
Abstract
Background
Little is known about the association between cataract and multimorbidity. Therefore, the aim of the present study was to examine the relationship between cataract and chronic conditions and multimorbidity in a large representative sample of Spanish adults.
Methods
This study used data from the Spanish National Health Survey 2017, a cross-sectional sample of 23,089 adults aged ≥15 years from Spain [54.1% female; mean (standard deviation) age 53.4 (18.9) years]. Cataract and 30 other physical and mental chronic conditions were self-reported. Multimorbidity was defined as the presence of at least two physical and/or mental chronic conditions (excluding cataract). Control variables included sex, age, marital status, education, smoking, and alcohol consumption. Multivariable logistic and negative binomial regression analyzes were conducted to assess associations.
Results
The prevalence of cataract and multimorbidity was 12.5% and 56.5%, respectively. All chronic conditions were significantly more frequent in individuals with than in those without cataract. Overall, there was a positive relationship between cataract and multimorbidity [odds ratio (OR) = 2.77; 95% confidence interval (CI): 2.39–3.21]. In addition, cataract was significantly associated with the number of chronic conditions in the whole population [incidence rate ratio (IRR) = 1.34; 95% CI: 1.29–1.38].
Conclusions
Cataract is positively associated with chronic conditions and multimorbidity in adults. Interventions specifically designed for those with cataract to reduce or manage co-occurring chronic conditions and multimorbidity are urgently required.
Similar content being viewed by others


Introduction
Cataract is defined as clouding of the lens of the eye which prevents clear vision [1]. Importantly, cataract is responsible for 51% of world blindness [2]. Worldwide women have a higher cataract burden than men [3], and most cases of cataract are related to the ageing process [4]. However, it should be noted that congenital forms of cataract also exist and that cataract can also develop as a consequence of eye injury, inflammation, and other diseases, such as rubella [2].
Multimorbidity may be defined as the simultaneous occurrence of two or more chronic diseases in one person and can include both physical and mental health complications. Ageing populations and an increase in chronic conditions mean that the number of people with multiple health conditions is set to rise [5]. Indeed, it has been found that in developed countries more than 40% of the population have at least one chronic condition and ~25% have greater than one condition [6]. Importantly, multimorbidity is associated with high mortality [7], reduced functional status [8], and increased use of both inpatient and ambulatory health care [9, 10]. Finally, previous studies have shown that multimorbidity tends to be more prevalent in women than men [11]. This difference might be related to biological, sociocultural, environmental, or economic factors [12].
One previous study investigated the relationship between visual impairment per se and multimorbidity in a Spanish population and found that arthritis, stroke, and the co-occurrence of various chronic physical diseases were associated with higher visual impairment [13]. Moreover, visual impairment was associated with higher prevalence of depression and poorer cognitive function [13]. Other studies have found similar findings in other countries (e.g., the USA) [14]. Visual impairment is defined as partial sight or blindness in the better seeing eye [15], and can be a consequence of many different eye conditions (e.g., cataract, macular degeneration, retinopathy, etc.). To inform practice and targeted interventions to reduce or manage multimorbidity it would be beneficial to investigate the relationship between specific eye conditions (such as cataract) and multimorbidity. It should be noted that some research has been carried out to identify common comorbidities in those who suffer from cataracts per se. For example, in a sample of 773 cataract surgical patients angina, previous myocardial infarct, diabetes and hypertension were found to be the most common comorbidities [16].
The aim of the present study was to examine the relationship between cataract and chronic conditions and multimorbidity (at least two physical and/or mental chronic conditions) in a large representative sample of Spanish adults. Moreover, owing to the higher prevalence of cataract and multimorbidity in women it is important to also investigate sex-specific associations. Finally, it is important to carry out age-stratified analyzes owing to cataracts mainly being present in older adults, resulting from aging of the tissue of the eye lens. However, younger adults can also develop cataract, resulting from pathways such as injury, diabetes, smoking, previous eye surgery, amongst others.
Methods
The survey
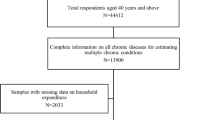
Data from the Spanish National Health Survey 2017 were analysed. This survey was undertaken in Spain between October 2016 and October 2017. Details of the survey method have been already published [17]. In brief, for the data collection, a stratified three-stage sampling was used in which the census sections were first considered, then the family dwellings, and then an adult (15 years or more) was selected within each dwelling. The dwellings were selected by systematic sampling and to select the person who had to complete the Adult Questionnaire, the random Kish method was used. The sample was representative of the adult population residing in Spain and consisted of 23,089 adults aged 15–103 years. The method of data collection used was computer-assisted personal interviewing, conducted in the homes of the selected participants. The interviewers, previously trained, completed the questionnaires with the information provided by the participants. All of them signed an informed consent form before responding to the survey questions. This research was conducted in accordance with the Declaration of Helsinki of 1961 (revised in Tokyo in 1989 and in Edinburgh in 2000).
Cataract (exposure)
The interviewer asked the participants the following question: “Have you ever been diagnosed with cataracts?” Those who answered affirmatively to the question were considered to have cataract. The interviewer was also in charge of solving the possible doubts that the participants had. Previous research has confirmed the validity and high accuracy of self-reported diagnosis of cataract [18].
Multimorbidity (outcome)
Multimorbidity was defined as the presence of two or more chronic conditions (excluding cataract). The interviewer asked the participants the following question: “Have you ever been diagnosed with ‘chronic condition’?” and read a list of chronic conditions. Those who answered affirmatively to the question were considered to have the specific chronic condition. The interviewer was also in charge of solving the possible doubts that the participants had. Previous research has confirmed the validity and high accuracy of self-reported diagnosis of chronic conditions [19]. Chronic conditions included obesity, hypertension, myocardial infarction, angina pectoris, and other coronary diseases, other cardiac diseases, varicose veins of lower extremities, osteoarthritis, chronic neck pain, chronic low back pain, chronic allergy (excluding allergic asthma), asthma (including allergic asthma), chronic bronchitis, emphysema or chronic obstructive pulmonary disease (COPD), diabetes, peptic ulcer disease, urinary incontinence, hypercholesterolemia, chronic skin disease, chronic constipation, liver cirrhosis and other hepatic disorders, depression, anxiety disorder, other psychiatric disorders, stroke, migraine and other frequent headaches, hemorrhoids, cancer, osteoporosis, thyroid disease, renal disease, and injury.
Control variables
The selection of the control variables was based on the past literature [20]. Sociodemographic variables included sex, age, marital status, and education. Marital status was categorized as married and not married (single/widowed/divorced/separated). Education was based on the highest educational level achieved and was categorized as ≤primary, secondary, and ≥tertiary. Smoking status was self-reported and categorized as never, past and current smoking. Alcohol consumption in the last 12 months was self-reported and categorized as yes (any) and no (none).
Statistical analysis
The statistical analysis was performed with R 3.5.2 (The R Foundation) [21]. Differences in the sample characteristics and in the prevalence of chronic conditions by cataract status were assessed by chi-squared tests for all variables except age (t-test), while effect size was calculated using the phi coefficient. The relationship of cataract (independent variable) with multimorbidity and the number of chronic conditions (dependent variables) was assessed using multivariable logistic regression models and multivariable negative binomial regression models, respectively. Multivariable negative binomial regression models were used instead of multivariable Poisson regression models because the number of chronic conditions was overdispersed (i.e., conditional variance exceeded conditional mean). The associations were investigated in the overall population and in sex- (i.e., men, women) and age- (i.e., age ≤ 40 years, age 41–65 years, age > 65 years) stratified samples. Interaction analyzes were conducted by including the product term of cataract × sex or cataract × age into the regression models. Independent variables were included in the models as categorical variables with the exception of age, which was included as a continuous variable. Multimorbidity and the number of chronic conditions were included in the models as dichotomous and count variables. Models were adjusted for sex (apart from the sex-stratified analyzes), age, marital status, education, smoking, and alcohol consumption. There were missing data only for the following variables: marital status (n = 39, 0.17%), smoking (n = 22, 0.10%), alcohol consumption (n = 26, 0.11%), and obesity (n = 1070, 4.63%). Complete-case analysis was carried out. The results from the logistic regression analyzes are presented as odds ratios (ORs) and 95% confidence intervals (CIs), while the results from the negative binomial regression analyzes are presented as incidence rate ratios (IRRs) and 95% CIs. CIs and p values were corrected using the Benjamini–Yekutieli and the Benjamini–Hochberg adjustment method, respectively. The level of statistical significance was set at p < 0.05.
Results
This study included 23,089 individuals residing in Spain [54.1% female; mean (standard deviation) age 53.4 (18.9) years; Table 1]. The prevalence of cataract and multimorbidity was 12.5% and 56.5%, respectively. Female gender, single/widowed/divorced/separated, ≤primary education, never smoking, and no alcohol consumption were more frequent in participants with than in those without cataract, while age was significantly higher in the cataract than in the no cataract group. All chronic conditions were significantly more frequent in individuals with than in those without cataract, and size effects were the highest for osteoarthritis (phi coefficient = 0.32), hypertension (0.27), and urinary incontinence (0.24; Table 2). Finally, the results of the regression models are displayed in Table 3. Overall, there was a positive association between cataract and multimorbidity (OR = 2.77; 95% CI: 2.39–3.21), and this association was significant in the different sex and age subgroups. In addition, cataract was significantly associated with the number of chronic conditions in the whole population (IRR = 1.34; 95% CI: 1.29–1.38), and all sensitivity analyzes were significant. Finally, there was a significant interaction between cataract and age in both the logistic and the negative binomial regression models, with the relationship between cataract and the number of chronic conditions being more pronounced in participants aged ≤40 years (IRR = 2.16; 95% CI: 1.23–3.79).
Discussion
To the best of our knowledge this is the first study to investigate the relationship between cataract and multimorbidity. The present study found that the prevalence of cataract was 12.5%, while the prevalence of multimorbidity was 56.5% in the general population. Importantly, all chronic conditions were more prevalent in those participants with cataract compared with those without. Those with cataract were found to be at a 2.77 higher odds of experiencing multimorbidity than those without. Moreover, the present study found that the number of chronic diseases increases by a factor of 1.34 in patients with cataract compared with those without cataract. Taken together these findings suggest that those with cataract residing in Spain have a poorer health profile than those without cataract.
Findings from the present study are in agreement with other previous studies investigating visual impairment per se [13, 14], and these studies found those with visual impairment are at greater risk of several chronic conditions and multimorbidity. Moreover, the present findings add to this body of knowledge by showing that such associations also exist specifically in relation to cataract. Several plausible pathways may explain the observed relationships. First, those with several chronic conditions, such as cardiovascular conditions, diabetes, or arthritis, may have cumulative risk for cataract due to vascular, neurodegenerative, biochemical, or inflammatory pathways [13, 22]. Second, those with cataract my exhibit a higher prevalence of harmful lifestyle behaviors. For example, it has been shown that those who are visually impaired have much lower levels of physical activity than those without [15, 23, 24]. Moreover, a diet with nutrient deficiencies is associated with several chronic conditions [25, 26] and potentially cataract [27]. Third, those with cataract are likely to experience a lower quality of life (QOL) [28] and QOL has been found to be associated with several physical and mental health complications [29,30,31]. Moreover, poor ocular health is associated with social isolation [32] and loneliness [33], while social isolation [34] and loneliness [35] are risk factors for multimorbidity. In line with this hypothesis, cataract may be a risk factor for several mental conditions such as depression [36]. Fourth, cataract increases the risk of falls [37], and falls are associated with fractures, pain, and functional decline [38]. Finally, cataract and multimorbidity may also share common risk factors that were not assessed in this study (e.g., income).
One finding of the present study that needs to be interpreted with caution is the lack of significant interaction between cataract and sex in the cataract–multimorbidity relationship. Indeed, previous work has shown that the prevalence of cataract and the prevalence of multimorbidity is higher in females than in males [3, 11]. This difference might be related to biological, sociocultural, environmental, or economic factors [12]. It may also be owing to the fact that generally QOL is lower in older women than men [39]. Taking these data together, further research is now required to elucidate the question about the role played by sex in the association between cataract and multimorbidity.
Finally, the high prevalence of cataract (12.5%) in the present study should also be noted. Owing to such a high prevalence, interventions to either prevent cataract or allow for early detection are warranted in Spain. To aid in the prevention of cataract development, interventions should focus on smoking cessation, reducing sunlight exposure by wearing ultraviolet A and B protective eyewear and wide-brimmed hats, optimal management of diabetes, and consuming a balanced diet [40]. To aid in early detection of cataracts, Spanish adults should be encouraged to undergo regular eye examinations.
This is the first study to investigate the relationship between cataract, chronic conditions, and multimorbidity. The large sample size and the stratification by sex and age are clear strengths. However, findings from this study must be interpreted in light of its limitations. Both cataract and all chronic conditions were self-reported, potentially introducing bias. Moreover, it is not known whether the person was operated on for cataracts. Indeed, if the person was operated on it is highly likely that the person no longer has visual problems. In addition, the survey did not include information about specific diagnostic criteria, while there was a lack of data on the onset, severity, and duration of the diseases, underlying the need for further surveys with more detailed questions. Finally, the cross-sectional nature of the study means the direction of observed associations is not known. Therefore, future longitudinal studies are warranted to clarify the direction of causality. Nevertheless, the mere coexisting presence of cataract with chronic conditions and multimorbidity highlights an important health priority and informs targeted intervention.
In conclusion, in this large sample of Spanish residents, those with cataract were at greater risk of chronic physical and mental health complications and multimorbidity. Interventions specifically designed for those with cataract to reduce or manage co-occurring chronic conditions and multimorbidity are urgently required. Such interventions may consist of group exercise to favor physical activity, adaptation of the home environment to reduce fall risk, and use of low vision devices to improve social participation. Finally, ophthalmologists should be aware that individuals with cataracts are at high risk of multimorbidity.
Summary
What was known before
-
Little is known about the association between cataract and multimorbidity.
-
To the best of our knowledge this is the first study to investigate the relationship between cataract and multimorbidity.
What this study adds
-
Cataract is positively associated with chronic conditions and multimorbidity in adults.
-
Interventions specifically designed for those with cataract to reduce or manage co-occurring chronic conditions and multimorbidity are urgently required.
References
Mayo Clinic. Cataracts. https://www.mayoclinic.org/diseases-conditions/cataracts/symptoms-causes/syc-20353790. Accesed 5 Dec 2019.
World Health Organization. Priority eye diseases. https://www.who.int/blindness/causes/priority/en/index1.html. Accesed 5 Dec 2019.
Lou L, Ye X, Xu P, Wang J, Xu Y, Jin K, et al. Association of sex with the global burden of cataract. JAMA Ophthalmol. 2018;136:116–21. https://doi.org/10.1001/jamaophthalmol.2017.5668.
World Health Organization. Blindness and vision impairment: key activities. https://www.who.int/blindness/key-activities/en/. Accesed 5 Dec 2019.
Mercer S, Furler J, Moffat K, Fischbacher-Smith D, Sanci L, editors. Multimorbidity: technical series on safer primary care. Geneva: World Health Organization; 2016.
Barnett K, Mercer SW, Norbury M, Watt G, Wyke S, Guthrie B. Epidemiology of multimorbidity and implications for health care, research, and medical education: a cross-sectional study. Lancet. 2012;380:37–43. https://doi.org/10.1016/S0140-6736(12)60240-2.
Gijsen R, Hoeymans N, Schellevis FG, Ruwaard D, Satariano WA, Van den Bos GA. Causes and consequences of comorbidity: a review. J Clin Epidemiol. 2001;54:661–74.
Kadam UT, Croft PR, North Staffordshire GP Consortium Group. Clinical multimorbidity and physical function in older adults: a record and health status linkage study in general practice. Fam Pract. 2007;24:412–9. https://doi.org/10.1093/fampra/cmm049.
Salisbury C, Johnson L, Purdy S, Valderas JM, Montgomery AA. Epidemiology and impact of multimorbidity in primary care: a retrospective cohort study. Br J Gen Pract. 2011;61:e12–21. https://doi.org/10.3399/bjgp11X548929.
Wolff JL, Starfield B, Anderson G. Prevalence, expenditures, and complications of multiple chronic conditions in the elderly. Arch Intern Med. 2002;162:2269–76. https://doi.org/10.1001/archinte.162.20.2269.
Violan C, Foguet-Boreu Q, Flores-Mateo G, Salisbury C, Blom J, Freitag M, et al. Prevalence, determinants and patterns of multimorbidity in primary care: a systematic review of observational studies. PLoS ONE. 2014;9:e102149. https://doi.org/10.1371/journal.pone.0102149.
Alimohammadian M, Majidi A, Yaseri M, Ahmadi B, Islami F, Derakhshan M, et al. Multimorbidity as an important issue among women: results of a gender difference investigation in a large population-based cross-sectional study in West Asia. BMJ Open. 2017;7:e013548. https://doi.org/10.1136/bmjopen-2016-013548.
Garin N, Olaya B, Lara E, Moneta MV, Miret M, Ayuso-Mateos JL, et al. Visual impairment and multimorbidity in a representative sample of the Spanish population. BMC Public Health. 2014;14:815. https://doi.org/10.1186/1471-2458-14-815.
Crews JE, Chou CF, Sekar S, Saaddine JB. The prevalence of chronic conditions and poor health among people with and without vision impairment, aged ≥ 65 years, 2010–2014. Am J Ophthalmol. 2017;182:18–30. https://doi.org/10.1016/j.ajo.2017.06.038.
Smith L, Timmis MA, Pardhan S, Latham K, Johnstone J, Hamer M. Physical inactivity in relation to self-rated eyesight: cross-sectional analysis from the English Longitudinal Study of Ageing. BMJ Open Ophthalmol. 2017;1:e000046. https://doi.org/10.1136/bmjophth-2016-000046.
Pham TQ, Wang JJ, Rochtchina E, Maloof A, Mitchell P. Systemic and ocular comorbidity of cataract surgical patients in a western Sydney public hospital. Clin Exp Ophthalmol. 2004;32:383–7. https://doi.org/10.1111/j.1442-9071.2004.00842.x.
Ministerio de Sanidad, Servicios Sociales e Igualdad & Instituto Nacional de Estadística. Spanish National Health Survey 2017: methodology. https://www.mscbs.gob.es/estadEstudios/estadisticas/encuestaNacional/encuestaNac2017/ENSE17_Metodologia.pdf. Accesed 5 Dec 2019.
Bergmann MM, Byers T, Freedman DS, Mokdad A. Validity of self-reported diagnoses leading to hospitalization: a comparison of self-reports with hospital records in a prospective study of American adults. Am J Epidemiol. 1998;147:969–77. https://doi.org/10.1093/oxfordjournals.aje.a009387.
Martin LM, Leff M, Calonge N, Garrett C, Nelson DE. Validation of self-reported chronic conditions and health services in a managed care population. Am J Prev Med. 2000;18:215–8. https://doi.org/10.1016/S0749-3797(99)00158-0.
Yawson AE, Ackuaku-Dogbe EM, Seneadza NA, Mensah G, Minicuci N, Naidoo N, et al. Self-reported cataracts in older adults in Ghana: sociodemographic and health related factors. BMC Public Health. 2014;14:1–8. https://doi.org/10.1186/1471-2458-14-949.
R Core Team. R: a language and environment for statistical computing. Vienna: R Foundation for Statistical Computing; 2018. https://www.R-project.org/. Accesed 5 Dec 2019.
Sayin N, Kara N, Pekel G. Ocular complications of diabetes mellitus. World J Diabetes. 2015;6:92–108. https://doi.org/10.4239/wjd.v6.i1.92.
López-Sánchez GF, Grabovac I, Pizzol D, Yang L, Smith L. The association between difficulty seeing and physical activity among 17,777 adults residing in Spain. Int J Environ Res Public Health. 2019;16:e4267. https://doi.org/10.3390/ijerph16214267.
Smith L, Jackson SE, Pardhan S, López-Sánchez GF, Hu L, Cao C, et al. Visual impairment and objectively measured physical activity and sedentary behaviour in US adolescents and adults: a cross-sectional study. BMJ Open. 2019;9:e027267. https://doi.org/10.1136/bmjopen-2018-027267.
Rao TS, Asha MR, Ramesh BN, Rao KJ. Understanding nutrition, depression and mental illnesses. Indian J Psychiatry. 2008;50:77–82. https://doi.org/10.4103/0019-5545.42391.
Hu FB. Protein, body weight, and cardiovascular health. Am J Clin Nutr. 2005;82:242S–7S. https://doi.org/10.1093/ajcn/82.1.242S.
Cumming RG, Mitchell P, Smith W. Diet and cataract: the blue mountains eye study. Ophthalmology. 2000;107:450–6. https://doi.org/10.1016/s0161-6420(99)00024-x.
Zhu M, Yu J, Zhang J, Yan Q, Liu Y. Evaluating vision-related quality of life in preoperative age-related cataract patients and analyzing its influencing factors in China: a cross-sectional study. BMC Ophthalmol. 2015;15:160. https://doi.org/10.1186/s12886-015-0150-8.
Aminisani N, Nikbakht H, Jafarabadi MA, Shamshirgaran SMDepression. anxiety, and health related quality of life among colorectal cancer survivors. J Gastrointest Oncol. 2017;8:81–8. https://doi.org/10.21037/jgo.2017.01.12.
Van Jaarsveld CH, Sanderman R, Ranchor AV, Ormel J, Van Veldhuisen DJ, Kempen GI. Gender-specific changes in quality of life following cardiovascular disease: a prospective study. J Clin Epidemiol. 2002;55:1105–12. https://doi.org/10.1016/s0895-4356(02)00506-1.
Öztürk A, Şimşek TT, Yümin ET, Sertel M, Yümin M. The relationship between physical, functional capacity and quality of life (QoL) among elderly people with a chronic disease. Arch Gerontol Geriatr. 2011;53:278–83. https://doi.org/10.1016/j.archger.2010.12.011.
Coyle CE, Steinman BA, Chen J. Visual acuity and self-reported vision status: their associations with social isolation in older adults. J Aging Health. 2017;29:128–48. https://doi.org/10.1177/0898264315624909.
Brunes A, Hansen MB, Heir T. Loneliness among adults with visual impairment: prevalence, associated factors, and relationship to life satisfaction. Health Qual Life Outcomes. 2019;17:24. https://doi.org/10.1186/s12955-019-1096-y.
Singer L, Green M, Rowe F, Ben-Shlomo Y, Morrissey K. Social determinants of multimorbidity and multiple functional limitations among the ageing population of England, 2002–2015. SSM Popul Health. 2019;8:100413. https://doi.org/10.1016/j.ssmph.2019.100413.
Jessen MAB, Pallesen AVJ, Kriegbaum M, Kristiansen M. The association between loneliness and health—a survey-based study among middle-aged and older adults in Denmark. Aging Ment Health. 2018;22:1338–43. https://doi.org/10.1080/13607863.2017.1348480.
Palagyi A, Rogers K, Meuleners L, McCluskey P, White A, Ng JQ, et al. Depressive symptoms in older adults awaiting cataract surgery. Clin Exp Ophthalmol. 2016;44:789–96. https://doi.org/10.1111/ceo.12800.
Krishnaiah S, Ramanathan RV. Impact of blindness due to cataract in elderly fallers: findings from a cross-sectional study in Andhra Pradesh, South India. BMC Res Notes. 2018;11:773. https://doi.org/10.1186/s13104-018-3883-7.
Terroso M, Rosa N, Marques AT, Simoes R. Physical consequences of falls in the elderly: a literature review from 1995 to 2010. Eur Rev Aging Phys Act. 2014;11:51–9. https://doi.org/10.1007/s11556-013-0134-8.
Hajian-Tilaki K, Heidari B, Hajian-Tilaki A. Are gender differences in health-related quality of life attributable to sociodemographic characteristics and chronic disease conditions in elderly people? Int J Prev Med. 2017;8:95. https://doi.org/10.4103/ijpvm.IJPVM_197_16.
American Optometric Association. Nutrition and cataracts. https://www.aoa.org/patients-and-public/caring-for-your-vision/nutrition/nutrition-and-cataracts. Accesed 21 Jan 2020.
Funding
GFL-S is funded by the Seneca Foundation—Agency for Science and Technology of the Region of Murcia, Spain (20390/PD/17). AK’s work is supported by the PI15/00862 project, integrated into the National R + D + I and funded by the ISCIII—General Branch Evaluation and Promotion of Health Research—and the European Regional Development Fund (ERDF-FEDER). These funders had no role in the study design, collection, analysis, and interpretation of the data; writing of the report; and the decision to submit the article for publication.
Author information
Authors and Affiliations
Contributions
LJ contributed to the design of the study, managed the literature searches, undertook the statistical analysis, and contributed to the correction of the paper. GFL-S contributed to the design of the study, managed the literature searches, wrote the first draft of the paper, and contributed to the correction of the paper. LY, JMH, JIlS, NV, PS, TG, and AK contributed to the design of the study and the correction of the paper. LS contributed to the design of the study, managed the literature searches, wrote the first draft of the paper, and contributed to the correction of the paper. All authors contributed to and have approved the final paper.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Jacob, L., López-Sánchez, G.F., Yang, L. et al. Associations between cataract and multimorbidity: a cross-sectional study of 23,089 adults from Spain. Eye 35, 791–798 (2021). https://doi.org/10.1038/s41433-020-0962-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41433-020-0962-5
This article is cited by
-
What makes a good survey?
Eye (2023)
