
Abstract
The relationship between microbiota, short chain fatty acids (SCFAs), and obesity remains enigmatic. We employ amplicon sequencing and targeted metabolomics in a large (n = 1904) African origin cohort from Ghana, South Africa, Jamaica, Seychelles, and the US. Microbiota diversity and fecal SCFAs are greatest in Ghanaians, and lowest in Americans, representing each end of the urbanization spectrum. Obesity is significantly associated with a reduction in SCFA concentration, microbial diversity, and SCFA synthesizing bacteria, with country of origin being the strongest explanatory factor. Diabetes, glucose state, hypertension, obesity, and sex can be accurately predicted from the global microbiota, but when analyzed at the level of country, predictive accuracy is only universally maintained for sex. Diabetes, glucose, and hypertension are only predictive in certain low-income countries. Our findings suggest that adiposity-related microbiota differences differ between low-to-middle-income compared to high-income countries. Further investigation is needed to determine the factors driving this association.
Similar content being viewed by others


Introduction
Obesity remains an ongoing global health epidemic that continues to worsen, affecting more than 600 million adults worldwide1, including over a third of Americans2. Importantly, comorbidities associated with obesity account for over 60% of deaths worldwide3. A major driver of obesity is the adoption of a Western lifestyle, which is characterized by excessive consumption of ultra-processed foods4,5,6. Obesity has been accompanied by dramatic increases in the prevalence of non-communicable diseases such as type two diabetes and hypertension among people of African origin5,6,7,8,9. Therefore, disrupting the rapidly expanding obesity epidemic, particularly among African-origin populations, is critical to controlling the cardiometabolic disorder epidemic10. However, successfully managing and treating obesity and its comorbidities, and specifically maintaining weight loss long-term, is particularly challenging due to an incomplete understanding of the heterogeneous and complex etiopathology, as well as additional challenges facing populations experiencing rapid urbanization10,11,12. The epidemiologic transition is a model able to capture these shifts in dietary and rural-to-urban movements and is characterized by diets that are high in ultra-processed foods with a significant loss in fiber, as evidenced in the United States, where less than 50% of the population meet dietary fiber recommendations13.
Gut microbial ecology and metabolism play pivotal roles in the onset and progression of obesity and its related metabolic disorders14. Obese and lean individuals have reported differences in the composition and functional potential of the gut microbiome, with an overall reduction in species diversity in the obese gut7,15,16,17,18,19, additionally, fecal microbiota transfer from obese donors to mouse models can recapitulate the obese phenotype20,21,22. Further, fecal microbiota transplant from healthy donors into patients with obesity and metabolic syndrome has been shown to improve markers of metabolic health in the recipients23. While these studies suggest that modification of microbial ecology may offer new options for the treatment and prevention of obesity, the mechanism that drives the microbiota-obesity relationship is not fully understood. The microbiota may facilitate greater energy exploitation from food and storage capacity by the host20,24, influencing adipose tissue composition and fat mass gain, as well as providing chronic low-grade inflammation and insulin resistance25,26.
Among the numerous microbial metabolites modulating obesity, there is an ever-growing interest in the role of short-chain fatty acids (SCFAs), which includes butyrate, acetate, and propionate as potential biomarkers for metabolic health as well as therapeutic targets. SCFAs derive primarily from microbial fermentation of non-digestible dietary fiber in the colon. They have many effects on host metabolism, including serving as an energy source for host colonocytes, used as precursors for the biosynthesis of cholesterol, lipids, and proteins, and regulating gut barrier activities27,28,29. Human and animal studies demonstrate a protective role of SCFAs in obesity and metabolic disease. In experimental animal models, SCFA supplementation reduces body weight, improves insulin sensitivity, and reduces obesity-associated inflammation30,31,32,33,34. In humans, increased gut production of butyrate correlates with improved insulin response after an oral glucose tolerance test35. Although increased SCFA levels are generally observed as positive for health36, other studies have suggested that overproduction may promote obesity, possibly resulting from greater energy accumulation37,38,39,40,41. Indeed, a previous study observed greater fecal SCFA concentrations to be linked with obesity, increased gut permeability, metabolic dysregulation, and hypertension in a human cohort42.
The conflicting obesity role of SCFAs identified by existing studies may result from the variation in the gut microbiota, which is shaped by lifestyle and diet. Adequately powered studies in well-characterized populations may permit more rigorous assessments of individual differences. Prior comparative epidemiological studies have broadly focused on either contrasting the gut microbiota of extremely different populations, such as the traditional hunter-gatherers and urban-westernized countries, or ethnically homogenous populations43,44,45,46. Demographic factors represent one of the largest contributors to the individualized nature of the gut microbiome46,47,48. The five diverse, well-characterized cohorts from the modeling of the epidemiologic transition study (METS) offer a unique opportunity to examine the issues since they are more representative of most of the world’s population. METS has longitudinally followed an international cohort of approximately 2500 African origin adults spanning the epidemiologic transition from Ghana, South Africa, Jamaica, Seychelles, and the US since 2010 to investigate differences in health outcomes utilizing the framework of the epidemiologic transition. Pioneering microbiome studies from the METS cohorts reveal that cardiometabolic risk factors, including obesity, are significantly associated with reduced microbial diversity and the enrichment of specific taxa and predicted functional traits in a geographic-specific manner7,49. While yielding valuable descriptions of the connections between the gut microbiota ecology and disease, particularly obesity, as well as pioneering the efforts of microbiome studies of populations of African origin on different stages of the ongoing nutritional epidemiologic transitions, these studies, however, have applied small sample size (N = 100 to N = 655), and also did not utilize all the countries in the METS cohort. Thus, uncertainties remain as to the precise interpretation of the microbiome-obesity associations, which hampers further progress toward diagnostic and clinical applications.
Our new study, METS-Microbiome, investigated associations between the gut microbiota composition and functional patterns, concentrations of fecal SCFAs, and obesity in a large (N = 1904) adult cohort of African origin, comprised of Ghana, South Africa, Jamaica, Seychelles, and the US spanning the epidemiologic transition50,51. The central hypothesis is that alterations to the gut microbiota and community composition will be associated with increasing stages of the epidemiologic transition, reductions in fecal SCFA levels, and higher obesity prevalence. Here, we show profound variations in gut microbiota, including significant changes in community composition, structure, and predicted functional pathways as a function of population obesity and geography. Importantly, the utility of the microbiota in predicting whether an individual is non-obese or obese differs considerably by country of origin and suggests that lifestyle traits in high-income countries may increase obesity risk even for lean individuals. Overall, our findings are important for understanding the complex relationships between the gut microbiota, population lifestyle, and the development of obesity, which may set the stage for defining the mechanisms through which the microbiome may shape health outcomes in populations of African origin.
Results
Obesity differs significantly across the epidemiological transition
From 2018 to 2019, the METS-Microbiome study recruited 2085 participants (~60% women) ages 35-55 years old from five different sites (Ghana, South Africa, Jamaica, Seychelles, and USA). Of these participants, 1249 have been followed on a yearly basis since 2010 under the parent METS study. Data from 1,867 participants with complete data sets were used in this analysis. The overall mean age was 42.5 ± 8.0 years (Table 1). Mean fasted blood glucose was 105.2 ± 39.4 mg/dL, mean systolic blood pressure was 123.4 ± 18.1 mm Hg, and mean diastolic blood pressure was 77.2 ± 13.1 mm Hg. When compared to high-income countries (Jamaica, Seychelles and USA), women and men from low- and middle-income (Ghana and South Africa) had significantly lower BMI (except South African women), fasted blood glucose, and blood pressure (systolic and diastolic). Mean BMI was lowest in South African men (22.3 kg/m2 ± 4.1) and highest in US women (36.3 kg/m2 ± 8.8). When compared to the US, all sites had a significantly lower prevalence of obesity (p < 0.001 for all sites except for Seychelles: p = 0.02). The prevalence of hypertension was lowest in Ghanaian men (33.1%) and highest in US men (72.7%). The prevalence of diabetes was lowest in South African women and men (3.5% for women and men) and highest in Seychellois men (22.8%). When compared to the US, the prevalence of hypertension and diabetes was significantly lower in countries at the lower end of the spectrum of HDI (i.e., Ghana and South Africa) when compared to the US (p < 0.001).
Microbial community composition and predicted metabolic potential differs significantly between countries and correlates with obesity
Following the removal of samples that had fewer than 6000 reads and featured less than ten reads in the entire dataset, a total of 433,364,873 16 S rRNA gene V4 region sequences were generated from the 1873 fecal samples, which were clustered into 13,254 amplicon sequence variants (ASVs). Country of origin describes most of the variation in microbial diversity and composition, with significant differences in both alpha and beta diversity. Although there were major variations in alpha diversity between countries and a large degree of inter-individual variation within countries, Ghana showed significantly greater diversity for all the alpha diversity metrics (Observed ASVs, Shannon Diversity, and Faith’s phylogenetic diversity) when compared to all other countries (Fig. 1a). Seychelles and US had the lowest alpha diversity (Fig. 1a; Kruskal–Wallis; FDR-corrected, q < 0.05). The stool microbiota alpha diversity of non-obese individuals was significantly greater when compared with that of obese individuals (Fig. 1b, Wilcoxon rank-sum; p < 0.05). Beta diversity was also significantly different between countries (Fig. 1c–f, Supplementary Table 2; weighted UniFrac distance; PERMANOVA; R2 = 0.118; p < 0.001; unweighted UniFrac distance; PERMANOVA; R2 = 0.083; p < 0.001) and obese group (weighted UniFrac distance; PERMANOVA; R2 = 0.001; p = 0.031; unweighted UniFrac distance; PERMANOVA, R2 = 0.003; p < 0.001).

a Alpha diversity estimated by Shannon, Observed ASVs and Faith’s PD (phylogenetic diversity) between countries. Exact false discovery rate (FDR)-corrected q values from left to right: Shannon: 2.33e − 08, 3.55e − 41, 2.42e − 37, 1.25e − 31, 6.70e − 20, 1.03e − 16, 3.02e − 12, 0.015, 0.1089; Observed: 0.0022, 2.84e − 26, 4.77e − 51, 7.90e − 43, 7.60e − 16, 2.06e − 40, 1.61e − 32, 3.39e − 06, 5.79e − 06, 0.058; PD: 0.067, 1.51e − 11, 3.69e − 41, 3.30e − 41, 2.59e − 05, 2.04e − 30, 5.77e − 31, 3.33e − 14, 7.86e − 15. b Alpha diversity estimated by Shannon, Observed ASVs and Faith’s PD (Phylogenetic Diversity) between obese and non-obese. Exact FDR-corrected q values from left to right: Shannon: 0.014; Observed: 1.86e − 05; PD: 6.05e − 06. Alpha diversity metrics (Faith’s PD, Observed ASVs, and Shannon) are shown on the y-axis in different panels, while country or obese groups are shown on the x-axis. c Beta diversity principal coordinate analysis based on weighted UniFrac distance between countries. d Beta diversity principal coordinate analysis based on weighted UniFrac distance between obese and non-obese. e Beta diversity principal coordinate analysis based on unweighted UniFrac distance between countries. f Beta diversity principal coordinate analysis based on unweighted UniFrac distance between obese and non-obese. The proportion of variance explained by each principal coordinate axis is denoted in the corresponding axis label. g Venn diagram of shared and unique genera between the five countries detected at a relative abundance >0.001 in more than 50% of the samples. Box plots show the interquartile range (IQR), the horizontal lines show the median values and the whiskers extend from the hinge no further than 1.5*IQR. Each colored dot denotes a sample. Statistical significance adjusted for multiple comparisons using false discovery rate (FDR) correction is indicated: *, P < 0.05; **, p < 0.01; ***, p < 0.001; ****, p < 0.0001, ns, non-significant; across countries and obese groups (Kruskal–Wallis test and pairwise Wilcoxon rank sum test; two-sided) for alpha diversity or by permutational multivariate analysis of variance (PERMANOVA) for beta diversity. Source data are provided as a Source Data file. Alpha diversity analysis for country, n = 1873 samples (Ghana, n = 373; South Africa, n = 390; Jamaica, n = 401; Seychelles, n = 396; USA, n = 313) and obesity status, n = 1764 samples. For Beta diversity analysis, n = 1764 samples.
Next, we compared fecal microbiota diversity between obese individuals with their non-obese counterparts within each country independently. Greater alpha diversity was detected in non-obese subjects in the Ghanaian (Observed ASVs, Faith PD) and South African cohorts (Observed ASVs) only (Supplementary Table 1; Wilcoxon rank-sum; p < 0.05). Similarly, significant differences in beta diversity between obese and non-obese microbiota were observed in Ghana (Unweighted UniFrac; PERMANOVA; R2 = 0.004; p < 0.05), South Africa (Unweighted UniFrac; PERMANOVA; R2 = 0.007; p < 0.05) and US (Weighted UniFrac; PERMANOVA; R2 = 0.007; p < 0.05) data sets (Supplementary Table 2). These results suggest that the beta diversity differences observed in the Ghanaian and South African participants may partly be due to the differences in rare taxa, whereas, among the US participants, the differences may be related to differences in proportional dominant microbial taxa. Collectively, these observations suggest that the country is a major driver of the variance in gut microbiota diversity and composition among participants with or without obesity, with marked contributions from Ghana and South Africa and modest contributions from the US in the overall cohort.
We also examined whether the country of origin or obesity relates to the presence of specific microbial genera frequently used to stratify humans into enterotypes52. As expected, large differences in enterotype between the countries were observed. The Prevotella enterotype (P-type) was enriched on the African continent, with 81% and 62% in Ghanaians and South Africans, respectively, while Bacteroides enterotype (B-type) was dominant in the US (75%), Jamaican cohorts (68%), and comparable proportions of both enterotypes among individuals from Seychelles (Supplementary Table 3). Further, obese individuals displayed a greater abundance of B-type, whereas a higher proportion of the P-type was associated with the non-obese group (Supplementary Table 3). Consistent with this observation, the abundance of B-type correlated with higher BMI (q = 0.004) than P-type. Significantly greater diversity and increased levels of total SCFA were observed in participants in the P-type (Supplementary Table 3). The relative abundance of shared and unique features between the different countries illustrated by the Venn diagram showed that Ghana has the largest number of unique genera, and the US has the lowest (Fig. 1g).
Microbial taxa differ significantly between countries and between lean and obese individuals
In comparison with the US, South African fecal microbiota had a significantly greater proportion of Clostridium, Olsenella, Bacilli, and Mogibacterium; Jamaican samples had a significantly greater proportion of Bacilli, Bacteroides, Clostridia, Dialister, Enterobacteriaceae, and Oscillospiraceae; Seychelles samples had a significantly greater proportion of Clostridium, Olsenella, and Haemophilus; and Ghanaian samples had a significantly greater proportion of Clostridium, Prevotella, Weisella, Enterobacteriaceae and Butyricicoccaceae. The US samples had a significantly greater proportion of Aldercreutzia, Anaerostipes, Clostridium, Eggerthella, Eisenbergiella, Ruminococcaceae, and Sellimonas compared to the four countries (Fig. 2a and Supplementary Fig. 1; ANCOM-BC; log fold change (LFC) > 1.4; q < 0.05).

a Differentially abundant taxa among countries with the US as the reference due to its status as the country with the highest HDI and highest obesity incidence (n = 1694). b Differentially abundant taxa between obese and non-obese groups in the entire cohort (n = 1694). Differentially abundant taxa between obese and non-obese groups within c Ghana (n = 329); d South Africa (n = 374); panel e Jamaica (n = 386); panel f US (n = 304). ANCOM-BC analyses adjusted for BMI, age, sex, and country. Data are presented by effect size (log fold change) with a 95% confidence interval (CI) calculated from the beta coefficient and standard errors estimated from the ANCOM-BC log-linear (natural log) model (two-sided; FDR-adjusted). The colored dot indicates effect size (log fold change), and the whiskers indicate 95% CI. Representative ASVs with log fold change >1.4 in at least one group are shown for the country. FDR-adjusted (q < 0.05) effect sizes are indicated by * q < 0.05; ** q < 0.01; *** q < 0.001. The exact p-values are available in the source data file. Source data are provided as a Source Data file. FDR false discovery rate, HDI human development index, ANCOM-BC analysis of compositions of microbiomes with bias correction.
When adjusted for country, age, and sex (ANCOM-BC; q < 0.05), 38 ASVs were significantly different between obese and non-obese groups. The obese group was characterized by an increased proportion of Allisonella, Dialister, Oribacterium, Mitsuokella, and Lachnospira, whereas non-obese microbiota had a significantly greater proportion of Alistipes, Bacteroides, Clostridium, Parabacteroides, Christensenella, Oscillospira, Ruminococcaceae (UBA1819), and Oscillospiraceae (UCG010) (Fig. 2b).
Overall, there was almost no overlap in the features discriminating obese from non-obese groups between the country-specific differential abundance analyses, except for a single Parabacteroides ASV that was differentially enriched in non-obese participants in both the Ghanaian and Jamaican cohorts (Fig. 2c, e; ANCOM-BC; q < 0.05). When comparing obese and non-obese groups in Ghana, 4 features, Colidextribacter, Butyricicoccaceae, Oscillospiraceae, and Parabacteroides were enriched in the non-obese group (Fig. 2c; ANCOM-BC; q < 0.05). The gut microbiota of the obese group in the South African cohort was enriched for 7 ASVs, including Lactobacillus, Oribacterium, and Megasphaera (Fig. 2d; ANCOM-BC; q < 0.05). In the Jamaican non-obese group, 6 ASVs were enriched including Christensenellaceae, Desulfovibrio, Eubacterium and Parabacteroides, whereas the relative proportion of Ruminococcus was greater in the obese Jamaican group (Fig. 2e; ANCOM-BC; q < 0.05). The US non-obese group was enriched for Intestinimonas and Ruminiclostridium when compared with their obese counterparts (Fig. 2f; ANCOM-BC; q < 0.05), whereas there were no significantly enriched features that discriminated obese from the non-obese group in participants from Seychelles.
Microbial taxonomic features predict obesity overall but not within each country
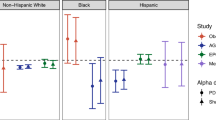
Using supervised Random Forest machine learning, the predictive capacity of the gut microbial features to stratify individuals to country of origin, sex, or metabolic phenotypes was assessed. The predictive performance of the model was calculated by area under the receiver operating characteristic curve (AUC) analysis, which showed a high accuracy for country of origin (AUC = 0.97) (Fig. 3a and Supplementary Table 4), and a comparatively lower level of predictive accuracy for the obese state (AUC = 0.65) (Fig. 3b and Supplementary Table 5). Diabetes status was predicted with AUC = 0.63 (Fig. 3c and Supplementary Table 4), glucose status with AUC = 0.66 (Fig. 3d and Supplementary Table 5), hypertensive status with AUC = 0.65 (Fig. 3e and Supplementary Table 5) and sex with AUC = 0.75 (Fig. 3f and Supplementary Table 5). Random Forest analysis was also used to identify the top 30 microbial taxonomic features that differentiate between countries and obese states. Similar to the ANCOM-BC results, Prevotella and Streptococcus were at a greater proportion in the microbiota of Ghanaian and non-obese individuals, whereas Mogibacterium was at a greater proportion in the South African cohort (Supplementary Fig. 2a, b). A greater proportion of Megasphaera was associated with the Jamaican cohort, while a greater proportion of Ruminococcaceae was observed in the American microbiota (Supplementary Fig. 2a). Weisella, which was identified as having a significantly greater proportion in the Ghanaian cohort using ANCOM-BC, was observed to be a discriminatory feature for Seychelles microbiota using Random Forest (Supplementary Fig. 2a).

Classification accuracy for estimating a all countries (n = 1694); b diabetes status (n = 1657); c glucose status (n = 1657); d hypertensive status (1694); e obesity status (n = 1694); f sex (n = 1694) are presented. Classification accuracy for estimating country-level obesity status in g Ghana (n = 329); h South Africa (n = 374); i Jamaica (n = 386); j Seychelles (n = 361); k USA (n = 304) are presented. Micro-averaging values are impacted by data imbalance since it averages across each sample, whereas Macro-averaging provides equal weight to the characterization of each sample. Macro-averaging values are reported in the text. AUC area under the curve.
Similarly, the predictive capacity of gut microbiota features in stratifying individuals by sex or metabolic phenotypes was assessed separately for each of the five study sites. The predictive performance of the model calculated by AUC analysis showed changes in accuracy for all parameters determined for all sites (Fig. 3g–k and Supplementary Tables 6–11). For example, the obese state was marginally predictive only for Ghana (AUC = 0.57), while all other countries lost accuracy (Fig. 3g–k). The predictive accuracy (Supplementary Table 6) for diabetes status was only retained for Ghana (AUC = 0.69), and Jamaica (AUC = 0.66); glucose status prediction was lost for all countries but South Africa, where it improved (AUC 0.78); and prediction of hypertension was only retained for Ghana (AUC = 0.63). The predictive ability for sex was maintained for all countries (Supplementary Table 6).
Predicted genetic metabolic potential differs by country and obesity status
The predicted potential microbial functional traits resulting from the compositional differences in microbial taxa between countries and obese states were assessed, although we acknowledge that currently available reference genome databases are likely biased toward well-studied Western populations and may have limited capacity to sufficiently characterize the gut microbiome from understudied populations43,53. Nonetheless, PICRUSt2 predicted a total of 372 MetaCyc functional pathways. ANCOM-BC analysis adjusted for sex, age, and BMI identified 67 pathways that accounted for discriminative features between the 4 different countries with the US (Supplementary Fig. 3a; ANCOM-BC; LFC > 1.4; q < 0.05). In comparison with the United States, MetaCyc pathways differentially increased in Ghana and Jamaica include methylgallate degradation, norspermidine biosynthesis (PWY-6562), gallate degradation I pathway, gallate degradation II pathway, histamine degradation (PWY-6185), toluene degradation III (via p-cresol) (PWY-5181). South African samples had a greater proportion of l-glutamate degradation VIII (to propanoate) (PWY-5088), isopropanol biosynthesis (PWY-6876), creatinine degradation (PWY-4722), adenosylcobalamin biosynthesis (anaerobic) (PWY-5507), respiration I (cytochrome c) (PWY-3781) (Supplementary Fig. 3a; ANCOM-BC; q < 0.05). MetaCyc pathways linked to norspermidine biosynthesis (PWy-6562), mycothiol biosynthesis (PWY1G-0), were at a greater proportion in the Seychelles samples, whereas reductive acetyl coenzyme A (CODH-PWY), and chorismate biosynthesis II (PWy-6165) were depleted in the US samples (Supplementary Fig. 3a, ANCOM-BC; q < 0.05). ANCOM-BC analysis adjusted for site, sex, and age identified 24 predicted pathways that differentiated between obese and non-obese individuals (Supplementary Fig. 3b; ANCOM-BC; q < 0.05). Notably, the microbiota of non-obese individuals had a greater proportion of predicted pathways, including the TCA cycle, amino acid metabolism (P162-PWY, PWY-5154, PWY-5345), ubiquinol biosynthesis-related pathways (PWY-5855, PWY-5856, PWY-5857, PWY-6708, UBISYN-PWY), cell structure biosynthesis and nucleic acid processing (PWY0 845, PYRIDOXSYN-PWY) (Supplementary Fig. 3b; ANCOM-BC; q < 0.05). On the contrary, when stratified by country, no statistically significant predicted functional pathways differentiated non-obese from obese participants within each country except in Jamaica, where only a single predicted pathway (PWY7377) involved in adenosylcobalamin biosynthesis (anaerobic) was differentially enriched in non-obese individuals (Supplementary Fig 3c, ANCOM-BC; q < 0.05).
Next, KEGG orthology (KO) involved in pathways related to butanoate (butyrate) metabolism and LPS biosynthesis were investigated. Predicted genes involved in butyrate biosynthesis pathways showed that enoyl-CoA hydratase enzymes (K01825, K01782, K01692), lysine, glutarate/succinate enzymes (K07250, K00135, K00247), glutarate/Acetyl CoA enzymes (K00175, K00174, K00242, K00241 K01040, K01039) were differentially abundant in participants from Ghana, South Africa, Jamaica, and Seychelles in comparison to the US cohort (Supplementary Fig. 4a; ANCOM-BC; q < 0.05). The relative abundance of succinic semialdehyde reductase (K18121) was significantly increased only in South Africa, Jamaica, and the Seychelles population. Further, predicted genes proportionally abundant only in specific countries were observed. For instance, succinate semialdehyde dehydrogenase (K18119) was enriched only in the Ghanaian cohort, 4-hydroxybutyrate CoA-transferase (K18122) was enriched among South African participants, and lysine/glutarate/succinate enzyme (K14268) differentially abundant within the Seychelles population (Supplementary Fig. 4a; ANCOM-BC; q < 0.05). The relative abundance of predicted genes encoding for enzymes such as maleate isomerase (K01799), 3-oxoacid CoA-transferase (K01027), and pyruvate/acetyl CoA (K00171, K00172, K00169) was greater in the US participants compared with participants from the 4 countries (Supplementary Fig. 4a; ANCOM-BC; q < 0.05). The non-obese exhibited a significantly greater abundance of genes that catalyze the production of butyrate via the fermentation of pyruvate or branched amino-acids such as enoyl-CoA hydratase enzyme (K01825), Leucine/Acetyl CoA enzyme (K01640) and pyruvate/acetyl CoA enzyme (K00171, K00172, K00169, K01907) by contrast obese individuals were differentially enriched for succinyl-CoA:acetate CoA-transferase (K18118) (Supplementary Fig. 4b; ANCOM-BC; q < 0.05). All analyses were adjusted for country, sex, BMI, and age (q < 0.05).
Exploring similar analysis at each study site, several predicted genes, including enzymes involved in the pyruvate/acetyl CoA pathway (K01907, K00023, K01640), 4−hydroxybutyrate dehydrogenase (K18120) and 4−hydroxybutyryl−CoA dehydratase (K14534) were differentially enriched in non-obese participants from Ghana (Supplementary Fig. 4c; ANCOM-BC; q < 0.05). The relative abundance of two genes both encoding pyruvate/acetyl CoA enzymes (K00171, K00169) was greater among the non-obese South African cohort (Supplementary Fig. 4d; ANCOM-BC; q < 0.05), while only a single gene encoding 4−hydroxybutyryl−CoA dehydratase (K14534) was found to be differentially abundant in non-obese individuals from Jamaica (Supplementary Fig. 4e; ANCOM-BC; q < 0.05). No statistically significant differences in the proportion of genes encoding enzymes in the butyrate synthesis pathway were observed among participants in the non-obese group compared with the obese counterparts in both Seychelles and the US.
Several gut microbial predicted genes involved in LPS biosynthesis differentially enriched among the countries were identified. In particular, the relative abundance of specific LPS genes (K02560, K12973, K02849, K12979, K12975, K12974) was significantly enriched in Ghana, South Africa, Jamaica, and Seychelles when compared with the US (Supplementary Fig. 5a; ANCOM-BC; q < 0.05). Higher proportions of LPS genes, including K12981, K12976 K09953, and K03280, were significantly increased in Seychelles samples in comparison with US samples and significantly increased in the US cohorts in comparison with participants from Ghana, South Africa, and Jamaica (Supplementary Fig. 5a, ANCOM-BC; q < 0.05). US samples had a greater proportion of the following genes (K15669, K09778, K03273, K03271) in comparison with the other 4 countries (Supplementary Fig. 5a; ANCOM-BC; q < 0.05). Obese individuals had a greater abundance of predicted genes encoding LPS biosynthesis (K02841, K02843, K03271, K03273, K19353), whereas only 1 LPS gene (K02850) differentially elevated in the non-obese group (Supplementary Fig. 5b; ANCOM-BC; q < 0.05). When analyzed separately for each country, the relative proportion of predicted genes encoding components of the LPS biosynthesis was not significantly different between non-obese and obese individuals at all 5 study sites. All analyses were adjusted for country, sex, BMI, and age.
Microbial community composition and taxonomy correlate with observed fecal SCFA concentrations
Using multiple linear regression analysis, adjusting for age and sex, all countries had significantly higher weight-adjusted fecal total SCFA levels when compared to the US participants (p < 0.001), with Ghanaians having the highest weight-adjusted fecal total SCFA levels (Supplementary Table 12). When compared to their obese counterparts, non-obese participants had significantly higher weight-adjusted fecal total and individual SCFA levels (Supplementary Table 13). Total SCFA levels displayed a weak but significantly positive correlation with Shannon diversity (Fig. 4a; Spearman r = 0.074). A similar trend was observed in the different individual SCFAs, namely acetate (Fig. 4a; Spearman r = 0.058), butyrate (Fig. 4a; Spearman r = 0.12), valerate (Fig. 4a; Spearman r = 0.19) and propionate (Fig. 4a; Spearman r = 0.073). Observed ASVs were not significantly correlated with total SCFAs (p > 0.05). Levels of acetate, butyrate, and propionate exhibited strong significant correlations with total SCFA, whereas valerate levels significantly correlated negatively (Spearman r = −0.09) with total SCFAs. Next, we assessed if levels of total SCFAs could be predicted by a mixed model. The country explained 45.7% of the variation in SCFAs. No significant effect was explained either by obesity or Shannon diversity.

a Correlations (Spearman’s rho, R; two-sided) between Shannon diversity and concentrations (n = 1704) of the different types of fecal short-chain fatty acids (SCFAs) among countries. b Country level correlations (Spearman’s rho, R; two-sided) between Shannon and valerate levels in Ghana (n = 331); South Africa (n = 362); Jamaica (n = 331); Seychelles (n = 374); US (n = 306). Each colored dot represents a sample of a specific country, and the horizontal line on the scatterplot denotes the line of best fit. Unadjusted p values are reported. Source data are provided as a Source Data file.
When stratified by country, Shannon diversity was negatively associated with acetate concentrations in Jamaica (Supplementary Table 14; Spearman r = −0.21, p < 0.001) and Seychelles (Supplementary Table 14; Spearman r = −0.11; p = 0.032), and negatively associated with propionate concentrations in Ghana (Supplementary Table 14; Spearman r = −0.14, p = 0.013) and South Africa (Supplementary Table 14; Spearman r = −0.16, p = 0.003). A negative relationship was observed between levels of total SCFA and Shannon in South Africa (Supplementary Table 14; Spearman r = −0.11, p = 0.046) and Jamaica (Supplementary Table 14; Spearman r = −0.12, p = 0.029), whereas butyrate correlated with Shannon in South Africa only (Supplementary Table 14; Spearman r = −0.14, p = 0.008). Finally, valerate levels showed significant correlations with Shannon in all countries (Fig. 4b; Spearman r = 0.12–0.41, p < 0.05).
Using the XGBoost machine learning model, the predictive capacity of SCFAs to stratify individuals to either obese or non-obese in the entire cohort was assessed. The predictive performance of the model was calculated by area under the receiver operating characteristic curve (AUC) analysis, which showed poor accuracy and similar outcomes for the different SCFAs. Total SCFA predicted an obese state with AUC = 0.55, acetate, and propionate with AUC = 0.53, butyrate with AUC = 0.52, and valerate with AUC = 0.51 (Supplementary Fig. 6). Similar analysis to determine obesity status was performed at the country-specific level and the results of the predictive performance of the model were comparable to that of the entire cohort analysis (Supplementary Fig. 6). The comparative predictive capacity for the obese state was higher in Ghana (AUC = 0.60) using valerate; higher in south Africa (AUC = 0.55) using propionate; higher in Jamaica using acetate (AUC = 0.56) and total SCFA (AUC = 0.56). The obese state predicted by butyrate was comparable among all countries (AUC = 0.51) except Ghana (AUC = 0.46). Overall, the predictive capacity of SCFAs was higher in Ghana, South Africa, and Jamaica compared with the US and Seychelles (Supplementary Fig. 6).
Based on the biological plausibility of the associations among the gut microbiota, SCFA, and obesity7,37,54, and our findings, we applied mediation analysis to evaluate whether the gut microbiota could mediate the relationship between SCFAs and obesity. Our results showed a significant direct effect (ADE) (estimate = −0.0003; p < 2e−16) and a total effect of SCFA (estimate = −0.0003; p < 2e−16) (Supplementary Table 15). However, the indirect effect (ACME) of SCFA on obesity through Shannon was not statistically significant (p > 0.05), suggesting that the effect of SCFA on obesity cannot be fully explained by the microbiota alpha diversity. When the analysis was stratified by country, the effect of SCFA on obesity diminished.
To further explore the connection between SCFAs with gut microbiota, Spearman correlations between taxa that were significantly proportionally different between countries and concentrations of SCFAs were determined. Valerate negatively correlated with the proportion of Faecalibacterium, Roseburia, and Streptococcus, which were all positively correlated with acetate, propionate, and butyrate (Fig. 5a; q < 0.05). In addition, the proportions of Christensenellaceae, and UCG 002 (Oscillospiraceae) were significantly positively associated with valerate and negatively correlated with acetate, propionate, and butyrate (Fig. 5a; q < 0.05). Similarly, Spearman’s rank correlation coefficients were calculated between the differentially abundant ASVs identified between obese and non-obese groups with concentrations of SCFAs. Broadly, the proportions of most ASVs were significantly positively associated with acetate in comparison with the other three SCFAs (Fig. 5b; q < 0.05). Consistent with the correlations mentioned above, valerate negatively correlated with most ASVs that were found to be positively correlated with the three major SCFAs, acetate, propionate, and butyrate, and vice versa. The relative proportions of ASVs belonging to Allisonella and Lachnospira positively correlated with acetate, propionate, and butyrate, whereas a significantly negative relationship was observed between Bacteroides abundances with the aforementioned SCFAs (Fig. 5b; q < 0.05). Valerate showed significantly positive associations with Oscillospirales and Ruminococcaceae abundances and significantly negative correlations with Lachnospira and Clostridium abundances (Fig. 5b; q < 0.05).

a Heatmap of Spearman’s correlation between concentrations of SCFAs and top 30 differentially abundant ASVs (identified by ANCOM-BC) among countries (n = 1694). b Heatmap of Spearman’s correlation between concentrations of SCFAs and differentially abundant ASVs (identified by ANCOM-BC) for obese (n = 1694). Heatmap of Spearman’s correlation between concentrations of SCFAs and top 30 relatively abundant features in the non-obese and obese group in c Ghana (n = 329); d South Africa (n = 374); e Jamaica (n = 386); f Seychelles (n = 361); g USA (n = 304). Correlations are identified by Spearman’s rank correlation coefficient. Brick red squares indicate positive correlation, gray squares represent negative correlation, and white squares are insignificant correlations. Exact Benjamini–Hochberg adjusted p values are shown. Source data are provided as a Source Data file.
At the country level, several genera contributed to variations in SCFAs. The genera that correlated with SCFA levels for obese and non-obese states differed at each site. For instance, acetate levels correlated negatively with the relative proportions of Anaerostipes among obese participants from Ghana and Seychelles and non-obese individuals from Jamaica (Fig. 5c–e; q < 0.05). By contrast, positive associations were observed between acetate and Cantebacterium among the non-obese US cohort and negative associations with Coproccocus within the non-obese Seychelles group (Fig. 5f, g). Butyrate levels positively correlated with 2 different ASVs assigned to the genus Subdoligranulum in all countries except the US; ASV 6915 was positively associated with non-obese individuals in Ghana, South Africa, and Jamaica, whereas ASV 7064 was positively associated with obese individuals in Jamaica and Seychelles, which could be indicative of two different species or functional niche differentiation within a taxon. Similarly, 3 Blautia ASVs positively correlated with butyrate levels in non-obese participants from Ghana (ASVs 12508, 12561), South Africa (ASVs 12508, 12561), and Jamaica (ASV 12630). Additionally, ASVs 12822 and 12561 positively correlated with butyrate levels in Jamaican participants irrespective of their obesity status (Fig. 5c–f). Propionate was found to be positively associated with Prevotella in the non-obese group from Jamaica and Ghana while positively correlated with Blautia (ASVs 12822, 12561) and Coprococcus (11,293) among obese participants from Seychelles and the US (Fig. 5c–f; q < 0.05). In the Ghanaian cohort, valerate positively correlated with Blautia, while being inversely associated with Streptococcus in the obese group in Jamaica and Seychelles and with all South African participants (Fig. 5c–e; q < 0.05). Collectively, more ASVs correlated with total SCFA among non-obese participants when compared to their obese counterparts.
Discussion
By leveraging a well-characterized large population-based cohort of African-origin adults residing in geographically distinct regions of Ghana, South Africa, Jamaica, Seychelles, and the US, we examined the relationships between gut microbiota, fecal SCFAs, and adiposity. Our data revealed profound variations in gut microbiota, including significant changes in community composition, structure, and predicted functional pathways as a function of population obesity and geography, despite their shared ancestral background. Our data further revealed an inverse relation between fecal SCFA concentrations, microbial diversity, and obesity; importantly, the utility of the microbiota in predicting whether an individual was non-obese or obese differed considerably by country of origin, being marginally better than chance only in Ghana and not predictive for all other countries. Interestingly, only sex was universally predicted at individual sites; while predictive accuracy for diabetes status was only retained for Ghana (AUC = 0.69) and Jamaica (AUC = 0.66); glucose status only in South Africa (AUC = 0.78); and hypertension was only retained for Ghana (AUC = 0.63), suggesting that predicting metabolic disease indicators from the microbiome was impacted by differences in this relationship between countries. Importantly, fecal SCFA concentrations could not predict obesity either globally or within each, which suggests that the relationship between SCFA and obesity is still unclear, and SCFA may be a poor biomarker for obesity. Overall, our findings are important for understanding the complex relationships between the gut microbiota, population lifestyle, and the development of obesity, which may set the stage for defining the mechanisms through which the microbiome may shape health outcomes in populations of African origin.
As reported previously, our data showed that geographic origin can modulate the composition of the gut microbiota. Our findings are also consistent with our previous METS studies7,49 and other large-scale continental cohort studies48,55,56,57,58,59,60,61, that report a higher bacterial diversity and composition/microbial richness in traditionally non-western groups that distinguish them from urban-industrialized individuals whose diets are low in fiber and high in saturated fats62,63. Although we observe enrichment in the relative abundance of several taxa associated with country of origin in our cohorts, we also detect a pattern where the gut microbiota of the Ghanaian and South African cohorts tend to share many features, while the gut microbiota of the Jamaican cohort shared many features with all 4 countries. It is plausible that Jamaica may be undergoing a more rapid transition than Ghana and South Africa, as reflected by their microbial communities overlapping with both Western and traditionally non-western populations. Notably, traditionally non-western associated taxa, including Prevotella, Butyrivibrio, Weisella, and Romboutsia, were enriched in participants from Ghana and South Africa, as suggested previously61. Western-associated taxa such as Bacteroides and Parabacteroides were enriched in individuals from Jamaica and the US61,64. We also found greater enrichment of VANISH taxa, including Butyricicoccus and Succinivibrio, in the Ghanaian cohort, in line with individuals practicing traditional lifestyles43. Prevotella is usually associated with plant-based diets rich in dietary fibers, while Bacteroides abundance broadly correlates with diets high in fat, animal protein, and sugars65,66, which is in agreement with our enterotype analysis where a Prevotella-rich microbiota dominates the Ghanaian and South African gut, while a Bacteroides-rich microbiota dominated in the high-income countries. As Prevotella synthesizes SCFAs67, its depletion may lead to the observed reduction in SCFA concentrations. Our results support a potential role for geography in reinforcing variations in the gut microbiota in our study cohort despite shared ethnicity. Geography may reflect subtle shifts in lifestyle and/or environmental exposures, including heterogeneity of dietary sources, exposure to medications, socioeconomic factors, medical history, and biogeographical patterns in microbial dispersion43,44,68,69.
We also inferred the metabolic capacity of the gut microbiota, which suggested that pathways that regulate processes, including energy metabolism, inflammation, epigenetic processes, and oxidative stress, were differently proportional between countries. Participants from Ghana and Jamaica were enriched for gallate degradation, which can result in phenolic catechin metabolites, which are thought to alleviate obesity-related pathologies70,71. Additionally, glutamate metabolism, which can be fermented to butyrate and propionate, was enriched in South Africans and Ghanaians compared to the US. In Seychelles, actinobacterial mycothiol biosynthesis was enriched, which is involved in antioxidant activity and the removal of toxic compounds from cells72. We further identified a depletion of SCFA synthesis pathways, e.g., acetyl coenzyme A pathway, threonine biosynthesis, and leucine degradation in the US cohort. Further studies are required to evaluate the potential causal relations of these gut microbial functions.
Preclinical mouse models provided early causal links between gut microbial ecology and obesity73,74, suggesting the potential to predict obesity risk from the microbiome. However, as we showed here, the prediction has proven difficult because the results are conflicting75. However, we identified several SCFA-producing bacteria that were significantly depleted in relative abundance among obese individuals, which may influence host energy metabolism. For example, Oscillospira and Christensenella, which were statistically associated with increased SCFA concentrations and reduced obesity, have previously been associated with a lean phenotype76,77,78,79 and produce SCFAs77,78, including butyrate, which improves insulin sensitivity and reduces inflammation80. We also detected several butyrate-producing ASVs, including Eubacterium, Alistipes, Clostridium, and Odoribacter, to be proportionally enriched in individuals who were non-obese. We observed that obese individuals presented a greater abundance of Lachnospira, which does produce SCFAs, a finding also consistent with our prior study in the same population7 and others81,82,83. However, other studies have observed the opposite84,85.
Some studies, mostly from Western populations, have reported that elevated SCFA concentrations in stool can associate with obesity37,42,54,86. For example, a Colombian cohort showed associations between elevated fecal SCFA levels, central obesity, gut permeability, and hypertension42. One potential explanation is that obese gut microbiota may lead to less efficient SCFA absorption, hence the increased SCFA excretion42. However, we found diets high in fiber correlate positively with weight loss87,88 and increased levels of fecal SCFAs89. One explanation may be differences in lifestyle factors, including medication, activity, and pollutant exposure, which could also impact intestinal absorption in Western countries. We note that fecal SCFA concentrations are not a direct measure of intestinal SCFA production but rather reflect a net result of the difference between production and absorption90. Studies using stable isotopes to measure SCFA dynamics would improve the interpretation of this dichotomy.
Our study, due to the size and diversity of the cohort, provides robust evidence to suggest that fecal SCFA concentrations are not predictive of obesity status and that fecal SCFA may function as a poor biomarker for obesity. Previous studies have suggested that measures of both circulating and fecal SCFAs could be more accurate prognostic markers of obesity status35,42,91,92, a hypothesis that remains to be fully elucidated in our study cohort. Additionally, controlled human intervention studies, including the quantitation of whole-body turnover rates of SCFAs40, are needed to ascertain the potential health benefits before clinical translation can be implemented to improve metabolic health. Broadly, our findings prompt caution in relying on fecal microbial metabolites alone to infer obesity outcomes since obesity is a heterogenous construct with several unique mechanisms involving host-related factors such as genetic predisposition and microbial SCFAs in precipitating disease susceptibility.
Another mechanism underpinning obesity is metabolic endotoxemia. An increase in Proteobacteria, which often accompanies a high fat/high sugar diet, is often associated with an increase in circulating lipopolysaccharide (LPS) and H2S, which provoke low-grade inflammation, increased intestinal permeability and clock gene disruption in the liver, which associate with adiposity93,94,95. We identified an increase in the LPS producer, Dialister96,97, and LPS-associated pathways in obese individuals, which have previously been associated with obesity98, sleep disruption, and chronic inflammation99,100,101,102,103. We posit that LPS production may result in a systemic inflammatory state favoring the development of obesity in concordance with the associated metabolic endotoxemia pathway linking gut bacteria to obesity.
In obese individuals, as well as SCFA metabolism, we also detected marked depletion in pathways involved in cell structure, vitamin B6, nicotinamide adenine dinucleotide, and amino acid biosynthesis. This suggests that pathways important for growth and energy homeostasis are disrupted in individuals with obesity. We also noted an enrichment of the formaldehyde assimilation I (serine pathway) pathway. A study reported increases in the abundance of formaldehyde assimilation pathway in a depressed group when compared with non-depressed controls104. Although we do not yet understand the mechanistic details, it is known that toxic formaldehyde is generated along with reactive oxygen species during inflammatory processes105. Thus, an increased capacity for formaldehyde pathway may indicate a microbiome-induced increase in reactive oxygen species in the gut of obese individuals. Indeed, prior work has identified the induction of oxygen stress by microbial perturbations as one of the mechanisms by which the microbiome can promote weight gain and insulin resistance106. The specific alterations of the gut microbiota and the associated predicted functionality may constitute a potential avenue for the development of microbiome-based therapeutics to treat obesity and/or to promote and sustain weight loss.
While our study has several strengths, including a large sample size, a diverse population along an epidemiological transition gradient with a comprehensive dataset that allowed the exclusion of the potential effects of origin as well as control of potential interpersonal covariates, and the use of validated and standard tools for data collection, we acknowledge some limitations as well. First, the cross-sectional nature of our study design is unable to establish temporality or identify mechanisms by which the gut microbiome may causally influence the observed associations. In that regard, we expect that prospective data from the METS cohort study will provide the basis to assess the longitudinal association between gut microbiota composition, metabolites, and obesity, and we have an ongoing study exploring the potential correlations longitudinally. We had no information on diet and physical activity, lifestyle factors that are well-recognized to have profound influences on the gut microbiota. The use of 16 S rRNA sequencing in our analysis for inferences on microbial functional ecology inherently has its limitations for drawing conclusions on species and strain level functionality due to its low resolution. Finally, here we report the associations between the gut microbiota and fecal SCFA concentrations, which may not reflect circulating SCFA concentration levels. Nevertheless, our results provide insight into the relationship between obesity, gut microbiota, and metabolic pathways in individuals of African origin across different geographies, stimulating further examination of large-scale studies using multi-omic approaches with deeper taxonomic and functional resolution and animal transplantation studies to investigate potentially novel microbial strains and to explore the clinical relevance of the observed metabolic differences.
Methods
Study cohort
Since 2010, METS and the currently funded METS-Microbiome study have longitudinally followed an international cohort of African origin adults (based on self-report) spanning the epidemiologic transition from Ghana, South Africa, Jamaica, Seychelles, and the US50,51. The site in Ghana was based at Nkwantakese, a rural village of approximately 20,000 inhabitants and about 25 km outside of Kumasi. The site in South Africa was in Khayelitsha, an urban informal settlement near Cape Town with over 400,000 inhabitants. The participants from Jamaica were from Spanish Town, an urban area 25 km from the center of Kingston. The Seychelles site was based at Mahé, the largest and most populated of the 100 islands forming the Republic of Seychelles, located approximately 1500 km east of Kenya in the Indian Ocean and home to approximately 81,000 inhabitants. Participants in the US were recruited in Maywood, IL, a suburb adjacent to the western border of Chicago and home to approximately 24,000 people. METS utilizes the framework of the epidemiologic transition to investigate differences in health outcomes based on country of origin. The epidemiologic transition is defined using the United Nations Human Development Index (HDI) as an approximation of the epidemiologic transition. Ghana represents a lower-middle-income country, South Africa represents a middle-income country, Jamaica and Seychelles represent high-income countries, and the US represents a very high-income country. This framework has allowed us to understand how increasing global Westernization, resulting in greater consumption of ultra-processed foods, is associated with a higher prevalence of obesity, type 2 diabetes, and cardiometabolic diseases. Our data from the original METS cohort demonstrate that the epidemiologic transition has altered habitual diets in the international METS sites and that reduced fiber intake is associated with higher metabolic risk, inflammation, and obesity across the epidemiologic transition107. Originally, 2,506 African-origin adults (25–45 yrs) were enrolled in METS between January 2010 and December 2011 and followed on a yearly basis. In 2018, METS participants were recontacted and invited to participate in METS-Microbiome (NCT03378765). Participants were excluded from participating in the original METS study if they self-reported being persons with an infectious disease, including HIV, being pregnant, breastfeeding, using antibiotics within 3 months, or having any condition which prevented the individual from participating in normal physical activities. METS-Microbiome was approved by the Institutional Review Board of Loyola University Chicago, IL, US; the Committee on Human Research Publication and Ethics of Kwame Nkrumah University of Science and Technology, Kumasi, Ghana; the Research Ethics Committee of the University of Cape Town, South Africa; the Board for Ethics and Clinical Research of the University of Lausanne, Switzerland; and the Ethics Committee of the University of the West Indies, Kingston, Jamaica. All study procedures were explained to participants in their native languages, and participants were provided written informed consent after being given the opportunity to ask any questions and compensated for their participation.
Anthropometry, sociodemographic, and biochemical measurements
Participants completed the research visits at the established METS research clinics located in the respective communities51. Briefly, they presented themselves at the site-specific research clinic early in the morning, following an overnight fast. The weight of the participant was measured without shoes and dressed in light clothing to the nearest 0.1 kg using a standard digital scale (Seca, SC, USA). Height was measured using a stadiometer without shoes and head held in the Frankfort plane to the nearest 0.1 cm. Waist circumference was measured to the nearest 0.1 cm at the umbilicus, while hip circumference was measured to the nearest 0.1 cm at the point of maximum extension of the buttocks. Adiposity (% body fat) was assessed using bioelectrical impedence analysis (Quantum, RJL Systems, Clinton Township, MI) and study-specific equations51. Blood pressure was measured using the standard METS protocol using the Omron Automatic Digital Blood Pressure Monitor (model HEM-747Ic, Omron Healthcare, Bannockburn, IL, USA), with the antecubital fossa at heart level. Metabolic disease risks were assessed as follows: hypertension was defined as mean systolic/diastolic blood pressure ≥ 130/80 mm Hg or on current treatment; diabetes was defined as >125 mg/dL or current treatment for all sites, except for Ghana as not all participants were fasted overnight. For the Ghanaian site, diabetes was defined as ≥140 mg/dL or current treatment according to American Diabetes Association guidelines for random glucose testing. Obesity was defined as ≥30 kg/m2. Participants were encouraged to provide stool samples in a clinic or just prior to clinic visits using a standard collection kit (EasySampler stool collection kit, Alpco, NH). In cases where this was not possible, participants stored stool samples in home freezers or coolers for 1–3 days prior to clinic visits. Fecal samples were placed within a −80° freezer immediately upon receipt at all the sites. Participants were requested to fast from 8 pm in the evening prior to the clinic examination, during which fasting capillary glucose concentrations were determined using a finger stick (Accu-check Aviva, Roche).
Fecal short-chain fatty acid quantification
As in our previous studies7,108,109,110,111,112, fecal SCFAs were measured using LC–MS/MS at the University of Illinois-Chicago Mass Spectrometry Core using previously published methods113,114. The LC–MS/MS analysis was completed on an AB Sciex Qtrap 5500 coupled to the Agilent UPLC/HPLC system. All samples were analyzed by Agilent poroshell 120 EC-C18 Column, 100 Å, 2.7 µm, 2.1 mm × 100 mm coupled to an Agilent UPLC system, which was operated at a flow rate of 400 µl/min. A gradient of buffer A (H20, 0.1% Formic acid) and buffer B (Acetonitrile, 0.1% Formic acid) was applied as 0 min, 30% of buffer B; increase buffer B to 100% in 4 min; maintain B at 100% for 5 min. The column was then equilibrated for 3 min at 30% B between the injections with the MS detection in negative mode. The MRM transitions of all targeted compounds include the precursor ions and the signature production ion. Unit resolution is used for both analyzers Q1 and Q3. The MS parameters, such as declustering potential, collision energy, and collision cell exit potential, are optimized in order to achieve optimal sensitivity. SCFAs are presented as individual SCFAs (μg/g), including butyric acid, propionic acid, acetic acid, and valeric acid, as well as total SCFAs (sum of 4).
DNA extraction and amplicon sequencing
Fecal samples were shipped on dry ice to the microbiome core sequencing facility, University of California, San Diego, for 16 S rRNA gene processing. Fecal samples were randomly sorted and transferred to 96‐well extraction plates, and DNA was extracted using the MagAttract Power Microbiome kit. Blank controls and ZymoBIOMICS mock controls (Cat. No. D6300) were included per extraction plate, which was carried through all downstream processing steps. Extracted DNA was used for amplification of the V4 region of the 16 S rRNA gene with 515F-806R region-specific primers (515 F: 5′GTGYCAGCMGCCGCGGTAA3′; 806 R: 5′GGACTACNVGGGTWTCTAAT3′) according to the Earth Microbiome Project115,116. No human DNA sequence depletion or enrichment of microbial or viral DNA was performed. Purified amplicon libraries were sequenced on the Illumina NovaSeq platform to produce 150 bp forward and reverse reads through the IGM Genomics Center at the University of California San Diego.
Bioinformatic analysis
The generated raw sequence data were uploaded and processed in Qiita117 (Qiita ID 13512), an open-source, web-enabled microbiome analysis platform. Sequences were demultiplexed, quality filtered, trimmed, erroneous sequences were removed, and ASVs were defined using Deblur118. The deblur ASV table was exported to Qiime2119,120, and representative sequences of the ASVs were inserted into the Greengenes 13.8 99% identity tree with SATé-enabled phylogenetic placement (SEPP) using q2-fragment-insertion119,121 to generate an insertion tree for diversity computation. Additionally, the deblur ASV table was assigned taxonomic classification using the Qiime2 feature classifier, with Naive Bayes classifiers trained on the SILVA database (version 138;122). A total of 463,258,036 reads, 154,952 ASVs, and 1902 samples were obtained from the deblur table. The resulting ASV count table, taxonomy data, insertion tree, and sample metadata were exported and merged into a phyloseq123 object in R (R Foundation for Statistical Computing, Vienna, Austria) for downstream analysis. Features with less than ten read in the entire dataset, and samples with fewer than 6000 reads were removed from the phyloseq object. In addition, mitochondrial and chloroplast-derived sequences, non-bacterial sequences, as well as ASVs that were unassigned at the phylum level were filtered prior to analyses. There were 433,364,873 reads and 13254 ASVs in the remaining 1873 fecal samples in the phyloseq object. The remaining samples, after filtering, were rarefied to a depth of 6000 reads to avoid sequencing bias before generating diversity measures, leaving 9917 ASVs across 1873 samples.
Diversity and differential proportional analyses
Alpha diversity measures based on Observed ASVs, Faith’s Phylogenetic Diversity, and Shannon Index were conducted on rarified samples using phyloseq v 1.38.0123 and picante v1.8.2124 libraries. Beta diversity was determined using both weighted and unweighted UniFrac distance matrices125, generated in phyloseq v 1.38.0. The Bacteroides Prevotella ratio was calculated by dividing the abundance of the genera Bacteroides by Prevotella. Participants were classified into Bacteroides enterotype (B-type) if the ratio was greater than 1. Otherwise, Prevotella enterotype (P-type). For differential abundance analysis, samples were processed to remove exceptionally rare taxa. First, the non-rarefied reads were filtered to remove samples with <10,000 reads. Next, ASVs with fewer than 50 reads in total across all samples and/or were present in less than 2% of samples were excluded. This retained 2061 ASVs across 1694 samples. The retained ASVs were binned at the genus level and subsequently used in the analysis of compositions of microbiomes with bias correction (ANCOM-BC v1.2.2)126 to determine specific taxa differentially abundant across sites or obese phenotype. ANCOM-BC is a statistical approach that accounts for sampling fraction and normalizes the read counts by a process identical to log-ratio transformations while controlling for false discovery rates and increasing power. The site, age, sex, and BMI were added as covariates in the ANCOM-BC formula to reduce the effect of confounders.
Machine learning
Random Forest supervised learning models implemented in Qiime2 was used to estimate the predictive power of microbial community profiles for the site and obese phenotype. The classifications were done with 500 trees based on 10-fold cross-validation using the QIIME “sample-classifier classify-samples” plugin120. A randomly drawn 80% of samples were used for model training, whereas the remaining 20% were used for validation. Further, the 30 most important ASVs for differentiating between site or obese phenotype were predicted and annotated. The predictive capacity of SCFAs to stratify individuals by country or either obese or non-obese was done using XGBoost v.1.7.5.1 machine learning model R package with parameters set at 10-fold CV and 100 repetitions.
Mediation analysis
The mediation package (v4.5.0) in R (v4.3.0) was used to infer causal relationships between gut microbial diversity, SCFAs, and obesity. The mediation analysis was performed with the same parameter settings (boot = “TRUE,” boot.ci.type = “perc”, conf.level = 0.95, sims = 1000). The total effect was obtained through the sum of a direct effect and a mediated (indirect) effect.
Predicted metabolic gene pathway analysis
The functional potential of microbial communities was inferred using the Phylogenetic Investigation of Communities by Reconstruction of Unobserved States 2 (PICRUSt2) v2.5.1 with the ASV table processed to remove exceptionally rare taxa and the representative sequences as input files127. The metabolic pathway from the PICRUSt2 pipeline was annotated using the MetaCyc database128. The predicted MetaCyc abundances (unstratified pathway abundances) were analyzed with ANCOM-BC to determine differentially abundant pathway associations across sites and obese status. The site, age, sex, and BMI were added as covariates in the ANCOM-BC formula to reduce the effect of confounders.
Statistical analysis
All statistical analyses and graphs were done with R v4.1.1 and Stata v5. Descriptive statistics for continuous variables are presented as mean ± standard deviation of the mean if normally distributed or as median (interquartile range) if non-normally distributed; categorical variables are shown as counts and percentages. P values were two-sided. Kruskal–Wallis test and Permutational Analysis of Variance (PERMANOVA) tests with 999 permutations using the Adonis function in the vegan package v 2.6.2129 were performed to compare alpha and beta diversity measures, respectively, with multiple groups comparison correction. PERMANOVA models were adjusted for BMI, age, and sex for the country, whereas age, sex, and country were accounted for in obese groups. For variables that showed significant differences in the PERMANOVA analyses, the PERMDISP test was performed to assess differences in dispersion or centroids. For differential abundance analysis, the false-discovery rate (FDR) method incorporated in the ANCOM-BC library was used to correct p-values for multiple testing. A cut-off of q < 0.05 was used to assess significance. Spearman correlations were performed between concentrations of short-chain fatty acids, Shannon diversity or concentrations of short-chain fatty acids, and differentially abundant taxa that were identified either among study sites or in obese and non-obese individuals. The resulting p-values were adjusted for multiple testing using the Benjamini–Hochberg FDR. A mixed model was built using lme4 package vk1-31 to assess whether total SCFAs could be predicted by Shannon diversity, obesity, and country, setting obesity and Shannon diversity as fixed effects and random intercept by country. Statistical analysis and data visualization performed in R version 4.1.1 used the following freely available packages: ANCOMBC v1.2.2, ggplot2 v 3.3.6, vegan v 2.6.2, phyloseq v 1.38.0, microbiome v 1.19.1, microbiomeutilities v 1.00.16, gghalves v 0.1.3, qiime2R v0.99.6, tidyverse v1.3.1, reshape v0.8.8, microViz v 0.9.4, cowplot v1.1.1, picante v1.8.2, reshape v 0.8.8, lme4 v1.1-31, RColorBrewer v1.1-3, gtable v 0.3, mediation v4.5.0, xGBoost v1.7.5.1, Biostrings v2.62.0, biomformat v1.22.0, rstatix 0.7.0, patchwork 1.1.1, readr v2.1.2. PICRUSt2 v2.5.1 was installed in Python v 3.7.4.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
All 16 S rRNA gene sequence data have been deposited at the European Bioinformatics Institute site under the accession code (https://www.ebi.ac.uk/ena/browser/view/PRJEB63378). Additionally, sequencing data and processed tables are available through QIITA117 under study identifier 13512. The SILVA 16 S rRNA database used for alignment is available at https://data.qiime2.org/2022.2/common/silva-138-99-515-806-nb-classifier.qza. The KEGG and MetaCyc Databases are available at https://www.genome.jp/kegg/ and https://metacyc.org/, respectively. The clinical and metadata are available under restricted access due to privacy regulations of our cohort, access can be obtained by request to the corresponding author (Lara Dugas: ldugas@luc.edu). The data and analyses generated in this study are available within the paper, Supplementary Information and Source Data files provided with this paper. Source data are provided in this paper.
Code availability
The R codes used for analysis and figure generation are available at https://doi.org/10.6084/m9.figshare.23542395.v1.
References
Obesity and overweight. https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight.
Hales, C. M., Carroll, M. D., Fryar, C. D. & Ogden, C. L. Prevalence of obesity and severe obesity among adults: United States, 2017-2018. NCHS Data Brief 360 1–8 (2020).
Tseng, C.-H. & Wu, C.-Y. The gut microbiome in obesity. J. Formos. Med. Assoc. 118, S3–S9 (2019).
Ecklu-Mensah, G., Gilbert, J. & Devkota, S. Dietary selection pressures and their impact on the gut microbiome. Cell Mol. Gastroenterol. Hepatol. 13, 7–18 (2022).
Abdelaal, M., le Roux, C. W. & Docherty, N. G. Morbidity and mortality associated with obesity. Ann. Transl. Med. 5, 161 (2017).
Ajala, O., Mold, F., Boughton, C., Cooke, D. & Whyte, M. Childhood predictors of cardiovascular disease in adulthood. A systematic review and meta-analysis. Obes. Rev. 18, 1061–1070 (2017).
Dugas, L. R. et al. Decreased microbial co-occurrence network stability and SCFA receptor level correlates with obesity in African-origin women. Sci. Rep. 8, 17135 (2018).
Gouda, H. N. et al. Burden of non-communicable diseases in sub-Saharan Africa, 1990-2017: results from the Global Burden of Disease Study 2017. Lancet Glob. Health 7, e1375–e1387 (2019).
Roth, G. A. et al. Global burden of cardiovascular diseases and risk factors, 1990-2019: update from the GBD 2019 study. J. Am. Coll. Cardiol. 76, 2982–3021 (2020).
Geng, J., Ni, Q., Sun, W., Li, L. & Feng, X. The links between gut microbiota and obesity and obesity related diseases. Biomed. Pharmacother. 147, 112678 (2022).
Nordmo, M., Danielsen, Y. S. & Nordmo, M. The challenge of keeping it off, a descriptive systematic review of high-quality, follow-up studies of obesity treatments. Obes. Rev. 21, e12949 (2020).
Barone, M. et al. Multi-omics gut microbiome signatures in obese women: role of diet and uncontrolled eating behavior. BMC Med. 20, 500 (2022).
Dahl, W. J. & Stewart, M. L. Position of the academy of nutrition and dietetics: health implications of dietary fiber. J. Acad. Nutr. Diet. 115, 1861–1870 (2015).
Ley, R. E. Obesity and the human microbiome. Curr. Opin. Gastroenterol. 26, 5–11 (2010).
Greenblum, S., Turnbaugh, P. J. & Borenstein, E. Metagenomic systems biology of the human gut microbiome reveals topological shifts associated with obesity and inflammatory bowel disease. Proc. Natl Acad. Sci. USA 109, 594–599 (2012).
Jumpertz, R. et al. Energy-balance studies reveal associations between gut microbes, caloric load, and nutrient absorption in humans. Am. J. Clin. Nutr. 94, 58–65 (2011).
Ley, R. E., Turnbaugh, P. J., Klein, S. & Gordon, J. I. Microbial ecology: human gut microbes associated with obesity. Nature 444, 1022–1023 (2006).
Turnbaugh, P. J. et al. A core gut microbiome in obese and lean twins. Nature 457, 480–484 (2009).
Le Chatelier, E. et al. Richness of human gut microbiome correlates with metabolic markers. Nature 500, 541–546 (2013).
Turnbaugh, P. J. et al. An obesity-associated gut microbiome with increased capacity for energy harvest. Nature 444, 1027–1031 (2006).
Turnbaugh, P. J., Bäckhed, F., Fulton, L. & Gordon, J. I. Diet-induced obesity is linked to marked but reversible alterations in the mouse distal gut microbiome. Cell Host Microbe 3, 213–223 (2008).
Ridaura, V. K. et al. Gut microbiota from twins discordant for obesity modulate metabolism in mice. Science 341, 1241214 (2013).
Vrieze, A. et al. Transfer of intestinal microbiota from lean donors increases insulin sensitivity in individuals with metabolic syndrome. Gastroenterology 143, 913–6.e7 (2012).
DiBaise, J. K. et al. Gut microbiota and its possible relationship with obesity. Mayo Clin. Proc. 83, 460–469 (2008).
Cani, P. D. & Delzenne, N. M. Interplay between obesity and associated metabolic disorders: new insights into the gut microbiota. Curr. Opin. Pharmacol. 9, 737–743 (2009).
Sonnenburg, J. L. & Bäckhed, F. Diet-microbiota interactions as moderators of human metabolism. Nature 535, 56–64 (2016).
Dalile, B., Van Oudenhove, L., Vervliet, B. & Verbeke, K. The role of short-chain fatty acids in microbiota-gut-brain communication. Nat. Rev. Gastroenterol. Hepatol. 16, 461–478 (2019).
Koh, A., De Vadder, F., Kovatcheva-Datchary, P. & Bäckhed, F. From dietary fiber to host physiology: short-chain fatty acids as key bacterial metabolites. Cell 165, 1332–1345 (2016).
van der Hee, B. & Wells, J. M. Microbial regulation of host physiology by short-chain fatty acids. Trends Microbiol. 29, 700–712 (2021).
Vinolo, M. A. R., Rodrigues, H. G., Nachbar, R. T. & Curi, R. Regulation of inflammation by short chain fatty acids. Nutrients 3, 858–876 (2011).
Gao, Z. et al. Butyrate improves insulin sensitivity and increases energy expenditure in mice. Diabetes 58, 1509–1517 (2009).
Henagan, T. M. et al. Sodium butyrate epigenetically modulates high-fat diet-induced skeletal muscle mitochondrial adaptation, obesity and insulin resistance through nucleosome positioning. Br. J. Pharmacol. 172, 2782–2798 (2015).
Lu, Y. et al. Short chain fatty acids prevent high-fat-diet-induced obesity in mice by regulating G protein-coupled receptors and gut microbiota. Sci. Rep. 6, 37589 (2016).
Bonomo, R. R. et al. Fecal transplantation and butyrate improve neuropathic pain, modify immune cell profile, and gene expression in the PNS of obese mice. Proc. Natl Acad. Sci. USA 117, 26482–26493 (2020).
Sanna, S. et al. Causal relationships among the gut microbiome, short-chain fatty acids and metabolic diseases. Nat. Genet. 51, 600–605 (2019).
Valdes, A. M., Walter, J., Segal, E. & Spector, T. D. Role of the gut microbiota in nutrition and health. Br. Med. J. 361, k2179 (2018).
Schwiertz, A. et al. Microbiota and SCFA in lean and overweight healthy subjects. Obesity 18, 190–195 (2010).
Rahat-Rozenbloom, S., Fernandes, J., Gloor, G. B. & Wolever, T. M. S. Evidence for greater production of colonic short-chain fatty acids in overweight than lean humans. Int. J. Obes. 38, 1525–1531 (2014).
Teixeira, T. F. S. et al. Higher level of faecal SCFA in women correlates with metabolic syndrome risk factors. Br. J. Nutr. 109, 914–919 (2013).
Perry, R. J. et al. Acetate mediates a microbiome–brain–β-cell axis to promote metabolic syndrome. Nature 534, 213–217 (2016).
Tirosh, A. et al. The short-chain fatty acid propionate increases glucagon and FABP4 production, impairing insulin action in mice and humans. Sci. Transl. Med. 11, eaav0120 (2019).
de la Cuesta-Zuluaga, J. et al. Higher fecal short-chain fatty acid levels are associated with gut microbiome dysbiosis, obesity, hypertension and cardiometabolic disease risk factors. Nutrients 11, 51 (2018).
Pasolli, E. et al. Extensive unexplored human microbiome diversity revealed by over 150,000 genomes from metagenomes spanning age, geography, and lifestyle. Cell 176, 649–662.e20 (2019).
He, Y. et al. Regional variation limits applications of healthy gut microbiome reference ranges and disease models. Nat. Med. 24, 1532–1535 (2018).
Peters, B. A. et al. A taxonomic signature of obesity in a large study of American adults. Sci. Rep. 8, 9749 (2018).
Zhernakova, A. et al. Population-based metagenomics analysis reveals markers for gut microbiome composition and diversity. Science 352, 565–569 (2016).
Falony, G. et al. Population-level analysis of gut microbiome variation. Science 352, 560–564 (2016).
Yatsunenko, T. et al. Human gut microbiome viewed across age and geography. Nature 486, 222–227 (2012).
Fei, N. et al. The human microbiota is associated with cardiometabolic risk across the epidemiologic transition. PLoS ONE 14, e0215262 (2019).
Dugas, L. R. et al. Gut microbiota, short chain fatty acids, and obesity across the epidemiologic transition: the METS-Microbiome study protocol. BMC Public Health 18, 978 (2018).
Luke, A. et al. Protocol for the modeling the epidemiologic transition study: a longitudinal observational study of energy balance and change in body weight, diabetes and cardiovascular disease risk. BMC Public Health 11, 927 (2011).
Arumugam, M. et al. Enterotypes of the human gut microbiome. Nature 473, 174–180 (2011).
Tamburini, F. B. et al. Short- and long-read metagenomics of urban and rural South African gut microbiomes reveal a transitional composition and undescribed taxa. Nat. Commun. 13, 1–18 (2022).
Riva, A. et al. Pediatric obesity is associated with an altered gut microbiota and discordant shifts in Firmicutes populations. Environ. Microbiol. 19, 95–105 (2017).
De Filippo, C. et al. Impact of diet in shaping gut microbiota revealed by a comparative study in children from Europe and rural Africa. Proc. Natl Acad. Sci. USA 107, 14691–14696 (2010).
De Filippo, C. et al. Diet, environments, and gut microbiota. A preliminary investigation in children living in rural and urban Burkina Faso and Italy. Front. Microbiol. 8, 1979 (2017).
Schnorr, S. L. et al. Gut microbiome of the Hadza hunter-gatherers. Nat. Commun. 5, 3654 (2014).
Clemente, J. C. et al. The microbiome of uncontacted Amerindians. Sci. Adv. 1, e1500183 (2015).
Rampelli, S. et al. Metagenome sequencing of the Hadza hunter-gatherer gut microbiota. Curr. Biol. 25, 1682–1693 (2015).
Gomez, A. et al. Gut microbiome of coexisting BaAka Pygmies and Bantu reflects gradients of traditional subsistence patterns. Cell Rep. 14, 2142–2153 (2016).
Mancabelli, L. et al. Meta-analysis of the human gut microbiome from urbanized and pre-agricultural populations. Environ. Microbiol. 19, 1379–1390 (2017).
Sonnenburg, E. D. & Sonnenburg, J. L. The ancestral and industrialized gut microbiota and implications for human health. Nat. Rev. Microbiol. 17, 383–390 (2019).
Kolodziejczyk, A. A., Zheng, D. & Elinav, E. Diet-microbiota interactions and personalized nutrition. Nat. Rev. Microbiol. 17, 742–753 (2019).
Kao, C. C. et al. The microbiome, intestinal function, and arginine metabolism of healthy indian women are different from those of American and Jamaican women. J. Nutr. 146, 706–713 (2015).
Gupta, V. K., Paul, S. & Dutta, C. Geography, ethnicity or subsistence-specific variations in human microbiome composition and diversity. Front. Microbiol. 8, 1162 (2017).
Wu, G. D. et al. Linking long-term dietary patterns with gut microbial enterotypes. Science 334, 105–108 (2011).
Chen, T. et al. Fiber-utilizing capacity varies in Prevotella- versus Bacteroides-dominated gut microbiota. Sci. Rep. 7, 2594 (2017).
Asnicar, F. et al. Microbiome connections with host metabolism and habitual diet from 1,098 deeply phenotyped individuals. Nat. Med. 27, 321–332 (2021).
Costello, E. K., Stagaman, K., Dethlefsen, L., Bohannan, B. J. M. & Relman, D. A. The application of ecological theory toward an understanding of the human microbiome. Science 336, 1255–1262 (2012).
Marchesi, J. R. et al. The gut microbiota and host health: a new clinical frontier. Gut 65, 330–339 (2016).
Liu, X., Zhao, K., Jing, N., Kong, Q. & Yang, X. Epigallocatechin gallate (EGCG) promotes the immune function of ileum in high fat diet fed mice by regulating gut microbiome profiling and immunoglobulin production. Front. Nutr. 8, 720439 (2021).
Newton, G. L., Buchmeier, N. & Fahey, R. C. Biosynthesis and functions of mycothiol, the unique protective thiol of Actinobacteria. Microbiol. Mol. Biol. Rev. 72, 471–494 (2008).
Ley, R. E. et al. Obesity alters gut microbial ecology. Proc. Natl Acad. Sci. USA 102, 11070–11075 (2005).
Bäckhed, F., Manchester, J. K., Semenkovich, C. F. & Gordon, J. I. Mechanisms underlying the resistance to diet-induced obesity in germ-free mice. Proc. Natl Acad. Sci. USA 104, 979–984 (2007).
Finucane, M. M., Sharpton, T. J., Laurent, T. J. & Pollard, K. S. A taxonomic signature of obesity in the microbiome? Getting to the guts of the matter. PLoS ONE 9, e84689 (2014).
Beaumont, M. et al. Heritable components of the human fecal microbiome are associated with visceral fat. Genome Biol. 17, 189 (2016).
Konikoff, T. & Gophna, U. Oscillospira: a central, enigmatic component of the human gut microbiota. Trends Microbiol. 24, 523–524 (2016).
Gophna, U., Konikoff, T. & Nielsen, H. B. Oscillospira and related bacteria—from metagenomic species to metabolic features. Environ. Microbiol. 19, 835–841 (2017).
Morotomi, M., Nagai, F. & Watanabe, Y. Description of Christensenella minuta gen. nov., sp. nov., isolated from human faeces, which forms a distinct branch in the order Clostridiales, and proposal of Christensenellaceae fam. nov. Int. J. Syst. Evol. Microbiol. 62, 144–149 (2012).
Kim, M.-H. et al. Gut microbiota and metabolic health among overweight and obese individuals. Sci. Rep. 10, 19417 (2020).
Lippert, K. et al. Gut microbiota dysbiosis associated with glucose metabolism disorders and the metabolic syndrome in older adults. Benef. Microbes 8, 545–556 (2017).
Meehan, C. J. & Beiko, R. G. A phylogenomic view of ecological specialization in the Lachnospiraceae, a family of digestive tract-associated bacteria. Genome Biol. Evol. 6, 703–713 (2014).
de la Cuesta-Zuluaga, J. et al. Gut microbiota is associated with obesity and cardiometabolic disease in a population in the midst of Westernization. Sci. Rep. 8, 11356 (2018).
Companys, J. et al. Gut microbiota profile and its association with clinical variables and dietary intake in overweight/obese and lean subjects: a cross-sectional study. Nutrients 13, 2032 (2021).
Stanislawski, M. A. et al. Pre-pregnancy weight, gestational weight gain, and the gut microbiota of mothers and their infants. Microbiome 5, 113 (2017).
Fernandes, J., Su, W., Rahat-Rozenbloom, S., Wolever, T. M. S. & Comelli, E. M. Adiposity, gut microbiota and faecal short chain fatty acids are linked in adult humans. Nutr. Diabetes 4, e121 (2014).
Hu, X. et al. Soy fiber improves weight loss and lipid profile in overweight and obese adults: a randomized controlled trial. Mol. Nutr. Food Res. 57, 2147–2154 (2013).
Esposito, K., Kastorini, C.-M., Panagiotakos, D. B. & Giugliano, D. Mediterranean diet and weight loss: meta-analysis of randomized controlled trials. Metab. Syndr. Relat. Disord. 9, 1–12 (2011).
De Filippis, F. et al. High-level adherence to a Mediterranean diet beneficially impacts the gut microbiota and associated metabolome. Gut 65, 1812–1821 (2016).
Canfora, E. E., Jocken, J. W. & Blaak, E. E. Short-chain fatty acids in control of body weight and insulin sensitivity. Nat. Rev. Endocrinol. 11, 577–591 (2015).
Wang, Y. et al. Circulating short-chain fatty acids are positively associated with adiposity measures in chinese Adults. Nutrients 12, 2127 (2020).
Müller, M. et al. Circulating but not faecal short-chain fatty acids are related to insulin sensitivity, lipolysis and GLP-1 concentrations in humans. Sci. Rep. 9, 12515 (2019).
Zhao, L. The gut microbiota and obesity: from correlation to causality. Nat. Rev. Microbiol. 11, 639–647 (2013).
Cani, P. D. et al. Changes in gut microbiota control metabolic endotoxemia-induced inflammation in high-fat diet-induced obesity and diabetes in mice. Diabetes 57, 1470–1481 (2008).
Leone, V. et al. Effects of diurnal variation of gut microbes and high-fat feeding on host circadian clock function and metabolism. Cell Host Microbe 17, 681–689 (2015).
Yang, T. et al. Plant and fungal species interactions differ between aboveground and belowground habitats in mountain forests of eastern China. Sci. China Life Sci. https://doi.org/10.1007/s11427-022-2174-3 (2022).
Boulangé, C. L., Neves, A. L., Chilloux, J., Nicholson, J. K. & Dumas, M.-E. Impact of the gut microbiota on inflammation, obesity, and metabolic disease. Genome Med. 8, 42 (2016).
Zhang, Q. et al. Comparison of gut microbiota between adults with autism spectrum disorder and obese adults. PeerJ 9, e10946 (2021).
Yan, H. et al. Gut microbiome alterations in patients with visceral obesity based on quantitative computed tomography. Front. Cell. Infect. Microbiol. 11, 823262 (2021).
Karlsson, F. H. et al. Symptomatic atherosclerosis is associated with an altered gut metagenome. Nat. Commun. 3, 1245 (2012).
Fei, N. & Zhao, L. An opportunistic pathogen isolated from the gut of an obese human causes obesity in germfree mice. ISME J. 7, 880–884 (2013).
Cani, P. D. et al. Metabolic endotoxemia initiates obesity and insulin resistance. Diabetes 56, 1761–1772 (2007).
Fei, N. et al. Gut microbiota alterations in response to sleep length among African-origin adults. PLoS ONE 16, e0255323 (2021).
Kim, S.-Y. et al. Association between gut microbiota and depressive symptoms: a cross-sectional population-based study in South Korea. Psychosom. Med. 84, 757–765 (2022).
Chen, N. H., Djoko, K. Y., Veyrier, F. J. & McEwan, A. G. Formaldehyde stress responses in bacterial pathogens. Front. Microbiol. 7, 257 (2016).
Qin, J. et al. A metagenome-wide association study of gut microbiota in type 2 diabetes. Nature 490, 55–60 (2012).
Mehta, S. et al. Consumption of monounsaturated fatty acids is associated with improved cardiometabolic outcomes in four African-origin populations spanning the epidemiologic transition. Nutrients 13, 2442 (2021).
Nooromid, M. et al. Microbe-derived butyrate and its receptor, free fatty acid receptor 3, but not free fatty acid receptor 2, mitigate neointimal hyperplasia susceptibility after arterial injury. J. Am. Heart Assoc. 9, e016235 (2020).
Lewandowski, C. T. et al. Metabolomic analysis of a selective ABCA1 inducer in obesogenic challenge provides a rationale for therapeutic development. EBioMedicine 66, 103287 (2021).
Reiman, D., Layden, B. T. & Dai, Y. MiMeNet: Exploring microbiome-metabolome relationships using neural networks. PLoS Comput. Biol. 17, e1009021 (2021).
Barengolts, E. et al. Predictors of obesity among gut microbiota biomarkers in african american men with and without diabetes. Microorganisms 7, 320 (2019).
Navarro, G. et al. Gut microbial features can predict host phenotype response to protein deficiency. Physiol. Rep. 6, e13932 (2018).
Moreau, N. M. et al. Simultaneous measurement of plasma concentrations and 13C-enrichment of short-chain fatty acids, lactic acid and ketone bodies by gas chromatography coupled to mass spectrometry. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 784, 395–403 (2003).
Richardson, A. J., Calder, A. G., Stewart, C. S. & Smith, A. Simultaneous determination of volatile and non‐volatile acidic fermentation products of anaerobes by capillary gas chromatography. Lett. Appl. Microbiol. 9, 5–8 (1989).
Thompson, L. R., Sanders, J. G., McDonald, D. & Amir, A. A communal catalogue reveals Earth’s multiscale microbial diversity. Nature 551, 457–463 (2017).
Walters, W. et al. Improved bacterial 16S rRNA gene (V4 and V4-5) and fungal internal transcribed spacer marker gene primers for microbial community surveys. mSystems 1, e00009–e00015 (2016).
Gonzalez, A. et al. Qiita: rapid, web-enabled microbiome meta-analysis. Nat. Methods 15, 796–798 (2018).
Amir, A. et al. Deblur rapidly resolves single-nucleotide community sequence patterns. mSystems 2, e00191–16 (2017).
Bolyen, E. et al. Reproducible, interactive, scalable and extensible microbiome data science using QIIME 2. Nat. Biotechnol. 37, 852–857 (2019).
Bokulich, N. A. et al. Optimizing taxonomic classification of marker-gene amplicon sequences with QIIME 2’s q2-feature-classifier plugin. Microbiome 6, 90 (2018).
Mirarab, S., Nguyen, N. & Warnow, T. SEPP: SATé-enabled phylogenetic placement. Pac. Symp. Biocomput. 2012, 247–258 (2012).
McLaren, M. R. Silva SSU taxonomic training data formatted for DADA2 (Silva version 138). https://doi.org/10.5281/zenodo.3731176 (2020).
McMurdie, P. J. & Holmes, S. phyloseq: an R package for reproducible interactive analysis and graphics of microbiome census data. PLoS ONE 8, e61217 (2013).
Kembel, S. W. et al. Picante: R tools for integrating phylogenies and ecology. Bioinformatics 26, 1463–1464 (2010).
Lozupone, C. & Knight, R. UniFrac: a new phylogenetic method for comparing microbial communities. Appl. Environ. Microbiol. 71, 8228–8235 (2005).
Lin, H. & Peddada, S. D. Analysis of compositions of microbiomes with bias correction. Nat. Commun. 11, 3514 (2020).
Douglas, G. M. et al. PICRUSt2 for prediction of metagenome functions. Nat. Biotechnol. 38, 685–688 (2020).
Caspi, R. et al. The MetaCyc database of metabolic pathways and enzymes and the BioCyc collection of pathway/genome databases. Nucleic Acids Res. 44, D471–D480 (2016).
Oksanen, J., Blanchet, F. G., Kindt, R., Legendre, P. & Wagner, H. Vegan: Community Ecology Package. R Package Version. 2.0-10. (2013).
Acknowledgements
We thank the METS participants who continue their ongoing participation in the METS studies, as well as the site-specific clinic staff in Ghana, South Africa, Jamaica, Seychelles, and the US. The UCSD Microbiome Core performed sample extractions and library preparation utilizing protocols and primers published on the Earth Microbiome Project website (https://earthmicrobiome.org/). This publication includes data generated at the UC San Diego IGM Genomics Center utilizing an Illumina NovaSeq 6000 that was purchased with funding from a National Institutes of Health SIG grant under Award Number S10 OD026929 (J.A.G.). This work was supported by the National Institutes of Health grant under Award Number R01-DK111848 (L.R.D.).
Author information
Authors and Affiliations
Contributions
L.R.D. and B.T.L. conceived the study. L.R.D., C.C.-K., P.B., B.V., K.B.-A., J.P.-R., P.O.B., T.E.F., M.W., E.V.L., D.R., N.S., S.O., and A.L. collected human samples and metadata. G.E.-M. and C.C.-K. curated metadata. S.D. performed sequencing of samples. G.E.-M., C.C.-K., and M.G.M. conducted formal analysis and visualization. J.A.G. and L.R.D. supervised and provided feedback on formal analysis and visualization. G.E.-M., C.C.-K., L.R.D., and J.A.G. wrote the original paper. L.R.D. and J.A.G. secured the funding. All authors edited and approved the final paper.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Peer review
Peer review information
Nature Communications thanks Christian Diener and the other anonymous reviewer for their contribution to the peer review of this work. A peer review file is available.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Source data
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ecklu-Mensah, G., Choo-Kang, C., Maseng, M.G. et al. Gut microbiota and fecal short chain fatty acids differ with adiposity and country of origin: the METS-microbiome study. Nat Commun 14, 5160 (2023). https://doi.org/10.1038/s41467-023-40874-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41467-023-40874-x
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
