig. S4.
Proteome and phosphoproteome analysis of human and porcine LV biopsies
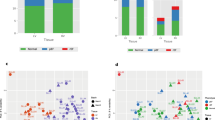
The proteome analysis of human LV biopsies taken at early reperfusion and lysed in Tris/SDS buffer detected 652 proteins after in-solution digestion and 1614 phosphorylation sites after phosphopeptide enrichment. Among these phosphopeptides, 1470 phosphorylation sites were associated with 391 proteins. The proteome analysis detected 3390 proteins after in-gel digestion and 2077 proteins after RIPA lysis and in-solution digestion (Fig. 3, line (a)). The false discovery rate (FDR)-based statistical analysis of all detected proteins/phosphopeptides in human LV biopsies did not identify a different protein expression/activation pattern with RIPC versus sham after phosphopeptide enrichment, in-gel digestion and in-solution digestion (Tris/SDS buffer), respectively (Fig. 4a–c). However, in RIPA buffer-lysed human LV biopsies taken at early reperfusion, there was a shift towards a greater number of proteins which had higher expression with RIPC than with sham (Fig. 4d). The FDR-based statistical analysis identified prostaglandin reductase 2 at higher expression at early reperfusion with RIPC than with sham.

Flow chart of sampling and proteome analysis of human left ventricular biopsies. Human left ventricular (LV) biopsies from patients without (sham) or with remote ischemic preconditioning (RIPC) were lysed in Tris/sodium dodecyl sulfate (Tris/SDS) or in radioimmunoprecipitation assay (RIPA) buffer. Proteome analysis was performed after phosphopeptide enrichment, in-solution digestion, and in-gel digestion with Tris/SDS buffer-lysed biopsies and after in-solution digestion with RIPA buffer-lysed biopsies, respectively. The numbers of all detected phosphopeptides/proteins were displayed in line (a), those with ≥2-fold higher phosphorylation/expression in line (b) and with significant (p < 0.05) ≥2-fold higher phosphorylation/expression with RIPC versus with sham in line (c), as well as those exclusively detected with RIPC or with sham in line (d). The sum of line (b), (c) and (d) was displayed in line (e). All detected phosphopeptides/proteins (line (a)) were subjected to false discovery rate (FDR)-based statistical analysis. Independently of lysis and digestion methods, all proteins detected with a ≥2-fold higher phosphorylation/expression with RIPC versus with sham and those exclusively detected in one group, respectively, were considered (line (f)) for an in-silico pathway analysis.

Vulcano plots of all detected proteins in the phosphoproteome/proteome analysis in human left ventricular biopsies. Vulcano plots of −Log(10)p-value over -fold higher phosphorylation/expression between groups (remote ischemic preconditioning (RIPC)/sham) of all proteins detected after (a) phosphopeptide enrichment, (b) in-gel digestion, (c) in-solution digestion of Tris/sodium dodecyl sulfate (Tris/SDS) and (d) radioimmunoprecipitation assay (RIPA) buffer-lysed human left ventricular biopsies taken at early reperfusion. A −Log(10)p-value of ≥1.3 corresponds to a p-value of ≤0.05. The false discovery rate (FDR) significance cut-off curve indicates only a significant increase of prostaglandin reductase 2 with RIPC than with sham in human biopsies lysed in RIPA buffer. Grey squares: phosphopeptides/proteins without FDR-based statistical difference between RIPC and sham. Black square: protein with FDR-based statistical difference between RIPC and sham.
The proteome analysis of porcine LV biopsies taken at baseline and early reperfusion detected 3660 and 3674 proteins after in-solution digestion and 2321 and 2452 phosphorylation sites after phosphopeptide enrichment, respectively. The comparison of the proteome analysis between RIPC and sham revealed 3706 and 3650 proteins after in-solution digestion and 2404 and 2405 phosphorylation sites after phosphopeptide enrichment (Fig. 5, line (a)), respectively.

Flow chart of sampling and proteome analysis of porcine left ventricular biopsies. Porcine left ventricular (LV) biopsies from pigs without (sham) or with remote ischemic preconditioning (RIPC) were taken at baseline and at early reperfusion and lysed in Tris/sodium dodecyl sulfate buffer (Tris/SDS). Proteome analysis was performed after phosphopeptide enrichment and in-solution digestion. The numbers of all detected phosphopeptides/proteins were displayed in line (a), those with ≥2-fold higher phosphorylation/expression in line (b), these with significant (p < 0.05) ≥2-fold higher phosphorylation/expression between groups (RIPC/sham) or between time points (baseline/early reperfusion), respectively, in line (c), and those exclusively detected in one group (RIPC/sham) or at one time point (baseline/early reperfusion) in line (d). The sum of lines (b), (c) and (d) was displayed in line (e). All detected phosphopeptides/proteins (line (a)) were subjected to false discovery rate (FDR)-based statistical analysis. All proteins detected at early reperfusion with a ≥2-fold higher phosphorylation/expression with RIPC than with sham (line (f)), were considered for an in-silico pathway analysis.
In porcine LV biopsies, there was no FDR-based statistical difference in the protein expression between baseline and early reperfusion or between RIPC and sham, respectively (Supplemental Fig. S5). There was also no difference in the protein phosphorylation at baseline between RIPC and sham (Fig. 6a and Table 2). The FDR-based statistical analysis revealed a higher phosphorylation of 3 proteins at early reperfusion with RIPC than with sham (Fig. 6b and Table 2). In pigs with RIPC, the comparison between baseline and early reperfusion revealed a decrease in 1 and an increase in phosphorylation of 47 proteins from baseline to early reperfusion (Fig. 6c and Table 2). In pigs with sham, the phosphorylation of 42 proteins was decreased and that of 82 proteins increased from baseline to early reperfusion (Fig. 6d and Table 2). Independent of the FDR-based statistical analysis, there was obviously a shift towards a greater number of proteins with increased phosphorylation at early reperfusion with RIPC than with sham (Fig. 6b and c).

Vulcano plots of all detected phosphopeptides after phosphoproteome phosphopeptide enrichement of porcine left ventricular biopsies. Vulcano plots of −Log(10)p-value over -fold higher phosphorylation of all proteins between groups (remote ischemic preconditioning (RIPC)/sham) detected after phosphopeptide enrichment of porcine left ventricular biopsies taken (a) at baseline and (b) at early reperfusion. Vulcano plots of −Log(10)p-value over -fold higher phosphorylation of all proteins in the comparison between time points (baseline versus early reperfusion) (c) with remote ischemic preconditioning (RIPC) and (d) with sham. A −Log(10)p-value of ≥1.3 corresponds to a p-value of ≤0.05. The false discovery rate (FDR) significance cut-off curve indicates differences in protein phosphorylation between RIPC and sham at early reperfusion and between time points (baseline/early reperfusion) with RIPC and with sham, respectively. Grey squares: phosphopeptides without FDR-based statistical difference between RIPC and sham or between baseline and early reperfusion. Black squares: phosphopeptides with FDR-based statistical difference between RIPC and sham or between baseline and early reperfusion.
The FDR-based statistically identified 175 phosphorylation sites which were associated with 116 different proteins, 39 of which were phosphorylation sites of 20 previously uncharacterized proteins (Table 2). There was an overlap of 48 phosphorylation sites of 21 identified proteins at early reperfusion with both, RIPC and sham, suggesting that phosphorylation of these proteins was induced by coronary occlusion/reperfusion per se. Fourty of these identified proteins were previously not described in cardiac cells, however, 45 proteins were previously described in cardiac cells, among them 4 in the context of ischemia/reperfusion, and 7 in relation to cardioprotection or ischemic conditioning maneuvers (Table 3).
Comparison and verification of proteome/phosphoproteome analysis with Western blot analysis
In human LV biopsies taken at early reperfusion and lysed with RIPA buffer, the FDR-based statistical analysis identified prostaglandin reductase 2 at ≥2-fold higher expression with RIPC than with sham after in-solution digestion. This ≥2-fold higher expression of prostaglandin reductase 2 with RIPC than with sham was also detected in the Tris/SDS buffer-lysed biopsies after in-solution digestion, but without FDR-based statistical significance (Fig. 7a and Supplemental Table S1 (ID: Q8N8N7)). The higher expression of prostaglandin reductase 2 with RIPC than with sham in RIPA buffer-lysed human LV biopsies was confirmed by Western blot analysis, whereas its expression in Tris/SDS buffer-lysed biopsies was not significantly higher with RIPC than with sham, in line with the FDR-based statistical analysis (Fig. 7a and Supplemental Fig. S6).

Comparison between proteome/phosphoproteome and Western blot analysis of prostaglandin reductase 2, α-crystallin B, α-endosulfine and p62 expression/phosphorylation. (a) The expression of prostaglandin reductase 2 (PGR2) in Tris/sodium dodecyl sulfate (Tris/SDS) and in radioimmunoprecipitation assay (RIPA) buffer lysed human left ventricular (LV) biopsies with remote ischemic preconditioning (RIPC; black symbols) and with sham (white symbols) in the proteome and in the Western blot analysis. The higher expression of PGR2 with RIPC than with sham in RIPA buffer-lysed human LV biopsies was confirmed by Western blot analysis. The immunoreactivity of PGR2 was normalized to Ponceau-S staining. The phosphorylation of (b) α-crystallin B at ser59, (c) α-endosulfine at ser67 and (d) p62 at thr269/ser272 in the phosphoproteome and in the Western blot analysis with RIPC and with sham in porcine left ventricular biopsies taken at baseline and at early reperfusion. The phosphoproteome analysis was verified by Western blot analysis for α-crystallin B and p62, but not for α-endosulfine. The immunoreactivities of the phosphorylated proteins were normalized to the respective total forms and compared by unpaired (between RIPC and sham) or by paired (between baseline and early reperfusion) Student’s t-tests. Total α-endosulfine was not detectable, therefore phosphorylated α-endosulfine was normalized to Ponceau-S staining. The blots were cropped to display the relevant bands, full-length blots and Ponceau-S stainings are presented in Supplemental Figs S6 and S7.
In porcine LV biopsies, the FDR-based statistical analysis identified a total of 175 phosphorylation sites, which were different between RIPC and sham at early reperfusion or between baseline and early reperfusion with RIPC or sham, respectively (Table 2). However, only 3 antibodies were commercially available to detect the respective phosphorylation sites, i.e. for: α-crystallin B, α-endosulfine, and p62.
The phosphorylation of α-crystallin B at ser59 was increased in the time course from baseline to early reperfusion with RIPC. This increased phopsphorylation was confirmed by Western blot analysis. However also with sham, phosphoproteome and Western blot analysis identified an increased phosphorylation of α-crystallin from baseline to early reperfusion by trend (Fig. 7b and Supplemental Fig. S7). The proteome and the Western blot analysis did not reveal any difference of α-crystallin B expression between baseline and early reperfusion and between RIPC and sham, respectively.
The decrease in the phosphorylation of α-endosulfine at ser67 from baseline to early reperfusion with sham by phosphoproteome analysis was confirmed by Western blot analysis. However, different from the phosphoproteome analysis, the phosphorylation of α-endosulfine was also decreased from baseline to early reperfusion with RIPC and was higher with RIPC than with sham at baseline in the Western blot analysis (Fig. 7c and Supplemental Fig. S7). The expression of α-endosulfine was not detectable with the used antibody in the Western blot analysis; its expression was also not detected in the proteome analysis.
Increased phosphorylation of p62 at ser272 at from baseline to early reperfusion with sham was confirmed via Western blot analysis by trend, when normalized to total p62 (Fig. 7d and Supplemental Fig. S7). However, this antibody detected phosphorylation of p62 not only at ser272, but also at thr269. The proteome analysis did not detect p62 expression per se.
In-silico pathway analysis of human and porcine LV biopsies: relation to mitochondria and cytoskeleton
AIl proteins detected in human and in porcine LV biopsies taken at early reperfusion which had ≥2-fold higher phosphorylation/expression with RIPC than with sham (Figs 3 and 5, line (f)), respectively, were considered for an in-silico pathway analysis. Almost none of these proteins displayed conformity between humans and pigs; only 15% and 8% of the proteins were detected at early reperfusion in both species with RIPC or with sham, respectively.
In human LV biopsies, we identified 774 proteins which had ≥2-fold higher expression/phosphorylation with RIPC than with sham and 379 proteins which had ≥2-fold higher expression/phosphorylation with sham than with RIPC (Fig. 3, line (f)). A comparison between these proteins identified in more than one lysis or digestion method just 30 of the total 774 proteins at higher expression with RIPC and 6 of the total 379 proteins at higher expression with sham, respectively (Supplemental Tables S1–S4).
In porcine LV biopsies taken at early reperfusion, 611 proteins had ≥2-fold higher expression/phosphorylation with RIPC than with sham and 374 proteins had ≥2-fold higher expression/phosphorylation with sham than with RIPC (Fig. 5, line (f), Supplemental Tables S5 and S4), but 115 (RIPC) and 117 (sham) proteins were labeled as uncharacterized proteins, and therefore could not be analyzed further. In-silico analysis revealed similar pathways for both species: proteins having higher expression/phosphorylation at early reperfusion with RIPC than with sham were related to mitochondrial function, cytoskeleton and epithelial adherens junction signaling, proteins having higher expression/phosphorylation with sham than with RIPC were related to tight junction signaling (Fig. 8 and Table 4).

In-silico pathway analysis. Independently of lysis and digestion methods, all proteins detected at a ≥2-fold higher expression/phosphorylation with RIPC versus with sham and those exclusively detected in one group (RIPC/sham) at early reperfusion in human and porcine LV biopsies were considered for an Ingenuity pathway analysis. This pathway analysis does not distinguish between activation (phosphorylation) or expression of the detected proteins. (a) Proteins having higher expression/phosphorylation with RIPC than with sham in human LV biopsies at early reperfusion after cardioplegic ischemic arrest are related to mitochondrial function, cytoskeleton and transcription/translation. (b) Proteins having higher expression/phosphorylation with RIPC than with sham in porcine LV biopsies at early reperfusion after coronary occlusion are related to mitochondrial function and cytoskeleton. Proteins marked in black had higher expression/phosphorylation with RIPC than with sham, and proteins marked in grey had higher expression/phosphorylation with sham than with RIPC. Continuous arrows are reflecting direct relations and broken arrows are reflecting indirect relations. APP: amyloid precursor protein, c-RAF: rapidly accelerated fibrosarcoma, ERK1/2: mitogen-activated protein kinase 3/mitogen-activated protein kinase 1, STAT1/3: signal transducer and activator of transcription 1/3, TRAK: trafficking kinesin protein, VDAC: voltage-dependent anion channel.
Discussion
The current unbiased, non-hypothesis-driven proteomics approach to analysis of human LV biopsies taken at early reperfusion after cardioplegic ischemic arrest identified only prostaglandin reductase 2, but no other established or previously unknown differences in protein expression by cardioprotection with RIPC. The phosphoproteome analysis of porcine LV biopsies, however, identified some phosphoproteins, which may be potential candidates for further analysis of cardioprotective signals.
In both species, the protection as such was confirmed in phosphoproteome/proteome analysis by higher tissue expression/activation of troponin I and troponin T with RIPC than with sham (Supplemental Tables S1 and S3).
A differential expression of total protein in LV biopsies from patients undergoing RIPC has not been reported so far26, 27, and indeed biosynthesis of new proteins is unlikely in the short time interval between the end of the RIPC/sham maneuver and the biopsy sampling at early reperfusion after cardioplegic ischemic arrest (Table 1). Therefore, changes in protein expression most likely reflect changes in proteolysis induced by ischemia. However, the FDR-based statistical analysis only identified prostaglandin reductase 2 at higher expression with RIPC than with sham in human LV biopsies. Prostaglandins are associated with cardioprotection by local ischemic preconditioning in pigs35 (Table 3). Thus, prostaglandin signaling may indeed be involved in cardioprotection by RIPC in the human myocardium. Again, however, a decreased proteolysis of prostaglandin reductase 2 by RIPC could cause this difference in expression, and the relative increase of prostaglandin reductase 2 in myocardium with RIPC than with sham may not at all reflect an increased prostaglandin concentration. Unfortunately, we were unable to determine changes in the prostaglandin concentration in the lysates from the available LV biopsies.
In porcine LV biopsies, the FDR-based statistical analysis did not identify any difference in protein expression between RIPC and sham or between baseline and early reperfusion, and thus did not confirm a higher prostaglandin reductase 2 expression at early reperfusion with RIPC than with sham.
Cardioprotective proteins are mainly regulated by phosphorylation33. Previously, we and others have used Western blot analysis and reported an increased phosphorylation of STAT5 in patients26, 27, 36 and of STAT3 in pigs28 at early reperfusion with protection by RIPC. Western blot analysis of the LV biopsies in the present study revealed a trend of increased STAT5/STAT3 phosphorylation at early reperfusion with RIPC than with sham, respectively, thus confirming our prior results. However, neither the expression nor the phosphorylation of STAT5 in patients and of STAT3 in pigs, respectively, were detected by the present proteome and phosphoproteome analysis. The extraction of high abundance-proteins and their detection via mass spectrometry37 may have hampered the detection of potentially small amounts of STAT5 or STAT3 in the proteome and phosphoproteome analysis.
In human LV biopsies, FDR-based statistical analysis did not reveal any difference in protein phosphorylation between RIPC and sham at early reperfusion. The reason for this unsatisfactory result may be related to the only small cohort of patients with its uneven distribution of co-morbidities and co-medications (Table 1), which both, potentially interfere with protection by ischemic conditioning maneuvers29, 34.
In contrast to patients, our translational pig model had less interindividual variability and no co-morbidities and co-medications34. In pigs, LV biopsies were also taken at baseline and at early reperfusion, allowing an intraindividual analysis of time course. This intraindividual comparison resulted in a relatively large yield of FDR-based statistically identified differences of protein phosphorylation between baseline and early reperfusion with RIPC and/or with sham, respectively (Table 2). Unfortunately, these identified proteins included 18% uncharacterized proteins as well as 35% candidates about which nothing is known for their role in cardiac cells. A verification of the characterized proteins via Western blot with commercially available antibodies was only possible for 3 candidates. From these 3 proteins, we indeed verified the phosphoproteome results for α-crystallin B and p62, but not for α-endosulfine. Alpha-endosulfine is a cytoplasmic, highly conserved cAMP-regulated phosphoprotein and regulator of KATP-channels, which modulates insulin secretion in the pancreas38. However, a role of α-endosulfine in cardiac cells is entirely unclear.
Among the identified proteins, 11 proteins have already been described in relation to myocardial ischemia/reperfusion and/or cardioprotection. These prior studies analyzed almost exclusively the expression and not the phosphorylation of these candidate proteins; therefore, nothing is known yet about the role of the here identified phosphorylation sites. These proteins may, however, be potential novel candidates as cardioprotective signals induced by RIPC than with sham (Table 3), and it may be worthwhile to analyze them further.
Independent of the FDR-based statistical analysis, the phosphoproteome analysis of porcine LV biopsies revealed a shift towards a greater number of proteins with increased phosphorylation at early reperfusion with RIPC than with sham (Fig. 6b and c). Such shift was not seen after phosphoproteome analysis of human LV biopsies.
Almost all identified proteins with a different expression/activation at early reperfusion were different between humans and pigs, reflecting and confirming the established species-specific differences. However, without differentiation between expression and phosphorylation of all detected proteins, the Ingenuity knowledge base identified mitochondria and cytoskeleton in association with RIPC at early reperfusion in both species. These associations may or may not relate to their causal involvement in cardioprotection by ischemic conditioning strategies (Fig. 8).
Mitochondria are well established end-effectors of cardioprotective strategies, and the preservation of mitochondrial function after ischemia/reperfusion is decisive for the survival of cardiomyocytes and thus salvage of myocardium22, 39. RIPC preserved mitochondrial respiration after ischemic cardioplegic arrest compared to sham in right atrial appendages of patients undergoing CABG40, 41. The plasma transfer from pigs, which had undergone RIPC, to isolated perfused rat hearts reduced infarct size and improved mitochondrial function at early reperfusion after global ischemia42.
The protection by simulated ischemic preconditioning was associated with attenuated osmotic fragility through cytochalasin D–sensitive stabilization of the actin cytoskeleton in isolated rabbit cardiomyocytes after simulated ischemia for 3 h43. Also, the phosphorylation of sarcomeric Z-disc associated proteins was increased immediately after the RIPC procedure compared to that after sham procedure in mice hearts44. Pharmacological interventions induced long-term expression changes of proteins related to cytoskeletal regulation in pig hearts45.
There are several limitations to our current analysis: 1) We analyzed biopsies from only a small cohort of patients with an uneven distribution of co-morbidities and co-medications (Table 1), which both, potentially interfere with ischemic conditioning maneuvers29, 34. To overcome this issue and to increase the power of a proteome analysis, the inclusion of more patients with a more balanced set of co-morbidities and co-medications would be required. 2) The size of human and porcine biopsies was small and precluded a parallel extraction of proteins from one sample with different lysis and digestion methods. A small sample size may result in a sampling error and a high variability of its cellular composition. 3) Given the small sample size, we analyzed total myocardial proteins and did not distinguish between different cellular and subcellular compartments. Proteome analysis targeting different, isolated cellular and subcellular compartments may decipher more complex, multivalent signals37. 4) We analyzed only one posttranslational protein modification, i.e. protein phosphorylation. Although cardioprotective proteins are mainly regulated by phosphorylation33, we cannot exclude differences by RIPC in other posttranslational modifications. Sufficient tissue sampling for additional analysis of acetylation, O-linked β-N-acetylglucosaminylation, S-nitrosylation, etc. was not possible. 5) Although we identified 116 proteins with a difference in phosphorylation mainly between baseline and early reperfusion in pigs with RIPC and/or with sham, only 3 antibodies were commercially available against proteins with the identified phosphorylation sites to verify the phosphoproteome data by Western blot analysis. 6) We analyzed human LV biopsies at only one time point, i.e. at early reperfusion after cardioplegic ischemic arrest. Biopsies taken at baseline after RIPC/sham, but before cardioplegic ischemic arrest were not available. Thus, in patients, we cannot distinguish between changes from baseline to early reperfusion after cardioplegic ischemic arrest induced by RIPC versus sham and, thus, between biosynthesis versus proteolysis. 6) The protein data repositories for pigs are not complete yet. In fact, 39 phosphorylation sites were identified with FDR-based statistical differences particularly between baseline and early reperfusion and had to be defined as uncharacterized proteins.
In conclusion, the current proteome and phosphoproteome analysis of human LV biopsies from patients undergoing CABG identified only prostaglandin reductase 2, but no other established difference in protein expression and activation by cardioprotection with RIPC at early reperfusion after cardioplegic ischemic arrest. However, the higher expression of prostaglandin reductase 2 with RIPC than with sham may point towards an involvement of prostaglandin metabolism in cardioprotective signaling in patients. In contrast, the phosphoproteome analysis of porcine LV biopsies taken at baseline and early reperfusion after coronary occlusion identified some previously unknown differences in protein phosphorylation between RIPC and sham, which are potential candidates for further investigation. The present patient cohort with its uneven distribution of co-morbidities and co-medications, the individual sampling, the sample processing for this approach, the number of uncharacterized or unverifiable porcine proteins, the method of proteome and phosphoproteome analysis and its bioinformatical evaluation per se may all have contributed to this unsatisfactory result.
In the future, specific phosphoproteome rather than proteome analysis of different, isolated cellular and subcellular compartments of myocardial biopsies taken at baseline and early reperfusion may reveal more insights into the signal transduction of cardioprotection by RIPC. Furthermore, independent analysis methods must be used for the characterization and validation of potentially identified pathways.
Methods
Materials
Chemicals were of the highest quality available, and all solutions were freshly prepared using MilliQ® water or high quality analytical grade organic solvents. Materials were obtained from Sigma-Aldrich (Deisenhofen, Germany) or purchased as indicated.
Patient study
The inclusion and exclusion criteria for as well as the results of the clinical trial (ClinicalTrials.gov NCT01406678, date of registration: December 1, 2009) have been reported7. The study conforms to the principles of the Declaration of Helsinki. With approval of the local ethics committee (Germany: Institutional Review Board, University of Duisburg-Essen, no. 08–3683) and patients’ written informed consent, LV biopsies were harvested in a subgroup of patients undergoing elective isolated first-time CABG, who were enrolled in this randomized, prospective, double-blind, placebo-controlled study without (sham) or with RIPC.
Anesthesia was induced with sufentanil (1 µg/kg), etomidate (0.3 mg/kg) and rocuronium (0.6 mg/kg) and maintained with isoflurane (0.6–1.0% end-tidal). The RIPC protocol consisted of 3 cycles of 5 min left upper arm ischemia/5 min reperfusion and was compared to sham (cuff left deflated for 30 min). Surgical revascularization was performed in all patients using median sternotomy, mild systemic hypothermia (>32 °C) and antegrade cold crystalloid Bretschneider (Köhler Chemie GmbH, Bensheim, Germany) cardioplegia with additional topical cooling and single aortic cross-clamping for all distal anastomoses7.
Human LV biopsies
Transmural LV biopsies of 2–5 mg were available from 22 patients (n = 11/11 RIPC/sham). LV biopsies were taken at 5–10 min reperfusion following aortic unclamping from the perfusion territory undergoing revascularization using a Tru-Cut R biopsy needle (Cardinal Health, Dublin, OH, USA). Biopsies were quickly frozen in liquid nitrogen and stored at −80 °C until subsequent analysis.
Serum troponin I
Venous blood samples were drawn from each patient on the day before surgery and postoperatively at 1, 6, 12, 24, 48, and 72 h and analyzed for serum cTnI. The AUC for serum cTnI was calculated according to the trapezoidal rule. Missing values were replaced by linear inter- and extrapolation7.
Pig studies
In a translational pig model, we analyzed the proteome and phosphoproteome of residual lysates of LV biopsies from pigs which had undergone coronary occlusion/reperfusion without (sham) or with RIPC in prior studies28. The experimental protocol was approved by the Landesamt für Natur, Umwelt und Verbraucherschutz Nordrhein-Westfalen, Germany (B1322/12) and the investigation conforms to the Guide for the Care and Use of Laboratory Animals published by the US National Institutes of Health (NIH Publication No. 85-23, revised 1996).
Male Göttinger minipigs were anesthetized with etomidate (0.3 mg/kg, Hypnomidat; Janssen-Cilag, Neuss) and sufentanil (1 μg/kg IV, Sufenta; Janssen-Cilag, Neuss, Germany), and anesthesia was maintained with isoflurane (2%) in oxygen-enriched air. The RIPC protocol consisted of 4 cycles of 5 min left hindlimb ischemia/5 min reperfusion (n = 4) and was compared to sham (n = 4; tourniquet not fixed for 40 min). After a left lateral thoracotomy, a silk suture was placed around the left anterior descending coronary artery (LAD) distal to its second diagonal branch for coronary occlusion. The suture around the LAD was carefully tightened against a soft silicone plate for 60 min. Reperfusion was induced by release and quick removal of the suture. For details see28.
Porcine LV biopsies
LV biopsies were sampled at baseline (after RIPC/sham and before 60 min LAD occlusion) and at 10 min reperfusion with a modified dental drill. Biopsies were quickly frozen in liquid nitrogen and stored at −80 °C until subsequent analysis.
Infarct size in pig hearts
At the end of each experiment, the LAD was re-occluded, and 5 ml blue dye (Patentblau V, Guerbet GmbH, Sulzbach, Germany) was quickly injected into the left atrium to delineate the area at risk as remaining unstained. The heart was then arrested by electrical induction of fibrillation, removed from the chest and sectioned from base to apex into 5 transverse slices. Slices were photographed from each side, and their shape and the unstained area at risk were traced manually on transparent film. Slices were then immersed in 0.09 mol/l sodium phosphate buffer containing 1% triphenyl tetrazolium chloride and 8% dextran for 20 min at 37 °C to demarcate viable from infarcted tissue. The infarcted areas were traced on the same transparent film as the area at risk. The total slice area, the area at risk, and the infarcted area were measured by computer-assisted planimetry. The area at risk was calculated as a fraction of the LV, and the infarct size was calculated as a fraction of the area at risk.
Sample processing of LV biopsies
Human LV biopsies (n = 11/11 RIPC/sham) were randomly split into two subsets and lysed either in the Tris/SDS (n = 6/6 RIPC/sham) or the RIPA (n = 5/5 RIPC/sham) buffer to obtain a broad range of solubilized proteins of all cellular components. Tris/SDS buffer, with SDS as ionic detergent, was used to gain a high protein yield of all cellular components, whereas RIPA buffer was used to extract predominantly nuclear, mitochondrial, cytoplasmic and intracellular proteins and to a lesser extent membrane, cytoskeletal and extracellular proteins46. The frozen LV biopsies were homogenized using a tissue homogenizer (Ultra-Turrax, IKA, Staufen, Germany) either in 0.1 mol/l Tris and 2% (w/v) SDS buffer and incubation for 5 min at 95 °C or in 1 × RIPA buffer (Cell Signaling, Danvers, MA, USA) supplemented with 1 × complete protease inhibitor cocktail (Roche, Basel, Switzerland). All samples were centrifuged at 16,000 g for 5 min. The protein concentration of the supernatant was determined using a protein assay (Bradford method, Biorad, Hercules, CA, USA) with bovine serum albumin (BSA) as standard (Thermo Scientific, Waltham, MA, USA).
The protein yield of the Tris/SDS buffer-lysed LV biopsies was sufficient to perform subsequent in-solution digestion and phosphopeptide enrichment (n = 6/6 RIPC/sham), respectively. For in-gel digestion, the protein yield of only n = 3/3 RIPC/sham lysates was sufficient. The protein yield of RIPA buffer-lysed LV biopsies (n = 5/5 RIPC/sham) was too low and precluded phosphopeptide enrichment and in-gel digestion. Thus, these lysates were exclusively used for in-solution digestion. Separate biopsies from the same pigs (n = 4/4) were taken at baseline and at early reperfusion, respectively, lysed in Tris/SDS buffer, and used for in-solution digestion and phosphopeptide enrichment.
In-solution digestion
Lysates (15 µg protein) were precipitated overnight with ice-cold acetone at −20 °C and then centrifuged (15,000 g, 10 min at 4 °C). Protein pellets were washed with 90% ice-cold acetone, centrifuged again (15,000 g, 10 min at 4 °C) and dissolved with 6 mol/l urea, 2 mol/l thiourea, 10 mmol/l 4-(2-hydroxyethyl)-1-piperazineethanesulfonic acid (HEPES), pH 8. Disulfide bonds on cysteine were reduced by adding 10 mmol/l dithiothreitol and alkylated by adding 55 mmol/l iodoacetamide. The endoproteinase Lys-C (Wako Chemicals, Osaka, Japan) was added at an enzyme:substrate ratio of 1:100 and incubated at room temperature for 120-180 min. The lysates were diluted with 50 mmol/l ammonium bicarbonate, and trypsin (Promega, Fitchburg, WI, USA) was added at an enzyme:substrate ratio of 1:100 and incubated at room temperature overnight. The digests were quenched by trifluoroacetic acid, and samples containing tryptic peptides were desalted and concentrated with “Stop and Go extraction” tips filled with C-18 (C-18 Empore Disks, 3 M, Minneapolis, MN, USA)47, 48.
Phosphopeptide enrichment
Phosphopeptide enrichment was performed using titanium dioxide, which enables robust and reproducible isolation of phosphopeptides from small amounts of tissue/cell material49. Samples were acidified by 6% trifluoroacetic acid after in-solution trypsin digestion. Titanium dioxide beads (0.1 mg/µl in 60% acetonitrile/6% trifluoroacetic acid) were added to the samples with a peptide:beats ratio of 1:3, incubated for 20 min on a rotor wheel and centrifuged (500 g, 1 min, room temperature). With the supernatant, the latter steps were repeated three times. Beads were transferred to C-8 columns, washed three times with 60% acetonitrile/1% trifluoroacetic acid and then with 80% acetonitrile/0.5% formic acid. Phosphopeptides were eluted with 40% acetonitrile/3.75% ammonium hydroxide, pH 10.5 and 80% acetonitrile. Samples were vacuum-centrifuged for 90 min at 30 °C until the volume of the samples was ~2 µl and filled up to 10 µl with 60% acetonitrile/6% trifluoroacetic acid.
Gel electrophoresis and in-gel digestion
LV biopsies were lysed in Tris/SDS buffer and loaded on a 4%–12% Bis-Tris gel (NuPAGE, Invitrogen, Carlsbad, CA, USA). After colloidal blue staining, evenly sized gel pieces were excised from the gel and digested with trypsin. Briefly, gel pieces were reduced with 10 mmol/l dithiothreitol, alkylated with 55 mmol/l iodoacetamide and digested with trypsin overnight. Peptides were extracted from the gel using an increasing acetonitrile concentration. Collected peptide mixtures were concentrated and desalted using the “Stop and Go extraction” tips47.
Liquid chromatography and mass spectrometry
A binary buffer system consisting of buffer A (0.1% formic acid) and buffer B (80% acetonitrile, 0.1% formic acid) was used for peptide separation on an Easy nano-flow high performance liquid chromatography 1000 system (Thermo Scientific, Waltham, MA, USA), which was coupled via a nano electrospray ionization source to a QExactive or a linear trap Quadropole Velos mass spectrometer (Thermo Scientific, Waltham, MA, USA). Peptide elution from the in-house packed 20 cm (3 mm beads, ID: 75 mm, Dr Maisch, Ammerbuch, Germany) or 50 cm (1.8 mm beads, ID: 75 mm, Dr Maisch, Ammerbuch, Germany) column was achieved by increasing the relative amount of B from 7% to 38% in a linear gradient within 150 min or 240 min50, 51.
QExactive and linear trap quadropole Velos
Mass spectrometry spectra were recorded at 70,000 resolution (200 m/z, 3E6 ions as the automatic gain control target) within a maximum injection time of 20 ms. Acquisition of tandem mass spectrometry (MS/MS) spectra in a data-dependent mode after higher-energy collisional dissociation fragmentation (Top10) was carried out at 17,500 (200 m/z) using 1E6 ions as the automatic gain control target and 60 ms for maximal injection time. The separation width was set to 1.7 m/z51.
For the identification of phosphopeptides, a linear trap quadropole-Orbitrap Velos mass spectrometer was used, and MS/MS spectra were generated by higher C-trap dissociation. Briefly, 30,000 ions were accumulated in the c-trap, and MS/MS spectra were detected in the Orbitrap at a resolution of 7,50052, 53.
Data processing and analysis
Acquired raw files were processed using the MaxQuant software tool (version 1.3.7.4; Max Planck Institute of Biochemistry, Martinsried, Germany). A maximum of two missed cleavages and a mass tolerance of 4.5 ppm and 7 ppm for MS/MS first and main search were set, respectively. A minimal peptide length of seven amino acids after Lys-C specificity for protein assignment and a minimal ratio count of two for quantification were required. For further data analysis, proteins/phosphopeptides were defined as detected proteins/phosphopeptides when measured at least in 50% of the samples in one group, respectively. For a number of proteins, which were identified as uncharacterized proteins in porcine LV biopsies by FDR-based statistical analysis, the corresponding IDs for humans were identified by the gene name, when available in the universal protein database UniProt (www.uniprot.org).
Pathway analysis
Independently of lysis and digestion methods, all proteins detected at early reperfusion in humans (Fig. 3, line (f)) and in pigs (Fig. 5, line (f)) with a ≥2-fold higher expression/phosphorylation with RIPC or sham, respectively, and those exclusively detected with RIPC or sham were considered for a pathway analysis; the pathway analysis does not distinguish between activation (phosphorylation) and expression.
In pigs, we restricted this pathway analysis to all proteins with higher expression/phosphorylation detected at early reperfusion with RIPC or sham, respectively. Cardioprotective signals must be present at early reperfusion to be causally involved in final infarct size reduction.
The in-silico pathway analysis was performed with Ingenuity pathway analysis software (Ingenuity Systems, Redwood City, CA, USA)54.
Western blot analysis
Residual LV biopsy lysates were used to compare the cellular composition of LV biopsies. Protein aliquots of 30 µg were electrophoretically separated on precasted SDS-polyacrylamide gels (BioRad, Munich, Germany) and transferred to polyvinylidene fluoride membranes. After Ponceau-S staining membranes were blocked and then incubated with antibodies directed against proteins encoding different cell types: CD1 (#3528) as endothelial cell marker55, enolase 2 (#8171) as neuronal marker56, hemoglobin γ (#39386; Cell Signaling Technology, Cambridge, UK) as erythrocyte marker57, collagen 3α (NBP2-15946, Novus Biological, Littleton, CO, USA) as fibroblast marker58 and tropomyosin (#T9283, Sigma-Aldrich, Deisenhofen, Germany) as cardiomyocyte marker59. The phosphorylation/expression of STAT5 in residual lysates from human LV biopsies and the phosphorylation/expression of STAT3 in residual lysates from porcine LV biopsies were analyzed with specific antibodies against phosphorylated STAT5 at tyr694 (#4322) and STAT3 at tyr705 (#9138) and the respective total forms of STAT5 (#9363) and STAT3 (#12640; Cell Signaling Technology, Cambridge, UK) to confirm our prior results26,27,28. The expression of prostaglandin reductase 2 (#ab84711, Abcam, Cambridge, UK), i.e. the only protein with a differential expression in human LV biopsies (see results), as well as the phosphorylation/expression of α-crystallin B (#LS-B3696; #LS-C22453, LifeSpan Biosciences, Seattle, WA, USA), α-endosulfine (#5240; #8770), and p62 (#13121; #5114, Cell Signaling Technology, Cambridge, UK), i.e. proteins where antibodies were commercially available against the identified phosphorylation site with a difference in protein phosphorylation between baseline and early reperfusion with RIPC or sham, were also analyzed.
After incubation with the respective secondary antibody, immunoreactive signals were detected by chemiluminescence and quantified with ChemoCam/LabImage1D software (INTAS, Göttingen, Germany). The immunoreactivity of PGR2 was normalized to Ponceau-S staining. The immunoreactivities of the phosphorylated proteins were normalized to the respective total forms. Total α-endosulfine was not detectable, therefore phosphorylated α-endosulfine was normalized to Ponceau-S staining. Full-length blot and Ponceau-S staining are presented in Supplemental Figs S2, S3, S4, S6 and S7, respectively.
Literature data search
The relation to heart, ischemia and reperfusion and cardioprotection of all identified phosphopeptides/proteins with a FDR-based statistical difference was analyzed from the literature using the electronic database pubmed up to May 2017. Search keywords were “heart” or “cardiac” combined with the protein name as indicated in UniProt, if applicable also with the alternative name(s) of the respective protein. These keywords were further combined with “ischemia” and “reperfusion” or “cardioprotection” or “conditioning”.
Statistics
Data are expressed as mean ± standard error of the mean (SEM). Statistics were performed using SigmaStat software (SigmaStat 2.03, SPSS Inc., Chicago, IL, USA). Patient baseline and intraoperative characteristics were compared using unpaired Student’s t-test (continuous data) and 2-tailed Fisher’s exact test (categorical data). Serum cTnI of patients was analyzed by 2-way (group, time) ANOVA for repeated measures. The AUC for the serum cTnI over 72 h was compared by unpaired Student’s t-test. Immunoreactivities on the blot were compared by unpaired (between RIPC and sham) or by paired (between baseline and early reperfusion in pigs) Student’s t-tests. Proteome data visualization was performed using the statistical environment R and Perseus (Max Planck Institute of Biochemistry, Martinsried, Germany)60. Proteome and phosphoproteome data were compared by unpaired (between RIPC and sham) or by paired (between baseline and early reperfusion in pigs) Student’s t-tests. The FDR-based statistical analysis was performed with number of randomization = 500, exchangeability factor s0 = 0.1 and q-value = 0.05. Differences were considered significant at the level of p < 0.05.
References
Heusch, G., Botker, H. E., Przyklenk, K., Redington, A. & Yellon, D. M. Remote ischemic conditioning. J Am Coll Cardiol 65, 177–195 (2015).
Heusch, G. & Rassaf, T. Time to give op on cardioprotection? A critical appraisal of clinical studies on ischemic pre-, post-, and remote conditioning. Circ Res. 119, 676–695 (2016).
Sardar, P. et al. Remote ischemic preconditioning in patients undergoing cardiovascular surgery: Evidence from a meta-analysis of randomized controlled trials. Int J Cardiol 221, 34–41 (2016).
Man, C., Gong, D., Zhou, Y. & Fan, Y. Meta-analysis of remote ischemic conditioning in patients with acute myocardial infarction. Sci Rep 7, 43529 (2017).
Davies, W. R. et al. Remote ischemic preconditioning improves outcome at 6 years after elective percutaneous coronary intervention: The CRISP stent trial long-term follow-up. Circ Cardiovasc Interv 6, 246–251 (2013).
Hausenloy, D. J. et al. Effect of remote ischaemic preconditioning on myocardial injury in patients undergoing coronary artery bypass graft surgery: a randomized controlled trial. Lancet. 370, 575–579 (2007).
Thielmann, M. et al. Cardioprotective and prognostic effects of remote ischaemic preconditioning in patients undergoing coronary artery bypass surgery: a single-centre randomised, double-blind, controlled trial. Lancet. 382, 597–604 (2013).
Candilio, L. et al. Effect of remote ischaemic preconditioning on clinical outcomes in patients undergoing cardiac bypass surgery: a randomised controlled clinical trial. Heart. 10, 185–192 (2015).
Nouraei, S. M., Baradari, A. G. & Jazayeri, A. Does remote ischaemic preconditioning protect kidney and cardiomyocytes after coronary revascularization? A double blind controlled clinical trial. Med Arch 70, 373–378 (2016).
Bøtker, H. E. et al. Remote ischaemic conditioning before hospital admission, as a complement to angioplasty, and effect on myocardial salvage in patients with acute myocardial infarction: a randomised trial. Lancet. 375, 727–734 (2010).
Sloth, A. D. et al. Improved long-term clinical outcomes in patients with ST-elevation myocardial infarction undergoing remote ischaemic conditioning as an adjunct to primary percutaneous coronary intervention. Eur Heart J 35, 168–175 (2014).
Eitel, I. et al. Cardioprotection by combined intrahospital remote ischaemic perconditioning and postconditioning in ST-elevation myocardial infarction: the randomized LIPSIA CONDITIONING trial. Eur Heart J 36, 3049–3057 (2015).
White, S. K. et al. Remote ischemic conditioning reduces myocardial infarct size and edema in patients with ST-segment elevation myocardial infarction. J Am Coll Cardiol Cardiovasc Interv 8, 178–188 (2015).
Yellon, D. M. et al. Remote ischemic conditioning reduces myocardial infarct size in STEMI patients treated by thrombolysis. J Am Coll Cardiol 65, 2764–2765 (2015).
Liu, Z., Zhao, L., Hong, D. & Gao, J. Remote ischaemic preconditioning reduces myocardial ischaemic reperfusion injury in patients with ST-elevation myocardial infarction undergoing primary percutaneous coronary intervention. Acta Cardiol. 71, 596–603 (2016).
Hausenloy, D. J. et al. Remote ischemic preconditioning and outcomes of cardiac surgery. N Engl J Med 373, 1408–1417 (2015).
Meybohm, P. et al. A multicenter trial of remote ischemic preconditioning for heart surgery. N Engl J Med 373, 1397–1407 (2015).
Kottenberg, E. et al. Protection by remote ischaemic preconditioning during coronary artery bypass grafting with isoflurane but not with propofol anesthesia - a clinical trial. Acta Anaesthesiol Scand 56, 30–38 (2012).
Heusch, G. & Gersh, B. J. ERICCA and RIPHeart: two nails in the coffin for cardioprotection by remote ischemic conditioning? Probably not! Eur Heart J 37, 200–202 (2016).
Kleinbongard, P. et al. Confounders of cardioprotection by remote ischemic preconditioning in patients undergoing coronary artery bypass grafting. Cardiology. 133, 128–133 (2016).
Kahlert, P. et al. No protection of heart, kidneys and brain by remote ischemic preconditioning before transfemoral transcatheter aortic valve implantation: interim-analysis of a randomized single-blinded, placebo-controlled, single-center trial. Int J Cardiol 231, 248–254 (2017).
Heusch, G. Molecular basis of cardioprotection: signal transduction in ischemic pre-, post- and remote conditioning. Circ Res. 116, 674–699 (2015).
Downey, J. M., Krieg, T. & Cohen, M. V. Mapping preconditioning’s signaling pathways: an engineering approach. Ann NY Acad Sci 1123, 187–196 (2008).
Kleinbongard, P. & Heusch, G. Extracellular signalling molecules in the ischaemic/reperfused heart - druggable and translatable for cardioprotection? Br J Pharmacol 172, 2010–2025 (2015).
Kleinbongard, P., Skyschally, A. & Heusch, G. Cardioprotection by remote ischemic conditioning and its signal transduction. Pflugers Arch - Eur J Physiol 469, 159–181 (2017).
Heusch, G. et al. STAT5 activation and cardioprotection by remote ischemic preconditioning in humans. Circ Res. 110, 111–115 (2012).
Gedik, N. et al. No evidence for activated autophagy in left ventricular myocardium at early reperfusion with protection by remote ischemic preconditioning in patients undergoing coronary artery bypass grafting. PLoS One. 9, e96567 (2014).
Skyschally, A. et al. Across-species transfer of protection by remote ischemic preconditioning with species-specific myocardial signal transduction by reperfusion injury salvage kinase and survival activating factor enhancement pathways. Circ Res. 117, 279–288 (2015).
Varga, Z. V. et al. Functional genomics of cardioprotection by ischemic conditioning and the influence of comorbid conditions: implications in target identification. Curr Drug Targets 16, 904–911 (2015).
Hausenloy, D. J. et al. Novel targets and future strategies for acute cardioprotection: Position Paper of the European Society of Cardiology Working Group on Cellular Biology of the Heart. Cardiovasc Res 113, 564–585 (2017).
Pavo, N. et al. Sequential activation of different pathway networks in ischemia-affected and non-affected myocardium, inducing intrinsic remote conditioning to prevent left ventricular remodeling. Sci Rep 7, 43958 (2017).
Perrino, C. et al. Epigenomic and transcriptomic approaches in the post-genomic era: path to novel targets for diagnosis and therapy of the ischaemic heart? Position Paper of the European Society of Cardiology Working Group on Cellular Biology of the Heart. Cardiovasc Res 113, 725–736 (2017).
Porter, K., Medford, H. M., McIntosh, C. M. & Marsh, S. A. Cardioprotection requires flipping the ‘posttranslational modification’ switch. Life Sci. 90, 89–98 (2012).
Ferdinandy, P., Hausenloy, D. J., Heusch, G., Baxter, G. F. & Schulz, R. Interaction of risk factors, comorbidities and comedications with ischemia/reperfusion injury and cardioprotection by preconditioning, postconditioning, and remote conditioning. Pharmacol Rev. 66, 1142–1174 (2014).
Gres, P., Schulz, R., Jansen, J., Umschlag, C. & Heusch, G. Involvement of endogenous prostaglandins in ischemic preconditioning in pigs. Cardiovasc Res 55, 626–632 (2002).
Wu, Q. et al. Cardiac protective effects of remote ischaemic preconditioning in children undergoing tetralogy of fallot repair surgery: a randomized controlled trial. Eur Heart J. doi:10.1093/eurheartj/ehx030 (2017).
Abdulkareem, N., Skroblin, P., Jahangiri, M. & Mayr, M. Proteomics in aortic aneurysm-what have we learnt so far? Proteomics Clin Appl 7, 504–515 (2013).
Heron, L., Virsolvy, A., Apiou, F., Le Cam, A. & Bataille, D. Isolation, characterization, and chromosomal localization of the human ENSA gene that encodes alpha-endosulfine, a regulator of beta-cell K(ATP) channels. Diabetes. 48, 1873–1876 (1999).
Heusch, G., Boengler, K. & Schulz, R. Cardioprotection: nitric oxide, protein kinases, and mitochondria. Circulation. 118, 1915–1919 (2008).
Slagsvold, K. H. et al. Remote ischemic preconditioning preserves mitochondrial function and activates pro-survival protein kinase Akt in the left ventricle during cardiac surgery: A randomized trial. Int J Cardiol 177, 409–417 (2014).
Slagsvold, K. H., Rognmo, O., Hoydal, M., Wisloff, U. & Wahba, A. Remote ischemic preconditioning preserves mitochondrial function and influences myocardial microRNA expression in atrial myocardium during coronary bypass surgery. Circ Res. 114, 851–859 (2014).
Gedik, N. et al. Cardiomyocyte mitochondria as targets of humoral factors released by remote ischemic preconditioning. Arch Med Sci 13, 448–458 (2016).
Baines, C. P. et al. Ischemic preconditioning depends on interaction between mitochondrial KATP channels and actin cytoskeleton. Am J Physiol Heart Circ Physiol 276, H1361–H1368 (1999).
Abdul-Ghani, S., Heesom, K. J., Angelini, G. D. & Suleiman, M. S. Cardiac phosphoproteomics during remote ischemic preconditioning: A role for the sarcomeric Z-disk proteins. Biomed Res Int 2014, 767812 (2014).
Potz, B. A. et al. Calpain inhibition modulates glycogen synthase kinase 3beta pathways in ischemic myocardium: A proteomic and mechanistic analysis. J Thorac Cardiovasc Surg 152, 342–357 (2017).
Ngoka, L. C. Sample prep for proteomics of breast cancer: proteomics and gene ontology reveal dramatic differences in protein solubilization preferences of radioimmunoprecipitation assay and urea lysis buffers. Proteome Sci. 6, 30 (2008).
Rappsilber, J., Mann, M. & Ishihama, Y. Protocol for micro-purification, enrichment, pre-fractionation and storage of peptides for proteomics using stage tips. Nat Protoc. 2, 1896–1906 (2007).
Kruger, M. et al. Dissection of the insulin signaling pathway via quantitative phosphoproteomics. Proc Natl Acad Sci USA 105, 2451–2456 (2008).
Montoya, A., Beltran, L., Casado, P., Rodriguez-Prados, J. C. & Cutillas, P. R. Characterization of a TiO(2) enrichment method for label-free quantitative phosphoproteomics. Methods. 54, 370–378 (2011).
Holper, S., Nolte, H., Bober, E., Braun, T. & Kruger, M. Dissection of metabolic pathways in the Db/Db mouse model by integrative proteome and acetylome analysis. Mol Biosyst. 11, 908–922 (2015).
Nolte, H. et al. Dynamics of zebrafish fin regeneration using a pulsed SILAC approach. Proteomics. 15, 739–751 (2015).
Drexler, H. C. et al. On marathons and Sprints: an integrated quantitative proteomics and transcriptomics analysis of differences between slow and fast muscle fibers. Mol Cell Proteomics 11, M111.010801 (2012).
Konzer, A. et al. Stable isotope labeling in zebrafish allows in vivo monitoring of cardiac morphogenesis. Mol Cell Proteomics 12, 1502–1512 (2013).
Schmidt, A., Forne, I. & Imhof, A. Bioinformatic analysis of proteomics data. BMC Syst Biol 8, S3 (2014).
Zhang, Y. et al. Endothelial to mesenchymal transition contributes to arsenic-trioxide-induced cardiac fibrosis. Sci Rep 6, 33787 (2016).
Semba, R., Asano, T. & Kato, K. Physiological expression of neural marker proteins in the heart of young rats. Brain Res Dev Brain Res 54, 217–220 (1990).
Tezel, T. H. et al. Synthesis and secretion of hemoglobin by retinal pigment epithelium. Invest Ophthalmol Vis Sci 50, 1911–1919 (2009).
Pan, L. L., Wang, X. L., Wang, X. L. & Zhu, Y. Z. Sodium hydrosulfide prevents myocardial dysfunction through modulation of extracellular matrix accumulation and vascular density. Int J Mol Sci 15, 23212–23226 (2014).
Canton, M. et al. Oxidative modification of tropomyosin and myocardial dysfunction following coronary microembolization. Eur Heart J 27, 875–881 (2006).
Tyanova, S. et al. The Perseus computational platform for comprehensive analysis of (prote)omics data. Nat Methods. 13, 731–740 (2016).
Penna, C., Mancardi, D., Tullio, F. & Pagliaro, P. Postconditioning and intermittent bradykinin induced cardioprotection require cyclooxygenase activation and prostacyclin release during reperfusion. Basic Res Cardiol 103, 368–377 (2008).
Cubedo, J. et al. Targeting the molecular mechanisms of ischemic damage: Protective effects of alpha-crystallin-B. Int J Cardiol 215, 406–416 (2016).
Hoover, H. E., Thuerauf, D. J., Martindale, J. J. & Glembotski, C. C. alpha B-crystallin gene induction and phosphorylation by MKK6-activated p38. A potential role for alpha B-crystallin as a target of the p38 branch of the cardiac stress response. J Biol Chem 275, 23825–23833 (2000).
Su, F. et al. Bcl-2-associated athanogene 3 protects the heart from ischemia/reperfusion injury. JCI Insight 1, e90931 (2016).
Neuhof, C. & Neuhof, H. Calpain system and its involvement in myocardial ischemia and reperfusion injury. World J Cardiol 6, 638–652 (2014).
French, J. P. et al. Ischemia-reperfusion-induced calpain activation and SERCA2a degradation are attenuated by exercise training and calpain inhibition. Am J Physiol Heart Circ Physiol 290, H128–136 (2006).
Zhang, C. M., Gao, L., Zheng, Y. J. & Yang, H. T. Berbamine protects the heart from ischemia/reperfusion injury by maintaining cytosolic Ca(2+) homeostasis and preventing calpain activation. Circ J. 76, 1993–2002 (2012).
Li, X. et al. Myocardial injury after ischemia-reperfusion in mice deficient in Akt2 is associated with increased cardiac macrophage density. Am J Physiol Heart Circ Physiol 301, H1932–1940 (2011).
Cao, S. et al. Ischemic postconditioning influences electron transport chain protein turnover in Langendorff-perfused rat hearts. PeerJ. 4, e1706 (2016).
Hausenloy, D. J. & Yellon, D. M. New directions for protecting the heart against ischaemia-reperfusion injury: targeting the reperfusion injury salvage kinase (RISK)-pathway. Cardiovasc Res. 61, 448–460 (2004).
Wang, C. et al. Hepatocyte growth factor upregulates nexilin gene expression in cardiomyocytes via JNK pathway. Genet Mol Res 13, 4976–4982 (2014).
Klionsky, D. J. for the Working Group Guidelines for Monitoring Autophagy. Guidelines for the use and interpretation of assays for monitoring autophagy. Autophagy. 8, 445–544 (2012).
Huang, C. et al. Preconditioning involves selective mitophagy mediated by Parkin and p62/SQSTM1. PLoS One. 6, e20975 (2011).
Muller, A. L., Freed, D. & Dhalla, N. S. Activation of proteases and changes in Na+ -K+ -ATPase subunits in hearts subjected to ischemia-reperfusion. J Appl Physiol (1985) 114, 351–360 (2013).
Ashton, K. J. et al. Unique transcriptional profile of sustained ligand-activated preconditioning in pre- and post-ischemic myocardium. PLoS One. 8, e72278 (2013).
Acknowledgements
PK and MK were supported by the Deutsche Herzstiftung (F/17/13). GH was supported by the German Research Foundation (He 1320/18-3).
Author information
Authors and Affiliations
Contributions
N.G., M.K. and P.K. conceived and designed the experiments. N.G., M.K. and A.S. performed the experiments. M.T., E.K., U.F., J.P. and H.J. performed the clinical study. N.G., M.K., E.C. and P.K. analyzed the data. M.K. and P.K. contributed reagents/materials/analysis tools. N.G., G.H. and P.K. wrote the paper. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing Interests
The authors declare that they have no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Gedik, N., Krüger, M., Thielmann, M. et al. Proteomics/phosphoproteomics of left ventricular biopsies from patients with surgical coronary revascularization and pigs with coronary occlusion/reperfusion: remote ischemic preconditioning. Sci Rep 7, 7629 (2017). https://doi.org/10.1038/s41598-017-07883-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-017-07883-5
This article is cited by
-
Cardioprotection by post-conditioning with exogenous triiodothyronine in isolated perfused rat hearts and isolated adult rat cardiomyocytes
Basic Research in Cardiology (2021)
-
Translational large animal model of hibernating myocardium: characterization by serial multimodal imaging
Basic Research in Cardiology (2020)
-
Survival pathways in cardiac conditioning: individual data vs. meta-analyses. What do we learn?
Basic Research in Cardiology (2018)
-
STAT3 as a common signal of ischemic conditioning: a lesson on “rigor and reproducibility” in preclinical studies on cardioprotection
Basic Research in Cardiology (2018)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
