
Abstract
A novel behaviorally dependent dosing (BDD) schedule was used to examine the relationship between doses of cocaine self-administered by rats and brain drug levels within a session. The BDD schedule used a hold-down response to activate a syringe pump. The length of time the lever was held down determined the duration that the syringe pump was activated. In the first experiment, rats self-administered cocaine for daily 3 h sessions and brain levels of cocaine were modeled using well-established parameters. Although analysis revealed that rats self-administered doses within a predicted range, one extremely large dose was consistently observed at the beginning of each session when brain levels of cocaine were low. In the second experiment, we introduced a range of timeout periods (10–25 min) in order to produce variability in brain-cocaine concentrations. Animals self-administered larger doses immediately following each timeout period and the dose size was inversely correlated with the length of the timeout. These results show that the dose of cocaine that rats self-administer within a session is inversely related to the amount of drug on board.
Similar content being viewed by others
INTRODUCTION
Cocaine self-administration procedures typically involve the infusion of a single unit dose of drug contingent upon the performance of an operant response (most commonly a lever press). These procedures have shown that the reinforcing effects of cocaine can be described by an ascending dose-response curve. The peak of the progressive ratio dose-response curve is typically in the range of 1.5 mg/kg (for review, see Arnold and Roberts, 1997; Stafford et al, 1998), and studies offering a choice between different doses of cocaine (Johanson and Schuster, 1975; Llewellyn et al, 1976; Lynch et al, 1998; Ward et al, 2005) have shown that larger doses on the ascending limb are generally preferred.
Given that unit doses up to ∼1.5 mg/kg are preferred, the results from an experiment using a behaviorally dependent dosing (BDD) schedule were unexpected (Morgan et al, 2009). Under the BDD schedule, the syringe pump was activated for the length of time that a lever was held down. The procedure was devised in order to provide access to a range of doses rather than a fixed unit dose selected by the experimenter. Morgan et al. (2009) showed that rats quickly learned to self-administer cocaine on the BDD schedule. Total intake during a 3-h BDD session was found to be almost identical to drug intake during a standard 3 h fixed ratio (FR1) session. When the concentration of cocaine was manipulated over a 16-fold range, rats adjusted their responding such that the total intake was consistent across concentrations. Although the findings seemed to indicate that the rats could effectively regulate their cocaine intake, the size of the self-administered doses was surprisingly low. Analysis of the lever responses revealed that rats generally held the lever down for very brief periods (<0.25 s) corresponding to very small doses of cocaine. These data show that rats appear to tightly regulate their cocaine intake on a BDD procedure; however, the doses self-administered were a full order of magnitude smaller than those predicted to be the most preferred from PR and choice studies (cited above).
The goal of the present study was to understand why doses self-administered using the BDD schedule are far smaller than those thought to be the most reinforcing. In the first experiment, animals were given access to cocaine on the BDD schedule and two new methods of analysis were used to better understand the behavior. First, having observed that BDD self-administration occurs in bursts of responses followed by long postinfusion pauses, we examined whether accounting for these clusters might more accurately reflect the size of the doses self-administered. The majority of doses were found to be within a range commonly used in self-administration studies (∼0.75 mg/kg; Caine and Koob, 1994; Ito et al, 2002; Liu et al, 2005; Pettit and Justice, 1991; Quadros and Miczek, 2009). Unexpectedly, however, a number of relatively large doses of cocaine (∼4 mg/kg) were also found. Second, we applied a mathematical model to calculate brain-cocaine concentrations (as described by Pan et al, 1991) and examined whether the size of the self-administered dose was correlated with current drugs levels. Very large doses were found to be self-administered at the beginning of the session when brain levels were low; however, later in the session much smaller doses were self-administered. In the second experiment, we introduced a range of timeout periods (10–25 min) in order to produce variability in brain-cocaine concentrations. The dose of cocaine was found to correlate with current brain-cocaine levels. One possible explanation of this relationship is that high levels of cocaine reduce the ability of the animal to hold the lever down. This hypothesis was tested in the third experiment in which animals self-administered on a BDD schedule with interspersed 5 min probe trials during which the lever was still present but responding did not activate the pump. Hold-down responding was shown to be increased during the probe trials, demonstrating that animals are fully capable of making the hold-down response. The data show that the dosage of cocaine self-administered changes within the session and is predicted by brain drug levels. These data have implications for the interpretation of results from more traditional self-administration procedures using experimenter-selected unit doses.
MATERIALS AND METHODS
Animals, Surgery, and Housing
All experiments were conducted using male, Sprague-Dawley rats (Harlan, Indianapolis, IN) weighing ∼350 g at the beginning of the experiment. Animals were given a week to acclimate to the laboratory environment. Animals were then anesthetized using a combination of ketamine (100 mg/kg; i.p.) and xylazine (8 mg/kg; i.p.), and a chronic, indwelling Silastic cannula was implanted into the right jugular vein that exited through the back of the animal in the region of the scapulae (Roberts and Goeders 1989). Ketoprofen (5 mg/kg; i.p.) was used as a postoperative analgesic, and animals were allowed to recover from surgery for a minimum of 3 days. Following surgery, animals were housed in 30 × 30 × 30 cm operant chambers under a reverse 12-h light/dark cycle with ad libitum access to food and water. All procedures were conducted in concordance with the Wake Forest University Animal Care and Use Committee guidelines.
Self-Administration Training
The beginning of the self-administration session was indicated by the extension of the lever into the self-administration chamber, which began 7 h into the dark cycle. A single response on the lever resulted in either a 0.75 or 1.5 mg/kg infusion (see below) of cocaine over ∼4 s period, followed by a 20 s timeout period during which a light cue above the lever was illuminated. The sessions occurred 7 days/week, and lasted 6 h. Two training procedures were used. Groups received access on an FR1 schedule to either (A) 0.75 mg/kg infusions until the maximum number of infusions (20) per session was self-administered for 2 consecutive days or (B) 1.5 mg/kg infusions until the maximum injections (40) per session was self-administered for 5 consecutive days. No differences between the two training protocols (A and B) were observed, and their data were combined. After completion of the FR1 training criteria, all rats were switched to a BDD schedule (see below for description of the BDD procedure) until responding was stable across three sessions.
BDD Schedule of Reinforcement Using a Hold-Down Response
The BDD schedule used the hold down as the operant response, in which depression of the lever resulted in the infusion pump turning on until the lever was released. In this way the volume of the injection was dependent on the length of time the animal held the lever down. The concentration of cocaine in the syringe and the pump speed were held constant at 5.0 mg/ml and 1.6 ml/min, respectively. The LED stimulus light above the lever was illuminated whenever the lever was depressed. Sessions lasted 3 h.
BDD with Intermittent Timeout Periods
Timeout periods of various lengths were introduced in order to force brain-cocaine levels to decline within a session. Under this condition, drug access was given for a 5-min period on the BDD schedule (as described above). Following the 5 min access period, the lever was retracted and a forced timeout period began that lasted 10, 15, 20, or 25 min depending on the experimental condition. All BDD timeout sessions lasted 6 h.
BDD with Probe Trials
For this experiment, six rats were given access to cocaine using a BDD schedule during daily 3 h sessions. Six equally spaced probe trials were inserted into each session. Every 25 min, a 5-min probe trial was introduced. During the probe trials, the lever remained extended and responding on it illuminated the stimulus light but did not activate the syringe pump. Three of the animals had extensive experience on the BDD schedule. To ensure that the results were not because of the behavioral history of these animals, an additional three animals were added to the experiment, having been trained to self-administer using training procedure A (see self-administration training above).
Modeling Brain-Cocaine Levels
Whole-brain levels of cocaine were mathematically modeled using a two-compartment model for rats receiving a chronic i.v. cocaine regimen derived by Pan et al. (1991). Briefly, we used the equation

where c is the concentration in the brain, d is the dose, k is the rate constant for transfer from the blood to the brain (0.233), v is volume of the brain (0.044), α and β (0.642 and 0.097, respectively) are constants representing the flow of cocaine between the blood and brain compartments and the elimination of cocaine from the body, and t is the time in min since the last infusion. All constants were based on the chronic i.v. administration values (Pan et al, 1991). Each infusion of cocaine was calculated independently and then summed in 5 s intervals to obtain the total concentration of cocaine (Stuber et al, 2005b).
Data Collection and Storage
Two IBM-compatible computers were used to control 16 self-administration chambers. Programs for controlling the equipment, storing the data, and analyzing the results were written in Borland Developer Suite (Embarcadero Technologies). Every event related to the physical equipment and the experimental session (lever up, lever down, pump on/off, session start time, etc.) was entered into a data stream with a time stamp in ms. Responses on the BDD schedule were analyzed into clusters; responses occurring within a specific time period of each other (measured from the end and beginning of two adjacent responses) were summed together.
Drug
Cocaine hydrochloride (National Institute on Drug Abuse Research, Research Triangle Park, NC) was dissolved in physiological saline. All drug concentrations are represented as the weight of the salt.
Statistics
Dependent measures were the size of clusters, the peak brain levels of cocaine within a 5-min BDD access period, and the trough brain levels following each timeout period. Peak levels of cocaine were analyzed by repeated measures analysis of variance. Trough levels failed the equal variance test, and therefore the χ2 test was performed in place of ANOVA. Our post hoc analysis was the Tukey test, and our probability level was 0.05. Correlation coefficients were calculated using Microsoft Excel, and all other statistical analyses were performed using SigmaPlot version 11.
RESULTS
A total of 17 rats satisfied our acquisition criterion. All but one of the 17 showed stable responding on the BDD schedule for 3 consecutive days. Four rats displayed a loss of patency before finishing the study and were therefore excluded from all analyses. The 12 remaining animals were used in the analyses of this study.
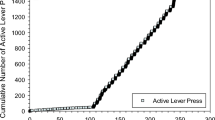
Figure 1a shows the cumulative duration of the syringe pump throughout a 3-h BDD session in a representative animal. The beginning of the session shows a steep incline, indicating the animal self-administered a large amount of cocaine in a small period of time, whereas the rest of the session is marked by a slower, stable rate of intake. Figure 1b illustrates the histogram of doses self-administered during the same BDD session. Pump intervals were grouped into bins of 0.1 mg/kg, and the peak of the histogram demonstrates that the majority of responses were for a dose of ⩽0.1 mg/kg.

Analyses of behavior on a BDD schedule of reinforcement. Data from a representative animal self-administering on a 3-h BDD schedule were graphed using multiple methods of analysis. (a) A cumulative record of the syringe pump throughout the session. (b) A histogram of the 218 responses on the lever. All responses were grouped into bins of 0.1mg/kg infusions. (c) An event record in which each line shows 1h of the session. Bars represent a response on the lever, and the height of the bar (scale equals a 1.0mg/kg infusion) represents the size of the dose injected. (d) A histogram of responses identical to (b) except that clusters of responses were accounted for such that any responses occurring within 20 s of each other were counted as a single behavior. Note the change in scale between (b) and (d). (e) The calculated brain-cocaine concentration throughout the 3 h session. (f) A scatter plot of each cluster of responses. The size of the injection is plotted on the ordinate, and the calculated brain-cocaine concentration is plotted on the abscissa. Closed circles represent responses occurring within the first 5 min of the session, whereas open circles occurred during the remainder of the session. The arrows in (d and f) highlight an extremely large dose (4.2 mg/kg) that the animal self-administered. The rate of consumption during this session was 9.80 mg/kg/h.
Closer examination of the data revealed a tendency for responses to be clustered together. Figure 1c represents the raw event record of the data. The height of each line represents the duration of the pump for each event (scale=1.0 mg/kg/inf). We accounted for clustering by grouping responses that occurred within 20 s of each other. Figure 1d shows a histogram of the same data after accounting for the clusters of responses. A consistent outlier was observed (arrow), and this outlier always occurred at the beginning of the session when blood levels were low. This observation prompted us to model whole-brain levels of cocaine using a two-compartment model described by Pan et al. (1991). Figure 1e shows the calculated brain-cocaine concentration over the 3 h BDD session. A sharp increase in brain levels is observed at the beginning of the session, and for the remainder of the session the animal maintained a consistent blood level of cocaine. Figure 1f represents the brain-cocaine concentration at the start of each cluster of responses the animal self-administered. Closed circles represent doses that were self-administered within the first 5 min of the session. Note the one outlier (arrow) occurs within the first 5 min of the session when brain levels are low. This led us to hypothesize that large doses are self-administered when brain levels are low, whereas small doses are taken when brain levels are high. However, to test this hypothesis it was necessary to manipulate brain-cocaine levels and measure the corresponding doses.
In order to manipulate the brain levels of cocaine, we used a discrete trial procedure that consisted of 5 min periods of BDD access to cocaine followed by a timeout period of 10, 15, 20, or 25 min (5–10, 5–15, 5–20, and 5–25, respectively). Figure 2a shows the event record of a representative animal on a 6-h 5–25 BDD schedule (top line). Note the large clusters occurring each time access is available. A representative 5 min access period shows that the majority of responses occur in one large cluster at the very beginning of the access period (Figure 2a, middle line). Also shown is the 20 s period in which this large cluster occurred (bottom line). Figure 2b shows the cumulative pump time during the same session. Note that the animal consistently took nearly 10 s of pump time (roughly 4.0 mg/kg) during each 5 min access period. Figure 2c shows the calculated brain-cocaine levels during this session. Note that the rat rapidly increased its brain-cocaine levels during each 5 min access period, and during the 25 min timeout period, brain levels decrease to a very consistent level (∼1.5 μM).

The effects of a timeout period on BDD self-administration behavior. Data from a representative animal during a 6 h BDD schedule consisting of alternating 5 min access periods to the BDD lever and 25 min timeout periods. (a) The event record. Bars indicates a response on the lever, and the height of the bar (scale equals a 1.0 mg/kg infusion) represents the size of the injected dose. The top line shows responses during the full 6 h session. The middle line illustrates the event record of a single 5 min BDD access period. The bottom line is an expansion of a 20-s period in which the animal self-administered a cluster of responses consisting of a mixture of relatively long and short HD responses. (b) The cumulative pump duration throughout the session. The gray shading indicates the 5 min access period. (c) The modeled brain-cocaine concentration throughout the session.
Figure 3a shows the calculated cocaine levels in a representative animal following a 10 min (top left, green), 15 min (top right, blue), 20 min (bottom left, red), or 25 min (bottom right, black) timeout period. The dashed line on each graph shows the mean level that cocaine levels fell to following each timeout period. These data illustrate that the length of the timeout determined the extent of the decrease in calculated cocaine levels. Figure 3b shows the data from Figure 3a (color matched) as a correlation (r=−0.77, P<0.001) between the dose the animal self-administered and the brain-cocaine level just before that dose was taken. Closed circles represent the first dose in each 5 min period. Correlation coefficients for all rats (n=12) and all conditions (n=4) revealed 33 out of 48 significant negative relationships (mean r value=−0.55, range=−0.27 to −0.80). The 15 nonsignificant days were due to low responding (eg, only self-administering during one of the available 5 min access period). Figure 4 shows the average highest and lowest points of modeled brain-cocaine concentrations for all rats during BDD sessions with varying timeouts. The length of the timeout had no significant effect on the peak cocaine concentration within each 5 min access period (F(3, 33)=2.149, p=0.113); however, there was a significant effect on the degree to which cocaine levels decreased (χ2 (3)=24.500, p<0.001). Post hoc analysis revealed that 5–10 trough levels were significantly higher than 5–25 or 5–20, and 5–15 levels were significantly higher than 5–25.

Current brain levels of cocaine predict subsequent dose. Data from a representative animal during four 6 h sessions consisting of alternating 5 min access periods to the BDD lever and timeout periods of varying length. (a) The calculated brain-cocaine concentration during a session with a 10 min (top left, green), 15 min (top right, blue), 20 min (bottom left, red), or 25 min (bottom right, black) timeout period. Dashed lines emphasize how far brain-cocaine levels declined following each timeout period. (b) The relationship between brain-cocaine concentration and subsequent doses animals self-administered. Data points are from the same sessions illustrated in (a). Colors represent a 10, 15, 20, or 25 min timeout period (green, blue, red, or black, respectively). Closed circles represent the first response of a 5-min BDD access period, and open circles represent a dose self-administered within the remainder of the period.

Animals maintain consistent brain-cocaine levels despite timeout length. Average peak and trough levels of brain-cocaine concentration for all animals during 6 h sessions of alternating access and timeout periods are shown. Data are sorted into sessions consisting of 10, 15, 20, or 25 min timeout periods. Closed circles represent the average (±SEM) peak level for all rats, and open circles represent the average trough levels following the timeout period. Data points significantly lower than the 5–10 or 5–15 trough levels are indicated by * and † symbols, respectively.
A third experiment was conducted to test the hypothesis that increasing cocaine levels decreased the ability of rats to respond on the lever. In this experiment, access to cocaine alternated 6 times during the 3 h session between a 25-min period of the BDD schedule and a 5-min probe trial during which responding on the lever did not activate the syringe pump. Responses on the lever were summed into 5 min bins. Figure 5a shows the total time the lever was depressed (seconds) within each 5 min bin averaged across animals. Results were converted to dose and are expressed on the right y axis as a reference. However, it should be noted that the syringe pump was not activated during probe trials. Responding during the 25 min BDD schedule periods (open circles) was consistent with our results above. However, during the 5 min probe trials (closed circles), responding on the lever increased significantly (F(35, 126)=1.662, p<0.05). Figure 5b shows the distribution of response durations for probe trials (closed circles) and the 5 min of BDD schedule immediately preceding each probe trial for all six animals. Figure 5c shows the same data converted to the amount of time the syringe pump was activated. Note that 49.8% of the total drug self-administered came from response durations <0.5 s, 21.8% came from responses >0.5 s and <1.0 s, and 28.4% came from response durations >1 s.

Within a BDD session, animals are capable of making the HD response. Animals were given access to cocaine on a BDD schedule of reinforcement, and twice an hour, 5 min probe trials were presented in which the lever was present but responding on it did not activate the pump. Open circles represent normal BDD 5 min bins and closed circles represent the probe trials in which the syringe pump was inactivated. (a) The total time the lever was depressed within each 5 min bin averaged across animals (±SEM). Rats dramatically increased their responding during the 5 min probe trials, indicating that they are capable of making a large HD response within a session when brain-cocaine levels are high. (b) The distribution of response durations for all six animals combined during the 5 min probe trials (closed circles) or the 5 min bin preceding each probe trial (open circles). (c) The same distribution converted to the amount of total pump time each response accounted for.
DISCUSSION
The primary objective of the present study was to explain the discrepancy between the small doses of cocaine self-administered under the BDD schedule using a hold-down response (Morgan et al. 2009) and the larger doses predicted by choice and PR procedures to be the most reinforcing. After accounting for the clustering of BDD responses, we found that the majority of doses were well within a range commonly used in self-administration studies (∼0.75 mg/kg; Caine and Koob, 1994; Ito et al, 2002; Liu et al, 2005; Pettit and Justice, 1991; Quadros and Miczek, 2009). However, a few surprisingly large doses (∼4 mg/kg) were also noted. These high doses occurred at the beginning of the session when brain levels would be very low; smaller doses were observed later in the session when steady rates of drug intake were being maintained. We undertook an analysis of the relationship between self-administered dose and calculated brain-cocaine levels. A range of timeout periods were introduced in order to force predictable declines in cocaine concentrations. The present data show that the dose is inversely related to the current brain levels of cocaine and can change predictably during the session. These results raise issues concerning the determination of ‘preferred’ doses and reinforcing efficacy.
Depending on the method of analysis, the data from a BDD session can be characterized in a variety of ways. On the BDD schedule, a range of doses are available to the subject by holding the lever down continuously for several seconds or by clustering many responses together; presumably the spacing within a cluster offers control over the speed of injection. Morgan et al. (2009) showed that total cocaine intake during a BDD session was almost exactly the same as the total intake during a FR1 session using a fixed unit dose (1.5 mg/kg/inj). Rats self-administering cocaine under a BDD schedule maintained a relatively constant rate of responding throughout the session, which was readily apparent by inspection of a cumulative record (see, eg, Figure 1a). Cumulative records, however, are not particularly useful in illustrating the fact that BDD responses are often grouped together—a point we failed to recognize in our initial report (Morgan et al, 2009). Plotting the data using histograms of the doses self-administered per session (see, eg, Figure 1b) and cumulative records (see, eg, Figure 1a) did not reveal clustering. However, event records (see, eg, Figure 1c) illustrated that multiple small injections were being self-administered in a short time span followed by what appeared to be a typical postinfusion pause. By combining responses that occurred within a short time frame (ie, 20 s—see below for further discussion on the selection of this criterion), we found that the majority of doses self-administered during the session were more in line with those commonly used in the literature (Caine and Koob, 1994; Ito et al, 2002; Liu et al, 2005; Pettit and Justice, 1991; Quadros and Miczek, 2009).
The mechanisms controlling drug intake at various times during a self-administration session are a matter of some debate. It has long been recognized that the initial period in a self-administration session is characterized by a burst of responding (Ettenberg et al, 1982; Wilson et al, 1971). This has been termed the ‘loading’ phase to reflect the presumption that the animal is attempting to increase the brain-cocaine concentration above some satiety threshold (Tsibulsky and Norman, 1999) or trigger point (Ranaldi et al, 1999; Wise et al, 1995). After these loading bursts, single infusions with consistent postinfusion pauses are typically observed (Wilson et al, 1971). This pattern of responding is often referred to as the ‘maintenance’ phase, during which animals presumably titrate their brain levels of cocaine within a preferred range (Tsibulsky and Norman, 1999; Wise et al, 1995). It would appear that BDD sessions also show characteristic loading and maintenance phases. Based on the present observations that during both the loading and maintenance phases the size of the self-administered cluster resulted in brain-cocaine concentration increasing into a relatively narrow range, we hypothesized that a single regulatory mechanism influences the self-administered dose throughout the session; specifically, this dose appears to reflect the amount of drug necessary to elevate brain levels into a preferred range. In order to test this, timeout periods were incorporated into the second experiment so as to manipulate brain levels of cocaine within a session. This consisted of repeated BDD access (5 min) periods followed by forced timeouts of varying length. The length of the timeout period predictably reduced brain-cocaine levels; the longer timeout periods (ie, 25 min) resulted in lower brain concentrations. We then compared the calculated brain-cocaine concentrations with the subsequent doses the animals self-administered. Results (illustrated in Figure 3) showed that introducing a timeout induced loading phase behavior, and that the size of the loading dose was highly correlated with the extent of the decline in brain levels of cocaine. These data illustrate that animals will self-administer a wide range of doses and that loading and maintenance doses simply represent the two extremes of a continuum. The size of the dose appears to be determined by the current levels of cocaine in the brain, and this single principle seems to be at work during the entire self-administration session.
Although the data clearly show that rats self-administer predictably different dosages during a session, it is presently unclear whether these varying doses should be considered to have been volitionally selected, are the most ‘preferred’, or are the most-reinforcing at that moment in the session. We suggest the most likely explanation of the fluctuations in doses is that termination of drug taking is controlled by interoceptive feedback or satiety mechanisms; the lower the brain levels are when responding begins, the longer it takes for these terminating processes to have an effect. This would be consistent with evidence and theoretical speculations concerning titration of blood levels with fixed unit doses (see above). If this is the case, it would not be necessary to invoke a volitional ‘selection’ of individual doses. Nonetheless, given the wide and predictable dose range that animals self-administer on the BDD schedule, it seems appropriate to consider whether the ‘preferred’ dose can in fact change throughout a session and whether the reinforcing effects might also be dynamically affected.
As parameters such as discrete trial interval and timeout necessarily force a decline in brain levels of cocaine, we predict that these parameters could systematically influence the results from a variety of self-administration studies. For example, one method of studying reinforcing efficacy has been to determine the peak of the dose-response curve on a PR schedule using experimenter-selected unit doses (Bergman and Paronis, 2006). In typical PR studies, rats are able to ‘load-up’ while the response requirements are minimal (ie, drug is cheap); however, as the time required to complete larger response ratios increases, greater declines in blood levels are observed (Nicola and Deadwyler, 2000). The breaking point is therefore presumably affected by the decline in blood levels and whether the experimenter-selected unit dose is sufficient to return brain concentrations to a preferred level. The present results suggest that a fixed unit dose may not be the most appropriate at any given point in time. Future work should consider whether allowing access to a range of doses using a BDD schedule at each stage of the PR session (rather than a single experimenter-selected unit does) might yield a better estimate of the maximal response output and the optimal dose. Choice procedures that use a discrete trial in order to avoid the ‘direct effects’ of a drug might be similarly affected. The intertrial interval would produce a dramatic decrease in brain-cocaine levels. Our data show that insertion of these timeout periods can increase the dose an animal self-administers, and could explain why choice studies in both rats (Lynch et al, 1998; Ward et al, 2005) and non-human primates (Johanson and Schuster, 1975; Llewellyn et al, 1976) typically report that animals prefer a higher dose of cocaine over the lower one.
A competing hypothesis that might account for the correlation between blood levels and dose during a BDD session is that higher drug concentrations interfere with the ability of the subject to hold the lever down appropriately. The idea that high drug levels somehow interfere with the ability of an animal to respond dates back to the earliest self-administration papers (Pickens and Thomspon 1968). In order to test this hypothesis, a third experiment investigated the effect of a non-reinforced probe trial at various intervals during a BDD session. Rats were given access to cocaine on a BDD schedule of reinforcement during 3 h sessions; twice an hour, 5 min probe trials occurred during which holding the lever down did not activate the syringe pump. Hold-down responding during these probe trials was greatly increased (Figure 5a), even though brain-cocaine levels were at high, mid-session levels. We interpret the increase in responding to reflect an attempt at titration and frustrative nonreward (Amsel, 1958). Regardless of the mechanism for the increase, the data clearly demonstrate that the animal is quite capable of clustering hold-down responses during periods when drug levels are relatively high. We therefore conclude that the observed relationship between brain levels of cocaine and self-administered dose is not because of an inhibition of the animal's ability to hold the lever down.
In this study, responses during a BDD procedure were grouped together into ‘clusters’ (see Materials and methods) in order to better characterize the size and duration of each drug bolus. One question that remains is why animals exhibit this clustered response pattern at all, when holding the lever down for the same total duration would presumably require less effort. One possible explanation is that holding down a lever for a significant duration is simply not in the rat's natural behavioral repertoire. Perhaps rats cannot or will not perform this type of response without behavioral shaping. This possibility can be ruled out because long hold-down responses (>4 s) have been frequently observed when rats were given BDD access to heroin (D Morgan et al. unpublished observations). Another possibility is that this behavior reflects the animal's preferred rate of injection. That is, by taking multiple microinfusions of drug within a short period of time, the animal is able to determine the speed of the infusion.
An unresolved issue is how best to define a cluster. Upon examination of a BDD event record, grouping responses into meaningful clusters is often easy and obvious. For example, subjectively counting the number of clusters during the last hour in Figure 1c (bottom line) would almost certainly yield a result of 15 clusters despite the fact that 40 responses actually occurred during this time. However, the distinction between one cluster and the next can often be much more difficult to discern (eg, the first hour of Figure 1c, top line). We spent a considerable amount of effort comparing results using different criteria, and concluded that a wide range of criteria could be used without affecting the statistical significance or conclusions of the study. For example, the BDD session illustrated in Figure 1 consisted of 218 total responses. A cluster criterion of 10, 20, or 30 s reduced these responses to 76, 66, and 59 clusters, respectively. We chose a 20 s cluster criterion because it represented a relatively conservative criterion and corresponded with the postinfusion forced timeout period that is normally imposed following each injection during more traditional self-administration procedures. In addition, we have increased confidence that this criterion is appropriate as its use reveals a high correlation between cluster size and postinfusion pause (Zimmer et al, 2011; in preparation).
The accuracy of the modeled brain-cocaine concentrations deserves comment. The equations have been extensively used in behavioral self-administration (Ahmed and Koob, 2005; Samaha et al, 2002; Zernig et al, 2007), electrophysiological (Nicola and Deadwyler, 2000; Peoples and Cavanaugh, 2003; Peoples et al, 2004, 2007), microdialysis (Wise et al, 1995), and voltammetric studies (Hermans et al, 2008; Stuber et al, 2005a, 2005b), and a remarkable temporal relationship between modeled brain-cocaine concentration, NAc dopamine levels (Hermans et al, 2008; Shou et al, 2006; Wise et al, 1995), and cocaine-induced locomotor behavior (Shou et al, 2006) have been demonstrated. It is acknowledged that the relationship demonstrated here used modeled and not actual brain levels; nonetheless, the conclusions are based on relative changes in brain-cocaine concentrations and not the absolute magnitude. It should be noted that the modeling is determined for each infusion regardless of size, and is completely independent of the clustering analysis and criterion.
In summary, we have shown here that on the BDD schedule of reinforcement, hold-down responses are often clustered together, resulting in a bolus injection of various sizes—some up to 4 mg/kg/inj. Rats typically self-administered large doses during the loading phase, followed by small, maintenance doses for the remainder of the session. The data are consistent with the idea that brain concentrations of cocaine are titrated within a restricted range and the size of the dose self-administered at any point during the session depends largely on the amount of cocaine already on board. The present results suggest that the ‘most preferred’ or ‘most reinforcing’ dose of cocaine might fluctuate according to the brain levels at any particular moment.
References
Ahmed SH, Koob GF (2005). Transition to drug addiction: a negative reinforcement model based on an allostatic decrease in reward function. Psychopharmacology (Berl) 180: 473–490.
Amsel A (1958). The role of frustrative nonreward in noncontinuous reward situations. Psychol Bull 55: 102–119.
Arnold JM, Roberts DC (1997). A critique of fixed and progressive ratio schedules used to examine the neural substrates of drug reinforcement. Pharmacol Biochem Behav 57: 441–447.
Bergman J, Paronis CA (2006). Measuring the reinforcing strength of abused drugs. Mol Interv 6: 273–283.
Caine SB, Koob GF (1994). Effects of mesolimbic dopamine depletion on responding maintained by cocaine and food. J Exp Anal Behav 61: 213–221.
Ettenberg A, Pettit HO, Bloom FE, Koob GF (1982). Heroin and cocaine intravenous self-administration in rats: mediation by separate neural systems. Psychopharmacology (Berl) 78: 204–209.
Hermans A, Keithley RB, Kita JM, Sombers LA, Wightman RM (2008). Dopamine detection with fast-scan cyclic voltammetry used with analog background subtraction. Anal Chem 80: 4040–4048.
Ito R, Dalley JW, Robbins TW, Everitt BJ (2002). Dopamine release in the dorsal striatum during cocaine-seeking behavior under the control of a drug-associated cue. J Neurosci 22: 6247–6253.
Johanson CE, Schuster CR (1975). A choice procedure for drug reinforcers: cocaine and methylphenidate in the rhesus monkey. J Pharmacol Exp Ther 193: 676–688.
Liu Y, Roberts DC, Morgan D (2005). Effects of extended-access self-administration and deprivation on breakpoints maintained by cocaine in rats. Psychopharmacology (Berl) 179: 644–651.
Llewellyn ME, Iglauer C, Woods JH (1976). Relative reinforcer magnitude under a nonindependent concurrent schedule of cocaine reinforcement in rhesus monkeys. J Exp Anal Behav 25: 81–91.
Lynch WJ, LaBounty LP, Carroll ME (1998). A novel paradigm to investigate regulation of drug intake in rats self-administering cocaine or heroin intravenously. Exp Clin Psychopharmacol 6: 22–31.
Morgan D, Liu Y, Oleson EB, Roberts DC (2009). Cocaine self-administration on a hold-down schedule of reinforcement in rats. Psychopharmacology (Berl) 201: 601–609.
Nicola SM, Deadwyler SA (2000). Firing rate of nucleus accumbens neurons is dopamine-dependent and reflects the timing of cocaine-seeking behavior in rats on a progressive ratio schedule of reinforcement. J Neurosci 20: 5526–5537.
Pan HT, Menacherry S, Justice Jr JB (1991). Differences in the pharmacokinetics of cocaine in naive and cocaine-experienced rats. J Neurochem 56: 1299–1306.
Peoples LL, Cavanaugh D (2003). Differential changes in signal and background firing of accumbal neurons during cocaine self-administration. J Neurophysiol 90: 993–1010.
Peoples LL, Kravitz AV, Lynch KG, Cavanaugh DJ (2007). Accumbal neurons that are activated during cocaine self-administration are spared from inhibitory effects of repeated cocaine self-administration. Neuropsychopharmacology 32: 1141–1158.
Peoples LL, Lynch KG, Lesnock J, Gangadhar N (2004). Accumbal neural responses during the initiation and maintenance of intravenous cocaine self-administration. J Neurophysiol 91: 314–323.
Pettit HO, Justice Jr JB (1991). Effect of dose on cocaine self-administration behavior and dopamine levels in the nucleus accumbens. Brain Res 539: 94–102.
Pickens R, Thompson T (1968). Cocaine-reinforced behavior in rats: effects of reinforcement magnitude and fixed-ratio size. J Pharmacol Exp Ther 161: 122–129.
Quadros IM, Miczek KA (2009). Two modes of intense cocaine bingeing: increased persistence after social defeat stress and increased rate of intake due to extended access conditions in rats. Psychopharmacology (Berl) 206: 109–120.
Ranaldi R, Pocock D, Zereik R, Wise RA (1999). Dopamine fluctuations in the nucleus accumbens during maintenance, extinction, and reinstatement of intravenous D-amphetamine self-administration. J Neurosci 19: 4102–4109.
Roberts DC, Goeders NE (1989). Drug self-administration: Experimental methods and determiants. Boalton AA, Baker GB, Greenshaw AS (eds). In: Neuromethods, vol. 13. Psychopharmacology. Humana press: Clifton, NJ. pp 349–398.
Samaha AN, Li Y, Robinson TE (2002). The rate of intravenous cocaine administration determines susceptibility to sensitization. J Neurosci 22: 3244–3250.
Shou M, Ferrario CR, Schultz KN, Robinson TE, Kennedy RT (2006). Monitoring dopamine in vivo by microdialysis sampling and on-line CE-laser-induced fluorescence. Anal Chem 78: 6717–6725.
Stafford D, LeSage MG, Glowa JR (1998). Progressive-ratio schedules of drug delivery in the analysis of drug self-administration: a review. Psychopharmacology (Berl) 139: 169–184.
Stuber GD, Roitman MF, Phillips PE, Carelli RM, Wightman RM (2005a). Rapid dopamine signaling in the nucleus accumbens during contingent and noncontingent cocaine administration. Neuropsychopharmacology 30: 853–863.
Stuber GD, Wightman RM, Carelli RM (2005b). Extinction of cocaine self-administration reveals functionally and temporally distinct dopaminergic signals in the nucleus accumbens. Neuron 46: 661–669.
Tsibulsky VL, Norman AB (1999). Satiety threshold: a quantitative model of maintained cocaine self-administration. Brain Res 839: 85–93.
Ward SJ, Morgan D, Roberts DC (2005). Comparison of the reinforcing effects of cocaine and cocaine/heroin combinations under progressive ratio and choice schedules in rats. Neuropsychopharmacology 30: 286–295.
Wilson MC, Hitomi M, Schuster CR (1971). Psychomotor stimulant self administration as a function of dosage per injection in the rhesus monkey. Psychopharmacologia 22: 271–281.
Wise RA, Newton P, Leeb K, Burnette B, Pocock D, Justice Jr JB (1995). Fluctuations in nucleus accumbens dopamine concentration during intravenous cocaine self-administration in rats. Psychopharmacology (Berl) 120: 10–20.
Zernig G, Ahmed SH, Cardinal RN, Morgan D, Acquas E, Foltin RW et al (2007). Explaining the escalation of drug use in substance dependence: models and appropriate animal laboratory tests. Pharmacology 80: 65–119.
Zimmer BA, Dobrin CV, Roberts DC (2011). The self-administered dose of cocaine predicts the subsequent inter-infusion interval. (unpublished data)
Acknowledgements
This study was supported by the NIDA research Grant R01 DA14030 (to DCSR).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Zimmer, B., Dobrin, C. & Roberts, D. Brain-Cocaine Concentrations Determine the Dose Self-Administered by Rats on a Novel Behaviorally Dependent Dosing Schedule. Neuropsychopharmacol 36, 2741–2749 (2011). https://doi.org/10.1038/npp.2011.165
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/npp.2011.165
Keywords
This article is cited by
-
Prelimbic and infralimbic medial prefrontal cortex neuron activity signals cocaine seeking variables across multiple timescales
Psychopharmacology (2023)
-
D-amphetamine maintenance therapy reduces cocaine use in female rats
Psychopharmacology (2022)
-
Amphetamine maintenance therapy during intermittent cocaine self-administration in rats attenuates psychomotor and dopamine sensitization and reduces addiction-like behavior
Neuropsychopharmacology (2021)
-
Effects of Kappa opioid receptor blockade by LY2444296 HCl, a selective short-acting antagonist, during chronic extended access cocaine self-administration and re-exposure in rat
Psychopharmacology (2020)
-
Hold-down as an alternative to unit dose in cocaine self-administration experiments: Characterization using a progressive ratio schedule
Psychopharmacology (2020)
