
Abstract
Background:
Data on the association between visual difficulty and physical activity (PA) from low- and middle-income countries (LMICs) are scarce. Thus, the aim of the study was to investigate the association between visual difficulty and PA among adults from 36 LMICs, and to assess the mediators in this association.
Methods:
Cross-sectional, community-based, predominantly nationally representative data from the World Health Survey were analysed. The final sample included 199,110 individuals aged ≥18 years [mean (SD) age 38.6 (16.1) years; 49.4% males]. Visual difficulty referred to having severe/extreme difficulties in seeing and recognizing a person that the participant knows across the road. Low PA was defined as not complying with PA recommendations of 150 min of moderate-vigorous PA per week. Multivariable logistic regression, meta-analysis, and mediation analysis were conducted to assess associations.
Results:
Meta-analysis based on country-wise multivariable logistic regression analysis showed that overall, visual difficulty is associated with a 1.53 (95% CI = 1.38–1.71) times higher odds for low PA. Particularly strong associations were observed in males (OR = 1.72; 95% CI = 1.45–2.05) and adults aged ≥65 years (OR = 1.95; 95% CI = 1.67–2.29). Interpersonal activities, cognition, and sleep/energy explained >10% of the association between visual difficulty and low PA.
Conclusions:
In conclusion, we found evidence that especially in the case of males and older adults with visual difficulties in LMICs, there were low levels of engagement with PA. Addressing issues such as interpersonal activities, cognition, and sleep/energy in people with visual difficulties may increase levels of PA.
Similar content being viewed by others

Introduction
Physical activity (PA) may be described as any bodily movement caused by contraction of skeletal muscle that results in energy expenditure and may include activities such as structured exercise and sport, active travel (walking and cycling), occupational activity, and household chores/gardening [1]. Regular and sustained participation in PA is beneficial for almost every facet of adult health. For example, a recent systematic review of review articles found that physically active older adults are at a reduced risk of cardiovascular mortality, breast and prostate cancer, fractures, recurrent falls, functional limitation, and depression. They also experience healthier ageing trajectories, better quality of life, and improved cognitive functioning [2]. Importantly, regular participation in PA is also associated with a reduction in all-cause mortality [3]. In light of this evidence, governments across the globe have produced recommendations for adequate levels of PA. One key message from the World Health Organization (WHO) guidance is that adults and older adults should achieve at least 150 min of moderate PA and/or 75 min of vigorous PA per week [4]. It is therefore important to ensure that all populations maintain adequate levels of PA for good health.
However, one group that has consistently been reported to have low levels of PA are those who are visually impaired. The authors of the present paper have shown in a sample of 6634 UK participants (mean age 65.0 ± 9.2 years) that those with poor vision were twice as likely to be physically inactive than those with good eyesight [5]. The present authors have also found similar associations in adults residing in the US [6] and Spain [7]. Moreover, other authors have found similar results [8]. However, all previous studies on this topic have been carried out in high-income countries (HICs) and there are no studies specifically on this topic from low- and middle-income countries (LMICs). This is an important research gap as the association may differ between HICs and LMICs due to differences in social and political contexts. For example, people with visual difficulties in LMICs may have more difficulty in engaging in PA owing to lack or scarcity of disability accessible facilities. Moreover, visual difficulties are more prevalent in LMICs than HICs. One study reported that across 70 countries, 21% of adults reported any visual difficulty but that the prevalence is higher in LMICs (23–24%) as compared to HICs (13%) [9].
Reasons why people with visual difficulties have low levels of PA is likely to be manyfold, e.g. due to factors such as lack of access to recreational and athletic programmes, and help or encouragement in developing suitable and safe physical recreation skills and habits [10]. Moreover, people with visual difficulties may experience activity limitations in walking and environmental barriers such as those for transport, and this can hamper a person’s ability to be physically active [10, 11]. In addition, it is possible that people with visual difficulties are more likely to lose jobs, develop mental health problems, or have problems with interpersonal activities, which may themselves also lead to less PA [12,13,14,15,16,17].
Identifying mediating factors will allow the development of targeted interventions to increase levels of PA in the visually impaired. However, there are no previous studies that have quantified the degree to which various factors may explain this association. Therefore, the aims of the present study were as follows (a) investigate the association between visual impairment and PA in 199,110 individuals aged ≥18 years from 36 LMICs (b) identify the potential mediating role of unemployment, depression, interpersonal activities, cognition, and sleep/energy in this association.
Methods
The World Health Survey (WHS) was a cross-sectional survey carried out in 70 countries in 2002–2004. Single-stage random sampling was undertaken in 10 countries, while stratified multi-stage random cluster sampling was conducted in 60 countries. Survey details are available elsewhere (http://www.who.int/healthinfo/survey/en/). In brief, individuals with a valid home address aged ≥18 years were eligible to participate. Kish tables were used so that all household members had an equal chance of being selected. The questionnaire was subject to standard translation procedures to ensure comparability. Information was obtained through face-to-face interviews and telephone interviews conducted by trained interviewers. Across all countries, the individual response rate was 98.5% [18]. To adjust for non-response, sampling weights were generated using the population distribution as reported by the United Nations Statistical Division. Ethical approval for the survey was provided by ethical boards at each study site. All participants gave their informed consent.
Visual difficulty
As in a previous WHS publication, we operationalized visual difficulty as having severe or extreme difficulty in seeing and recognizing a person that the participant knows across the road (i.e. from a distance about 20 m) [9]. If the participant wore glasses or contact lenses then they were asked to answer this question taking into account glasses or contact lenses. A validity study using the exact same question in the WHS showed that this response (i.e. severe/extreme) likely corresponds to WHO definitions of visual impairment (20/60 or 0.48 logMAR) [9].
Physical activity
Items from the International Physical Activity Questionnaire [19] were used to categorize PA. Specifically, participants were asked how many days over the past week on average they engaged in moderate and vigorous PA. Second, participants were asked for how many minutes on average, they engage in PA at a moderate and vigorous level. The total amount of moderate to vigorous PA over the last week was calculated and those scoring ≥150 min were classified as meeting the recommended guidelines (coded 0), and those scoring <150 min (low physical activity) were classified as not meeting the recommended guidelines (coded 1).
Mediators
The mediators in the current analysis (unemployment, anxiety, depression, cognition, interpersonal activities, sleep/energy) were based on the possibility that they may be the consequence of visual impairment, while they may also be the cause of low PA [20,21,22,23,24,25,26,27,28,29]. Unemployment referred to not working for pay or not currently in paid employment. Anxiety was assessed by the question ‘Overall in the past 30 days, how much of a problem did you have with worry or anxiety’ with answer options being none, mild, moderate, severe, and extreme. In accordance with previous WHS publications, those who answered severe and extreme were considered to have anxiety [30, 31]. Depression was defined using the DSM-IV algorithm and was based on duration and persistence of depressive symptoms in the past 12 months [32, 33]. Cognition, interpersonal activities, and sleep/energy were assessed with two questions each that assessed health function in the past 30 days. The actual questions can be found in Table S1 in the Supplementary. Each item was scored on a five-point scale ranging from ‘none’ to ‘extreme/cannot do’. As in previous WHS publications, for each separate domain, we used factor analysis with polychoric correlations to obtain a factor score, which was later converted to scores ranging from 0 to 100 with higher values representing worse health function [34].
Control variables
The control variables were selected based on past literature and included age (18–44, 45–64, ≥65 years), sex, wealth quintiles, current smoking (yes or no), obesity, and chronic physical conditions (angina, arthritis, diabetes). The wealth quintiles were created using principal component analysis based on 15–20 assets including country-specific items for some countries. Obesity was defined as body mass index ≥30 kg/m [2] based on self-reported weight and height. Arthritis and diabetes were based on self-reported lifetime diagnosis. For angina, in addition to a self-reported diagnosis, a symptom-based diagnosis based on the Rose questionnaire was also used [35]. Chronic physical conditions referred to having at least one of angina, arthritis, or diabetes.
Statistical analysis
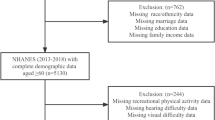
Data were publicly available for 69 countries but 10 countries with no sampling information were excluded. Of the remaining 59, a total of 10 HICs were deleted as the focus on this paper was on LMICs. Two LMICs were deleted as data on PA were not collected. Furthermore, 11 LMICs were deleted as >25% of data on PA and/or visual difficulty were missing. Thus, individuals from 36 LMICs constituted the analytical sample. The classification of country-income level was based on the World Bank classification at the time of the survey (2003). All data were nationally representative with the exception of Russia, India, China, Comoros, and Ivory Coast.
The statistical analysis was done with Stata 14.1 (Stata Corp LP, College station, Texas). The difference in sample characteristics by visual difficulty or low PA was tested by Chi-squared tests for categorical variables and Student’s t tests for continuous variables. Multivariable logistic regression analysis was conducted to assess the association between visual difficulty (exposure) and low PA (outcome). Analyses using the overall sample, and age- (i.e. 18–44, 45–64, ≥65 years), sex-, and country-stratified samples were done. In order to assess whether the magnitude of the association between visual difficulty and low PA is statistically different between age groups and sex, we conducted interaction analysis by including the product term [age group (18–44, 45–64, ≥65 years) X visual difficulty] or (sex X visual difficulty)] using the overall sample.
Furthermore, to assess whether there is between-country heterogeneity in the association between visual difficulty and low PA, the Higgins’s I [2] statistic was calculated. This represents the degree of heterogeneity that is not explained by sampling error with a value of <40% often considered as negligible and 40–60% as moderate heterogeneity [36]. A pooled estimate was obtained by combining the estimates for each country into a random effect meta-analysis.
Next, we conducted mediational analysis to understand the extent to which various factors (unemployment, anxiety, depression, cognition, interpersonal activities, and sleep/energy) may explain the association between visual difficulty and low PA using the overall sample. The mediational analysis was done using the khb (Karlson Holm Breen) command in Stata [37]. This method decomposes the total effect of a variable into direct and indirect effects and can be used with logistic regression models. This method also allows for the calculation of the mediated percentage, which is interpreted as the percentage of the main association that can be explained by the mediator. Each potential mediator was included in the model separately.
The regression analyses were adjusted for age, sex, wealth, smoking, obesity, chronic conditions, and country with the exception of the age-, sex-, and country-stratified analyses that were not adjusted for age, sex, and country, respectively. Adjustment for country was done by including dummy variables for each country as in previous WHS publications [38, 39]. The sample weighting and the complex study design were taken into account in all analyses. Results from the logistic regression models are presented as odds ratios (ORs) with 95% confidence intervals (CIs). The level of statistical significance was set at P < 0.05.
Results
The analytical sample consisted of 199,110 individuals aged ≥18 years [mean (SD) age 38.6 (16.1) years; 49.4% males]. The overall prevalence (95% CI) of visual difficulty and low PA were 5.0 (4.7-5.2) and 30.5 (29.6-31.4), respectively. There was a large range in this prevalence by country with it being 1.2% (Malaysia) to 9.9% (Comoros) and 9.6% (Comoros) to 81.8% (Mauritania) for visual difficulty and low PA, respectively (Table 1). The sample characteristics are provided in Table 2. The prevalence of low PA was much higher among those with visual difficulty (vs. those without this condition) (46.3% vs. 29.8%; P < 0.001). Also, the prevalence of older age, females, obesity, chronic physical conditions, unemployment, anxiety, and depression were higher among those with visual difficulty or low PA, while they had worse health status in terms of cognition, interpersonal activities, and sleep/energy. Lower levels of wealth and smoking were more common among those with visual difficulty, but these were less common among those with low levels of PA.
The country-wise association between visual difficulty and low PA estimated by multivariable logistic regression is shown in Fig. 1. The overall pooled estimate based on a meta-analysis was 1.53 (95% CI = 1.38–1.71) with a moderate level of heterogeneity (I2 = 53.1%). The pooled estimate for low-income countries and middle-income countries were similar. There was a significant interaction in the association between visual difficulty and low PA by age group and sex (i.e. interaction term P < 0.05). Specifically, the association was strongest among those aged ≥65 years (OR = 1.95; 95% CI = 1.67–2.29), compared to those aged 18–44 years (OR = 1.23; 95% CI = 0.97–1.58) and 45–64 years (OR = 1.26; 95% CI = 1.05–1.51). Furthermore, this association was stronger among males than females [males OR 1.72 (95% CI = 1.45–2.05) vs. females OR 1.42 (95% CI = 1.25–1.62)] (Fig. 2).

OR Odds ratio, CI Confidence interval. Models were adjusted for age, sex, wealth, smoking, obesity, and chronic conditions. Overall estimate was obtained by meta-analysis with random effects.

OR Odds ratio, CI Confidence interval. Age-stratified analysis is adjusted for sex, wealth, smoking, obesity, chronic conditions, and country. Sex-stratified analysis is adjusted for age, wealth, smoking, obesity, chronic conditions, and country.
The mediation analysis showed that interpersonal activities, cognition, and sleep and energy explained >10% of the association between visual difficulties and low PA, while unemployment, anxiety, and depression explained this association to a lesser degree (Table 3).
Discussion
In this large sample of 199,110 individuals aged ≥18 years from 36 LMICs, we found that, overall, those with visual difficulty were 1.53 (95% CI = 1.38–1.71) times more likely to have low PA. This association was particularly pronounced among males (OR = 1.72) and those aged ≥65 years (OR = 1.95). Moreover, interpersonal activities, cognition, and sleep/energy explained >10% of the association between visual difficulties and low PA, while unemployment, anxiety, and depression explained this association to a lesser degree.
Our finding that visual impairment is associated with lower levels of PA is in line with previous studies on this topic from HICs [5,6,7] but expands previous knowledge by showing that this association also exists in multiple LMICs. Previous studies have shown that the main barriers to an active lifestyle in people with difficulty seeing are lack of access to recreational and athletic programmes, lack of transport, lack of accessible exercise equipment, lack of help or encouragement in developing suitable and safe physical recreation skills and habits, and activity limitations in walking [10, 11]. Thus, in order to increase levels of PA among people in LMICs, it may be important to address these issues which are often lacking in many LMICs.
Interestingly, we found that interpersonal activities, cognition, and sleep/energy explained >10% of the association between visual difficulties and low PA. First, literature has shown that those who are visually impaired find it difficult to establish new relationships [14, 15], while social isolation and loneliness are associated with lower levels of PA in the general adult population [40]. Second, those who have visual impairment have worse cognitive functioning as they age. For example, one study in older adults found that good visual acuity and wearing glasses correlated with better cognitive function. Indeed, the study concluded that reading glasses can serve as a protective factor against cognitive deterioration associated with sensory (visual) deprivation in old age [16]. Moreover, lower cognitive functioning has been found to be associated with lower level of PA [17]. Finally, those who are visually impaired tend to report poor sleep (short and long sleep duration) compared to the general population [41] and poor sleep is associated with lower levels of PA possibly due to factors such as fatigue [42].
It should be noted that the association between visual impairment and PA was most pronounced among those aged ≥65 years and also among males. Literature suggests that visual impairment in older people is associated with increases in the incidence of falls and hip fractures [43]. Compared to the general older population, this group is 1.7 times more likely to fall, 1.9 times more likely to have multiple falls and 1.3–1.9 times more likely to experience hip fractures [44]. Thus, the more pronounced association observed in older adults may be partly explained by fear of falling [45]. Next, the reason why the association was stronger among males is unclear. However, one can speculate that it may be owing to the difference in gender roles in LMICs. In this setting, the role of domestic duties may lay with the female regardless of visual difficulty status and these domestic duties will likely yield sufficient levels of PA. Further research of a qualitative nature is needed to confirm or refute this hypothesis.
Finally, a moderate level of between-country heterogeneity in the association between visual difficulty and low PA was observed. Although the reasons for this can only be speculated, it is possible that this may be related with differences in environmental barriers to engage in PA, availability of family members to help in physical activities, or the need to be physically active and work due to economic needs despite visual difficulties.
The use of a large predominantly nationally representative dataset across multiple LMICs is a clear strength of the present study. However, findings must be interpreted in light of the study limitations. First, PA and visual difficulty were assessed using self-reported measures, and this may have introduced some level of bias (e.g. recall bias). Future studies using objective data on visual acuity and PA from LMICs are warranted. Second, the study is of a cross-sectional nature and it is not known whether lower levels of PA precede visual difficulty or whether visual difficulty precedes low levels of PA. Finally, it is important to note that our mediation analysis was based on cross-sectional data and thus, it is not possible to differentiate the factors as mediators or confounders. Mediation and confounding are identical statistically and can only be distinguished on conceptual grounds.
In conclusion, we found evidence that especially males and older adults with visual difficulties in LMICs engage in low levels of PA. Addressing issues such as interpersonal activities, cognition, and sleep/energy in people with visual difficulties may increase levels of PA. However, given that the influence of these factors in the association between visual difficulty and low PA was small, addressing other environmental factors are also likely to be important to increase PA levels in this population. Future studies of longitudinal design are warranted to understand the potentially complex interplay of factors assessed in this study and others to obtain a more profound understanding on why people with visual difficulties are less likely to engage in PA. This information is essential for the design of future policies to increase PA in people with visual difficulty.
Summary
What was known before
-
Regular and sustained participation in PA is beneficial for almost every facet of adult health.
-
One group that has consistently been reported to have low levels of PA are those who are visually impaired.
-
Data on the association between visual difficulty and PA from LMICs are scarce.
What this study adds
-
Visual difficulty was associated with a 1.53 (95% CI = 1.38–1.71) times higher odds for low PA with strong associations being observed in males and older adults.
-
Interpersonal activities, cognition, and sleep/energy explained >10% of the association between visual difficulties and low PA.
-
Addressing issues such as interpersonal activities, cognition, and sleep/energy in people with visual difficulties may increase levels of PA.
References
Caspersen CJ, Powell KE, Christenson GM. Physical activity, exercise, and physical fitness: definitions and distinctions for health-related research. Public Health Rep. 1985;100:126–31.
Cunningham C, O’Sullivan R, Caserotti P, Tully MA. Consequences of physical inactivity in older adults: a systematic review of reviews and meta‐analyses. Scand J Med Sci Spor. 2020;30:816–27.
Mok A, Khaw KT, Luben R, Wareham N, Brage S. Physical activity trajectories and mortality: population based cohort study. BMJ .2019;365:l2323.
World Health Organization. Global recommendations on physical activity for health. 2020. https://www.who.int/dietphysicalactivity/factsheet_recommendations/en/ Accessed July, 2020.
Smith L, Timmis MA, Pardhan S, Latham K, Johnstone J, Hamer M. Physical inactivity in relation to self-rated eyesight: cross-sectional analysis from the English Longitudinal Study of Ageing. BMJ Open Ophthalmol. 2017;1:e000046.
Smith L, Jackson SE, Pardhan S, López-Sánchez GF, Hu L, Cao C, et al. Visual impairment and objectively measured physical activity and sedentary behaviour in US adolescents and adults: a cross-sectional study. BMJ Open. 2019;9:e027267.
López-Sánchez GF, Grabovac I, Pizzol D, Yang L, Smith L. The association between difficulty seeing and physical activity among 17,777 adults residing in Spain. Int J Environ Res Public Health. 2019;16:4267.
Willis JR, Jefferys JL, Vitale S, Ramulu PY. Visual impairment, uncorrected refractive error, and accelerometer-defined physical activity in the United States. Arch Ophthalmol. 2012;130:329–35.
Freeman EE, Roy-Gagnon MH, Samson E, Haddad S, Aubin MJ, Vela C, et al. The global burden of visual difficulty in low, middle, and high income countries. PloS One. 2013;8:e63315.
Capella-McDonnall M. The need for health promotion for adults who are visually impaired. J Vis Impair Blind. 2007;101:133–45.
Phoenix C, Griffin M, Smith B. Physical activity among older people with sight loss: a qualitative research study to inform policy and practice. Public Health. 2015;129:124–30.
Harrabi H, Aubin MJ, Zunzunegui MV, Haddad S, Freeman EE. Visual difficulty and employment status in the world. PloS One. 2014;9:e88306.
Nollett C, Ryan B, Bray N, Bunce C, Casten R, Edwards RT, et al. Depressive symptoms in people with vision impairment: a cross-sectional study to identify who is most at risk. BMJ Open. 2019;9:e026163.
Fichten CS, Goodrick G, Amsel R, McKenzie SW. Reactions toward dating peers with visual impairments. Rehabil Psychol. 1991;36:163.
Salminen AL, Karhula ME. Young persons with visual impairment: challenges of participation. Scand J Occup Ther 2014;21:267–76.
Spierer O, Fischer N, Barak A, Belkin M. Correlation between vision and cognitive function in the elderly: a cross-sectional study. Medicine .2016;95:e2423.
Jedrziewski MK, Lee VM, Trojanowski JQ. Physical activity and cognitive health. Alzheimer’s Dement. 2007;3:98–108.
Nuevo R, Chatterji S, Verdes E, Naidoo N, Arango C, Ayuso-Mateos JL. The continuum of psychotic symptoms in the general population: a cross-national study. Schizophr Bull. 2012;38:475–85.
Craig CL, Marshall AL, Sjöström M, Bauman AE, Booth ML, Ainsworth BE, et al. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sport Exer. 2003;35:1381–96.
Choi HG, Lee MJ, Lee SM. Visual impairment and risk of depression: a longitudinal follow-up study using a national sample cohort. Sci Rep. 2018;8:2083.
Azevedo Da Silva M, Singh-Manoux A, Brunner EJ, Kaffashian S, Shipley MJ, Kivimäki M, et al. Bidirectional association between physical activity and symptoms of anxiety and depression: the Whitehall II study. Eur J Epidemiol. 2012;27:537–46.
McCarty CA, Burgess M, Keeffe JE. Unemployment and under-employment in adults with vision impairment: the RVIB employment survey. Aust N. Z J Ophthalmol. 1999;27:190–3.
Ali SM, Lindstrom M. Psychosocial work conditions, unemployment, and leisure-time physical activity: a population-based study. Scand J Public Health. 2006;34:209–16.
Daly M, McMinn D, Allan JL. A bidirectional relationship between physical activity and executive function in older adults. Front Hum Neurosci. 2014;8:1044.
Zheng DD, Swenor BK, Christ SL, West SK, Lam BL, Lee DJ. Longitudinal associations between visual impairment and cognitive functioning: the salisbury eye evaluation study. JAMA Ophthalmol. 2018;136:989–95.
Bassey E, Ellison C, Walker R. Social capital, social relationships and adults with acquired visual impairment: a Nigerian perspective. Disabil Rehabil. 2019;41:1169–76.
Koyanagi A, Stubbs B, Smith L, Gardner B, Vancampfort D. Correlates of physical activity among community-dwelling adults aged 50 or over in six low- and middle-income countries. PLoS One. 2017;12:e0186992.
Vancampfort D, Stubbs B, Smith L, Hallgren M, Firth J, Herring MP, et al. Physical activity and sleep problems in 38 low- and middle-income countries. Sleep Med. 2018;48:140–7.
Dirks C, Grunewald D, Young P, Heidbreder A. Pilot study to investigate sleep disorders in the blind and persons with relevant visual impairment. Ophthalmologe. 2019;116:435–40.
Koyanagi A, Stickley A. The association between sleep problems and psychotic symptoms in the general population: a global perspective. Sleep. 2015;38:1875–85.
Wong KO, Hunter Rowe B, Douwes J, Senthilselvan A. Asthma and wheezing are associated with depression and anxiety in adults: an analysis from 54 countries. Pulm Med. 2013;2013:929028.
Loerbroks A, Herr RM, Subramanian S, Bosch JA. The association of asthma and wheezing with major depressive episodes: an analysis of 245 727 women and men from 57 countries. Int J Epidemiol. 2012;41:1436–44.
Cifuentes M, Sembajwe G, Tak S, Gore R, Kriebel D, Punnett L. The association of major depressive episodes with income inequality and the human development index. Soc Sci Med. 2008;67:529–39.
Stubbs B, Koyanagi A, Schuch F, Firth J, Rosenbaum S, Gaughran F, et al. Physical activity levels and psychosis: a mediation analysis of factors influencing physical activity target achievement among 204 186 people across 46 low- and middle-income countries. Schizophr Bull. 2017;43:536–45.
Rose GA. The diagnosis of ischaemic heart pain and intermittent claudication in field surveys. Bull World Health Organ. 1962;27:645–58.
Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21:1539–58.
Breen R, Karlson KB, Holm A. Total, direct, and indirect effects in logit and probit models. Sociol Methods Res. 2013;42:164–91.
Stubbs B, Koyanagi A, Veronese N, Vancampfort D, Solmi M, Gaughran F, et al. Physical multimorbidity and psychosis: comprehensive cross sectional analysis including 242,952 people across 48 low- and middle-income countries. BMC med. 2016;14:189.
Koyanagi A, Vancampfort D, Carvalho AF, DeVylder JE, Haro JM, Pizzol D, et al. Depression comorbid with tuberculosis and its impact on health status: cross-sectional analysis of community-based data from 48 low- and middle-income countries. BMC med. 2017;15:209.
Kobayashi LC, Steptoe A. Social isolation, loneliness, and health behaviors at older ages: longitudinal cohort study. Ann Behav Med. 2018;52:582–93.
Ramos AR, Wallace DM, Williams NJ, Spence DW, Pandi-Perumal SR, Zizi F, et al. Association between visual impairment and sleep duration: analysis of the 2009 National Health Interview Survey (NHIS). BMC ophthalmol. 2014;14:115.
Štefan L, Sporiš G, Krističević T, Knjaz D. Associations between sleep quality and its domains and insufficient physical activity in a large sample of Croatian young adults: a cross-sectional study. BMJ Open. 2018;8:e021902.
Crews JE, Campbell VA. Vision impairment and hearing loss among community-dwelling older Americans: implications for health and functioning. Am J Public Health. 2004;94:823–9.
Legood R, Scuffham P, Cryer C. Are we blind to injuries in the visually impaired? A review of the literature. Inj Prev. 2002;8:155–60.
Jefferis BJ, Iliffe S, Kendrick D, Kerse N, Trost S, Lennon LT, et al. How are falls and fear of falling associated with objectively measured physical activity in a cohort of community-dwelling older men? BMC geriatr. 2014;14:114.
Funding
Dr. Guillermo Felipe López-Sánchez. Seneca Foundation – Agency for Science and Technology of the Region of Murcia, Spain. [20390/PD/17].
Author information
Authors and Affiliations
Contributions
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Smith, L., Pardhan, S., Gorely, T. et al. Physical activity and visual difficulties in 36 low- and middle-income countries. Eye 36, 585–593 (2022). https://doi.org/10.1038/s41433-021-01439-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41433-021-01439-8
