
Abstract
Objective:
Recent reports have posited a temporal association between blood transfusion with packed red blood cells (BT) and necrotizing enterocolitis (NEC). We evaluated the relationship between BT and NEC among infants at three hospitals who were consented at birth into a prospective observational study of NEC.
Study Design:
We used a case–control design to match each case of NEC in our study population of infants born at<33 weeks postmenstrual age (PMA) to one control infant using hospital of birth, PMA, birth weight and date of birth.
Result:
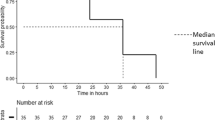
The number of transfusions per infant did not differ between 42 NEC cases and their controls (4.0±4.6 vs 5.4±4.1, mean±s.d., P=0.063). A matched-pair analysis did not identify an association of transfusion with NEC in either the 48-h or 7-day time periods before the onset of NEC. Stratifying on matched-sets, the Cox proportional hazard model did not identify any difference in the total number of BTs between the two groups (hazard ratio 0.78, 95% confidence interval 0.57 to 1.07, P=0.11).
Conclusion:
In contrast to previous studies, our case–control study did not identify a significant temporal association between BT and NEC. Additional large prospective randomized studies are needed to clarify the relationship between BT and NEC.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout

Similar content being viewed by others


References
Neu J, Walker WA . Necrotizing enterocolitis. N Engl J Med 2011; 364: 255–264.
Sharma R, Hudak ML . A clinical perspective of necrotizing enterocolitis: past, present, and future. Clin Perinatol 2013; 40: 27–51.
Wiedmeier SE, Henry E, Baer VL, Stoddard RA, Eggert LD, Lambert DK et al. Center differences in NEC within one health-care system may depend on feeding protocol. Am J Perinatol 2008; 25: 5–11.
Hay WW Jr . Strategies for feeding the preterm infant. Neonatology 2008; 94: 245–254.
Nanthakumar N, Meng D, Goldstein AM, Zhu W, Lu L, Uauy R et al. The mechanism of excessive intestinal inflammation in necrotizing enterocolitis: an immature innate immune response. PloS One 2011; 6: e17776.
Sharma R, Tepas JJ 3rd, Hudak ML, Mollitt DL, Wludyka PS, Teng R-J et al. Neonatal gut barrier and multiple organ failure: role of endotoxin and proinflammatory cytokines in sepsis and necrotizing enterocolitis. J Pediatr Surg 2007; 42: 454–461.
Mai V, Young CM, Ukhanova M, Wang X, Sun Y, Casella G et al. Fecal microbiota in premature infants prior to necrotizing enterocolitis. PloS One 2011; 6: e20647.
Mally P, Golombek SG, Mishra R, Nigam S, Mohandas K, Depalma H et al. Association of necrotizing enterocolitis with elective packed red blood cell transfusions in stable, growing, premature neonates. Am J Perinatol 2006; 23: 451–458.
Christensen RD, Lambert DK, Henry E, Wiedmeier SE, Snow GL, Baer VL et al. Is “transfusion-associated necrotizing enterocolitis” an authentic pathogenic entity? Transfusion 2010; 50: 1106–1112.
Paul DA, Mackley A, Novitsky A, Zhao Y, Brooks A, Locke RG . Increased odds of necrotizing enterocolitis after transfusion of red blood cells in premature infants. Pediatrics 2011; 127: 635–641.
Blau J, Calo JM, Dozor D, Sutton M, Alpan G, La Gamma EF . Transfusion-related acute gut injury: necrotizing enterocolitis in very low birth weight neonates after packed red blood cell transfusion. J Pediatr 2011; 158: 403–409.
Demirel G, Celik IH, Aksov HT, Erdeve D, Oguz SS, Uras N et al. Transfusion-associated necrotising enterocolitis in very low birth weight premature infants. Transfus Med 2012; 22: 332–337.
Elabiad MT, Harsono M, Talati AJ, Dhanireddy R . Effect of birth weight on the association between necrotising enterocolitis and red blood cell transfusions in≤1500 g infants. BMJ Open 2013; 3: e003823.
Miner CA, Fullmer S, Eggett DL, Christensen RD . Factors affecting the severity of necrotizing enterocolitis. J Matern Fetal Neonatal Med 2013; 26: 1715–1719.
Josephson CD, Wesolowski A, Bao G, Sola-Visner MC, Dudell G, Castillejo MI et al. Do red cell transfusions increase the risk of necrotizing enterocolitis in premature infants? J Pediatr 2010; 157 (972-978): e1–e3.
El-Dib M, Narang S, Lee E, Massaro AN, Aly H . Red blood cell transfusion, feeding and necrotizing enterocolitis in preterm infants. J Perinatol 2011; 31: 183–187.
Singh R, Visintainer PF, Frantz ID 3rd, Shah BL, Meyer KM, Favila SA et al. Association of necrotizing enterocolitis with anemia and packed red blood cell transfusions in preterm infants. J Perinatol 2011; 31: 176–182.
Stritzke AI, Smyth J, Synnes A, Lee SK, Shah PS . Transfusion-associated necrotising enterocolitis in neonates. Arch Dis Child Fetal Neonatal Ed 2013; 98: F10–F14.
Wan-Huen P, Bateman D, Shapiro DM, Parravicini E . Packed red blood cell transfusion is an independent risk factor for necrotizing enterocolitis in premature infants. J Perinatol 2013; 33: 786–790.
Martin FG, Sáenz de Pipaón M, Pėrez Rodriguez J, Jimėnez JG . Risk factors for the development of necrotizing enterocolitis: a case-control study. J Neonatal Perinatal Med 2013; 6: 311–318.
Kirpalani H, Zupancic JA . Do transfusions cause necrotizing enterocolitis? The complementary role of randomized trials and observational studies. Semin Perinatol 2012; 36: 269–276.
Ballard JL, Khoury JC, Wedig K, Wang L, Eilers-Walsman BL, Lipp R . New Ballard Score expanded to include extremely premature infants. J Pediatr 1991; 119: 417–423.
Bell MJ, Ternberg JL, Feigin RD, Keating JP, Marshall R, Barton L et al. Neonatal necrotizing enterocolitis. Therapeutic decisions based upon clinical staging. Ann Surg 1978; 187: 1–7.
Strauss RG . Data-driven blood banking practices for neonatal RBC transfusions. Transfusion 2000; 40: 1528–1540.
Roseff SD, Luban NL, Manno CS . Guidelines for assessing appropriateness of pediatric transfusion. Transfusion 2002; 42: 1398–1413.
SAS® for Windows, Version 9.3. SAS Institute, Cary, NC, USA. 2002–2010.
Papile LA, Burstein J, Burstein R, Koffler H . Incidence and evolution of subependymal and intraventricular hemorrhage: a study of infants with birth weights less than 1,500 gm. J Pediatr 1978; 92: 529–534.
Tugwell P, Haynes B . Assessing claims of causation. In: Haynes RB, Sackett DL, Guyatt GH, Tugwell P (eds). Clinical Epidemiology: How to do clinical practice research, 3rd edn. Lippincott, Williams and Wilkins: New York, NY, 2005, pp 356–381.
Young CM, Kingma SD, Neu J . Ischemia-reperfusion and neonatal intestinal injury. J Pediatr 2011; 158 (2 Suppl): e25–e28.
Mohamed A, Shah PS . Transfusion associated necrotizing enterocolitis: a meta-analysis of observational data. Pediatrics 2012; 129: 529–540.
Ng EW, Poon TC, Lam HS, Cheung HM, Ma TP, Chan KY et al. Gut-associated biomarkers L-FABP, I-FABP, and TFF3 and LIT score for diagnosis of surgical necrotizing enterocolitis in preterm infants. Ann Surg 2013; 258: 1111–1118.
Bell EF, Strauss RG, Widness JA, Mahoney LT, Mock DM, Seward VJ et al. Randomized trial of liberal versus restrictive guidelines for red blood cell transfusion in preterm infants. Pediatrics 2005; 115: 1685–1691.
Kirpalani H, Whyte RK, Andersen C, Asztalos EV, Heddle N, Blajchman MA et al. The premature infants in need of transfusion (PINT) study: a randomized, controlled trial of a restrictive (low) versus liberal (high) transfusion threshold for extremely low birth weight infants. J Pediatr 2006; 149: 301–307.
Acknowledgements
This work was supported in part by the National Institute of Child Health and Human Development Grant RO1 HD059143 and in part by the National Center for Advancing Clinical and Translational Sciences Grant 1UL1TR000064.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Appendix Transfusion guidelines in the study population
Appendix Transfusion guidelines in the study population
Hematocrit<35% and any of the following conditions:
Patient receiving⩾0.4 supplemental fractional inspired oxygen concentration by hood or continuous positive airway pressure or receiving fractional inspired oxygen concentration supplementation⩾0.35 on mechanical ventilation with mean airway pressure⩾9 or hypotension.
Hematocrit<28% and any of the following conditions:
Receiving⩾0.4 fractional inspired oxygen concentration by nasal cannula or⩾0.35 by mechanical ventilation;
Apnea or bradycardia⩾2 episodes in 24 h requiring bag and mask ventilation without any definite cause;
Heart rate⩾175 beats min−1 or respiratory rate⩾70 breaths min−1 for 24 h without any definite cause; and
Weight gain<10 g kg−1 day−1 for 4 days, while receiving⩾110 cal kg−1 day−1.
Hematocrit<20% asymptomatic with reticulocyte count<2%.
Rights and permissions
About this article

Cite this article
Sharma, R., Kraemer, D., Torrazza, R. et al. Packed red blood cell transfusion is not associated with increased risk of necrotizing enterocolitis in premature infants. J Perinatol 34, 858–862 (2014). https://doi.org/10.1038/jp.2014.59
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/jp.2014.59
This article is cited by
-
The short-term effects of RBC transfusions on intestinal injury in preterm infants
Pediatric Research (2023)
-
Development of necrotizing enterocolitis after blood transfusion in very premature neonates
World Journal of Pediatrics (2023)
-
Neonatal anemia relates to intestinal injury in preterm infants
Pediatric Research (2022)
-
Blood group AB increases risk for surgical necrotizing enterocolitis and focal intestinal perforation in preterm infants with very low birth weight
Scientific Reports (2021)
-
Risk of Necrotizing Enterocolitis Following Packed Red Blood Cell Transfusion in Very Low Birth Weight Infants
The Indian Journal of Pediatrics (2019)
