
Abstract
Purpose
To assess the effect of capsular bend and axial length on the rotational stability of toric IOL.
Methods
The prospective study included patients with preexisting astigmatism that were implanted with Acrysof IQ Toric IOL. According to the pre‑operative axial length, all patients were divided into 2 groups: high myopia (AL ≥ 26 mm) group, and emmetropia or low to moderate myopia group (AL <26 mm). High-speed Swept-source Optical Coherence Tomography (SS-OCT) radial scanning was performed after pupil dilation to obtain the toric IOL axial orientation and capsular bending index (CBI) at 1-day, 1-week, 1-month and 3-month intervals postoperatively. The correlation between the rotation of toric intraocular lens and the axial length or CBI was subsequently analyzed.
Results
68 eyes of 57 patients were included in the research. The rotation of toric IOL within the high myopia group was greater than the control group (P = 0.001, 1month postoperative). Capsular contact with the IOL was delayed in highly myopic eyes, although the results were not statistically significant (P = 0.094, 1-month postoperatively). There was a positive correlation between the degree of rotation and axial length at the interval found between 1-week and 1-month after the operation (r = 0.333, P = 0.005). There was a significant negative correlation between the IOL rotational speed and CBI (P < 0.001). The regression equation was Y = −0.441*X + 1.712 (R2 = 0.323, P < 0.001).
Conclusion
There was a significant negative correlation between the IOL rotation speed and the CBI, while the influence of the axial length and capsular bending mainly occurred between one week and one month after the operation.
Similar content being viewed by others


Introduction
Over the years, rapid advances in surgical technique and intraocular lens designs during cataract surgery have greatly diminished the postoperative need for spectacles. Among all patients undergoing cataract surgery, ~36–47% of patients undergoing cataract surgery have preexisting astigmatism of 1.00 diopter (D) or higher [1, 2]. Several methods for correcting preexisting astigmatism are available during cataract surgery, such as limbal relaxing incision, corneal relaxing incisions, selective phacoemulsification incision placement, and toric intraocular lens (Toric IOL) [3]. Among these options, to achieve optimal postoperative visual quality precisely and safely, the use of and rotational stability of a toric lens is vital, with previous research showing 1° of toric IOL misalignment correlates with a loss of 3.3% corrective efficacy [4].
Risk factors affecting the rotational stability of toric IOLs have been reported, including axial length (AL), IOL design and material, capsulorhexis size, capsular bag shrinkage and lens thickness, etc. [5]. Similarly, previous research speculated that increased diameter of the capsular bag and delay of capsular bend formation in patients with high myopia affects rotational stability [6, 7]. And Nishi et al. [8] described the characteristics of different stages of capsular bend formation through two-dimensional (2-D) slit-lamp photos and first proposed using the capsule bend index (CBI) for classification. Further research, the viewpoint that capsular contact and fibrosis cannot be neglected on IOL decentration and tilt were put forward [9]. And Chang et al. [10] showed the relationship between the change of intraocular lens position and capsular bend. However, the direct relationship between the capsular bend formation process and the rotational stability of toric IOLs is still unknown.
Fortunately, technological advances have allowed us to observe this relationship. The SS-OCT system (Casia SS-1000 OCT, Tomey, Japan) is a commercially available Fourier-domain, swept-source OCT with a swept-source laser wavelength of 1310 nm. It is able to observe capsular bend-IOL complex configurations and has the advantages of non-contact, fast scanning with clear imaging [11]. The CBI analyzed by the OCT image can then subsequently be used to represent the capsular bend formation process [8].
Utilizing such methods, the aim of this study was to evaluate rotational stability postoperatively, total misalignment, and to determine the influence of AL and capsular bend formation process on the rotational stability of Acrysof IQ Toric IOL.
Methods
Patients
This prospective study was performed at the Eye Hospital of Wenzhou Medical University, Hangzhou, China. All patients underwent phacoemulsification and implantation with Acrysof IQ Toric IOL (SN6ATT, Alcon Laboratories, Inc., USA) from October 2018 to October 2020. According to the pre‑operative AL, all patients were divided into 2 groups: Group1, high myopia (AL ≥ 26 mm); and Group 2, emmetropia or low to moderate myopia (AL < 26 mm). Inclusion criteria were cataracts and coexisting regular corneal astigmatism of >0.75D with a consistent astigmatism meridian between IOLMaster and Pentacam(meridian difference within 15° between the two instruments). The exclusion criteria were as follows: irregular corneal astigmatism, combination with other ophthalmic diseases, partial anterior capsule overlap (the IOL optic edge in some positions was exposed instead of anterior capsule overlapping), intraoperative complications including posterior capsule rupture, and pupil diameter less than 7 mm after mydriasis, corneal endothelial less than 1800 cells/mm2. The study was performed in accordance with the tenets of the Declaration of Helsinki and approved by the local ethics committee. This study has been registered at Clinicaltrials.gov (https://register.clinicaltrials.gov; numbered: NCT03779542). All patients provided written informed consent.
Pre‑operative assessment
All patients underwent a comprehensive ophthalmic examination to exclude unsuitable patients. Among this examination included corneal endothelial microscope, B-ultrasound, non-contact tonometer, and optical coherence tomography. Optical coherence interferometry (IOLMaster; Karl Zeiss AG, Germany) was utilized to determine the axial length (AL), anterior chamber depth (ACD), flat curvature power (K1), and steep curvature power (K2). The Three-dimensional Anterior Segment Analyzer (Pentacam, Oculus, Germany) was then used to determine preexisting corneal astigmatism and rule out irregular astigmatism. IOL spherical power was calculated using the Barrett Universal II formula. Cylinder power and target IOL axis were calculated using the Alcon online calculator based on the data of IOLMaster (http://www.myalcon-toriccalc.com/). A surgically induced astigmatism of 0.47 D was assumed to fill in the calculator.
Preoperative corneal marking
After topical anesthesia, with the patient sitting upright and with the head carefully aligned, the patient was asked to blink completely. Then, if the right eye is to be marked, the patient is instructed to look at the doctor’s right ear and keep it with the opposite eye. First, adjust the slit light to a sharp line, turn the direction to the desired axis, adjust the light through the center of the cornea. Next, the target axis position was marked as a sharp line by scratching the cornea epithelium at the limbus with a 27 gauge needle. Then, the 120° of the main corneal incision was marked in the same way. Finally, these scratch marks were stained with a surgical marking pen.
Surgical procedure
All surgeries were performed by the same experienced surgeon (Yun-e Zhao). Surgery was performed through a 2.2 mm clear corneal incision at 120° of the corneal limbus. A 5.0–5.5 mm continuous curvilinear capsulorhexis was then made, followed by hydrodissection, phacoemulsification, posterior capsule polish. The Toric IOL was then implanted with Monarch II delivery system and rotated into a position ~10–20° short of the intended axis. Finally, the IOL was rotated to the right position after the residual viscoelastics device was completely removed. The IOL axis was double-checked after incision hydrated and anterior chamber reinflated, also after the eye speculum removal.
Postoperative assessment
The follow-ups were performed at 1-day, 1-week, 1-month, and 3-months intervals after surgery. The actual IOL axis and CBI were assessed from images taken with SS-OCT after pupils were completely dilated.
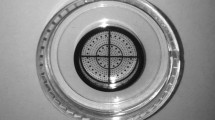
The images of SS-OCT show the optic edge and IOL axis marking. The marker line within the built-in program of the SS-OCT can be rotated to align the IOL axis marks, as shown in Fig. 1a. The examination was performed with the patient sitting in an upright position and gazing straight‑ahead by the same examiner. During the examination, the patient’s head was properly fixed on the rest, with careful adjustment of the height of the jaw bracket so that the lateral canthus of the patient’s eyes were aligned with the marked line on the column.

a The yellow marker line on the left represents the horizontal position, while the right marker line indicates the actual IOL axis (72° as illustrated in the Figure). b Capsular bend index assessed from four sections.
The capsular bend formation process was captured by the SS-OCT radial 3-D anterior chamber angle scan protocol. According to the process, the capsular bend can be divided into five stages [8], as seen in Fig. 2. Afterwards, scans of four sites within the IOL at an angle of 45° to the haptics were then taken to evaluate the capsular bend index, as shown in Fig. 1b. The specific calculation formula used here is \({{{{{{{\mathrm{CBI}}}}}}}} = \frac{1}{4}\mathop {\sum }\nolimits_{{{{{{{{\mathrm{K}}}}}}}} = 1}^4 {{{{{{{\mathrm{C}}}}}}}}_{{{{{{{\mathrm{K}}}}}}}}\) (Ck: Specific stage of each section of the toric IOL).

A Stage 0: No adhesion between the capsule and IOL. B Stage 1: Adhesion of the anterior capsule and IOL. C Stage 2: Adhesion between the anterior and posterior capsules peripherally. D Stage 3: Anterior and posterior capsules further adhered. E Stage 4: Adhesion completely between the capsule and IOL.
Total misalignment, postoperative IOL rotation
Total misalignment is the difference between the target IOL axis and the final postoperative axial orientation of Toric IOL. It includes surgical misalignment and toric IOL rotation and is affected by many factors during preoperative, intraoperative, postoperative periods. Our study mainly assessed the rotational stability and capsular bend formation from the first day postoperatively. To eliminate other confounding factors, such as corneal marking errors, intraoperative misalignment, postoperative IOL rotation only represents the rotation in axial orientation between the follow-up intervals.
Statistical analysis
Statistical analysis was performed by using SPSS20 (SPSS, Chicago, Illinois, USA). Computing). Normal distribution of variances was tested via Shapiro–Wilks tests. If variables were in accordance with normal distribution, the t-test was selected, otherwise, the non-parametric Wilcoxon signed-rank test was used. Relationships between variables were assessed using Pearson’s correlation analysis for continuous variables while Spearman’s correlation analysis for discrete variables. P values of <0.05 were considered statistically significant.
Results
Patient characteristics
A total of 57 patients (68 eyes) were met the inclusion criteria and included in the analysis follow up to three months after surgeries. The mean age and AL were significantly different between the two groups (P < 0.001). However, no significant differences in other data were found (patient demographics are presented in Table 1).
IOL rotation and misalignment
The IOL was misaligned counterclockwise in 69.1% of eyes on the 1-day follow-up after surgeries. Similarly, 48.5%, 50.0%, 35.3% of IOLs were rotated clockwise on the 1-week, 1-month and 3-month follow-ups respectively (Table 2).
As Table 2 and Fig. 3 show, a Toric IOL tends to be stable in the capsule over time. The postoperative total misalignment was 2.99 ± 1.68°, 3.10 ± 1.89°, 2.57 ± 1.86°, 2.47 ± 1.88° on 1-day, 1-week, 1-month, 3-month. Total misalignment of 63 eyes was within 5°, 4 eyes were 6°, 1 eye was 7° follow-up to 3-month after surgeries. There was no significant difference in the total misalignment between the two groups. Mean Toric IOL rotation during the three follow-up intervals from the first day after operation was 1.65 ± 1.30°, 1.68 ± 1.40°, 0.90 ± 1.16°. In addition, the mean Toric IOL rotation of high myopic patients was significantly greater at the 1-week to 1-month post‑operative follow-up when compared with the emmetropia or low to moderate myopic patients (P = 0.001).

(1) Overall. (2) Emmetropia or low to moderate myopia group. (3) High myopia group. (4) Toric IOL rotation was significantly and positively correlated with AL at 1 week to 1 month post-surgery (spearman r = 0.333, P = 0.005). (5) IOL rotation speed (°/week) was significantly and negatively correlated with mean CBI (Y = −0.441*X + 1.712, R2 = 0.323, P < 0.001).
Capsular bend index
Table 2 showed the summary of CBI at each follow-up in both groups. The CBI exhibited a slightly smaller value from the 1-day to 3-month post‑surgery follow-up in the high myopia group, although these results were not statistically significant.
Correlation analysis
There was no correlation between AL and total misalignment at each follow-up point. Noticeable, as shown in Fig. 3(4), the 1-week to 1-month post-surgery interval was the only time that showed a significant correlation between AL and IOL rotation. Moreover, the mean value of the CBI of two adjacent follow-up points was used as X-axis, and the rotation speed (° per week) of the IOL in corresponding follow-up intervals was used as the Y-axis scatter-plotting the results. This yielded a significant negative correlation (P < 0.001). Finally, the regression equation was Y = −0.441*X + 1.712 (Fig. 3(5): R2 = 0.323, P < 0.001).
Discussion
Toric IOLs allow the surgeon to correct preexisting astigmatism in a safe and predictable way during phacoemulsification cataract surgery. Orientation originating by errors in preoperative preparation, intraoperative misalignment, or postoperative rotation stability will reduce efficacy. The current study assessed the influence of AL and capsular bend formation process on the rotational stability of a toric IOL. To our knowledge, this is the first study confirming the relationship between CBI and rotation stability.
The mean misalignment of 2.47 ± 1.88° of Acrysof IQ Toric IOL seen in the present study for the total group follow-up to 3-month post-operation is consistent with that reported in previous Toric IOL studies. [12, 13] The similar values of mean misalignment proved the SS-OCT is a simple and practical way to capture the actual IOL axis in a clinical setting; however, there was no significant difference in mean misalignment between the two groups, which is consistent with the research of Guo et al. [14] Therefore, toric IOLs have good rotational stability in most high myopic patients.
In our present study, toric IOL tended to rotate counterclockwise from the end of the initial surgery to 1-day after surgery. This is probably attributed to the combined influence of manual marking, intraoperative alignment and postoperative rotation stability. Manual marking alone has previously been observed to contribute ~2.5° in misalignment in prior studies [15]. Similarly, Patel et al. [16] suggested that expansion of the capsular bag produces counterclockwise rotation. Therefore, the counterclockwise rotation in the early postoperative period of our study may be explained by the large proportion of high myopia patients. In accordance with previous studies [17], following the first day after surgery, toric IOLs tend to rotate clockwise, which may be related to the open-loop design of IOL [13]. The clockwise rotation could also be attributed to haptic compression caused by capsular bend and fibrosis.
As for the mean Toric IOL rotation, the high myopia group had significantly greater rotation from the 1-week to 1-month postoperative interval when compared with the comparison group. Moreover, AL showed a significant correlation with IOL rotation from the 1-week to 1-month postoperative interval in our study; however, there is still debate about the correlation between AL and IOL rotation in past studies. Some views [6, 17] indicated that AL is positively related to IOL rotation, while others showed no correlation [14, 18, 19]. In addition, prior studies [12, 20, 21] showed the misalignment of high myopic patients was more likely to exceed 10°. It is evident postoperative rotation is likely to occur in high myopic patients [22], but the mechanism remains unclear.
Toric IOLs that are currently available have an overall IOL diameter ranging from 11.0 mm to 13.0 mm, which matches with the capsular diameter of normal patients. The large capsule and the weak zonule of high myopic patients [23] are then considered to cause the more evident IOL rotation of early-stage post-operation, while the delaying of capsular bend formation affects the long-term rotation stability [7]. In order to further explore the influence of the capsular bend formation process on the IOL rotation stability, the CBI was used in the present study. In our results, CBI values in high myopia patients were lower, especially at 1-month postoperatively (P = 0.094), although these results were not statistically significant. It may be influenced by grouping criterion, patients whose axial length between 24 and 26 mm indicated moderate myopia included in the control group. However, this enabled the correlation analysis to be continuous. Accordingly, it meant 1-week to 1-month after the operation was the main period of delay in the capsular bend formation process in high myopic patients. This result is consistent with previous research [14], which speculated the shift of rotational degrees of IOL from 1-week to 1-month postoperatively was due to a climax of capsular bag shrinkage and fibrosis. In further correlation analysis, there was a significant negative correlation between the CBI and the rotation of the IOL, which indicated that an IOL tended to be stable in a capsule with capsular bend formation. Overall, the present study suggested that the delay in the formation of capsular bend in patients with a longer AL played an important role in the rotational stability of toric IOL, and its impact existed mainly from the 1-week to 1-month interval postoperatively. Certainly, a larger sample of improving research is further needed.
IOL repositioning surgery can be considered when correcting the misalignment of more than 15° off-axis misalignment in patients whose visual quality was significantly affected [20]. A multicentre case research [24] showed the incidence of re-orientating surgery was 0.213–1.942% after implantation of three different toric IOL. The benefit of repositioning surgery is self-evident; however, it is a difficult challenge for doctors in part because of the timing of the operation. Oshika et al. [25] suggested that repositioning surgery should be performed sometime between 1 and 3 weeks after the primary IOL implantation. It was stated that appropriate operation time can reduce risks, including rotation occurring again, difficult intraoperative rotation and damaging the Zinn’s zonules. Within our study, the regression equation between the CBI and rotation speed of IOL supports these suggestions, and has the potential to ultimately help surgeons to better find ideal intervals or operation opportunities.
It is worth noting that we have excluded the eyes with partial anterior capsule overlap IOL optic in our study. Actually, CBI could not be evaluated in these cases, and in addition, total anterior capsule overlap is considered as a mechanical force critical to the IOL stability [26,27,28]. Li et al. [29] examined the relationship between the capsulorhexis size and Toric IOL rotation, and demonstrated the diameter of capsulorhexis should be controlled within the range of 5.0–5.80 mm. Based on their research, 66.7% of eyes with partial anterior capsule overlap rotate over 5° at 3 months after surgery.
All things considered, there are still some limitations in this study. One is the small sample size and short follow-up intervals, while some of the patients had not completely formed the capsular bend until the 3-month postoperative follow-up. Another consideration is the method to capture the actual IOL axis by SS-OCT may be influenced by cyclotorsion. In addition, the axial orientation of SS-OCT can only be accurate to one digit, which may result in researcher bias; however, due to the examination being performed with the patient sitting in an upright position by the same examiner, and with similar values of mean misalignment with the previous study, it has also suggested the bias can be accepted. Furthermore, toric IOL rotation is affected by multiple factors, we only focused on the capsular bend formation which is also affected by axial myopia and a large capsular bag, a large sample multifactorial study is necessary.
In conclusion, although toric IOLs have ideal rotational stability in most high myopic patients, longer axial length is still a risk factor affecting rotation stability due to the possible delay in capsular bend formation, with the impact mainly occurring 1-week to 1-month after surgery.
Summary
What was known before
-
Risk factors affecting the rotational stability of toric IOLs have been reported, including axial length (AL), IOL design and material, capsulorhexis size, capsular bag shrinkage, and lens thickness, etc.
-
Increased diameter of the capsular bag and delay of capsular bend formation in patients with high myopia affects rotational stability.
What this study adds
-
A significant negative correlation between the IOL rotation speed and the capsular bending index (CBI).
-
The influence of the axial length and capsular bending mainly occurred between one week and one month after the operation.
References
Hoffmann PC, Hutz WW. Analysis of biometry and prevalence data for corneal astigmatism in 23,239 eyes. J Cataract Refract Surg. 2010;36:1479–85.
Yu JG, Zhong J, Mei ZM, Zhao F, Tao N, Xiang Y. Evaluation of biometry and corneal astigmatism in cataract surgery patients from Central China. BMC Ophthalmol. 2017;17:56.
Yang LH, Tang X. The research progress in treating astigmatism at the time of cataract surgery. Zhonghua Yan Ke Za Zhi. 2011;47:573–6.
Alpins NA. Vector analysis of astigmatism changes by flattening, steepening, and torque. J Cataract Refract Surg. 1997;23:1503–14.
Visser N, Bauer NJ, Nuijts RM. Toric intraocular lenses: historical overview, patient selection, IOL calculation, surgical techniques, clinical outcomes, and complications. J Cataract Refract Surg. 2013;39:624–37.
Zhu X, He W, Zhang K, Lu Y. Factors influencing 1-year rotational stability of AcrySof Toric intraocular lenses. Br J Ophthalmol. 2016;100:263–8.
Zhao Y, Li J, Lu W, Chang P, Lu P, Yu F, et al. Capsular adhesion to intraocular lens in highly myopic eyes evaluated in vivo using ultralong-scan-depth optical coherence tomography. Am J Ophthalmol. 2013;155:484–91. e481
Nishi O, Nishi K, Akura J. Speed of capsular bend formation at the optic edge of acrylic, silicone, and poly(methyl methacrylate) lenses. J Cataract Refract Surg. 2002;28:431–7.
Meng J, He W, Rong X, Miao A, Lu Y, Zhu X. Decentration and tilt of plate-haptic multifocal intraocular lenses in myopic eyes. Eye Vis. 2020;7:17.
Chang P, Li X, Chen D, Xu Z, Ding X, Zhao YE. The relationship between the change of intraocular lens position and capsular bend after cataract surgery. J Refract Surg. 2021;37:324–30.
Fang Y, Xixia D, Jin L, Lei L, Pingjun C, Hongfang Z, et al. Relationship of posterior capsular opacification and capsular bend type investigation based on swept-source optical coherence tomography. Curr Eye Res. 2020;45:17–23.
Lee BS, Chang DF. Comparison of the rotational stability of two toric intraocular lenses in 1273 consecutive eyes. Ophthalmology. 2018;125:1325–31.
Koshy JJ, Nishi Y, Hirnschall N, Crnej A, Gangwani V, Maurino V, et al. Rotational stability of a single-piece toric acrylic intraocular lens. J Cataract Refract Surg. 2010;36:1665–70.
Guo T, Gao P, Fang L, Guo L, Fan Y, Liu C. Efficacy of Toric intraocular lens implantation in eyes with high myopia: a prospective, case-controlled observational study. Exp Ther Med. 2018;15:5288–94.
Farooqui JH, Koul A, Dutta R, Shroff NM. Comparison of two different methods of preoperative marking for toric intraocular lens implantation: bubble marker versus pendulum marker. Int J Ophthalmol. 2016;9:703–6.
Patel CK, Ormonde S, Rosen PH, Bron AJ. Postoperative intraocular lens rotation: a randomized comparison of plate and loop haptic implants. Ophthalmology. 1999;106:2190–5. discussion 2196
Shah GD, Praveen MR, Vasavada AR, Vasavada VA, Rampal G, Shastry LR. Rotational stability of a toric intraocular lens: influence of axial length and alignment in the capsular bag. J Cataract Refract Surg. 2012;38:54–59.
Schartmuller D, Schriefl S, Schwarzenbacher L, Leydolt C, Menapace R. True rotational stability of a single-piece hydrophobic intraocular lens. Br J Ophthalmol. 2019;103:186–90.
Klamann MK, Von Sonnleithner C, Gonnermann J, Maier AK, Torun N, Bertelmann E. Influence of biometric parameters on rotational stability of toric IOLs. Eur J Ophthalmol. 2013;23:836–40.
Chang DF. Repositioning technique and rate for toric intraocular lenses. J Cataract Refract Surg. 2009;35:1315–6.
Miyake T, Kamiya K, Amano R, Iida Y, Tsunehiro S, Shimizu K. Long-term clinical outcomes of toric intraocular lens implantation in cataract cases with preexisting astigmatism. J Cataract Refract Surg. 2014;40:1654–60.
Ruhswurm I, Scholz U, Zehetmayer M, Hanselmayer G, Vass C, Skorpik C. Astigmatism correction with a foldable toric intraocular lens in cataract patients. J Cataract Refract Surg. 2000;26:1022–7.
Tehrani M, Dick HB, Krummenauer F, Pfirrmann G, Boyle T, Stoffelns BM. Capsule measuring ring to predict capsular bag diameter and follow its course after foldable intraocular lens implantation. J Cataract Refract Surg. 2003;29:2127–34.
Oshika T, Fujita Y, Hirota A, Inamura M, Inoue Y, Miyata K, et al. Comparison of incidence of repositioning surgery to correct misalignment with three toric intraocular lenses. Eur J Ophthalmol. 2020;30:680–4.
Oshika T, Inamura M, Inoue Y, Ohashi T, Sugita T, Fujita Y, et al. Incidence and outcomes of repositioning surgery to correct misalignment of toric intraocular lenses. Ophthalmology. 2018;125:31–35.
Hayashi H, Hayashi K, Nakao F, Hayashi F. Elapsed time for capsular apposition to intraocular lens after cataract surgery. Ophthalmology. 2002;109:1427–31.
Xixia D, Pingjun C, Hongfang Z, Giacomo S, Jinhai H, Feixue C, et al. Three-dimensional morphology study of capsule in pseudophakic eyes with high-speed swept-source optical coherence tomography. Curr Eye Res. 2019;44:607–13.
Sasaki K, Eguchi S, Miyata A, Nishimura T, Miyata K, Hasegawa Y, et al. Anterior capsule coverage and rotational stability of an acrylic toric intraocular lens. J Cataract Refract Surg. 2021;47:618–21.
Li S, Li X, He S, Zheng Q, Chen X, Wu X, et al. Early Postoperative Rotational stability and its related factors of a single-piece acrylic toric intraocular lens. Eye. 2020;34:474–9.
Funding
This study was supported by Medical and Health Science and Technology Project of Zhejiang Province (2018KY538) and Zhejiang Provincial health leading talent project.
Author information
Authors and Affiliations
Contributions
PJC and DJC conceived and designed the presented study. BH, YLW and SYQ performed the data collection. PJC and DJC performed the analysis and wrote the manuscript. XXD and YEZ provided a critical review of the manuscript.
Corresponding author
Ethics declarations
Competing interests
All authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Chang, P., Chen, D., Hu, B. et al. Effect of capsular bend on the rotational stability of toric intraocular lens. Eye 37, 480–485 (2023). https://doi.org/10.1038/s41433-022-01964-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41433-022-01964-0
This article is cited by
-
Visual performance and rotational stability of a multifocal toric intraocular lens in myopic eyes
Graefe's Archive for Clinical and Experimental Ophthalmology (2023)
