
Abstract
Background
Canthal rounding can occur following trauma or surgery to the medial or lateral canthus, causing possible aesthetic or functional deficits to patients. Several surgical techniques to repair canthal rounding have been described previously. We report a new technique for canthoplasty repair of canthal rounding with the use of illustrative cases.
Methods
This is a retrospective case series describing the technique using illustrative cases from across three sites (London [UK], Adelaide [Australia], Sydney [Australia]). Twelve patients with post-surgical canthal rounding were included. Information collected for our illustrative cases include patient demographics, diagnosis, complications, outcomes and further treatment.
Results
There were no peri- or post-operative complications. All except one patient reported good surgical outcomes after one procedure. In one patient there was rounding recurrence.
Conclusions
Our patients reported excellent outcomes post-operatively without any significant scarring.
Similar content being viewed by others

Introduction
Canthal rounding can occur following surgery to the medial or lateral canthus. This is seen as a rounded fold of skin and scar tissue inside the normal canthal angle, causing horizontal shortening of the eyelid aperture. Canthal rounding is a separate entity from canthal webbing, which is seen as semilunar folds of skin and scar that can overlie, or sit outside, the canthal angle. Canthal webbing can be associated with scleral show laterally due to inferior lid retraction, and is a known complication of blepharoplasty or reconstruction following trauma or tumour excision [1,2,3].
Canthal rounding can be cosmetically-unacceptable to patients. In more severe cases, the rounding can cause functional deficit with visual obstruction on lateral gaze. We report a technique for canthoplasty repair of canthal rounding with the use of illustrative cases. All research was conducted in accordance with the Declaration of Helsinki. Institutional Review Board/Ethics Committee approval was obtained.
Materials and methods
The surgical technique was developed by one of the senior authors (NJ). The procedure can be carried out under local anaesthesia only or in combination with sedation.
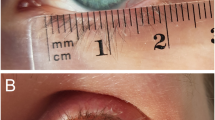
The area of canthal rounding is assessed and the new eyelid margin is marked (Fig. 1a). The canthal rounding is split into its anterior and posterior lamellae using a 15-blade followed by Westcott spring scissors (Fig. 1b). Local anaesthetic infiltration in between the anterior and posterior lamella can help hydrodissect the layers prior to surgical separation of the layers.

a The new eyelid margin is marked (dotted line). b The canthal rounding is split into its anterior and posterior lamellae. c The anterior flap is created and folded into its new position. d The posterior flap is created. e The posterior flap is folded into its new position. f The flaps are secured into their new positions. g Lateral canthopexy. h Flap is marked. i Anterior flap is completely excised. j and k Posterior flap is folded over and sutured into the new inferior lid margin.
The anterior flap is cut along the new superior lid margin using Westcott spring scissors and folded downwards to create the anterior lamella of the new inferior lid margin (Fig. 1c). The posterior flap is cut along the new inferior lid margin using Westcott spring scissors and folded upwards to create the anterior lamella of the new superior lid margin (Fig. 1d and 1e). The flaps are secured into their new positions with interrupted vicryl 6/0 sutures (Fig. 1f). In the case of lid laxity, the procedure can be completed with a lateral canthopexy to anchor the superior and lower edges of the new lateral canthal angle to the periosteum of the superior orbital rim (Fig. 1g).
If there is insufficient tissue to create both anterior and posterior flaps, for example in smaller areas of canthal rounding with less conjunctiva available, a modification to the above method to create a single flap can be used instead (DS). The canthal rounding is marked (Fig. 1h) then split into its anterior and posterior lamellae as described earlier. The anterior flap is then cut along both superior and inferior lid margins and completely excised (Fig. 1i). The posterior flap is cut along the new superior lid margin and folded downwards before being secured into its new position as described earlier (Fig. 1j and 1k). The new superior lid margin is left to heal by granulation.
Results
Twelve patients have undergone this surgical technique for correction of post-surgical canthal rounding. There were five men and seven women. The median age was 65.5 years (range: 26–88). There were no peri- or post-operative complications. Median follow up was 12 months (range: 1.5–48). All patients except one reported good surgical outcomes, defined as cosmetically and functionally acceptable result to the patient and surgeon, after one procedure. There was one recurrence of rounding, which was noted at the first post-operative review at 2 weeks following surgery. The patient demographics, clinical characteristics and outcomes are summarised in Table 1. Pre- and post-operative photographs of selected cases are shown in Fig. 2.

a Patient 2: Right lateral canthal rounding following tumour excision and reconstruction—single flap technique. b. Patient 3: Left lateral canthal rounding following tumour excision and reconstruction—single flap technique. c. Patient 6: Right lateral canthal rounding following tumour reconstruction—single flap technique. Note the widened aperture but rounding recurrence. d. Patient 9: Left lateral canthal rounding following blepharoplasty—double flap technique (right side not shown). e. Patient 12: Left lateral canthal rounding following blepharoplasty—single flap technique.
Discussion
Canthal rounding has been reported following periocular tumour or trauma reconstruction [4, 5]. The rounding can have a significant component of scar tissue, creating an aesthetic or functional deficit that can be distressing for patients.
Several surgical techniques exist for addressing canthal rounding, but they are not described in the literature. Anecdotally, these techniques involve dividing the rounded canthus, with or without the use of bolsters, to try and prevent re-adhesion of the new margins.
With our technique, we make use of the excess horizontal tissue to create the flaps, which in turn are folded and secured to realign the canthal angle discrepancies. The conjunctivalised tissue appears effective at increasing the lid aperture and preventing re-adhesions, even when only a single flap is used and one lid margin is left to granulate. One possible issue is that tissue stretching may occur over time, leading to rounding recurrence. Another possible issue is post-operative conjunctival thickening and persistent redness in the operated area. However, this was not encountered in our patient group.
In conclusion, our technique demonstrates a method for reconstructing a natural-looking canthal angle with good cosmetic outcomes and minimal scarring.
Summary
What was known before
-
Canthal rounding can occur following surgery to the medial or lateral canthus.
-
Canthal rounding can cause cosmetic or functional deficit with visual obstruction on lateral gaze.
What this study adds
-
We report a technique for canthoplasty repair of canthal rounding with the use of illustrative cases.
-
Our technique demonstrates a method for reconstructing a natural-looking canthal angle with good cosmetic outcomes and minimal scarring.
References
Massry GG. Cicatricial canthal webs. Ophthalmic Plast Reconstr Surg. 2011;27:426–30.
Yaremchuk MJ. Restoring palpebral fissure shape after previous lower blepharoplasty. Plast Reconstr Surg. 2003;111:441–50.
Millman AL, Williams JD, Romo T, Taggert N. Septal-myocutaneous flap technique for lower lid blepharoplasty. Ophthalmic Plast Reconstr Surg. 1997;13:84–9.
Yazici B, Çetinkaya A, Çakirli E. Bilobed flap in the reconstruction of inferior and/or lateral periorbital defects. Ophthalmic Plast Reconstr Surg. 2013;29:208–14.
Clark ML, Kneiber D, Neal D, Etzkorn J, Maher IA. Safety of Periocular Mohs Reconstruction: a Two-Center Retrospective Study. Dermatol Surg. 2020;46:521–4.
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Juniat, V., Joshi, S., Hersh, D. et al. Canthoplasty repair for canthal rounding. Eye 36, 564–567 (2022). https://doi.org/10.1038/s41433-021-01497-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41433-021-01497-y
