
Abstract
Objective:
The definition of bronchopulmonary dysplasia (BPD) among very-low birth weight (VLBW) infants is based upon oxygen requirement at 36 weeks gestation, but oxygen may be required at altitude because of hypoxia. This study determined the effect of altitude on BPD rates.
Study Design:
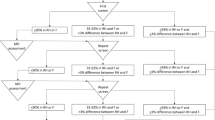
For 63 VLBW infants at high altitude, oxygen concentrations were measured by a hood oxygenation test (HOT) and BPD rates were determined with altitude adjustment.
Result:
BPD rates before and after altitude adjustment were 71.8 and 26.7%, respectively. Of oxygen-dependent infants analyzed by HOT, 33.3% needed room air. HOT oxygen requirement correlated with gestational age of last apnea episode (r=0.42, P<0.001).
Conclusion:
Although BPD rates may be adjusted for altitude with the HOT, the test does not accurately predict clinical oxygen need. Persistent requirement for supplemental oxygen beyond that needed in the HOT may be partially due to immaturity of respiratory control mechanisms.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout

Similar content being viewed by others

References
Jobe A, Bancalari E . Bronchopulmonary dysplasia. Am J Respir Crit Care Med 2001; 163: 1723–1729.
Ehrenkranz R, Walsh M, Vohr B, Jobe A, Wright L, Fanaroff A et al. Validation of the National Institutes of Health consensus definition of bronchopulmonary dysplasia. Pediatrics 2005; 116: 1353–1360.
Walsh M, Yao Q, Gettner P, Hale E, Collins M, Hensman A et al. Impact of a physiologic definition on bronchopulmonary dysplasia rates. Pediatrics 2004; 114: 1305–1311.
Walsh M, Engle W, Laptook A, Kazzi N, Buchter S, Rasmussen M et al. Oxygen delivery through nasal cannulae to preterm infants: can practice be improved? Pediatrics 2005; 116: 857–861.
Ellsbury D, Acarregui M, McGuinness G, Klein J . Variability in the use of supplemental oxygen for bronchopulmonary dysplasia. J Pediatr 2002; 140: 247–249.
Samuels M . The effects of flight and altitude. Arch Dis Child 2004; 89: 448–455.
Benaron D, Benitz W . Maximizing the stability of oxygen delivered via nasal cannula. Arch Pediatr Adolesc Med 1994; 148 (3): 294–300.
Red Oaks Trading Ltd. Altitudes of major US cities. http://www.altimeters.net/cityaltitudes.html.
Gonzales G, Salirrosas A . Arterial oxygen saturation in healthy newborns delivered at term in Cerro de Pasco (4340 m) and Lima (150 m). Rep Biol Endocrinol 2005; 3: 1186.
Salas A . Pulse oximetry values in healthy term newborns at high altitude. Ann Trop Paediatr 2008; 28 (4): 275–278.
Niermeyer S . Cardiopulmonary transition in the high altitude infant. High Alt Med Biol 2003; 4 (2): 225–239.
Bakr A, Habib H . Normal values of pulse oximetry in newborns at high altitude. J Trop Med 2005; 51 (3): 170–173.
Horne R, Parslow P, Harding R . Postnatal development of ventilatory and arousal responses to hypoxia in human infants. Respir Physiol Neurobiol 2005; 149: 257–271.
Niermeyer S, Yang P, Shanmina, Drolkar, Zhuang J, Moore L . Arterial oxygen saturation in Tibetan and Han infants born in Lhasa, Tibet. N Eng J Med 1995; 333: 1248–1252.
de Meer K, Heymans H, Zijlstra E . Physical adaptation of children to life at higher altitude. Eur J Pediatr 1995; 154: 263–272.
Mortola J, Frappell P, Frappell D, Villena-Cabrera N, Villena-Cabrera M, Pena F . Ventilation and gaseous metabolism in infants born at high altitude, and their responses to hypoxia. Am Rev Respir Dis 1992; 146: 1206–1209.
Wilkinson M, Skuza E, Rennie G, Sands S, Yiallourou S, Horne R et al. Postnatal development of periodic breathing cycle duration in term and preterm infants. Pediatr Res 2007; 62 (3): 331–336.
Parkins K, Poets C, O’Brien L, Stebbins V, Southall D . Effect of exposure to 15% oxygen on breathing patterns and oxygen saturation in infants: interventional study. BMJ 1998; 316 (7135): 887–891.
Poets C, Southall D . Patterns of oxygenation during periodic breathing in preterm infants. Early Hum Devt 1991; 26 (1): 1–12.
Steinhorn R . Neonatal pulmonary hypertension. Pediatr Crit Care Med 2010; 11: S79–S84.
Brockmann P, Poets A, Urschitz M, Sokollik C, Poets C . Reference values for pulse oximetry recordings in healthy term neonates during their first 5 days of like. Arch Dis Child Fetal Neonatal Ed 2011; 96: F335–F338.
Resnick S, Hall G, Simmer K, Stick S, Sharp M . The hypoxia challenge test does not accurately predict hypoxia in flight in ex-preterm neonates. Chest 2008; 133 (5): 1161–1166.
Niermeyer S, Mollinedo P, Huicho L . Child health and living at high altitude. Arch Dis Child 2009; 94: 806–811.
Saugstad O, Speer C, Halliday H . Oxygen saturation in immature babies: revisited with updated recommendations. Neonatology 2011; 100: 217–218.
Jones M . Effect of preterm birth on airway function and lung growth. Paediatr Respir Rev 2009; 10: 9–11.
Acknowledgements
The author wishes to thank Sue Danielson for assistance with data tabulation.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The author declares no conflict of interest.
Appendix
Appendix
Calculation of oxygen concentration required at altitude to simulate an oxygen concentration at sea level
The behavior of gases is governed by the Ideal Gas Equation:

where P=pressure, V=volume, n=number of moles, R=ideal gas constant, and T=temperature.
At sea level (s) and altitude (a), gas may be described by respective equations

and

Dividing the equation at altitude by the equation at sea level yields

Assuming constant temperature and volume (constant tidal volume and minute ventilation) yields

This equation gives the ratio of the number of oxygen molecules in a given volume at altitude to the number in the same volume at sea level. In Denver Pa=630 mm Hg and at sea level Ps=760 mm Hg. Therefore, in Denver there are only 630/760=0.829 as many oxygen molecules in a given volume of air as there are at sea level. The inverse of this ratio allows the calculation of the number of additional molecules of oxygen, or alternatively the fraction of inspired oxygen (FIO2)a, required at a given altitude to simulate an (FIO2)s at sea level: (FIO2)a=(FIO2)s (Ps/Pa). For room air at sea level (FIO2)s is 0.21. So for Denver, Ps/Pa=1.21 and (FIO2)a=0.253 to simulate room air at sea level.
Rights and permissions
About this article
Cite this article
Britton, J. Altitude, oxygen and the definition of bronchopulmonary dysplasia. J Perinatol 32, 880–885 (2012). https://doi.org/10.1038/jp.2012.6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/jp.2012.6
Keywords
This article is cited by
-
Measuring quality of care in moderate and late preterm infants
Journal of Perinatology (2022)
-
Bronchopulmonary dysplasia: effect of altitude correction and role for the Neonatal Research Network Prediction Algorithm
Journal of Perinatology (2018)
-
Oxygen dependency as equivalent to bronchopulmonary dysplasia at different altitudes in newborns ⩽1500 g at birth from the SIBEN network
Journal of Perinatology (2014)
-
Histological chorioamnionitis and bronchopulmonary dysplasia: a retrospective cohort study
Journal of Perinatology (2013)
