
Abstract
Despite a high rate of concurrent mathematical difficulties among children with dyslexia, we still have limited information regarding the prevalence and severity of mathematical deficits in this population. To address this gap, we developed a comprehensive battery of cognitive tests, known as the UCSF Mathematical Cognition Battery (MCB), with the aim of identifying deficits in four distinct mathematical domains: number processing, arithmetical procedures, arithmetic facts retrieval, and geometrical abilities. The mathematical abilities of a cohort of 75 children referred to the UCSF Dyslexia Center with a diagnosis of dyslexia, along with 18 typically developing controls aged 7 to 16, were initially evaluated using a behavioral neurology approach. A team of professional clinicians classified the 75 children with dyslexia into five groups, based on parents’ and teachers’ reported symptoms and clinical history. These groups included children with no mathematical deficits and children with mathematical deficits in number processing, arithmetical procedures, arithmetic facts retrieval, or geometrical abilities. Subsequently, the children underwent evaluation using the MCB to determine concordance with the clinicians’ impressions. Additionally, neuropsychological and cognitive standardized tests were administered. Our study reveals that within a cohort of children with dyslexia, 66% exhibit mathematical deficits, and among those with mathematical deficits, there is heterogeneity in the nature of these deficits. If these findings are confirmed in larger samples, they can potentially pave the way for new diagnostic approaches, consistent subtype classification, and, ultimately personalized interventions.
Similar content being viewed by others
Introduction
Dyslexia is a neurodevelopmental disorder characterized by difficulties with accurate or fluent word recognition, poor decoding, and poor spelling abilities, despite normal intelligence, schooling, and language exposure. This disorder affects ~5–10% of the global population and is primarily associated with reading impairment. However, increasing evidence suggests that neurodevelopmental disorders rarely occur in isolation. The rate of overlap between dyslexia and other learning disorders is extremely high, ranging from 20% to 70%. This suggests that individuals with dyslexia may also experience challenges in other cognitive domains. Specifically, children with dyslexia often exhibit lower mathematical achievement and encounter specific difficulties in various mathematical domains1. Around 40% of children with reading difficulties are reported to have difficulties in learning math2,3,4. Prevalence estimates for children with dyscalculia who also have dyslexia vary widely, from 17%5 to as high as 64%6,7.
Despite the evident coexistence of dyslexia and mathematical deficits, the specific profiles and underlying cognitive mechanisms that characterize the relation between linguistic and mathematical aspects of cognition are still a matter of debate. Mathematical difficulties observed in children with dyslexia are generally not specific to number processing2,3,4. Difficulties in retrieving arithmetic facts from long-term memory8 are common in dyslexia9. Impairments in specific cognitive domains (such as verbal working memory, visuospatial working memory, and lexical naming speed) could also explain the co-occurrence of deficits in mathematical cognition and reading challenges4,10,11.
Understanding the nature of mathematical deficits in children with dyslexia is essential for designing appropriate interventions and elucidating the complex relationship between reading and mathematical abilities. To address this knowledge gap, we designed and tested a new battery of tests, the UCSF Mathematical Cognition Battery (MCB), specifically designed to comprehensively assess mathematical deficits in a cohort of dyslexic children. The development of the MCB is rooted in the extensive body of cognitive and neuroscientific research. Here, we provide a comprehensive description of this research and elucidate its influence in shaping the selection of the four mathematical domains evaluated by the MCB: 1. number processing; 2. arithmetical procedures; 3. arithmetic facts retrieval; and 4. geometrical abilities.
Research in neuroscience12 provides evidence supporting a potential classification of mathematical impairments. It reveals that a selective deficit in numerical processing, which is typical in dyscalculia, is just one among several possible deficits. Specifically, difficulties in arithmetic fact retrieval, calculation abilities13,14,15,16, and visuospatial skills17 have been associated with distinct brain regions.
Moreover, multiple research groups2,14,18,19,20,21,22,23 provide converging evidence that emphasizes the fundamental role of four cognitive and neural domains in acquiring mathematical skills. These domains encompass number processing; arithmetical procedures; arithmetic facts retrieval; and geometrical abilities.
These four domains, which affect mathematical cognition and differ in their cognitive and neural correlates, can be differentially impacted by neurological processes and environmental factors. Consequently, they likely contribute to the classification of mathematical deficits.
Number processing skill refers to the ability to manipulate, generate, and interpret numbers. The development of the number concept requires an innate basic number sense24 or number module2 and the acquisition of its exact numerical and linguistic representations. Converging evidence indicates that humans are born with the ability to represent numbers as continuous quantities along a mentally organized number line25,26,27,28. Additionally, the foundation of the number concept has been associated with two nonverbal systems: subitizing, which involves quickly recognizing the cardinality of small sets of objects29, and the approximate number system (ANS), which enables estimation of numerical magnitude for larger sets of objects18. These systems are present from infancy27,30,31,32,33 and are shared with various animal species31,34.
While there is ongoing debate regarding whether subitizing abilities are linked to counting skills and other non-numerical capacities such as attention and working memory35,36,37,38,39, the ANS is considered a fundamental component of numerical cognition development27,29,40,41. Numerous studies have shown that ANS acuity predicts later mathematical achievement42,43, and it is frequently impaired in children with mathematics learning disorders12,29.
The brain network involved in number processing primarily encompasses the lateral parietal lobe but also extends to the inferior frontal gyri, insula, and subcortical structures44. With such an extensive network of brain regions, problems in mathematical reasoning can stem from various underlying computations, leading to different behavioral phenotypes.
Deficits in number processing, which characterize developmental dyscalculia, manifest through multiple symptoms in learning mathematics, including difficulties in manipulating and transcribing numbers45. A lack of understanding of the concept of numerosity hinders the normal development of number representation13, as well as number production and comprehension14,20,21. Children with deficits in number processing exhibit impairments in transcribing numbers across different formats (e.g., from pictures or words to Arabic numerals) and in comparing and ordering quantities46,47. Regarding counting, process deficits are primarily observed in counting backward, counting by twos or threes, and completing sequences48.
Therefore, clinical assessment of deficits in number processing should include subitizing, non-symbolic ANS (comparison between two arrays of dots), symbolic ANS (comparison between two numbers written in digit form), and principles of counting, comparisons, ordering, and transcribing between number digits and number words.
Arithmetical procedures (or calculation) skill refers to the ability to perform mental and written addition, subtraction, multiplication, or division strategies, typically without relying on counting. This skill is crucial for providing accurate mathematical solutions and plays a significant role in speeding up the problem-solving process. The activation of appropriate numerical representations is essential for executing calculations correctly49,50. However, deficits in arithmetical procedures may arise even when numerical skills remain intact51,52,53. These deficits may manifest as isolated difficulties in solving arithmetic problems13,15,54.
The brain network involved in calculation processes seems to encompass a complex system of interconnected fronto-parietal cortical and subcortical regions55,56,57.
Finger counting is often observed in children experiencing difficulties with arithmetic procedures58,59, possibly as a means to reduce the load on working memory during calculation processing46 or due to reliance on immature calculation strategies. Deficits in arithmetical procedures can also arise when children struggle to acquire efficient calculation strategies16,60, which are known to follow specific developmental trajectories61. For instance, a child might have difficulty transitioning from relying on external aids, such as fingers, to employing more advanced mental strategies like counting on (e.g., solving 2 + 7 = 9 by recognizing the larger addend as 7 and then counting on from eight to nine62,63).
When assessing calculation arithmetical procedures skills clinically, it is important to cover mental calculations, particularly addition and subtraction, as well as written calculations involving all four operations.
Arithmetic facts are simple mathematical operations that children are expected to memorize and store in long-term memory52,64,65. Memorizing these facts is crucial for performing quick calculations, which form the foundation of mathematical competence. Without knowledge of multiplication tables, for example, children cannot effectively learn written multiplication and division. Difficulties in mastering arithmetic facts can sometimes manifest as isolated challenges in mathematics13,15,54.
The retrieval and calculation of arithmetic facts involve overlapping yet distinct brain areas66,67. While calculations have been linked to the previously mentioned fronto-parietal network, the learning and recall of arithmetic facts appear to rely on the hippocampal, para-hippocampal, and retrosplenial structures, with the angular gyrus playing a critical role56,68.
Children who struggle with arithmetic facts often face difficulties in memorizing basic addition and subtraction facts (e.g., 2 + 2 = 4, 3–1 = 2) or recalling multiplication tables (e.g., the tables of 6, 7, and 8). However, if their number processing and arithmetical procedures skills remain intact, they may be able to reconstruct operation results using counting and mental strategies.
When conducting clinical assessments of arithmetic facts retrieval, it is crucial to evaluate an individual’s knowledge of these facts. The testing should include appropriate assessments of multiplication tables, taking into account the individual’s age and educational level.
Difficulties in mathematics can still be observed in children who have intact numerical skills, calculation abilities, and memory functions for recalling arithmetic facts. In such cases, deficits often lie in the non-linguistic aspects of mathematical information69, including visuo-perceptual, visuospatial, and visuo-constructional skills. These nonverbal abilities have been shown to predict mathematical performance, particularly in geometry acquisition70,71.
Geometrical knowledge is believed to be based on two core knowledge systems: an innate ability to quantitatively process visual properties (e.g., length, angle, and shape) and a later-developed ability to process specific geometrical concepts (e.g., parallel vs. perpendicular lines)72. Visuo-perceptual, visuospatial, and visuo-constructional abilities have been localized in the occipito-temporal73,74, temporo-parietal75, and parietal76 cortices, respectively, with a right hemisphere lateralization.
Deficits in geometrical abilities can manifest as visuo-perceptual difficulties in processing symbols, arranging numbers for written calculations, interpreting graphs and figures, and recognizing salient visual features of objects13. Symptoms may also be present in processing visuospatial information, such as spatial reasoning about orientations, directions, and distances, as well as visuo-constructional information necessary for transforming three-dimensional objects77,78,79.
When clinically assessing geometrical abilities, tasks should include (1) processing distances and directions to assess visuospatial ability, (2) matching shapes presented in different orientations or decomposed to demonstrate visuo-perceptual ability, and (3) mental rotations of 2D and 3D objects to assess visuo-constructional functions80. It is important to note that stimuli in 3D and 2D are processed differently in the brain81; for example, 3D stimuli impose a higher load on the perceptual system but are memorized better than 2D stimuli82.
Drawing from research in mathematical cognition and neuroscience, which supports the potential classification of four distinct mathematical deficits, we have developed and evaluated a new battery of tests called the UCSF MCB. The MCB is specifically designed to comprehensively assess the four previously mentioned mathematical domains: 1. number processing; 2. arithmetical procedures; 3. arithmetic facts retrieval; and 4. geometrical abilities. In this article, we provide a detailed description of the battery and present the results obtained from a large cohort of children (n = 75) referred to the UCSF Dyslexia Center with a dyslexia diagnosis, as well as 18 typically developing control children. Our focus is on classifying mathematical cognitive deficits in children with dyslexia.
Results
Performance in MCB for clinically defined groups
There were no group differences noted in the demographic characteristics, such as sex, handedness, and age at testing. As expected and defined, there was a significant group difference in diagnoses. However, when the controls were removed from the analysis, the significant group difference in diagnoses was no longer present (p = 0.318).
No significant differences were found in the distribution of mathematical deficits across grades (p = 0.83). However, it should be noted that this analysis may be underpowered due to the relatively low number of cases in some groups.
The UCSF-MCB confirmed the clinicians’ impression for the 18 typically developing control children and the 25 children with dyslexia but no challenges in mathematics (referred to as the Dysl_notM group in Table 1). The Dysl_notM group (n = 25, one-third of the dyslexia sample) and the typically developing group (referred to as the TD group in Table 1) differed significantly only in the Approximate Number System (ANS) for digits. The TD group performed significantly better than all other subgroups on the ANS for digits. It is possible that the Dysl_notM group performed worse than the TD group in this subtest because 20% of the Dysl_notM group had ADHD, and attentional deficits may affect the ANS score. Additionally, performance on the subitizing subtest revealed a main effect of group (p = 0.031), but post hoc analysis indicated a specific group effect only for TD compared to all other groups combined (TD mode = 6 dots; all other groups combined mode = 5; p = 0.016).
The Dysl_notM group performed well on the MCB subtests evaluating number processing, arithmetical procedures, arithmetic facts retrieval, and geometrical abilities. Some of these participants obtained low scores only on subtests assessing teaching exposure (e.g., 8% obtained a low score in the “equivalent fractions” subtest, and 18% in the “percentage” subtest) or more complex mathematical skills (e.g., 30% obtained a low score in the “simplifying expressions” subtest, and 36% obtained a low score in the “solving equations” subtest).
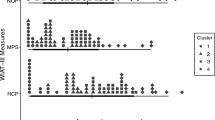
The other 50 participants from our dyslexic cohort (50/75, 66.6%), classified by the clinicians’ team as having deficits in mathematics, performed poorly on specific subtests of the MCB corresponding to their specific deficit (refer to Fig. 1b). Significant group differences were found in all subtests of the MCB math battery (refer to Table 1), except for the 2D shape reconstruction test (refer to Supplementary Table 1, # 26).

a The distribution of each group across our sample (n = 90): typical developing controls (TD, n = 18), dyslexia and no challenges in mathematics (Dysl_notM; n = 25), deficits in number processing (n = 10), deficits in arithmetical procedures (n = 15), deficits in arithmetic facts (n = 15), or deficits in geometry (n = 7). b Standard score performance on tasks weighing on number processing (yellow), arithmetical procedures (green), arithmetic fact retrieval (blue), and geometrical abilities (purple), for the six groups identified: typically developing (TD) children, children with dyslexia not affecting mathematical abilities (Dysl_notM), children with deficits in number processing, arithmetical procedures, arithmetic facts retrieval, and geometrical abilities. Errors bars represent standard errors of the mean. Details on the different subtests (including examples of incorrect responses) are in Supplementary Table 1.
Children with deficits in number processing (n = 10, 13.3% of dyslexia sample) performed significantly lower than all other groups on number subtests and obtained low scores in most of the MCB’s subtests. They showed a pattern of weakness in at least three of the number subtests (shown in Supplementary Table 1, #1–8) or a severe deficit in comparing, ordering, or transcoding numbers from one representation to another with lexical or syntactical mistakes (see Supplementary Table 2 for inclusion and exclusion criteria). Lexical mistakes refer to instances when digits are incorrectly chosen, but the order of magnitude is correct, e.g., 250 instead of 215. Syntactical mistakes refer to instances when digits are correctly chosen, but the order of magnitude is incorrect, e.g., 20,053 instead of 2053. Children with deficits in number processing performed significantly lower than all other groups in the addition and subtraction subtests of the calculations section and the multiplication subtest of the arithmetic facts section, which suggests that deficits in number processing represent more fundamental deficits in learning mathematics. They also performed worse than TD and Dysl_notM subgroups on the ANS for digits.
Children with deficits in arithmetical procedures (n = 15, 20% of dyslexia sample) showed a pattern of weakness in at least one of the three calculation subtests (Supplementary Table 1: #9. Mental additions, #10. Mental subtractions, #13. Written calculation) or were accurate but slow at calculations (see Supplementary Table 2 for inclusion and exclusion criteria. Notably, they performed significantly differently from all other groups on the subtraction subtest: the completion time is the highest of all groups, and the performance is lower than the other groups, except for those with deficits in number processing. The group of children showing deficits in arithmetical procedures also had low scores on the sequencing subtest (Supplementary Table 1, #3). They correctly identified the pattern in each sequence but made mistakes in calculating the answer. Surprisingly, the arithmetical procedures group exhibited comparable performance to children with number processing deficits. Notably, they did not demonstrate strong performance in the number processing subtests. However, their scores in these particular subtests were still relatively higher than those of the number processing group. In general, the group showing deficits in arithmetical procedures performed better on most subtests than the group showing deficits in number processing but worse than the other subgroups.
Children with deficits in arithmetic facts retrieval (n = 15, 20% of dyslexia sample) obtained low scores or accurate but slow performance on multiplication and division problems (Supplementary Table 1: #11. Mental multiplication and #13. Written Calculation). They demonstrated a specific deficit in the time to complete the multiplication table (see Supplementary Table 2 for inclusion and exclusion criteria). They also took the longest to complete the written calculation subtest, which also includes multiplication and division.
Children with deficits in geometry (n = 7, 9.3% of dyslexia sample) performed lower than TD group, Dysl_notM group, and the group with deficits in arithmetic facts retrieval on the computerized geometrical test (Supplementary Table 1, #27). They showed a pattern of weakness in the geometry subtests (Supplementary Table 1: #25. 2D shape reconstruction, #26. From 2D shapes to 3D models) performing significantly lower on the 3D models than that Dysl_notM group (see Supplementary Table 2 for inclusion and exclusion criteria). However, they performed not significantly different from the group with deficits in number processing on both computerized geometrical subtest and the 3D models subtest. The group with deficits in geometrical abilities was the only group to perform worse than TD on the ANS for dots (p = 0.032). In this subtest, numbers are represented through dots, which might be confusing for children who have trouble perceiving forms and identifying shapes. Visual impairments were excluded.
Three participants (4% of dyslexia sample) were excluded from further analyses because their deficits overlapped in arithmetic procedures and fact retrieval, and a clear subgroup could not be determined.
In summary, among the 75 participants referred with a diagnosis of dyslexia, 50 had trouble in mathematics (i.e., two-thirds of dyslexia sample). The clinician’s assessment was confirmed for all but three (n = 47) of the children in the dyslexia group. Only 13.3% of dyslexia sample showed impairment in number processing (n = 10). Most children (40% of the dyslexia sample) had impairments in arithmetical procedures (n = 15) or arithmetic facts retrieval (n = 15). Only 9.3% of dyslexia sample showed impairments in geometry (n = 7). See Fig. 1a for more details.
Performance in the WJ-IV calculation test
In the WJ-IV Calculation test, around 30% of children with no apparent difficulties in mathematics (8 out of 25 children) obtained a result below the 16 percentiles outside the average range (any score that falls one standard deviation below the mean indicates below-average performance). However, not one of these children obtained a low score in prior mathematical assessments using the WJ-IV (Broad Math, Applied Problems, Fluency), Wechsler Individual Achievement Test (WIAT; Math, Numerical, Problem Solving, Fluency), Kaufman Test of Educational Achievement (KTEA; Math Concepts and Applications, Computation, Fluency, Problem Solving), or the Feifer Assessment of Mathematics83. Furthermore, their previous and current history did not indicate any symptoms of mathematical difficulty.
On the other hand, ~25% of the children with dyslexia and mathematics difficulties (12 out of 47) obtained a score on the WJ-IV Calculation test at or greater than the 25th percentile (average performance); of these children, none had deficits in number processing, five had deficits on arithmetic facts retrieval, three on arithmetical procedures, and four on geometrical abilities.
Group performance in neuropsychological and academic assessments
Despite the small number of children in each group with impairment in mathematics, we nevertheless present results in neuropsychological and academic tests. Among the groups with dyslexia, statistically significant differences were also noted in the performance of WJ-IV Calculations (WJ Calc), nonverbal reasoning (Matrix Reasoning), and judgment of line orientation (JLO) tests (Table 2). Specifically, the group with Dysl_notM had higher scores on the WJ Calc and Matrix Reasoning subtests than the groups showing deficits in number processing and arithmetical procedures. There were also group differences on JLO, but the Dysl_notM and the group with a deficit in arithmetic facts retrieval performed better than the group with a deficit in number processing.
Children with deficits in number processing obtained the lowest scores in all neuropsychological assessments except for the CCT 1 (timed ordinal number sequencing), the Beery VMI, and the DKEFS Design Fluency-filled. Post-hoc analyses revealed they performed significantly worse than the Dysl_notM group on WJ Calc, Matrix Reasoning, and JLO tests (Table 2; all p’s < 0.05 Bonferroni-corrected). They also had significantly lower scores on JLO than the arithmetic fact retrieval group (p < 0.05 Bonferroni-corrected). Most deficits appeared in tests that require visual reasoning and judgments, but verbal knowledge was spared.
Children with deficits in arithmetical procedures obtained lower scores than the Dysl_notM group on WJ Calc and Matrix Reasoning.
Children with deficits in arithmetic facts retrieval did not perform worse than other groups in any of the neuropsychological tests. They had the highest group average of the dyslexia sample on untimed line degree matching (JLO) and performed significantly better than the children with deficits in number processing. The children with deficits in arithmetic facts retrieval also had the highest scores on geometry subtests of the MCB among the groups with math difficulties.
Children with deficits in geometry obtained good scores in general cognitive and academic tests, as well as in processing speed tests. Even though not significantly different, their scores on the visuomotor test (Beery VMI) were the lowest. They also had a low score in long-term visual recall (Rey-Osterrieth Figure 3-minute Delay). Notably, both these tests require drawing.
Discussion
There is a notable lack of comprehensive studies that have systematically examined various components of mathematical skills in cohorts of children with concurrent learning difficulties. Despite the significant prevalence of mathematical deficits among children with dyslexia (average 40%4), our understanding of the frequency and severity of these deficits in this population remains limited.
To address this gap, we have developed and evaluated the UCSF MCB, a set of subtests specifically designed to classify mathematical cognitive deficits in children with dyslexia. The MCB was developed at UCSF Dyslexia Center (UCSF-DC) and tailored for children ranging from 2nd to 8th grade. It spans number processing, arithmetical procedures, arithmetic facts retrieval, and geometrical abilities, allowing for personalized educational practices and interventions based on individual profiles. In this study, we present the initial results of a large cohort of children referred with a diagnosis of dyslexia (n = 75) who were carefully evaluated by a group of expert clinicians. The MCB confirmed the clinicians’ mathematical impressions, demonstrating its potential as a promising assessment tool that can be scaled to larger cohorts of children. In the following discussion, we explore the clinical and educational implications of our findings and their relationship to current neurocognitive theories of mathematical deficits.
The main result of our study is that the MCB can effectively identify mathematical impairments in children with dyslexia. Among our cohort, 50 out of the 75 participants referred with a diagnosis of dyslexia at the UCSF-DC were found to have deficits in mathematics, which were rarely identified in their previous evaluations. This suggests that many cases of mathematical difficulties are currently going undetected. The commonly administered assessments such as WJ (Calculation Test, Broad Math, Applied Problems, Fluency), WIAT (Math, Numerical, Problem Solving, Fluency), KTEA (Math Concepts and Applications, Computation, Fluency, Problem Solving), and FAM may not capture difficulties in mathematics, particularly if those difficulties are not severe or related to number deficits.
Moreover, the currently available mathematical assessments do not effectively distinguish between deficits in number processing, arithmetical procedures, arithmetic facts retrieval, and geometrical abilities. Specifically, geometry is under-assessed in psychoeducational evaluations and should be included in the assessment of mathematical cognition. Identifying difficulties in geometry early on is crucial because it is possible to detect these difficulties even before formal instruction begins (which typically occurs in the 10th grade in the US). Children possess an innate capacity for geometrical intuition from an early age, as they are sensitive to shapes in both 2D and 3D and can recognize relationships between shapes and forms72,84,85,86. Difficulties in geometrical abilities can also impact a student’s ability to use mathematical symbols correctly (e.g., using “x” for multiplication and “+” for addition) and interpret graphs and charts, which are essential for tests in sciences and math, standardized placement tests, and job skills87.
A significant finding of our study highlights the potential of the MCB to classify mathematical deficits in children with dyslexia (refer to Supplementary Table 2: preliminary diagnostic decision guide). By assessing the participants’ performance and completion time on the MCB, dyslexic children with mathematical impairments can be categorized into one of four groups representing specific mathematical deficits: number processing, arithmetical procedures, arithmetic facts retrieval, and geometrical abilities. Two groups (the number processing group and the geometrical abilities group) demonstrated lower performance in the specific subtests associated with their respective subgroup (refer to Fig. 1). Conversely, the arithmetical procedures group and the arithmetic facts group did not show significantly poorer performance in their corresponding subtests. It is worth noting that the number processing group displayed inferior performance across the subtests related to arithmetical procedures and arithmetic facts retrieval. However, the arithmetic facts retrieval group exhibited the lowest scores in the subtests designed to identify challenges in arithmetic facts retrieval. Similarly, the arithmetical procedures group demonstrated the lowest scores in the subtests designed to pinpoint difficulties in calculation.
We will briefly explore potential criteria to describe the main characteristics of each group and the likely neurocognitive correlates.
Deficits in number processing are characterized by difficulties in understanding and manipulating numerical quantities. Children with deficits in number processing struggle with comprehending the magnitude of numbers, estimating quantities, and grasping numerical relationships. They may face challenges in counting, recognizing numbers, comparing numbers, and ordering them.
In the UCSF MCB, deficits in number processing were observed in at least three of the following subtests: translating numbers between different representations (digits, words, pictorial), comparing and ordering numbers, and completing number sequences. Sometimes deficits may also be observed in subitizing, and more frequently in the Approximate Number System (ANS), both in symbolic (digits) and non-symbolic (dots) formats. We found no significant difference in the group of children with a number processing deficit compared to the other groups in the subitizing test. However, these children often struggled to provide an accurate estimation of the number of dots when the quantity exceeded five. They would often state that there were 30, 40, 50, or 100 dots, even when the maximum number of dots on the screen was nine. In the MCB, children with a deficit in number processing performed worse than the control group and the other subgroups on the ANS for digits. While all groups tended to perform better on digits than dots, the children with a deficit in number processing only showed a slight improvement in digits compared to dots (a difference of one point), whereas the other groups showed greater differences (minimum difference: 6, maximum difference: 14). This further highlights the pervasive difficulties experienced by children with a deficit in number processing, regardless of the presentation format.
Numbers form the foundation of calculations, logical reasoning, and problem-solving; therefore, a deficit in numbers inevitably compromises many aspects of mathematical thinking88. It is not surprising that deficits in number processing have a detrimental impact on all other mathematical skills, as indicated by the low scores observed in this subgroup across the entire battery. These children exhibited impairments in calculation skills and geometrical abilities. Furthermore, the positive relationship between numerical skills and visuospatial skills36,89,90,91,92 may help explain the low scores obtained by these participants in the geometrical subtest. In these tests, no significant difference was observed between children with a deficit in number processing and children with a deficit in geometrical abilities in the geometrical subtests.
Additionally, children with a deficit in number processing demonstrated difficulties in various tests that require visual reasoning and judgment but showed preserved verbal knowledge. This suggests that a cognitive mechanism involving higher-order nonverbal reasoning and attention may underlie the difficulties observed in this subgroup.
It is plausible to consider that this subgroup represents the co-occurrence of dyslexia and dyscalculia. Dyscalculia is characterized by impairments arising from difficulties in connecting a number to its corresponding magnitude (number sense for Cohen & Dehaene24; number module for Butterworth2). Children with deficits in number processing often exhibit this difficulty through mistakes in counting, comparing and ordering numbers, and identifying patterns in numerical sequences.
In our sample, only 13.3% (10 out of 75) of the children with dyslexia were diagnosed with deficits in number processing. This indicates that only a small portion of dyslexic children who struggle in mathematics may also have dyscalculia.
Deficits in arithmetical procedures are characterized by a focal impairment when applying arithmetic procedures. While not showing deficits in numerical skills, children with deficits in arithmetical procedures struggle with understanding, applying, and reproducing mental and/or written calculations.
In the UCSF MCB, these children performed significantly differently from the other subgroups, except for the number subgroup, both in terms of accuracy and speed in calculations. Errors include treating subtraction as a commutative operation (e.g., 5–3 ≠ 3–5) and inverting the order of digits (e.g., 30−11 = 21 because 3–1 = 2, and 1–0 = 1). Slow processing was often due to the adoption of ineffective counting strategies, often supported by fingers or drawing. However, this group did not demonstrate a significant difference in performance compared to the number subgroup, making it challenging to precisely characterize their mathematical deficits. It is possible that they share similarities with the number subgroup, displaying mild difficulties. Alternatively, it is more likely that their difficulties stem from cognitive mechanisms unrelated to the mathematical domain, indicating that other factors might contribute to their challenges.
Unexpectedly, children with a deficit in arithmetical procedures performed poorly on some of the geometry subtests. A common denominator for this pattern of difficulties could be working memory, as previously suggested11,93,94. However, in our study, this group did not show group differences in working memory measures. Although the group sizes are relatively small, the standard deviations overlap with the means, and the sample includes individuals with co-occurring dyslexia, so it is possible that the results are concealed within this sample, indicating a potential sampling effect. Another possibility is that this group may have some visuospatial difficulties that make it challenging for them to keep numbers aligned during arithmetical procedures, leading to errors of alignment53. However, we do not have evidence to support this possibility in our data (only a few errors are due to misalignment of numbers in columns). Nonetheless, more than 50% of the children with deficits in arithmetical procedures (8 out of 15) incorrectly calculated the difference between two numbers, subtracting the smaller digit from the larger without respecting the order of subtraction with regard to the whole number (e.g., in 90 – 47, they subtract 0 from 7 and 4 from 9). This error could be associated with deficits in the spatial representation of quantitative information95 because the “direction” of the operation is incorrectly interpreted. They may also rigidly apply one rule, “subtract the smaller number from the larger,” at the expense of other rules, which may suggest difficulties in ranking competing choices.
It is also possible that when performing written calculations, we are constantly dividing our attention. If someone has proficient calculation skills and knowledge, they may divide their attention between the motor program of writing and the estimation of the correct result in order to check their work simultaneously. However, a child who has not mastered calculations may instead divide their attention between the motor program of writing and searching their mind for the appropriate calculation rules/algorithms for those numbers. If this is the case, interventions for this type of deficit may focus on alternate strategies that reduce the burden of divided attention.
Deficits in arithmetic facts are characterized by impairments in arithmetic facts retrieval. Children with deficits in arithmetic facts do not show difficulties in number subtests, and they are able to perform calculations. However, they struggle to recall the results of operations that should have been learned through rote memorization, such as multiplication facts. The deficit in recalling multiplication tables is coupled with difficulties in writing multi-step multiplications and divisions.
In the UCSF MCB, children with a deficit in arithmetic facts took the longest time to complete the multiplication table subtest and the written calculation subtest. It is crucial to evaluate not only the overall performance but also the response time: slow responses are likely associated with compensatory strategies that are only partially effective. For instance, complex multiplication can be solved by relying on the lengthy mental strategy of repeated addition (e.g., 8 × 4 is broken down into 8 + 8 = 16 and then 16 + 16 = 32). Children with deficits in arithmetic facts generally performed well in addition and subtraction tasks. Subtraction and multiplication are associated with distinct neural systems for numerosity and language96.
Children with deficits in arithmetic facts retrieval also had the highest scores on the geometry subtests of the MCB. One potential explanation is that this group may have developed enhanced visuospatial skills either in response to or because of their language difficulties. Balancing resources across the brain may lead to increased functionality in visuospatial skills to compensate for diminished functionality in language. Although fluency in reading and arithmetic are considered distinct abilities, significant correlations have been found between them97,98. Due to the similarities between the initial stages of reading and mathematical fluency development, it is likely that the same brain and cognitive mechanisms are involved in both domains99. Since our cohort was recruited based on symptoms of dyslexia, it is difficult for us to distinguish these differences. Future studies using the MCB to evaluate the performance of children with dyslexia compared to dyscalculia could help address this question.
Deficits in geometry are characterized by impairments in geometrical abilities. Children with deficits in geometry exhibit difficulties in the nonverbal representations of mathematical information. They may struggle to process distances and directions, match shapes, recognize geometrical transformations (e.g., symmetries, rotations), and mentally reconstruct a 3D model from a 2D shape.
In the UCSF MCB, children with deficits in geometrical abilities obtained the lowest scores on the geometry subtest and performed significantly worse on the 3D model test compared to the typical development (TD) group, the group with no deficits in math, and the group with deficits in arithmetic facts. In the computerized test72, they made mistakes in solving problems related to geometrical transformations (symmetries, rotations, and translations), distinguishing distances, and identifying characteristics of geometrical figures.
Notably, the group with a deficit in geometrical abilities was the only one to perform worse than the TD group on the Approximate Number System (ANS) for dots. There is a positive correlation between numerical skills and visuospatial skills, so it is not surprising that these individuals struggled to connect numbers with visual objects11,36,89,90,92.
Recent research suggests that spatial ability predicts performance in mathematics100, but it remains unclear which mathematical skills are involved. Our group of children with deficits in geometry is not large enough to draw conclusions on this point, and further research is necessary to validate our findings.
The existing research examining the relationship between dyslexia and mathematical impairments is limited and still underdeveloped. Interestingly, cognitive and neuropsychological research, along with an increasing body of evidence, including neuroimaging studies, has accepted the existence of different subtypes of dyslexia. This raises the possibility of subtyping difficulties in mathematics as well.
For instance, core deficit dyscalculia has been associated with abnormalities in the left IPS48,101,102. Moreover, arithmetic problem-solving difficulties have been associated with aberrant responses (hyperactivity and hyper-connectivity) in a number of posterior brain areas suggesting a critical role of parietal circuits in deficits related to arithmetical procedures103. Conversely, the medial temporal lobe, specifically the left hippocampus, has been implicated in arithmetic facts retrieval104,105. Finally, posterior inferior-temporal cortex (including the fusiform gyrus) and the posterior parietal cortex have been linked with geometry problem solving106, but further studies might aim at disentailing the specific neural correlates associated with visuo-perceptual, visuospatial, and visuo-constructional deficits.
The emerging line of research indicates that mathematical impairments may exhibit different profiles and underlying mechanisms, similar to the subtypes observed in dyslexia.
The MCB has not yet been standardized, and the current criteria rely on clinical and qualitative evaluations. Additionally, the MCB is relatively long and includes subtests that might be redundant (Supplementary Table 1: #14: Find the missing sign in the expression, #15: Find the missing number in the expression, #16: True/False) or unnecessary in identifying deficits in mathematics (Supplementary Table 1: #6: Estimation, #18: Percentage, #22: Name Figure, #24: 2D shape reconstruction). Other subtests appear to simply differentiate typically developing children from children with dyslexia but do not provide information on the specific deficits (subitizing and ANS for digits).
We have identified four subtypes of mathematical deficits: number processing, arithmetical procedures, arithmetic facts retrieval, and geometry. This is a preliminary classification of mathematical deficits, and further distinctions may be necessary. For example, transcoding numbers and understanding the magnitude of numbers are skills associated with different neurocognitive profiles107, suggesting that deficits in number processing might be subdivided into two distinct groups.
Given the developmental nature of learning difficulties related to mathematics, it is possible that mathematical deficits may present differently at different ages and/or be partially compensated through other cognitive strengths, such that one may only show difficulty when math reasoning becomes more complex, and the learning environment is less scaffolded. Therefore, future work should be careful to include skill assessments at varying points of development through adulthood.
Three subjects showed a pattern of errors so diverse as to preclude labeling in a specific subtype. As for all neurocognitive continuums that can be broken down into clinically meaningful subtypes, there will likely always be cases that cannot be ascribed to one specific category108. However, future studies might help to elucidate the unique cognitive and neural correlates of these mixed cases.
Finally, the cohort of children we tested (n = 93) is relatively small and unequal in group size, preventing more advanced statistical comparisons of the distinct mathematical deficits. It would be helpful to replicate these findings in larger studies and with reliability metrics for the MCB.
Despite recognizing the limitations in our approach, we believe that the MCB provides a foundation for clinically relevant and neurocognitively informed diagnoses and models. Currently, we are still in the development stage of the battery in which we are relying on detailed clinical observation to determine relevant subtests following a behavioral neurology methodological approach. We are currently administering a second version of the MCB, based on the present results, to increase our sample size with an independent group of subjects which will allow us to conduct refined psychometric standardization and to identify cut-off scores for each group. We plan to use the MCB to assess children who only have mathematical learning differences to investigate whether the four deficits align with subtypes of dyscalculia.
Methods
The UCSF MCB
The UCSF MCB is a comprehensive experimental battery developed to identify and differentiate difficulties in various mathematical domains, allowing for the identification of individual mathematical strengths and weaknesses. The MCB is designed for students ranging from the 2nd to the 8th grade and consists of seven different forms tailored to each specific grade level. It encompasses a total of 19 subtests, including 4 computer-based subtests and 15 paper-based subtests, targeting number processing, arithmetical procedures, arithmetic facts retrieval, and geometrical abilities. Additionally, eight subtests are included to evaluate more complex mathematical skills such as simplifying expressions, solving equations, and geometrical problems, while also assessing the level of teaching exposure, which is crucial for diagnosing learning differences in mathematics. Examples and detailed information can be found in Supplementary Table 1.
To evaluate the ability to recognize and compare magnitudes expressed through digits, words, or arrays of dots, eight subtests were designed, consisting of five paper-based problems and three computer-based tasks adopted from previous literature109.
Four subtests were specifically created to assess arithmetical procedures skills, with three focusing on mental calculation skills and the fourth evaluating written calculation abilities. The addition and subtraction problems within the calculation subtests were designed to target difficulties related to arithmetic procedures, while a mental multiplication subtest and the multiplication and division problems in the written calculation subtest aimed to evaluate arithmetic facts retrieval skills. Additionally, the time taken to complete the calculation subtests was recorded to assess fluency, which can help differentiate between difficulties in arithmetic procedures and arithmetic facts retrieval.
To assess geometrical abilities, a computerized task72,110 and three paper-based subtests were included. These tasks involved items that varied in terms of symmetry, rotation, shape, angles, and other relevant aspects.
Furthermore, three tasks were added to evaluate mathematical abilities in older children, such as simplifying expressions, solving equations, and modeling, in order to detect instances when individuals might have compensated for basic deficits but still experience difficulties with more complex problems. Additionally, seven supplementary tasks were designed to verify adequate teaching exposure and to confirm or exclude specific deficits, such as fractions. For instance, a deficit in arithmetical procedures could be confirmed when solving word problems if the appropriate operation is identified, but the calculation is performed incorrectly.
Participants
Participants were recruited through the UCSF-DC, a multidisciplinary research center dedicated to studying dyslexia and related neurodevelopmental cognitive disorders. At the UCSF-DC, participants who were referred due to concerns of dyslexia underwent a comprehensive research evaluation conducted by a team of clinicians, including neurologists, neuropsychologists, genetic counselors, speech and language pathologists, psychiatrists, and educational specialists. This team provided an overall diagnostic impression based on various factors, including clinical history (first symptoms and most severe impairments reported by parents and teachers), family history (similarities between siblings and/or parents), standard neuropsychological and academic testing, and questionnaire responses indicating clinical significance. Participants were excluded from the study if they exhibited borderline or impaired general cognitive scores, had a known history of severe perinatal events such as strokes or acquired brain injuries, or had genetic, neurological, or psychiatric disorders associated with seizures, impaired sensory processing, or aphasia. Inclusion criteria required fluency in English and an age between 7 and 16 years. The group of typically developing control participants consisted of volunteers recruited through advertisements and families expressing interest in participating in the study. Typically developing control participants had no subjective concerns regarding academic achievement, no prior diagnoses of neurodevelopmental disorders, an age range between 7 and 16 years, and fluency in English.
The final study cohort consisted of 93 children, including 18 typically developing children (7 female, mean age = 10.40 ± 1.66, 94% right-handed), 50 children diagnosed with dyslexia, and 25 children diagnosed with dyslexia and suspected attention-deficit/hyperactivity disorder (ADHD; 27 female, mean age = 11.78 ± 2.05, 92% right-handed). Detailed demographics can be found in Table 1.
Most children in the clinical group (57 out of 75, 76%) attended independent schools specifically tailored to children with learning differences, allowing their teachers to provide detailed descriptions of their academic challenges.
The guardians of the participants provided informed written consent, and the participants themselves provided assent. The study was approved by the University of California San Francisco (UCSF) Institutional Review Board and complied with the Declaration of Helsinki.
Study procedure
Clinical classification. As part of the UCSF-DC diagnostic process, the team of clinicians considered each child’s clinical history, conducted teacher interviews, performed cognitive and academic evaluations, and determined whether the child exhibited difficulties in mathematical cognition, and, if so, which aspect was most affected: number processing, arithmetical procedures, arithmetic fact retrieval, or geometrical abilities. The assessment of these children’s mathematical abilities was not solely based on standardized assessments since their previous diagnoses primarily focused on cognitive and linguistic abilities. However, for 70 out of the 75 participants (93%), mathematical abilities were also evaluated using the Woodcock–Johnson IV Test of Academic Achievement, Calculation Subtest.
The clinical evaluation process began with a comprehensive assessment of the participant’s clinical history, which carried significant weight in the overall evaluation. If parents and teachers did not report any difficulties in math learning, but the participant’s performance on a math subtest was below average, the implications of the poor performance were carefully examined. Possible attributions such as ADHD, anxiety, reading difficulties, or subthreshold math deficits were considered. Clinical impressions were formed based on a convergence of positive historical evidence of mathematical learning difficulties, teacher-reported challenges in mathematics, and either notably low performance on any math subtest (falling below the 5th percentile) or below-average scores across multiple math subtests.
From the clinical assessment, 50 out of the 75 participants with a previous diagnosis of dyslexia were classified as having difficulties in some aspect of mathematics (66.6%). Among these 50 children, 10/50 (20%) were judged to have an overall impairment in mathematics, experiencing difficulties in understanding basic concepts such as numbers and magnitudes. These children were described as struggling to process numbers correctly. For example, teachers often reported that these children had trouble connecting numbers to their corresponding magnitudes, while parents recalled instances during early learning when their child struggled with counting or understanding differences in quantities of objects. The team classified these participants as having difficulties in number processing. The majority of children who struggled in mathematics (32/50, 64%) appeared to understand numbers but still faced challenges in calculation activities. Among them, 16 children experienced difficulties primarily in mental or written calculations, while the other 16 had impairments in memorizing multiplication tables and math facts. The team classified these participants as having deficits in arithmetical procedures and arithmetic fact retrieval, respectively. Finally, 8 out of the 50 children (16%) who struggled in mathematics were described as having difficulty with mathematical activities involving orientation, direction, distance, and the processing of visuospatial information (such as reading graphs and comparing similarities and differences in figures). These children did not have trouble with calculations but struggled to understand mathematical concepts when presented visually. The team classified these participants as having visuospatial difficulties, which we identified as impairments in geometrical math abilities.
In summary, based on the clinician assessment, 25/75 children were classified as not having trouble in mathematics (33.3%). Among the 50 children with math difficulties, 10/75 were classified as having impairments in number processing (13.3%), 16 in arithmetical procedures (21.3%), 16 in arithmetic fact retrieval (21.3%), and 8 in geometrical abilities (10.7%). The UCSF Dyscalculia MCB was not used for the clinical impression evaluation.
The 75 dyslexic participants and the 18 typically developing children were tested with the UCSF MCB) to investigate whether new measures of mathematical cognition could be used to identify different mathematical deficits in this cohort of children.
On average, each participant was tested for a total of 1 hour and fifteen minutes. Performance and time were recorded for each subtest. Each child was assessed with the battery tailored to the child’s grade level. Children tested during the first three months of the scholastic year (until Christmas break) were evaluated with the battery tailored to their previous grade level to help alleviate didactical confounds. In total, 12 children were tested on the 2nd grade battery form, 6 on the 3rd grade form, 16 on the 4th grade form, 23 on the 5th grade form, 12 on the 6th grade form, 8 on the 7th grade form, and 16 on the 8th grade form.
Neuropsychological and academic assessment
Neuropsychological and academic testing were administered or supervised by a licensed neuropsychologist. The tests covered screening of nonverbal reasoning (WASI - Wechsler Abbreviated Scale of Intelligence, Matrix Reasoning111), vocabulary (ROWPVT - Receptive One-Word Picture Vocabulary Test112 and WJ-IV: Woodcock–Johnson, Oral Vocabulary113), processing speed (WISC-IV - Wechsler Intelligence Scale for Children, Symbol Search, Coding111, and CCT 1 - Color Trails Test114), attention and working memory (Digit and Spatial Spans), verbal and visual recall (CVLT - California Verbal Learning Test115 and Rey-Osterrieth Test116), visuospatial and visuo-construction abilities (Judgment of Line Orientation, Rey-Osterrieth116, and Beery VMI - Beery Visual-Motor Integration117), and executive functions (DKEFS - Delis-Kaplan Executive Function System, Design Fluency, Flanker118, and CCT 2113; please refer to Table 2 for a full list of tests). Academic testing was conducted using the Woodcock–Johnson IV113. In addition to some of the untimed reading measures in the WJ-IV, participants also underwent administration of the Test of One-Word Reading Efficiency, version 2119.
Statistical analysis
Demographic, neuropsychological, and MCB measures were compared across groups (refer to Table 1). Group differences in MCB were evaluated to potentially classify mathematical cognitive deficits in children with dyslexia.
The data were analyzed using Stata 15 (StatCorp, College Station, TX). Parametric data were analyzed using ANOVA and independent sample t tests, while non-parametric data were analyzed using chi-squared analyses. Tests for unequal variances were employed as appropriate. A Bonferroni correction was applied to account for multiple comparisons. All statistical analyses were reviewed and, if necessary, revised by a statistician. The statistical analysis of group performance in the UCSF MCB is presented along with a general description of the performance in clinically defined groups. The z scores were calculated based on the average of each group.
Reporting summary
Further information on research design is available in the Nature Research Reporting Summary linked to this article.
Data availability
The datasets generated and analyzed during the study are not publicly available because not all research on our project has been completed. The data are available from the corresponding author upon completion of the study, with protected health information excluded per HIPAA requirements, and pending any other university obligations or requirements regarding data sharing.
Code availability
No undisclosed code was used in this study.
References
Lambert, R. & Harriss, E. Insider accounts of dyslexia from research mathematicians. Educ. Stud. Math. 111, 89–107 (2022).
Butterworth, B. The mathematical brain. (Macmillan, 1999).
Dirks, E., Spyer, G., van Lieshout, E. C. D. M. & de Sonneville, L. Prevalence of combined reading and arithmetic disabilities. J. Learn Disabil. 41, 460–473 (2008).
Wilson, A. J. et al. Dyscalculia and dyslexia in adults: cognitive bases of comorbidity. Learn. Individ. Differ. 37, 118–132 (2015).
Gross-Tsur, V., Manor, O. & Shalev, R. S. Developmental dyscalculia: prevalence and demographic features. Dev. Med. Child Neurol. 38, 25–33 (1996).
Lewis, C., Hitch, G. J. & Walker, P. The prevalence of specific arithmetic difficulties and specific reading difficulties in 9- to 10-year-old boys and girls. J. Child Psychol. Psychiatry 35, 283–292 (1994).
Morsanyi, K., van Bers, B. M. C. W., McCormack, T. & McGourty, J. The prevalence of specific learning disorder in mathematics and comorbidity with other developmental disorders in primary school-age children. Br. J. Psychol. 109, 917–940 (2018).
Träff, U. & Passolunghi, M. C. Mathematical skills in children with dyslexia. Learn. Individ. Differ. 40, 108–114 (2015).
De Smedt, B. & Boets, B. Phonological processing and arithmetic fact retrieval: evidence from developmental dyslexia. Neuropsychologia 48, 3973–3981 (2010).
Bull, R., Espy, K. A. & Wiebe, S. A. Short-term memory, working memory, and executive functioning in preschoolers: longitudinal predictors of mathematical achievement at age 7 years. Dev. Neuropsychol. 33, 205–228 (2008).
Szűcs, D. Chapter 11 - Subtypes and comorbidity in mathematical learning disabilities: multidimensional study of verbal and visual memory processes is key to understanding. In: Progress in Brain Research (eds. Cappelletti, M. & Fias, W.) 227, 277–304 (Elsevier, 2016).
Wilson, A. J. & Dehaene, S. Number sense and developmental dyscalculia. In: Human behavior, learning, and the developing brain: atypical development, 212–238 (The Guilford Press, 2007).
Geary, D. C. Mathematical disabilities: Cognitive, neuropsychological, and genetic components. Psychol. Bull. 114, 345–362 (1993).
Temple, C. M. Digit dyslexia: a category-specific disorder in development dyscalculia. Cogn. Neuropsychol. 6, 93–116 (1989).
Temple, C. M. Procedural dyscalculia and number fact dyscalculia: double dissociation in developmental dyscalculia. Cogn. Neuropsychol. 8, 155–176 (1991).
von Aster, M. Developmental cognitive neuropsychology of number processing and calculation: varieties of developmental dyscalculia. Eur. Child Adolesc. Psychiatry 9, II41–II57 (2000).
Rourke, B. P. & Conway, J. A. Disabilities of arithmetic and mathematical reasoning: perspectives from neurology and neuropsychology. J. Learn Disabil. 30, 34–46 (1997).
Dehaene, S. The number sense: how the mind creates mathematics. (Oxford University Press, 1997).
Geary, D. C. & Hoard, M. K. Numerical and arithmetical deficits in learning-disabled children: relation to dyscalculia and dyslexia. Aphasiology 15, 635–647 (2001).
McCloskey, M. Cognitive mechanisms in numerical processing: evidence from acquired dyscalculia. Cognition 44, 107–157 (1992).
McCloskey, M., Caramazza, A. & Basili, A. Cognitive mechanisms in number processing and calculation: evidence from dyscalculia. Brain Cogn. 4, 171–196 (1985).
Rubinsten, O. & Henik, A. Developmental Dyscalculia: heterogeneity might not mean different mechanisms. Trends Cogn. Sci. 13, 92–99 (2009).
Von Aster, M. G. & Shalev, R. S. Number development and developmental dyscalculia. Dev. Med. Child Neurol. 49, 868–873 (2007).
Cohen, L. & Dahaene, S. Towards an anatomical and functional model of number processing. Math. Cogn. 1, 83–120 (1995).
de Hevia, M. D., Izard, V., Coubart, A., Spelke, E. S. & Streri, A. Representations of space, time, and number in neonates. Proc. Natl Acad. Sci. USA 111, 4809–4813 (2014).
Dehaene, S. Varieties of numerical abilities. Cognition 44, 1–42 (1992).
Izard, V., Sann, C., Spelke, E. S. & Streri, A. Newborn infants perceive abstract numbers. Proc. Natl Acad. Sci. USA 106, 10382–10385 (2009).
Piazza, M., Izard, V., Pinel, P., Le Bihan, D. & Dehaene, S. Tuning curves for approximate numerosity in the human intraparietal sulcus. Neuron 44, 547–555 (2004).
Piazza, M. Neurocognitive start-up tools for symbolic number representations. Trends Cogn. Sci. 14, 542–551 (2010).
Carey, S. Evidence for numerical abilities in young infants: a fatal flaw? Dev. Sci. 5, 202–205 (2002).
Feigenson, L., Dehaene, S. & Spelke, E. Core systems of number. Trends Cogn. Sci. 8, 307–314 (2004).
Hyde, D. Two systems of non-symbolic numerical cognition. Front. Hum. Neurosci. 5, 150 (2011).
Xu, F. Numerosity discrimination in infants: evidence for two systems of representations. Cognition 89, B15–B25 (2003).
Brannon, E. M. & Merritt, D. J. Chapter 14 - evolutionary foundations of the approximate number system. In: Space, Time and Number in the Brain (eds. Dehaene, S. & Brannon, E. M.) 207–224 (Academic Press, 2011). https://doi.org/10.1016/B978-0-12-385948-8.00014-1.
Anobile, G., Turi, M., Cicchini, G. M. & Burr, D. C. The effects of cross-sensory attentional demand on subitizing and on mapping number onto space. Vis. Res. 74, 102–109 (2012).
Anobile, G., Bartoli, M., Masi, G., Tacchi, A. & Tinelli, F. Math difficulties in attention deficit hyperactivity disorder do not originate from the visual number sense. Front. Hum. Neurosci. 16, 949391 (2022).
Burr, D. C., Turi, M. & Anobile, G. Subitizing but not estimation of numerosity requires attentional resources. J. Vis. 10, 20 (2010).
Piazza, M., Fumarola, A., Chinello, A. & Melcher, D. Subitizing reflects visuo-spatial object individuation capacity. Cognition 121, 147–153 (2011).
Vetter, P., Butterworth, B. & Bahrami, B. Modulating attentional load affects numerosity estimation: evidence against a pre-attentive subitizing mechanism. PLOS One 3, e3269 (2008).
Fazio, L. K., Bailey, D. H., Thompson, C. A. & Siegler, R. S. Relations of different types of numerical magnitude representations to each other and to mathematics achievement. J. Exp. Child Psychol. 123, 53–72 (2014).
Schneider, M. et al. Associations of non-symbolic and symbolic numerical magnitude processing with mathematical competence: a meta-analysis. Dev. Sci. 20, e12372 (2017).
Feigenson, L., Libertus, M. E. & Halberda, J. Links between the intuitive sense of number and formal mathematics ability. Child Dev. Perspect. 7, 74–79 (2013).
Mazzocco, M. M. M., Feigenson, L. & Halberda, J. Impaired acuity of the approximate number system underlies mathematical learning disability (dyscalculia). Child Dev. 82, 1224 (2011).
Menon, V. Arithmetic in the Child and Adult Brain. Oxf. Handb. Numer. Cogn. 1, 1–23 (2015).
Moura, R. et al. From “Five” to 5 for 5 min: arabic number transcoding as a short, specific, and sensitive screening tool for mathematics learning difficulties. Arch. Clin. Neuropsychol. 30, 88–98 (2015).
Attout, L. & Majerus, S. Working memory deficits in developmental dyscalculia: the importance of serial order. Child Neuropsychol. 21, 432–450 (2015).
Mussolin, C., Mejias, S. & Noël, M.-P. Symbolic and nonsymbolic number comparison in children with and without dyscalculia. Cognition 115, 10–25 (2010).
Landerl, K., Bevan, A. & Butterworth, B. Developmental dyscalculia and basic numerical capacities: a study of 8–9-year-old students. Cognition 93, 99–125 (2004).
Ansari, D. The foundations of numerical and mathematical abilities: a literature review. https://openknowledge.worldbank.org/handle/10986/26821 (2012).
Piazza, M. et al. Developmental trajectory of number acuity reveals a severe impairment in developmental dyscalculia. Cognition 116, 33–41 (2010).
Ganor-Stern, D. Can Dyscalculics estimate the results of arithmetic problems? J. Learn Disabil. 50, 23–33 (2017).
Jordan, N. C. & Montani, T. O. Cognitive arithmetic and problem solving: a comparison of children with specific and general mathematics difficulties. J. Learn Disabil. 30, 624–634 (1997).
Russell, R. L. & Ginsburg, H. P. Cognitive analysis of children’s mathematics difficulties. Cogn. Instr. 1, 217–244 (1984).
Pesenti, M., Seron, X. & Van Der Linden, M. Selective impairment as evidence for mental organisation of arithmetical facts: BB, a case of preserved subtraction? Cortex 30, 661–671 (1994).
De Smedt, B., Taylor, J., Archibald, L. & Ansari, D. How is phonological processing related to individual differences in children’s arithmetic skills? Dev. Sci. 13, 508–520 (2010).
Grabner, R. H. et al. To retrieve or to calculate? Left angular gyrus mediates the retrieval of arithmetic facts during problem solving. Neuropsychologia 47, 604–608 (2009).
Peters, L. & De Smedt, B. Arithmetic in the developing brain: a review of brain imaging studies. Dev. Cogn. Neurosci. 30, 265–279 (2018).
Crollen, V. Is finger-counting necessary for the development of arithmetic abilities? Front. Psychology 2, 242 (2011).
Vandervert, L. The origin of mathematics and number sense in the cerebellum: with implications for finger counting and dyscalculia. Cerebellum Ataxias 4, 12 (2017).
Rapin, I. Dyscalculia and the calculating brain. Pediatr. Neurol. 61, 11–20 (2016).
Robinson, K. M. et al. Stability and change in children’s division strategies. J. Exp. Child Psychol. 93, 224–238 (2006).
Fuson, K. C. An analysis of the counting-on solution procedure in addition. In: Addition and Subtraction (Routledge, 1982).
Geary, D. C., Bow-Thomas, C. C. & Yao, Y. Counting knowledge and skill in cognitive addition: a comparison of normal and mathematically disabled children. J. Exp. Child Psychol. 54, 372–391 (1992).
Carpenter, T. P. & Moser, J. M. The acquisition of addition and subtraction concepts in grades one through three. J. Res. Math. Educ. 15, 179–202 (1984).
De Visscher, A. & Noël, M.-P. A case study of arithmetic facts dyscalculia caused by a hypersensitivity-to-interference in memory. Cortex 49, 50–70 (2013).
Dehaene, S. & Cohen, L. Cerebral pathways for calculation: double dissociation between rote verbal and quantitative knowledge of arithmetic. Cortex 33, 219–250 (1997).
Semenza, C., Miceli, L. & Girelli, L. A deficit for arithmetical procedures: lack of knowledge or lack of monitoring? Cortex 33, 483–498 (1997).
Menon, V. & Chang, H. Emerging neurodevelopmental perspectives on mathematical learning. Dev. Rev. 60, 100964 (2021).
Rourke, B. P. Arithmetic disabilities, specific and otherwise: a neuropsychological perspective. J. Learn Disabil. 26, 214–226 (1993).
Battista, M. T. Spatial visualization and gender differences in high school geometry. J. Res. Math. Educ. 21, 47–60 (1990).
Shea, D. L., Lubinski, D. & Benbow, C. P. Importance of assessing spatial ability in intellectually talented young adolescents: a 20-year longitudinal study. J. Educ. Psychol. 93, 604–614 (2001).
Izard, V. & Spelke, E. S. Development of sensitivity to geometry in visual forms. Hum. Evol. 23, 213–248 (2009).
Epstein, R. & Kanwisher, N. A cortical representation of the local visual environment. Nature 392, 598–601 (1998).
Kanwisher, N., McDermott, J. & Chun, M. M. The fusiform face area: a module in human extrastriate cortex specialized for face perception. J. Neurosci. 17, 4302–4311 (1997).
Kravitz, D. J., Saleem, K. S., Baker, C. I. & Mishkin, M. A new neural framework for visuospatial processing. Nat. Rev. Neurosci. 12, 217–230 (2011).
Galletti, C., Fattori, P., Kutz, D. F. & Battaglini, P. P. Arm movement-related neurons in the visual area V6A of the macaque superior parietal lobule. Eur. J. Neurosci. 9, 410–413 (1997).
Kinach, B. M. Fostering spatial vs. metric understanding in geometry. Math. Teach. 105, 534–540 (2012).
Simic, N., Khan, S. & Rovet, J. Visuospatial, visuoperceptual, and visuoconstructive abilities in congenital hypothyroidism. J. Int. Neuropsychol. Soc. 19, 1119–1127 (2013).
Stern, T. A., Fava, M., Wilens, T. E. & Rosenbaum, J. F. Massachusetts general hospital comprehensive clinical psychiatry (Elsevier, 2015).
Bruce, C. D. & Hawes, Z. The role of 2D and 3D mental rotation in mathematics for young children: what is it? Why does it matter? And what can we do about it? ZDM Math. Educ. 47, 331–343 (2015).
McGraw, T. M. The effects of two-dimensional stimuli and three-dimensional stereoptic stimuli on spatial representation in drawings. Stud. Art. Educ. 45, 153–169 (2004).
Nejati, V. Effect of stimulus dimension on perception and cognition. Acta Psychol. 212, 103208 (2021).
Feifer, S. G. Feifer assessment of mathematics | FAM. (2016).
Lourenco, S. F. & Huttenlocher, J. The representation of geometric cues in infancy. Infancy 13, 103–127 (2008).
Schwartz, M. & Day, R. H. Visual shape perception in early infancy. Monogr. Soc. Res Child Dev. 44, 1–63 (1979).
Slater, A., Johnson, S. P., Kellman, P. J. & Spelke, E. S. The role of three-dimensional depth cues in infants’ perception of partly occluded objects. Early Dev. Parent. 3, 187–191 (1994).
Sherard, W. H. Why is geometry a basic skill? Math. Teach. 74, 19 (1981).
Butterworth, B. The development of arithmetical abilities. J. Child Psychol. Psychiatry 46, 3–18 (2005).
Castaldi, E., Pomè, A., Cicchini, G. M., Burr, D. & Binda, P. The pupil responds spontaneously to perceived numerosity. Nat. Commun. 12, 5944 (2021).
Castaldi, E., Turi, M., Cicchini, G. M., Gassama, S. & Eger, E. Reduced 2D form coherence and 3D structure from motion sensitivity in developmental dyscalculia. Neuropsychologia 166, 108140 (2022).
Sella, F., Sader, E. & Lolliot, S. & Cohen Kadosh, R. Basic and advanced numerical performances relate to mathematical expertise but are fully mediated by visuospatial skills. J. Exp. Psychol. Learn. Mem. Cogn. 42, 1458–1472 (2016).
Szucs, D., Devine, A., Soltesz, F., Nobes, A. & Gabriel, F. Developmental dyscalculia is related to visuo-spatial memory and inhibition impairment. Cortex 49, 2674–2688 (2013).
Berg, D. H. Working memory and arithmetic calculation in children: the contributory roles of processing speed, short-term memory, and reading. J. Exp. Child Psychol. 99, 288–308 (2008).
DeStefano, D. & LeFevre, J. The role of working memory in mental arithmetic. Eur. J. Cogn. Psychol. 16, 353–386 (2004).
Raghubar, K. et al. Errors in multi-digit arithmetic and behavioral inattention in children with math difficulties. J. Learn Disabil. 42, 356–371 (2009).
Prado, J. et al. Distinct representations of subtraction and multiplication in the neural systems for numerosity and language. Hum. Brain Mapp. 32, 1932–1947 (2011).
Balhinez, R. & Shaul, S. The relationship between reading fluency and arithmetic fact fluency and their shared cognitive skills: a developmental perspective. Front. Psychol. 10, 1281 (2019).
Singer, V. & Strasser, K. The association between arithmetic and reading performance in school: a meta-analytic study. Sch. Psychol. Q. 32, 435–448 (2017).
Qin, S. et al. Hippocampal-neocortical functional reorganization underlies children’s cognitive development. Nat. Neurosci. 17, 1263–1269 (2014).
Tosto, M. G. et al. Why do spatial abilities predict mathematical performance? Dev. Sci. 17, 462–470 (2014).
Ansari, D. Effects of development and enculturation on number representation in the brain. Nat. Rev. Neurosci. 9, 278–291 (2008).
Isaacs, E. B., Edmonds, C. J., Lucas, A. & Gadian, D. G. Calculation difficulties in children of very low birthweight: a neural correlate. Brain 124, 1701–1707 (2001).
Rosenberg-Lee, M. et al. Brain hyper-connectivity and operation-specific deficits during arithmetic problem solving in children with developmental dyscalculia. Dev. Sci. 18, 351–372 (2015).
Cho, S. et al. Hippocampal–prefrontal engagement and dynamic causal interactions in the maturation of children’s fact retrieval. J. Cogn. Neurosci. 24, 1849–1866 (2012).
De Smedt, B., Holloway, I. D. & Ansari, D. Effects of problem size and arithmetic operation on brain activation during calculation in children with varying levels of arithmetical fluency. Neuroimage 57, 771–781 (2011).
Amalric, M. & Dehaene, S. A distinct cortical network for mathematical knowledge in the human brain. NeuroImage 189, 19–31 (2019).
Haase, V. et al. Contributions from specific and general factors to unique deficits: two cases of mathematics learning difficulties. Front. Psychol. 5, 102 (2014).
Peters, L. & Ansari, D. Are specific learning disorders truly specific, and are they disorders? Trends Neurosci. Educ. 17, 100115 (2019).
Pinheiro-Chagas, P. et al. In how many ways is the approximate number system associated with exact calculation? PLoS One 9, e111155 (2014).
Dehaene, S., Izard, V., Pica, P. & Spelke, E. Core knowledge of geometry in an amazonian indigene group. Science 311, 381–384 (2006).
Wechsler, D. Wechsler Intelligence Scale for Children | 5th Edition. (Pearson, 2014).
Nancy A, M. ATP: receptive one-word picture vocabulary test-4 (ROWPVT-4). https://www.academictherapy.com/detailATP.tpl?eqskudatarq=8547-8.
Schrank, F. A., Mather, N. & McGrew, K. S. Woodcock-Johnson IV Tests of Achievement. (Riverside, 2014).
Llorente, A. M. et al. Children’s color trails test 1 & 2: test–retest reliability and factorial validity. Clin. Neuropsychol. 23, 645–660 (2009).
Delis, D. C., Kramer, J. H., Kaplan, E. & Ober, B. A. California verbal learning test-second edition (CVLT-II). (Psychological Corporation, 2000).
Meyers, J. E. & Meyers, K. R. Rey complex figure test under four different administration procedures. Clin. Neuropsychol. 9, 63–67 (1995).
Beery, K. E. The Beery-Buktenica VMI: Developmental test of visual-motor integration with supplemental developmental tests of visual perception and motor coordination: administration, scoring, and teaching manual (4th ed). (Modern Curriculum, 1997).
Korkman, M., Kirk, U. & Kemp, S. NEPSY—2nd edition (NEPSY-II). (Harcourt Assessment, 2007).
Torgesen, J. K., Wagner, R. K. & Rashotte, C. A. Test of word reading efficiency, 2nd Edition. (Pro-Ed, 2012).
Acknowledgements
This work was made possible by the Charles and Helen Schwab Foundation and K24 DC015544. The authors thank the children who participated in this study and their families for the time and effort they dedicated to this research.
Author information
Authors and Affiliations
Contributions
BP, CWP, VB, and MG contributed to the conceptualization and design of the study. BP and ME were involved in the implementation of the study. BP, CWP, VB, ME, PP, and IA analyzed the data. BP, CWP, and VB wrote parts of the manuscript. BP, CWP, VB, PP, and MG edited the first draft of the manuscript. All authors contributed to the manuscript revision and read and approved the submitted version.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Pedemonte, B., Pereira, C.W., Borghesani, V. et al. Profiles of mathematical deficits in children with dyslexia. npj Sci. Learn. 9, 7 (2024). https://doi.org/10.1038/s41539-024-00217-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41539-024-00217-x
