
Abstract
Worldwide, cannabis is one of the most widely used psychoactive substances and cannabis use has been implicated in poorer performance in several cognitive domains, including working memory (WM). However, the neural mechanisms underlying these WM decrements are not well understood and the current study investigated the association of cannabis involvement with WM performance and associated neural activation in the Human Connectome Project (N = 1038). Multiple indicators of cannabis involvement were examined in relation to behavioral performance and brain activity in a visual N-back task using functional magnetic resonance imaging. A positive urine drug screen for tetrahydocannabinol (THC+ status), the principal psychoactive constituent in cannabis, was associated with worse WM performance and differential brain response in areas previously linked to WM performance. Furthermore, decreases in blood-activation-level-dependent (BOLD) signal in WM task-positive brain regions and increases in task-negative regions mediated the relationship between THC+ status and WM performance. In contrast, WM performance and BOLD response during the N-back task were not associated with total lifetime cannabis use, age of first use, or other indicators of involvement, suggesting that the effects of cannabis on WM were short-term residual effects, rather than long-term persistent effects. These findings elucidate differential influences of cannabis involvement on neurocognition and have significant potential implications for occupational performance in diverse settings.
Similar content being viewed by others

Introduction
Worldwide, cannabis is one of the most widely used psychoactive substances [1] and, among a number of associated harms, there is increasing evidence that cannabis use is associated with poorer neuropsychological functioning in a number of domains [2,3,4]. One such domain is working memory (WM), which refers to the brain’s capacity to hold and manipulate information. Specific daily activities that are reliant on WM include language comprehension [5], logical reasoning [6, 7], and self-regulation [8]. A recent meta-analysis found worse WM performance in current cannabis users (N = 2152) with a small effect size (d = .22, p < 0.001), with deficits existing in both adults and adolescents [9]. However, not all studies in this review found worse WM performance; indeed, studies that required greater than 72 h of abstinence from cannabis did not show a significant relationship between cannabis use and WM. Additionally, age of initiation of cannabis use was not related to WM performance. Thus, while there is strong evidence that recent use of cannabis may be a reliable predictor of WM deficits, it is unclear whether past use of cannabis has lasting effects on WM.
While there is a relatively robust literature suggesting that recent cannabis use is associated with decrements in WM performance, the literature on the neural mechanisms of this relationship is much less developed. Some studies have found cannabis users have greater neural activation in regions known to underpin WM ability generally [10, 11]. Other studies have not detected differences in WM-related brain activity [12], including the largest and most recent study to date (N = 73), which did not detect any differences in WM brain response to an N-back WM task [13]. Interestingly, none of these studies found differences in WM performance between cannabis users and controls, likely reflecting issues of power and the exclusion of very poorly performing participants.
There are several possible reasons for these inconsistent findings, but the small sample sizes in the existing literature suggest that low statistical power may be contributing to unreliable results, an increasingly common concern in fMRI research (i.e., power failure, cluster failure [14]). This is compounded by the fact that differences in neural activity are likely small in effect size, mirroring the small differences seen in WM performance in non-MRI studies. Another potential confound within previous fMRI studies is different operationalization of cannabis use, with some studies classifying it by current or recent use (e.g., [10, 13]) and others by previous heavy use among currently abstinent individuals (e.g., [12]). Consequently, it is unclear what aspects of cannabis use are most important to WM decrements and their associated neural correlates. As noted, a recent meta-analysis suggested that deficits may only be detectable for a relatively short period immediately after cannabis use [9]. However, there are also systematic reviews suggesting that effects on some cognitive functions are longer lasting, specifically following heavy use or early initiation of use [15].
To address these issues, the current study examined the association of behavioral performance and neural response during a WM task with several indicators of cannabis involvement in the context of the Human Connectome Project (HCP [16]; a large-scale open-science investigation of brain connectomics in a cohort of generally normative adults, age 22–35). It was hypothesized that differences in WM performance would be present in recent cannabis users and that there may also be differences associated with lifetime use and age of initiation of use. It was also hypothesized that these differences would be explained by differences in neural activation while engaging WM during an fMRI N-back task. Cannabis variables investigated included ever having used cannabis at all (i.e., defined as having used cannabis one or more time in life), age of initiation (i.e., age at which first cannabis use occurred), total lifetime use (i.e., self-reported number of times used cannabis), lifetime problematic cannabis use (i.e., meeting the criteria for cannabis use disorder at any point in life, CUD Dx), and recent cannabis use (i.e., a positive urine THC screen, THC+).
Methods
Participant characteristics
Participants were recruited with the assistance of the Missouri Department of Health and Senior Services Bureau of Vital Records [16]. Participants were contacted by phone, provided information about the study, and gave informed consent for an initial phone interview. Then participants meeting the inclusion criteria were invited for a 2-day data collection procedure with informed consent obtained on the first day. No instructions were given to participants regarding abstaining from cannabis or other drug use prior to the visit. Participants were monetarily compensated for completion of study procedures. All procedures were approved by the institutional review board of Washington University (IRB number 201204036). Only HCP participants with complete data for the N-back task (fMRI and behavioral) and all covariates were included, resulting in a sample of 1038 participants (Table 1).
Measures
Cannabis use variables
Five cannabis use variables were tested for their relationship with WM performance and neural response to the WM task: (1) ever used—having used cannabis once or more in their lifetime; (2) age of first use—the age at which an individual first used cannabis; (3) times used—estimated total number of cannabis use episodes across the lifespan; (4) lifetime cannabis use disorder (CUD Dx)—ever met diagnostic criteria for cannabis use disorder; and (5) presence of circulating cannabis metabolites—positive urine drug screen for tetrahydocannabinol (i.e., THC+ status). See Supplemental Methods for information about the HCP measures from which these variables were drawn.
N-back working memory task
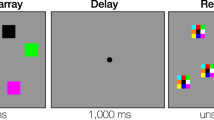
Two 5-min imaging runs of the N-back fMRI paradigm were completed. In these, participants were presented with trial blocks of images consisting of places, tools, faces, and body parts. Within each imaging run, the four different stimulus types were presented in separate blocks. Each of two runs contained eight N-back task blocks (27.5 s each), consisting of four 0-back blocks and four 2-back blocks, and four resting/eye fixation blocks (15 s each). A 2.5-s cue was presented at the beginning of each block to inform participants which task followed (i.e., 0-back or 2-back); ten trials of 2.5 s each were included in each block. On each trial, the stimulus was presented for 2 s, followed by a 500 ms inter-trial interval. During 0-back task blocks, participants were presented with cues serially and instructed to identify any stimuli that matched a predetermined target. During 2-back task blocks, the subject was required to identify stimuli that matched the stimulus presented two trials prior. The paradigm used is described further in ref. [17]. Additionally, the fMRI protocol is described in Supplemental Methods.
Data processing and analysis
Candidate covariates included age, sex, income, education, race, ethnicity, current and heaviest alcohol use, current tobacco use, cigarette smoking history, body mass index (BMI), current and past use of illicit drugs (other than cannabis), current symptoms of depression, current symptoms of anxiety, and current symptoms of attention deficit hyperactivity disorder. The measures used to derive these covariates are reported in Supplemental Methods. Covariates were evaluated using t test/χ2 tests to determine if differences between cannabis users and nonusers were present and using simultaneous multiple linear regression to determine if a significant relationship to WM accuracy was present, with those demonstrating a relationship to WM performance or cannabis use being used in all analyses (i.e., all candidate covariates except for ethnicity). Additionally, given that the HCP dataset includes a subset of twin pairs, twin status was accounted for using covariates for monozygotic twin status and dizygotic twin status, as was done by a previous manuscript investigating cannabis use effects on the brain in the HCP dataset [18]. Cannabis use variables were tested as predictors of WM accuracy beyond these covariates, one-by-one, in second levels of hierarchical multiple regression models. Then, to confirm that relationships between cannabis use variables and WM accuracy were not due to collinearity among the cannabis use variables all cannabis variables were entered into a regression model simultaneously. In these analyses, multiple comparisons were accounted for using a Bonferroni correction for the five cannabis use variables being tested; this resulted in a threshold of p < 0.01 being used. The fMRI analyses were then conducted on cannabis use variables that were significantly associated with WM accuracy.
Preprocessed fMRI data were downloaded from the HCP website (for details of preprocessing, see ref. [19]). Additional fMRI data processing and analysis were then conducted using Analysis of Functional NeuroImages software (AFNI [20]). Data were spatially smoothed using a 6 mm full width half maximum Gaussian filter. General linear modeling was completed using regressors representing the time course for blocks of each condition (2-back, 0-back, and instruction screens), six nuisance regressors to account for motion, and regressors for linear, quadratic, and cubic trends. Activation during the 2-back WM task was compared to a baseline of activation during the 0-back task, which is a sustained attention task matched on visual, motor, timing, and target frequency characteristics (but not WM demands). Primary regions of interest (Table 3 and Supplementary Figure 1) were based on clusters found in a prior study conducted in the same sample [21] and represent regions in which WM accuracy is most associated with activation during the 2-back (relative to 0-back). To demonstrate that results were generalizable to other samples, analyses were also repeated in separate secondary regions of interest (ROIs) derived from an automated meta-analysis of the term “Working Memory” using Neurosynth (http://neurosynth.org/) on March 6, 2018. In both ROI analyses, neural activation was averaged across all voxels of each ROI in AFNI then exported for further analysis.
Using separate multiple regressions, each region was tested for its association with each cannabis use variable that was associated with WM accuracy. To account for multiple comparisons, false discovery rate of q = 0.05 was used for these fMRI comparisons [22]. Mediational analyses were conducted to test for significant mechanistic relationships (indirect effects) present for the a priori ROIs that may be links between cannabis use and WM performance. Given anticipated collinearity representing the neural networks of the ROIs, principal component analysis was used to reduce the data to network components. Specifically, oblique rotation (direct oblimin, δ = 0) was used based on the presumption of correlated components (i.e., significant anticorrelation between task-positive and task-negative networks); components were extracted based on eigenvalue >1 and scree plot discontinuity. Subsequently, mediation analyses were conducted using the PROCESS macro (model 4 [23]) with the cannabis use variable associated with WM accuracy (THC+) as the independent variable, WM accuracy as the dependent variable, the two fMRI response components as mediators, and the predetermined variables as covariates.
Following ROI analysis, group-level voxelwise GLM analyses were conducted on activation during the 2-back (relative to the 0-back) for each cannabis use variable that was significantly associated with WM accuracy using the AFNI program 3dttest++. A voxelwise false discovery rate of q = 0.05 was used with a cluster forming threshold of 30 voxels. For all group level voxelwise analyses candidate covariates that were significantly associated with cannabis use were used as covariates.
Results
Behavioral analyses
In step one of the hierarchical regression model (Table 2), there were significant associations between 2-back accuracy and all demographic variables (except ethnicity), alcoholic drinks per week, and number of days used tobacco per week (p < 0.05). In step two of the hierarchical model (Table 2), THC+ was significantly associated with 2-back accuracy, but ever used, age of first use, times used, and CUD Dx were not. When all five cannabis variables were entered into a model simultaneously, THC+ remained predictive of WM performance, while other variables remained unrelated (Table 2). As a result, only THC+ was the primary focus of analyses on brain activity during 2-back. Intercorrelations of the cannabis use variables were .315–.796 and are reported in Supplemental Table 1.
Primary ROI analyses
As expected, zero-order correlations among the a priori ROIs were large in magnitude and statistically significant (Supplemental Tables 2 and 3).
Results of regression analyses for individual regions of interest with THC+ are presented in Table 3. In the majority of brain regions tested, THC+ was uniquely predictive of level of brain response to the 2-back task. Specifically, it was negatively associated with regions activated by the 2-back task and positively associated with the bilateral ventromedial prefrontal cortex, which exhibited relative deactivation during the 2-back task.
Principal components analysis revealed two components accounting for approximately 70% of total variance: one associated with task-positive regions and one associated with task-negative regions. The pattern matrix of the principal components analysis is presented in Supplemental Table 4. Activation in the task-positive component was negatively associated with THC+ (β = −0.125, t = −3.808, p < 0.001, R2∆ = 0.012) and activation in the task-negative component was positively associated with THC+ (β = 0.097 t = 2.937, p = 0.003, R2∆ = 0.007). No other cannabis use variables (e.g., ever used, times used, age of first use, and CUD Dx) were associated with either component.
Mediation analyses found significant indirect effects from THC+ to WM accuracy through each of the two components indicating that brain activation was serving as a mediator of the effects of THC+ on WM accuracy (Fig. 1). For the total indirect effect, B = −1.77 [95% CI −2.72 to −0.94]. For the indirect effect of task-positive network: B = −1.12 [95% CI −1.81 to −0.52]. For the indirect effect of task-negative network, B = −0.65 [95% CI −1.18 to −0.21]. After accounting for the effects of neural activation in the two components, the relationship of THC+ to WM performance (i.e., the C′ path) was no longer significant, B = −1.95, t = −1.92, p = 0.06.

Mediation model of effects of recent cannabis use on working memory performance through brain activation during engagement of working memory. Total indirect effect: B = −1.77 [95% CI −2.72 to −0.94]; indirect effect of task-positive network: B = −1.12 [95% CI −1.81 to −0.52]; indirect effect of task-negative network: B = −0.65 [95% CI −1.18 to −0.21]. C′ path represents effect of THC+ on WM accuracy removing the indirect effects
Secondary Neurosynth ROIs
Secondary ROI analysis using the alternate ROIs derived from Neurosynth (shown in Supplemental Fig. 2) resulted in very similar findings as the primary ROI analysis. In Pearson’s correlations, all ten Neurosynth ROIs were significantly associated with each other (Supplemental Table 5). Multiple regression analyses indicated that activation in all ten ROIs were significantly associated with WM performance (Supplemental Table 6). The ten regions composed a single task-positive component (Supplemental Table 7), which was significantly associated with THC+ (β = −0.132, t = −4.07, p < 0.001, R2∆ = 0.014). Mediation modeling showed that this task-positive component mediated the relationship of THC+ on WM performance (Supplemental Figure 3).
Voxelwise analyses
Voxelwise regression analyses of 2-back (relative to 0-back) showed a similar pattern to ROI analyses (Fig. 2; coordinates and cluster extents in Supplementary Table 8). THC+ was associated with similar activation clusters to the regions identified with THC+ effects in ROI analyses, including the middle frontal gyrus, the inferior and superior parietal lobules, and supplementary motor area, as well as deactivation in the ventromedial prefrontal cortex.

THC+ status controlling for age, sex, income, education, race, current and heaviest alcohol use, current tobacco use, cigarette smoking history, body mass index (BMI), current and past use of illicit drugs (other than cannabis), current symptoms of depression, current symptoms of anxiety, and current symptoms of attention deficit hyperactivity disorder, MZ twin status, DZ twin status. a shows axial slices with z coordinates (in RAI) at 17, 30, 45, 56. b shows sagittal slice at x coordinate 0. Blue reflects less activity during 2-back (relative to 0-back) and yellow reflects greater activity during 2-back (relative to 0-back) in THC+ individuals compared to THC− individuals
Discussion
The goal of the current study was to investigate the relationship between five indicators of cannabis involvement and both behavioral and neural indicators of WM. Results indicate that recent cannabis use measured by urinary THC was the only cannabis variable associated with lower WM performance on an N-back WM task. The study also found recent cannabis use measured by urinary THC was associated with less activation during the WM task in the task-positive network (dorsolateral prefrontal cortex, posterior parietal, supplementary motor area, insula) and greater activation in a hub of the task-negative network (ventromedial prefrontal cortex). Overall, the effect sizes were relatively small in absolute magnitude, but exhibited robust statistical significance and were consistent across two different sets of regions of interest and voxelwise analysis. Mechanistic analyses suggest that lower levels of activity in the task-positive network and higher levels of activity in the task-negative network mediated the relationship between recent cannabis use and poorer WM performance.
The findings of decrements in WM performance is consistent with prior literature suggesting that recent cannabis use, but not more distant past use, is associated with poorer WM performance [9]. However, the current results substantially extend the literature by showing that differences in WM performance in recent cannabis users are mediated by differences in brain activity in specific regions known to be most important to successful WM performance. The task-positive network elicited during this task has been widely interpreted as an “executive control network,” as it has been shown repeatedly to activate during tasks requiring WM and other executive functions [24, 25]. Moreover, higher levels of activation of this network while engaging WM ability has been associated with better WM performance [21]. The task-negative network is a resting state network that has been termed the “default mode network,” and is typically more active during periods of low task demand and less active during more difficult, externally focused tasks such as the N-back WM task [26]. In fact, this reduction in activation has been shown to be adaptive to successful performance of these externally focused tasks, with activation in the task-negative network being inversely associated with WM performance [21, 27]. The relationship between these two networks has been described as “intrinsically anticorrelated” with greater activity in one predicting less activity in the other in healthy individuals [28], as was evident in the present study. Broadly speaking, switching from default mode network activity to task-positive networks can be thought of as capacity to efficiently toggle from undirected internally focused mentation to externally focused responding to cognitive demands. Reductions in this anticorrelation have been linked to impaired cognitive ability under diverse conditions including age-induced mild cognitive impairment [29], sleep deprivation [30], and attention deficit hyperactivity disorder [31]. Thus, the location and direction of the effects found in this study are highly consonant with the literature, as the current results suggest that in recent cannabis users not only is activation lower in areas of the brain needed for successful WM performance, but it is higher in the ventromedial prefrontal cortex where activation is disengaged during successful WM performance.
Implications
These findings have substantive implications for potential risk associated with cannabis use. WM has been shown to be one of the strongest predictors of academic and professional success [32], meaning that small, residual consequences of cannabis use on WM may have a discernable impact on academic performance in chronic users in educational settings. Specific academic processes that may rely on WM include reading comprehension [33] and mathematical ability [34]. WM decrements from recent cannabis use may compound existing disorders associated with impairments in WM such as attention deficit hyperactivity disorder [35, 36] and learning disabilities [37, 38].
Another group for whom the current results are relevant is individuals working in high-stake jobs with high WM demands, such as airline pilots, air traffic controllers, first responders, and train and bus operators [39]. In these cases, even a small decrease in neurocognitive function may be extremely consequential. While the Federal Aviation Administration already requires strict drug testing (www.faa.gov), the current results suggest that these requirements and those in other fields with comparable demands and risks are justified, despite, and perhaps especially because of, cannabis’s increasing legalization. Furthermore, the current results are highly relevant considering the increasing utilization of medical cannabis, which can be legally used to treat a variety of conditions in an increasingly large number of jurisdictions. In medical applications, consumption is typically of higher volume and chronic, rather than episodic, making residual effects on cognition potentially more likely and larger in magnitude. Although this remains conjecture, these findings suggest an important side effect of medical cannabis may be residual cognitive and neural effects.
Considerations
Several factors must be considered when evaluating the results of the current study. It is important to remember that the HCP study was designed to be an expansive undertaking to map the human connectome, but was not designed specifically to understand cannabis’s effects on cognition. As such, the HCP employed relatively coarse measurement of cannabis use. Categorically defined urine THC screening (as was used in the variable THC+) is not the optimal way of measuring recent exposure and is influenced by a number of factors; measuring specific levels of THC and other metabolites would likely produce more sensitive results. Also notable is that the HCP sample represents a community sample with levels of cannabis use typical to the population at large, not very heavy cannabis users. However, this is also beneficial, providing an opportunity to measure the effects of cannabis on WM when used as is more typical in the general population. That reduced WM performance and associated brain activity are not limited to the most severe users means the current results are likely to generalize to a larger proportion of cannabis users.
A further consideration is the demographic differences between cannabis users and nonusers, which are reflective of differences in users and nonusers in the population generally. In the current study, those who tested positive for THC differed from those who did not in a number of areas. While these variables were statistically controlled in all analyses, it is still possible that these groups differed in other unmeasured ways, which may influence the differences observed (i.e., “third variable confounds”). Finally, as with any cross-sectional study, causality cannot be definitively ascertained, which limits the degree of certainty that it is recent cannabis use that is driving differences in WM performance and WM-related brain activity. It is possible that the directionality is opposite (WM giving rise to recent cannabis use), although this would be surprising given that none of the other cannabis variables were associated with WM. Nonetheless, the mediation models in particular should be interpreted cautiously given concerns for the potential of bias in cross-sectional mediation models [40, 41].
Conclusions
The current study is the largest neuroimaging study on cannabis and WM to date, with all prior studies having fewer than 100 participants and most fewer than 30. As such, the present study has much higher statistical power, reducing the likelihood of either Type I or Type II errors and permitting inclusion of an extensive list of covariates that may have had confounding influences in previous studies. An additional methodological strength was the HCP’s state-of-the-art fMRI data acquisition and processing pipeline, which allows for higher resolution fMRI data than available in prior studies. The study is the first to delineate differences in WM-related brain function in relation to a number of indicators of cannabis involvement, including both self-report and a urinary biomarker. Although a number of considerations apply, the current findings nonetheless provide strong evidence of residual effects of recent cannabis use on WM performance, differences that appear to be the result of alterations in brain activity reflecting deficits in both engagement of executive function and disengagement of default mode processing.
Funding and disclosure
The WU-Minn Consortium Human Connectome Project is funded by the 16 NIH Institutes and Centers that support the NIH Blueprint for Neuroscience Research (Principal Investigators: David Van Essen and Kamil Ugurbil; 1U54MH091657); and by the McDonnell Center for Systems Neuroscience at Washington University in St. Louis. In addition, the current work was supported by the Peter Boris Chair in Addictions Research (JM), the Gary Sperduto Endowed Professorship in Clinical Psychology (LHS), and NIH grant P30 DA027827. No funding sources were involved in the study design or collection, analysis, and interpretation of the data. These findings do not reflect the official position of the National Institutes of Health. MMO, SM, TP, and IB declare no competing interests. MTA receives research funding from the National Institutes of Health and Correctional Service of Canada. LHS receives research funding from the National Institutes of Health. JM receives research funding from the National Institutes of Health, the Canadian Institutes of Health Research, and Correctional Service of Canada, and is a principal in BEAM Diagnostics, Inc.
References
World Health Organization. The health and social effects of nonmedical cannabis use. Geneva, Switzerland; 2016.
Meier MH, Caspi A, Ambler A, Harrington H, Houts R, Keefe RSE, et al. Persistent cannabis users show neuropsychological decline from childhood to midlife. Proc Natl Acad Sci. 2012;109:E2657–E2664.
Tait RJ, Mackinnon A, Christensen H. Cannabis use and cognitive function: 8-year trajectory in a young adult cohort. Addiction. 2011;106:2195–203.
Board on Population Health and Public Health Practice, Health and Medicine Division, National Academies of Sciences Engineering and Medicine. The health effects of cannabis and cannabinoids. Washington, DC: National Academies Press; 2017. https://doi.org/10.17226/24625.
Daneman M, Merikle PM. Working memory and language comprehension: a meta-analysis. Psychon Bull Rev. 1996;3:422–33.
Kyllonen PC, Christal RE. Reasoning ability is (little more than) working-memory capacity?! Intelligence. 1990;14:389–433.
Süß HM, Oberauer K, Wittmann WW, Wilhelm O, Schulze R. Working-memory capacity explains reasoning ability—and a little bit more. Intelligence. 2002;30:261–88.
Wesley MJ, Bickel WK. Remember the future II: meta-analyses and functional overlap of working memory and delay discounting. Biol Psychiatry. 2014;75:435–48.
Scott JC, Slomiak ST, Jones JD, Rosen AF, Moore TM, Gur RC. Association of cannabis with cognitive functioning in adolescents and young adults: a systematic review and meta-analysis. JAMA Psychiatry. 2018. https://doi.org/10.1001/jamapsychiatry.2018.0335.
Kanayama G, Rogowska J, Pope HG, Gruber SA, Yurgelun-Todd DA. Spatial working memory in heavy cannabis users: a functional magnetic resonance imaging study. Psychopharmacol (Berl). 2004;176:239–47.
Smith AM, Longo CA, Fried PA, Hogan MJ, Cameron I. Effects of marijuana on visuospatial working memory: an fMRI study in young adults. Psychopharmacol (Berl). 2010;210:429–38.
Jager G, Kahn RS, Van Den Brink W, Van Ree JM, Ramsey NF. Long-term effects of frequent cannabis use on working memory and attention: an fMRI study. Psychopharmacol (Berl). 2006;185:358–68.
Cousijn J, Wiers RW, Ridderinkhof KR, van den Brink W, Veltman DJ, Goudriaan AE. Effect of baseline cannabis use and working-memory network function on changes in cannabis use in heavy cannabis users: a prospective fMRI study. Hum Brain Mapp. 2014;35:2470–82.
Button KS, Ioannidis JPA, Mokrysz C, Nosek BA, Flint J, Robinson ESJ, et al. Power failure: why small sample size undermines the reliability of neuroscience. Nat Rev Neurosci. 2013;14:365–76.
Broyd SJ, Van Hell HH, Beale C, Yücel M, Solowij N. Acute and chronic effects of cannabinoids on human cognition—a systematic review. Biol Psychiatry. 2016;79:557–67.
Van Essen DC, Smith SM, Barch DM, Behrens TEJ, Yacoub E, Ugurbil K. The WU-Minn Human Connectome Project: an overview. Neuroimage. 2013;80:62–79.
Barch DM, Burgess GC, Harms MP, Petersen SE, Schlaggar BL, Corbetta M, et al. Function in the human connectome: task-fMRI and individual differences in behavior. Neuroimage. 2013;80:169–89.
Pagliaccio D, Barch DM, Bogdan R, Wood PK, Lynskey MT, Heath AC, et al. Shared predisposition in the association between cannabis use and subcortical brain structure. JAMA Psychiatry. 2015;72:994–1001.
Glasser MF, Sotiropoulos SN, Wilson JA, Coalson TS, Fischl B, Andersson JL, et al. The minimal preprocessing pipelines for the Human Connectome Project. Neuroimage. 2013;80:105–24.
Cox RW. AFNI: software for analysis and visualization of functional magnetic resonance neuroimages. Comput Biomed Res. 1996;29:162–73.
Owens MM, Duda B, Sweet L, MacKillop J. Distinct functional and structural neural underpinnings of working memory. Neurimage. 2018. https://doi.org/10.1016/j.neuroimage.2018.03.022.
Benjamini Y, Hochberg Y. Controlling the false discovery rate: a practical and powerful approach to multiple testing. J R Stat Soc Ser B. 1995;57:289–300.
Hayes, A. F. PROCESS: a versatile computational tool for observed variable moderation, mediation, and conditional process modeling. Manuscr Submitt Publ. 2012;1–39. http://www.afhayes.com/public/process2012.pdf.
Duncan J, Owen AM. Common regions of the human frontal lobe recruited by diverse cognitive demands. Trends Neurosci. 2000;23:475–83.
Cole MW, Schneider W. The cognitive control network: integrated cortical regions with dissociable functions. Neuroimage. 2007;37:343–60.
Buckner RL, Andrews-Hanna JR, Schacter DL. The brain’s default network: anatomy, function, and relevance to disease. Ann N Y Acad Sci. 2008;1124:1–38.
Sweet LH, Paskavitz JF, Haley AP, Gunstad JJ, Mulligan RC, Nyalakanti PK, et al. Imaging phonological similarity effects on verbal working memory. Neuropsychologia. 2008;46:1114–23.
Fox MD, Snyder AZ, Vincent JL, Corbetta M, Van Essen DC, Raichle ME. The human brain is intrinsically organized into dynamic, anticorrelated functional networks. Proc Natl Acad Sci USA. 2005;102:9673–8.
Esposito R, Cieri F, Chiacchiaretta P, Cera N, Lauriola M, Di Giannantonio M, et al. Modifications in resting state functional anticorrelation between default mode network and dorsal attention network: comparison among young adults, healthy elders and mild cognitive impairment patients. Brain Imaging Behav. 2018;12:127–41.
De Havas JA, Parimal S, Soon CS, Chee MWL. Sleep deprivation reduces default mode network connectivity and anti-correlation during rest and task performance. Neuroimage. 2012;59:1745–51.
Peterson BS, Potenza MN, Wang Z, Zhu H, Martin A, Marsh R, et al. An fMRI study of the effects of psychostimulants on default-mode processing during stroop task performance in youths with ADHD. Am J Psychiatry. 2009;166:1286–94.
Alloway TP, Alloway RG. Investigating the predictive roles of working memory and IQ in academic attainment. J Exp Child Psychol. 2010;106:20–29.
Cain K, Oakhill J, Bryant P. Children’s reading comprehension ability: concurrent prediction by working memory, verbal ability, and component skills. J Educ Psychol. 2004;96:31–42.
Raghubar KP, Barnes MA, Hecht SA. Working memory and mathematics: a review of developmental, individual difference, and cognitive approaches. Learn Individ Differ. 2010;20:110–22.
Gropper RJ, Tannock R. A pilot study of working memory and academic achievement in college students with ADHD. J Atten Disord. 2009;12:574–81.
Rogers M, Hwang H, Toplak M, Weiss M, Tannock R. Inattention, working memory, and academic achievement in adolescents referred for attention deficit/hyperactivity disorder (ADHD). Child Neuropsychol. 2011;17:444–58.
Gathercole SE, Alloway TP, Willis C, Adams A-M. Working memory in children with reading disabilities. J Exp Child Psychol. 2006;93:265–81.
de Weerdt F, Desoete A, Roeyers H. Working memory in children with reading disabilities and/or mathematical disabilities. J Learn Disabil. 2013;46:461–72.
Niessen C, Eyferth K, Bierwagen T. Modelling cognitive processes of experienced air traffic controllers. Ergonomics. 1999;42:1507–20.
Maxwell S, Cole D. Bias in cross-sectional analyses of longitudinal mediation. Psychol Methods. 2007. https://doi.org/10.1037/1082-989X.12.1.23.
Maxwell SE, Cole DA, Mitchell MA. Bias in cross-sectional analyses of longitudinal mediation: Partial and complete mediation under an autoregressive model. Multivariate Behav Res. 2011. https://doi.org/10.1080/00273171.2011.606716.
Acknowledgements
These data are from the Human Connectome Project, WU-Minn Consortium (Principal Investigators: David Van Essen and Kamil Ugurbil). The authors are deeply appreciative to the Human Connectome Project for open access to its data.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Rights and permissions
About this article

Cite this article
Owens, M.M., McNally, S., Petker, T. et al. Urinary tetrahydrocannabinol is associated with poorer working memory performance and alterations in associated brain activity. Neuropsychopharmacol 44, 613–619 (2019). https://doi.org/10.1038/s41386-018-0240-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41386-018-0240-4
This article is cited by
-
Understanding the Overlap Between Cannabis Use and Gambling Behaviour: A Systematic Review of Empirical Findings and Consideration of Policy Implications
Current Addiction Reports (2021)
-
Visuospatial Processing Decline Due to Cannabis Consumption in Nondependent High School Students
Educational Psychology Review (2021)
-
Daily, but not occasional, cannabis use is selectively associated with more impulsive delay discounting and hyperactive ADHD symptoms in binge-drinking young adults
Psychopharmacology (2021)
