
Abstract
The radiation-attenuated Plasmodium falciparum sporozoite (PfSPZ) vaccine provides protection against P. falciparum infection in malaria-naïve adults. Preclinical studies show that T cell-mediated immunity is required for protection and is readily induced in humans after vaccination. However, previous malaria exposure can limit immune responses and vaccine efficacy (VE) in adults. We hypothesized that infants with less previous exposure to malaria would have improved immunity and protection. We conducted a multi-arm, randomized, double-blind, placebo-controlled trial in 336 infants aged 5–12 months to determine the safety, tolerability, immunogenicity and efficacy of the PfSPZ Vaccine in infants in a high-transmission malaria setting in western Kenya (NCT02687373). Groups of 84 infants each received 4.5 × 105, 9.0 × 105 or 1.8 × 106 PfSPZ Vaccine or saline three times at 8-week intervals. The vaccine was well tolerated; 52 (20.6%) children in the vaccine groups and 20 (23.8%) in the placebo group experienced related solicited adverse events (AEs) within 28 d postvaccination and most were mild. There was 1 grade 3-related solicited AE in the vaccine group (0.4%) and 2 in the placebo group (2.4%). Seizures were more common in the highest-dose group (14.3%) compared to 6.0% of controls, with most being attributed to malaria. There was no significant protection against P. falciparum infection in any dose group at 6 months (VE in the 9.0 × 105 dose group = −6.5%, P = 0.598, the primary statistical end point of the study). VE against clinical malaria 3 months after the last dose in the highest-dose group was 45.8% (P = 0.027), an exploratory end point. There was a dose-dependent increase in antibody responses that correlated with VE at 6 months in the lowest- and highest-dose groups. T cell responses were undetectable across all dose groups. Detection of Vδ2+Vγ9+ T cells, which have been correlated with induction of PfSPZ Vaccine T cell immunity and protection in adults, were infrequent. These data suggest that PfSPZ Vaccine-induced T cell immunity is age-dependent and may be influenced by Vδ2+Vγ9+ T cell frequency. Since there was no significant VE at 6 months in these infants, these vaccine regimens will likely not be pursued further in this age group.
This is a preview of subscription content, access via your institution
Access options
Access Nature and 54 other Nature Portfolio journals
Get Nature+, our best-value online-access subscription
$29.99 / 30 days
cancel any time
Subscribe to this journal
Receive 12 print issues and online access
$209.00 per year
only $17.42 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout




Similar content being viewed by others


Data availability
The data that support the findings of this study are available upon request to the corresponding authors and approval from Sanaria. Restrictions apply to the availability of these data, which were used under an investigational new drug application, so they are not publicly available. All requests for raw and analyzed data will be promptly reviewed by the trial sponsor, Sanaria, to verify if the request is subject to any confidentiality obligations. Patient-related data not included in the paper were generated as part of clinical trials and may be subject to patient confidentiality. Any data that can be shared will be released via a data use agreement.
Code availability
No custom code was generated for the analyses presented in this paper. Standard analysis packages and commands in the specified software were used.
References
World Malaria Report 2020: 20 Years of Global Progress and Challenges (WHO, 2020).
Bhatt, S. et al. The effect of malaria control on Plasmodium falciparum in Africa between 2000 and 2015. Nature 526, 207–211 (2015).
Agnandji, S. T. et al. Efficacy and safety of the RTS,S/AS01 malaria vaccine during 18 months after vaccination: a phase 3 randomized, controlled trial in children and young infants at 11 African sites. PLoS Med. 11, e1001685 (2014).
RTS,S Clinical Trials Partnership Efficacy and safety of RTS,S/AS01 malaria vaccine with or without a booster dose in infants and children in Africa: final results of a phase 3, individually randomised, controlled trial. Lancet 386, 31–45 (2015).
White, M. T. et al. Immunogenicity of the RTS,S/AS01 malaria vaccine and implications for duration of vaccine efficacy: secondary analysis of data from a phase 3 randomised controlled trial. Lancet Infect. Dis. 15, 1450–1458 (2015).
Seder, R. A. et al. Protection against malaria by intravenous immunization with a nonreplicating sporozoite vaccine. Science 341, 1359–1365 (2013).
Ishizuka, A. S. et al. Protection against malaria at 1 year and immune correlates following PfSPZ vaccination. Nat. Med. 22, 614–623 (2016).
Epstein, J. E. et al. Live attenuated malaria vaccine designed to protect through hepatic CD8+ T cell immunity. Science 334, 475–480 (2011).
Lyke, K. E. et al. Attenuated PfSPZ vaccine induces strain-transcending T cells and durable protection against heterologous controlled human malaria infection. Proc. Natl Acad. Sci. USA 114, 2711–2716 (2017).
Mordmüller, B. et al. Sterile protection against human malaria by chemoattenuated PfSPZ vaccine. Nature 542, 445–449 (2017).
Charoenvit, Y. et al. Inability of malaria vaccine to induce antibodies to a protective epitope within its sequence. Science 251, 668–671 (1991).
Charoenvit, Y. et al. Monoclonal, but not polyclonal, antibodies protect against Plasmodium yoelii sporozoites. J. Immunol. 146, 1020–1025 (1991).
Potocnjak, P., Yoshida, N., Nussenzweig, R. S. & Nussenzweig, V. Monovalent fragments (Fab) of monoclonal antibodies to a sporozoite surface antigen (Pb44) protect mice against malarial infection. J. Exp. Med. 151, 1504–1513 (1980).
Schofield, L., Ferreira, A., Altszuler, R., Nussenzweig, V. & Nussenzweig, R. S. Interferon-gamma inhibits the intrahepatocytic development of malaria parasites in vitro. J. Immunol. 139, 2020–2025 (1987).
Weiss, W. R., Sedegah, M., Beaudoin, R. L., Miller, L. H. & Good, M. F. CD8+ T cells (cytotoxic/suppressors) are required for protection in mice immunized with malaria sporozoites. Proc. Natl Acad. Sci. USA 85, 573–576 (1988).
Zaidi, I. et al. γδ T cells are required for the induction of sterile immunity during irradiated sporozoite vaccinations. J. Immunol. 199, 3781–3788 (2017).
Sissoko, M. S. et al. Safety and efficacy of PfSPZ vaccine against Plasmodium falciparum via direct venous inoculation in healthy malaria-exposed adults in Mali: a randomised, double-blind phase 1 trial. Lancet Infect. Dis. 17, 498–509 (2017).
Epstein, J. E. et al. Protection against Plasmodium falciparum malaria by PfSPZ vaccine. JCI Insight 2, e89154 (2017).
Jongo, S. A. et al. Safety and differential antibody and T-cell responses to Plasmodium falciparum sporozoite vaccine by age in Tanzanian adults, adolescents, children, and infants. Am. J. Trop. Med. Hyg. 100, 1433–1444 (2019).
Illingworth, J. et al. Chronic exposure to Plasmodium falciparum is associated with phenotypic evidence of B and T cell exhaustion. J. Immunol. 190, 1038–1047 (2013).
Teirlinck, A. C. et al. Longevity and composition of cellular immune responses following experimental Plasmodium falciparum malaria infection in humans. PLoS Pathog. 7, e1002389 (2011).
Diallo, H. et al. Longitudinal analysis of gamma delta T cell subsets during malaria infections in Malian adults. Malar. J. 18, 69 (2019).
Jagannathan, P. et al. Vδ2+ T cell response to malaria correlates with protection from infection but is attenuated with repeated exposure. Sci. Rep. 7, 11487 (2017).
De Rosa, S. C. et al. Ontogeny of γδ T cells in humans. J. Immunol. 172, 1637–1645 (2004).
Kisalu, N. K. et al. Author correction: a human monoclonal antibody prevents malaria infection by targeting a new site of vulnerability on the parasite. Nat. Med. 25, 188–189 (2019).
Jongo, S. A. et al. Safety, immunogenicity, and protective efficacy against controlled human malaria infection of Plasmodium falciparum sporozoites vaccine in Tanzanian adults. Am. J. Trop. Med. Hyg. 99, 338–349 (2018).
Morita, C. T., Jin, C., Sarikonda, G. & Wang, H. Nonpeptide antigens, presentation mechanisms, and immunological memory of human Vγ2Vδ2 T cells: discriminating friend from foe through the recognition of prenyl pyrophosphate antigens. Immunol. Rev. 215, 59–76 (2007).
Vantourout, P. & Hayday, A. Six-of-the-best: unique contributions of γδ T cells to immunology. Nat. Rev. Immunol. 13, 88–100 (2013).
Bonneville, M., O’Brien, R. L. & Born, W. K. γδ T cell effector functions: a blend of innate programming and acquired plasticity. Nat. Rev. Immunol. 10, 467–478 (2010).
Greenwood, B. M., Bradley-Moore, A. M., Bryceson, A. D. & Palit, A. Immunosuppression in children with malaria. Lancet 1, 169–172 (1972).
Ho, M. et al. Antigen-specific immunosuppression in human malaria due to Plasmodium falciparum. J. Infect. Dis. 153, 763–771 (1986).
McBride, J. S. & Micklem, H. S. Immunosuppression in murine malaria. II. The primary response to bovine serum albumin. Immunology 33, 253–259 (1977).
Whittle, H. C. et al. T-cell control of Epstein–Barr virus-infected B cells is lost during P. falciparum malaria. Nature 312, 449–450 (1984).
Division of AIDS, National Institute of Allergy and Infectious Diseases, National Institutes of Health, US Department of Health and Human Services. Division of AIDS (DAIDS) Table for Grading the Severity of Adult and Pediatric Adverse Events. Version 2.0. https://rsc.niaid.nih.gov/clinical-research-sites/daids-adverse-event-grading-tables (2014).
Steinhardt, L. C. et al. Safety, tolerability, and immunogenicity of PfSPZ vaccine administered by direct venous inoculation to infants and young children: findings from an age de-escalation, dose-escalation double-blinded randomized, controlled study in western Kenya. Clin. Infect. Dis. 71, 1063–1071 (2020).
U.S. Department of Health and Human Services, National Institutes of Health, National Institute of Allergy and Infectious Diseases. Division of Microbiology and Infectious Diseases (DMID) Pediatric Toxicity Tables November 2007 Draft https://www.niaid.nih.gov/sites/default/files/dmidpedtox.pdf (2007).
World Health Organization. Microscopy for the Detection, Identification and Quantification of Malaria Parasites on Stained Thick and Thin Films in Research Settings (WHO, 2015).
Swysen, C. et al. Development of standardized laboratory methods and quality processes for a phase III study of the RTS, S/AS01 candidate malaria vaccine. Malar. J. 10, 223 (2011).
Informal Consultation on Quality Control of Malaria Microscopy (WHO, 2006).
Taylor, S. M. et al. A quality control program within a clinical trial Consortium for PCR protocols to detect Plasmodium species. J. Clin. Microbiol. 52, 2144–2149 (2014).
Hermsen, C. C. et al. Detection of Plasmodium falciparum malaria parasites in vivo by real-time quantitative PCR. Mol. Biochem. Parasitol. 118, 247–251 (2001).
Beddall, M., Chattopadhyay, P. K., Kao, S.-F., Foulds, K. & Roederer, M. A simple tube adapter to expedite and automate thawing of viably frozen cells. J. Immunol. Methods 439, 74–78 (2016).
Swanson, P. A.2nd & Seder, R. A. OMIP-067: 28-color flow cytometry panel to evaluate human T-cell phenotype and function. Cytometry A 97, 1032–1036 (2020).
Monaco, G. et al. flowAI: automatic and interactive anomaly discerning tools for flow cytometry data. Bioinformatics 32, 2473–2480 (2016).
Zou, G. A modified Poisson regression approach to prospective studies with binary data. Am. J. Epidemiol. 159, 702–706 (2004).
Andersen, P. K. & Gill, R. D. Cox’s regression model for counting processes: a large sample study. Ann. Stat. 10, 1100–1120 (1982).
Acknowledgements
We thank the caregivers and infants and the study staff who made this study possible. We thank the data safety and monitoring board members for their careful review of safety data and recommendations: K. Kester (chair), A. Durbin, M. Molyneux, M. Spring, J. Ciolino and J. Otieno (local safety monitor). We thank the Sanaria Manufacturing and Quality Teams for providing the PfSPZ Vaccine for this study and W. Wijayalath for pharmaceutical operations support. We also thank the Sanaria Clinical and Regulatory team for supporting this trial. We thank the Kenya Medical Research Institute for support and for providing permission to publish the results. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the U.S. Centers for Disease Control and Prevention. This work was supported by the NIH Vaccine Research Center. Manufacturing and quality control release and stability assays for the PfSPZ Vaccine were supported in part by the National Institute of Allergy and Infectious Diseases, NIH (Small Business Innovation Research grant nos. 5R44AI055229-09A1 and 2R44AI058375-06A1 to S.L.H.).
Author information
Authors and Affiliations
Contributions
M.O., L.C.S., R.Y., S.L.H., T.L.R. and R.A.S. planned the study. M.O., R.Y., D.A., T.S., E.L.N., A.D., P.N.O., K.O., D.K.B., S.K., W.C. and A.M.S. conducted the study. B.K.L.S., E.R.J., N.K.C., P.F.B., T.L.R. and S.L.H. provided the study product. P.A.S.II, R.A.S., K.O., W.C. and N.K.C. conducted the laboratory and immunogenicity analyses. G.A. analyzed all the ECGs. R.E.W., D.S. and G.E.P. analyzed the data. S.J., S.A., C.D. and M.M. provided samples for the immunogenicity data. M.O., L.C.S., K.O., R.E.W., J.R.G., T.S., S.K., A.M.S., T.L.R., B.K.L.S., S.L.H., P.A.S.II and R.A.S. interpreted the study results. M.O., L.C.S., S.L.H., T.L.R., P.A.S.II and R.A.S. wrote the paper. All authors reviewed, edited and approved the paper.
Corresponding authors
Ethics declarations
Competing interests
T.L.R., N.K.C., P.F.B., E.R.J., B.K.L.S. and S.L.H. are employees of Sanaria, which manufactures the vaccine tested in this study. S.L.H. and B.K.L.S. are named inventors on patents related to the PfSPZ Vaccine. All other authors report no potential conflicts of interest.
Additional information
Peer review information Nature Medicine thanks Laurent Renia, W. Ripley Ballou, Kennedy Otwombe and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. Alison Farrell was the primary editor on this article and managed its editorial process and peer review in collaboration with the rest of the editorial team.
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Extended data
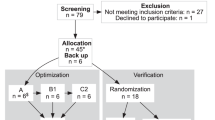
Extended Data Fig. 1 Trial Profile.
Trial enrolment and participation details.
Extended Data Fig. 2 Proportional efficacy of PfSPZ Vaccine over time.
Proportional efficacy of various doses of PfSPZ Vaccine against Plasmodium falciparum parasitemia (>0 parasites/µL) at 3, 6, 9, and 12 months follow-up.
Extended Data Fig. 3 Survival analysis of first/only clinical malaria.
Kaplan-Meier survival analysis of time-to first or only clinical malaria episode over 12 months, by treatment group.
Extended Data Fig. 4 Flow cytometry gating for analysis of T cells.
(a–g) Cellular gating tree using the 28-color panel outlined in Supplementry Information Tables 10 and 11. (a) Lineage gating of T cells. After gating on single cells, lymphocytes, and live CD3+ T cells, a pan-TCRγδ antibody was used to separate γδ and αβ T cells, which were further subdivided into CD4+ and CD8+ αβ T cells. (b) CCR7 and CD45RA antibodies were used to gate CD4+ and CD8+ αβ T cell naïve and memory subsets. Naive T cells (naïve), Central and transitional memory T cells (Tcm/Ttm), Effector memory T cells (Tem), and Effector T cells (Tef). (c) CD38 and HLA-DR were used to identify activated non-naïve CD4 and CD8 αβ T cells and γδ T cells. (d) CXCR5+ was used to identify blood T follicular helper (TfH) cells of non-naïve CD4 T cells, and blood TfH subsets were further characterized using PD-1 and CXCR3. (e) CD25 and CD127 were used to identify T regulatory cells (Tregs). (f) CD31 and CD45RA were used to identify recent thymic emigrants (RTEs) of CD4 T cells. (g–i) Gating to measure T cell function following no stimulation or stimulation with PfSPZ. The panel used in Supplementary Table 10 was used for the functional gating of non-naïve CD4 and CD8 T cells in (g) and (h), respectively, while the panel in Supplementary Table 11 was used for the Th2 and Th17 gating of non-naïve CD4 T cells in (i). (j) TCR Vδ1 and Vδ2 antibodies were used to identify γδ T cell subsets. Vδ1 and Vδ1/Vδ2- T cell subsets were further analyzed for naïve (CD27+CD127+) vs clonal expansion (CX3CR1+CD127−). Vγ9 was used to identify Vγ9+ or Vγ9- Vδ2+ T cells.
Extended Data Fig. 5 PfSPZ Vaccine-induced T cell responses.
(a–d) T cell response to PfSPZ Vaccine. Percent of non-naïve CD4 T cells in the blood expressing IL-8 (A), IL-21 (b), Th2 cytokines (c), or IL-17 (d) at pre-immunization (blue) or 2 weeks after the 3rd immunization (red) of the indicated dose of PfSPZ Vaccine. Results are the percentage of cytokine-producing cells after incubation with PfSPZ minus the percentage of cytokine-producing cells after incubation with vaccine diluent (medium with 1% human serum albumin). Bars indicate median values within each group. Bars indicate median values and differences at each timepoint between pre and post vaccination groups were assessed using multiple T tests with Holm-Sidak’s correction for multiple comparisons. (e) A single PfSPZ-vaccinated adult PBMC sample was included in each batch as a positive control for PfSPZ stimulation. Each symbol represents the percent of non-naïve CD4 T cells expressing CD154, IFNγ, IL-2, or TNF (blue) or γδ T cells expressing IFNγ, IL-2, or TNF (red) in the positive control sample within a single batch. Green bars indicate median values. (f) Percent of non-naïve CD4 T cells expressing CD154, IFNγ, IL-2, or TNF or CD8 T cells expressing IFNγ, IL-2, or TNF in adult control samples following PMA/ionomycin stimulation.
Extended Data Fig. 6 Infection susceptibility correlates with pre-vaccination γδ T cell frequencies.
Pre-vaccination frequencies of Vδ1 (left) and Vδ2 (right) γδ T cell populations in subjects that were either uninfected (blue) or infected (red) during the vaccination period (dVax), during 3-month ATP, or during 6-month ATP. Differences at each timepoint between pre and post vaccination groups were assessed using multiple T tests with Holm-Sidak’s correction for multiple comparisons. *P<0.05, **P<0.01.
Extended Data Fig. 7 Net increase of IgG and IgM antibodies to PfCSP two weeks after the last dose of PfSPZ Vaccine in infants by dosage group who were followed for at least 3 months and 6 months.
Filled and unfilled circles represent uninfected (protected) and infected subjects.
Extended Data Fig. 8 Median and interquartile range of net OD 1.0 for IgG and IgM antibodies to PfCSP two weeks after the last dose of PfSPZ Vaccine in infants who were uninfected (protected) and infected during 3 months follow up.
Filled and unfilled circles represent uninfected (protected) and infected subjects.
Extended Data Fig. 9 Flow cytometry gating for phenotyping analysis of B/innate immune cells.
Cellular gating tree using the 25-color panel outlined in Supplementry Table 4. (A) Lineage gating includes gating on single cells, leukocytes, live cells, and then CD19 and CD3 are used to separate live B cells, T cells, and NK/myeloid cells. (B) T cell gating to identify γδ T cells (pan-γδ TCR) and mucosal-associated invariant T (MAIT) cells (CD161+TCRVα7.2+). (C) Gating for B cell populations. B cells were further divided into memory B cells (CD27+IgD+), immature B cells (CD10+CD21+), and atypical B cells (CD27-CD21+). Memory B cells were further divided into plasmablasts (CD38+CD20-), plasmodium (CSP)-specific B cells (CSP-probe+), and B cell isotypes using IgG and IgM antibodies. (D) Gating tree to identify various subsets of NK/myeloid cell populations. NK cell populations were first divided by CD56 expression. From the CD56- cell gate, monocyte subsets were characterized using CD14 and CD16. CD14-CD16- that were HLA-DR+ were used to identify dendritic cell (DC) populations including plasmacytoid DCs (pDCs) (CD123+CD11c-) myeloid-derived DCs (mDCs) (CD123-CD11c+). mDCs subsets were identified using CD1c and CD141.
Supplementary information
Supplementary Information
Supplementary Tables 1–14.
Rights and permissions
About this article

Cite this article
Oneko, M., Steinhardt, L.C., Yego, R. et al. Safety, immunogenicity and efficacy of PfSPZ Vaccine against malaria in infants in western Kenya: a double-blind, randomized, placebo-controlled phase 2 trial. Nat Med 27, 1636–1645 (2021). https://doi.org/10.1038/s41591-021-01470-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41591-021-01470-y
This article is cited by
-
Ageing of Plasmodium falciparum malaria sporozoites alters their motility, infectivity and reduces immune activation in vitro
Malaria Journal (2024)
-
A replication competent Plasmodium falciparum parasite completely attenuated by dual gene deletion
EMBO Molecular Medicine (2024)
-
Malaria vaccine efficacy, safety, and community perception in Africa: a scoping review of recent empirical studies
Infection (2024)
-
Current Status of Malaria Control and Elimination in Africa: Epidemiology, Diagnosis, Treatment, Progress and Challenges
Journal of Epidemiology and Global Health (2024)
-
Protective efficacy and safety of radiation-attenuated and chemo-attenuated Plasmodium Falciparum sporozoite vaccines against controlled and natural malaria infection: a systematic review and meta-analysis of randomized controlled trials
Infection (2024)
