
Abstract
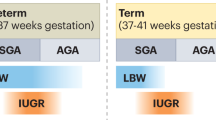
Low birth weight is associated with adult-onset diseases including hypertension and renal disease; altered renal development after intrauterine growth restriction (IUGR) may underlie such prenatal programming. Our aim was to investigate nephron endowment and renal filtration surface area in fetal sheep in which IUGR resulted from late gestational umbilico-placental embolization (UPE) or natural twinning. UPE was performed between 120 and 140 d of gestation (term ∼147 d). At autopsy (140 d), body weights of UPE and twin fetuses were, respectively, 34% and 28% lower than controls. Kidneys were sampled using a smooth fractionator approach and glomerular number was estimated using a physical disector/fractionator technique. Glomerular capillary length and filtration surface area were estimated using unbiased stereological techniques. Although relative kidney weights (grams per kilogram body weight) were not different between groups, nephron endowment was 40% lower in twin fetuses compared with controls (34.3 ± 10.6 × 104 and 55.9 ± 19.8 × 104, respectively; p < 0.05); UPE did not alter nephron number (50.7 ± 13.2 × 104). There was no difference in the glomerular capillary length or surface area between the UPE and control fetuses. IUGR due to twinning leads to reduced nephron endowment whereas late gestational IUGR does not, suggesting that reduced nephron endowment is dependent on the timing of the growth restriction. Our findings demonstrate that reduced birth weight per se does not necessarily imply reduced nephron endowment.
Similar content being viewed by others
Main
In humans, the full complement of nephrons in the kidneys has formed by approximately 36 wk of gestation and no further nephrons are formed after this time (1). A number of experimental and human studies have demonstrated reduced nephron endowment as a result of IUGR, suggesting that a compromised in utero environment impairs nephrogenesis (1–3). A reduction in nephron number at birth could have long-lasting effects on renal function. Although IUGR infants may exhibit postnatal catch-up growth, in terms of body weight and height (4), the nephrons of the kidney can only enlarge after birth. Hence, a reduction in nephron endowment during fetal development could be causally related to the high incidence of renal disease in populations that have a high incidence of IUGR, such as the Australian Aborigines (5).
The sheep is a suitable species in which to study the effects of intrauterine factors on renal development, as the gestational timing of nephrogenesis in sheep closely resembles that of humans. As in the human, nephrogenesis is completed in the sheep during the last third of gestation, at around 120 d postmating (6), with no nephrons formed after birth (∼147 d) (6). In addition, sheep usually give birth to single or twin (dizygotic) offspring, enabling the effects of twinning to be studied. In the present study, using unbiased stereological methods, the number of glomeruli was estimated in normally grown fetuses, in fetuses after naturally induced IUGR as a result of twinning, and in fetuses in which IUGR was induced experimentally during late gestation by UPE. Twinning is a natural form of IUGR, with 55% of human twins reported to have birth weights below 2500 g (7); this growth restriction occurs mainly in the third trimester (8), which is the time when nephrogenesis is greatest. To date, there is very little data on the effects of twinning on nephron endowment. Thus, the major aim of this study was to determine the effects of two forms of IUGR on nephron endowment in fetal sheep and to determine whether UPE had any effect on the capillary length and surface area of glomeruli. We studied two groups of IUGR fetuses, those that were growth restricted from experimentally induced placental insufficiency (UPE) in late gestation and those that were naturally growth restricted due to twinning. By comparing renal development in these groups, we have been able to obtain data on the relation between the timing of IUGR and altered renal development.
METHODS
Surgical procedures.
Studies were conducted on the fetuses of 15 Border Leicester X Merino ewes of known mating date. There were six control fetuses (all singletons), five fetuses that had undergone UPE to induce IUGR (all singletons), and seven fetuses from twin pregnancies. Control and UPE fetuses underwent surgery for the chronic implantation of catheters at 116 ± 1d ga as previously described (9). In brief, anesthesia was induced in ewes and fetuses with sodium pentothal (1 g, i.v.) and maintained with halothane (1.5–2% in O2). Under aseptic conditions, the fetal hindquarters were exposed to allow the implantation of a femoral artery catheter that was later used for blood sampling and to inject microspheres for UPE; this catheter was inserted such that its tip was positioned in the abdominal aorta, 1–2 cm below the level of the renal arteries. A catheter was also inserted into the fetal femoral vein. Antibiotics (procaine penicillin 500 mg, dihydrostreptomycin 500 mg, Troy Laboratories Pty Ltd, Sydney, Australia) were administered intramuscularly to all fetuses. After exteriorization of catheters and closure of surgical sites, sheep were housed in individual cages and allowed a 3- to 4-d recovery period before UPE commenced. Fetal arterial blood samples were collected daily to measure pH and blood gas tensions (Radiometer ABL 510, Copenhagen, Denmark) and blood glucose and lactate concentrations (YSI 2300 STAT Glucose and L-Lactate analyser, YSI Inc., Yellow Springs, OH, U.S.A.). All procedures were approved by the Monash University Animal Welfare Committee.
Induction of IUGR.
Fetuses in the UPE group underwent placental embolization between 120 d and 140 d ga as previously described (9, 10). In brief, daily injections of micro-spheres (diameter 40–70 μ m) into the umbilico-placental circulation (via the fetal femoral artery catheter) reduced fetal arterial O2 saturation to approximately 50% of control values. The control fetuses received saline injections only.
Autopsy.
At 140 d of gestation, all ewes and fetuses were humanely killed with an i.v. overdose of sodium pentobarbitone (325 mg/mL) (9). Before euthanasia, the control and UPE fetuses were given 6 mg of papaverine hydrochloride (i.v.) to maximally dilate the vasculature, followed by 2500 IU of heparin to minimize blood clotting in small arteries. The fetus was removed and weighed. After the right fetal kidney was removed, a further dose of papaverine hydrochloride (1.2 mg) was injected via the renal artery before perfusion at 50 mm Hg with 0.9% saline, followed by 4% paraformaldehyde and 0.2% glutaraldehyde (pH 7.4) in 0.1 M phosphate buffer. The weight of the fixed kidney was recorded.
In the twin pregnancies, fetuses were removed from the uterus and weighed. The right kidney was excised and weighed before it was immersion fixed in 4% paraformaldehyde and 0.2% glutaraldehyde in 0.1 M phosphate buffer.
Kidney sampling.
The renal capsule and fat around the hilus was removed. The kidney was then cut in half longitudinally through the hilus and again laterally through the hilus, providing four quarters. All of these were weighed and one quarter (chosen at random) and its diagonally opposite counterpart were selected. The two quarters were then cut laterally into slices 1.5-mm thick with systematic sampling of every nth segment starting from a random number. The majority of the renal medulla was removed from these 8–10 selected slices, which were then embedded in glycol methacrylate resin (Technovit 7100 resin, Heraeus Kulzer GmbH, Hanau, Germany) for the stereological determination of nephron number (11). Kidneys from control, UPE, and twin fetuses were sampled in the same manner.
In the remaining slices from the UPE and control kidneys, 10 pieces of cortex extending from the capsule to the medulla, each of which was approximately 1 mm3 in volume, were sampled and embedded in Epon-Araldite for the determination of glomerular capillary length and surface area (12).
Estimation of nephron number and renal corpuscle volume.
The kidney slices embedded in glycol methacrylate resin were sectioned at a nominal thickness of 20 μ m and the 10th and 11th sections (beginning with a random number) were collected and stained with hematoxylin and eosin. Using a physical disector/fractionator technique, the number of glomeruli in the kidneys was estimated (13). Renal corpuscle volume was also determined in the kidney sections using stereological techniques (13). Renal corpuscle volume was determined rather than glomerular tuft volume as kidneys from the twins were immersion fixed.
Estimation of glomerular capillary length and surface area.
The tissue embedded in Epon-Araldite was sectioned at 1 μ m and stained with toluidine blue. Using an unbiased stereological technique, the length and surface area of glomerular capillaries were estimated (12). The total renal filtration surface area (TRFSA) was estimated by multiplying the number of nephrons by the filtration surface area per glomerulus.
Glomerular capillary length and surface area were not determined in the kidneys from twin fetuses, as these kidneys were immersion fixed. As these morphometric measurements require the capillaries to be at a standardized state of dilation, it was deemed invalid to determine capillary length and surface area in the immersion-fixed kidneys from the twin fetuses.
Statistical analysis.
Statistical analysis was performed using GraphPad Prism version 3.0 for Windows (GraphPad Software, San Diego, CA, U.S.A.). Comparison of glomerular capillary length and surface area, as well as TRFSA, between groups were analyzed using a t test. The body weights, kidney weights, glomerular volume, and nephron number data for all three groups (control, UPE, and twin) were analyzed using a one-way ANOVA followed by a Tukey's posthoc test. All results are presented as mean ± SD. Statistical significance was taken as p < 0.05.
RESULTS
Fetal body and kidney weights.
Compared with control fetuses, body weights of UPE fetuses were reduced by 34% and those of twins by 28% (Table 1). The kidneys of the UPE fetuses were 27% lighter and those of the twin kidneys were 36% lighter than in controls (Table 1). There was no significant difference in the adjusted kidney weights of the UPE fetuses relative to controls; however, the adjusted kidney weights of the twin fetuses were 20% lower (p < 0.01) than those of the UPE fetuses.
Nephron number.
Nephron numbers in each group are shown in Figure 1. The total number of nephrons in the kidneys of twins was 40% lower than in controls (34.3 ± 10.6 × 104versus 55.9 ± 19.8 × 104, respectively; p < 0.05). The number of nephrons in the UPE kidneys (50.7 ± 13.2 × 104) was not significantly different from that of controls.

The number of glomeruli in the right kidney of control, UPE, and twin fetuses at 140 d of gestation; *p < 0.05 vs control. Bar shows the mean for each group.
Renal corpuscle volume.
Although nephron number was reduced in the twin fetuses, the mean volume of the renal corpuscle was significantly greater in the twins (6.71 ± 2.08 × 10−4 mm3) compared with controls and UPE fetuses (4.39 ± 1.27 × 10−4 mm3 and 3.74 ± 0.59 × 10−4 mm3, respectively) (Fig. 2).

The mean volume of renal corpuscles in the right kidney of control, UPE, and twin fetuses at 140 d gestation; *p < 0.05 vs control, †p < 0.05 vs UPE. Bar shows the mean for each group.
Glomerular capillary length and surface area.
There was no significant difference in the average length of capillaries per glomerulus or the total length of glomerular capillaries between the UPE and control fetuses. Similarly, there was no difference in the filtration surface area per glomerulus and TRFSA between the UPE and control groups (Table 2).
DISCUSSION
IUGR induced by UPE or naturally through twinning led to a significant reduction in fetal kidney weight, but this reduction in kidney weight was proportional to body weight. In the twin fetuses, IUGR was associated with a 40% reduction in nephron endowment, whereas in the UPE group, although absolute kidney weights were markedly reduced, nephron endowment was not affected. A reduction in nephron endowment in the twins was accompanied by an increase in renal corpuscle size in this group.
Placental embolization was accomplished by the injection of microspheres, which induces IUGR by blocking umbilico-placental blood vessels and hence restricts substrate exchange across the placenta. The effects of UPE on the sheep fetus resemble those of placental insufficiency in the human IUGR fetus (14). The induction of IUGR by UPE did not result in a reduction in the number of nephrons, which raises some interesting issues as to the influence of the timing of growth restriction. IUGR has been reported as causing a reduction in nephron numbers in rats (2, 3), rabbits (15), pigs (16), sheep (17), and even human infants (1). Surprisingly, in our study this was not the case when IUGR was induced by UPE. The UPE fetuses, although significantly growth retarded as indicated by their reductions in body and kidney weights, did not show a significant reduction in the number of nephrons. The lack of a reduced nephron endowment in the UPE fetuses highlights the importance in understanding the precise timing of the induction of IUGR. In our UPE fetuses, nephrogenesis would have been already complete by the time the embolization commenced (120 d) (6). Hence, even though the 3 wk of UPE reduced the weight of the offspring, they would already have had their full complement of nephrons. Our findings highlight the importance of ascertaining the gestational timing of IUGR to determine whether it will have significant effects on nephrogenesis; that is, birth weight alone is unlikely to provide an accurate indication of altered nephrogenesis. The lack of an effect on nephrogenesis in UPE fetuses may explain why no change was seen in the length and surface area of the capillaries in these fetuses compared with controls.
The number of glomeruli was significantly reduced in the twin fetuses. The reduction in nephron number is consistent with the more prolonged period of growth restriction in twins, which extends at least throughout the third trimester (8). Further investigation is required to ascertain the mechanisms and time course of events leading to the reduced nephrogenesis in the twins.
Interestingly, within twin pairs, reduced birth weight for gestational age is associated with elevated arterial pressure in both infants (18) and adults (19). Based on our findings, a reduced nephron number may be causally involved. Although most epidemiologic studies performed in human twins combine monozygotic and dizygotic twins, the few studies examining the difference show that dizygotic twins are less growth restricted than monozygotic twins (20, 21). The ovine twins we examined were dizygotic, suggesting that an analysis of monozygotic twins may produce an even greater nephron deficit. This is not possible to investigate in sheep as twins are usually dizygotic.
A previous stereological study of the kidneys of fetal sheep has reported 300,000–400,000 nephrons per kidney (17). The lambs studied included stillborn, sudden unexplained deaths, and twins, which could explain why nephron numbers in our control fetuses were slightly higher. In humans, it has been suggested that sudden infant death syndrome is associated with lower birth weights (22) and lower nephron numbers (23), although later studies do not confirm this (24). The range of nephrons found in our control fetuses was large, as in the human population (25). Given the strong link between birth weight and nephron number in many studies, the wide range in the control animals is probably due to the spectrum in birth weights observed in a normal population (26). In our study, birth weights in the control fetuses ranged from 4.54 to 5.82 kg, with birth weights at the lower end of the range similar to those of the IUGR fetuses (2.43–4.62 kg). The twins on the other hand had a much smaller range of nephron numbers than the controls.
The number and volume of glomeruli have long been known to be associated (27), presumably resulting in maintenance of the overall filtration capabilities of the kidney, when nephron number varies (28). Very few studies have examined the relationship between the number of glomeruli and TRFSA. An examination of TRFSA fully addresses the possibility of compensation. As expected, in our study there was no significant difference in TRFSA in the UPE fetuses compared with controls.
The mean volume of the renal corpuscle in twin fetuses is likely increased to counterbalance the decrease in number of glomeruli. It would be expected that the twin fetuses would also have an increase in capillary length and surface area to compensate for their reduction in nephron number and thus maintain their TRFSA. The TRFSA was not estimated in the twin fetuses as their kidneys were immersion fixed and thus it was considered invalid to compare them to control kidneys, in which glomerular capillaries were maximally dilated.
In the present study, the kidneys of the newborn UPE and twin fetuses appeared to be less mature histologically than those of the controls. The tissue itself and glomeruli appeared to be less mature; the tubules were not as well defined and fewer glomeruli had a visible Bowman's space. The apparent immaturity of the kidneys in the IUGR fetuses warrants further investigation. Interestingly, the macula densa appeared longer in the UPE and twin kidneys compared with controls. A quantitative stereological assessment of macula densa length, however, is required to verify these apparent differences.
In conclusion, fetal growth restriction due to twinning leads to reduced nephron endowment. However, late gestational IUGR does not alter nephron number, implying that reduced nephron endowment is dependent on the timing of IUGR in pregnancy. Hence, our findings demonstrate that reduced birth weight per se does not necessarily imply reduced nephron endowment. The long-term, postnatal effects of IUGR, either naturally occurring or experimentally induced by UPE, on kidney function and structure remain unknown.
Abbreviations
- IUGR:
-
intrauterine growth restriction
- TRFSA:
-
total renal filtration surface area
- ga:
-
gestational age
- UPE:
-
umbilico-placental embolization
References
Hinchliffe SA, Lynch MR, Sargent PH, Howard CV, Van Velzen D 1992 The effect of intrauterine growth retardation on the development of renal nephrons. Br J Obstet Gynaecol 99: 296–301.
Merlet-Benichou C, Gilbert T, Muffat-Joly M, Lelievre-Pegorier M, Leroy B 1994 Intrauterine growth retardation leads to a permanent nephron deficit in the rat. Pediatr Nephrol 8: 175–180.
Zimanyi M, Bertram JF, Black MJ 2000 Nephron number in the offspring of rats fed a low protein diet during pregnancy. Image Anal Stereol 19: 219–222.
Albertsson-Wikland K, Boguszewski M, Karlberg J 1998 Children born small-for-gestational age: postnatal growth and hormonal status. Horm Res 49: ( suppl 2) 7–13.
Spencer JL, Silva DT, Snelling P, Hoy WE 1998 An epidemic of renal failure among Australian Aboriginals. Med J Aust 168: 537–541.
Gimonet V, Bussieres L, Medjebeur AA, Gasser B, Lelongt B, Laborde K 1998 Nephrogenesis and angiotensin II receptor subtypes gene expression in the fetal lamb. Am J Physiol 274:F1062–F1069.
Martin JA, Hamilton BE, Ventura SJ, Menacker F, Park MM, Sutton PD 2002 Births: final data for 2001. Natl Vital Stat Rep 51: 1–102.
Kinzler WL, Ananth CV, Vintzileos AM 2000 Medical and economic effects of twin gestations. J Soc Gynecol Investig 7: 321–327.
Cock ML, Harding R 1997 Renal and amniotic fluid responses to umbilicoplacental embolization for 20 days in fetal sheep. Am J Physiol 273:R1094–R1102.
Louey S, Cock ML, Stevenson KM, Harding R 2000 Placental insufficiency and fetal growth restriction lead to postnatal hypotension and altered postnatal growth in sheep. Pediatr Res 48: 808–814.
Bertram JF 1995 Analyzing renal glomeruli with the new stereology. Int Rev Cytol 161: 111–172.
Nyengaard JR, Marcussen N 1993 The number of glomerular capillaries estimated by an unbiased and efficient stereological method. J Microsc 171: 27–37.
Black MJ, Briscoe TA, Dunstan HJ, Bertram JF, Johnston CI 2001 Effect of angiotensin-converting enzyme inhibition on renal filtration surface area in hypertensive rats. Kidney Int 60: 1837–1843.
Nicolaides KH, Economides DL, Soothill PW 1989 Blood gases, pH, and lactate in appropriate- and small-for-gestational-age fetuses. Am J Obstet Gynecol 161: 996–1001.
Bassan H, Trejo LL, Kariv N, Bassan M, Berger E, Fattal A, Gozes I, Harel S 2000 Experimental intrauterine growth retardation alters renal development. Pediatr Nephrol 15: 192–195.
Bauer R, Walter B, Ihring W, Kluge H, Lampe V, Zwiener U 2000 Altered renal function in growth-restricted newborn piglets. Pediatr Nephrol 14: 735–739.
Bains RK, Sibbons PD, Murray RD, Howard CV, Van Velzen D 1996 Stereological estimation of the absolute number of glomeruli in the kidneys of lambs. Res Vet Sci 60: 122–125.
Levine RS, Hennekens CH, Jesse MJ 1994 Blood pressure in prospective population based cohort of newborn and infant twins. BMJ 308: 298–302.
Poulter NR, Chang CL, MacGregor AJ, Snieder H, Spector TD 1999 Association between birth weight and adult blood pressure in twins: historical cohort study. BMJ 319: 1330–1333.
Ramos-Arroyo MA, Ulbright TM, Yu PL, Christian JC 1988 Twin study: relationship between birth weight, zygosity, placentation, and pathologic placental changes. Acta Genet Med Gemellol (Roma) 37: 229–238.
Senoo M, Okamura K, Murotsuki J, Yaegashi N, Uehara S, Yajima A 2000 Growth pattern of twins of different chorionicity evaluated by sonographic biometry. Obstet Gynecol 95: 656–661.
Buck GM, Cookfair DL, Michalek AM, Nasca PC, Standfast SJ, Sever LE, Kramer AA 1989 Intrauterine growth retardation and risk of sudden infant death syndrome (SIDS). Am J Epidemiol 129: 874–884.
Hinchliffe SA, Howard CV, Lynch MR, Sargent PH, Judd BA, Van Velzen D 1993 Renal development arrest in sudden-infant-death-syndrome. Pediatr Pathol 13: 333–343.
Beech DJ, Sibbons PD, Howard CV, van Velzen D 2000 Renal developmental delay expressed by reduced glomerular number and its association with growth retardation in victims of sudden infant death syndrome and in “normal” infants. Pediatr Dev Pathol 3: 450–454.
Hoy WE, Douglas-Denton RN, Hughson MD, Cass A, Johnson K, Bertram JF 2003 A stereological study of glomerular number and volume: preliminary findings in a multiracial study of kidneys at autopsy. Kidney Int S31–S37
Hughson M, Farris AB, Douglas-Denton R, Hoy WE, Bertram JF 2003 Glomerular number and size in autopsy kidneys: the relationship to birth weight. Kidney Int 63: 2113–2122.
Marcussen N, Nyengaard JR, Christensen S 1994 Compensatory growth of glomeruli is accomplished by an increased number of glomerular capillaries. Lab Invest 70: 868–874.
Nyengaard JR 1993 Number and dimensions of rat glomerular capillaries in normal development and after nephrectomy. Kidney Int 43: 1049–1057.
Acknowledgements
The authors thank Alex Satragno for surgical assistance, Kerryn Westcott and Todd Briscoe for technical assistance, and Penelope Simmonds for the provision of the twin fetuses.
Author information
Authors and Affiliations
Corresponding author
Additional information
Supported by the National Health and Medical Research Council of Australia.R.H. and M.J.B are joint senior authors.
Rights and permissions
About this article
Cite this article
Mitchell, E., Louey, S., Cock, M. et al. Nephron Endowment and Filtration Surface Area in the Kidney after Growth Restriction of Fetal Sheep. Pediatr Res 55, 769–773 (2004). https://doi.org/10.1203/01.PDR.0000120681.61201.B4
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/01.PDR.0000120681.61201.B4
This article is cited by
-
Twin gestation and the burden of adult cardio-renal disease
Pediatric Nephrology (2020)
-
Low birth weight, later renal function, and the roles of adulthood blood pressure, diabetes, and obesity in a British birth cohort
Kidney International (2013)
-
No juvenile arterial hypertension in sheep multiples despite reduced nephron numbers
Pediatric Nephrology (2010)
-
Hypertension and impaired renal function accompany juvenile obesity: The effect of prenatal diet
Kidney International (2007)
-
Low nephron number?a new cardiovascular risk factor in children?
Pediatric Nephrology (2004)
