
Abstract
Purpose
To evaluate the long-term visual prognosis and intraocular pressure (IOP) control following direct and indirect cycloplexy for the surgical treatment of traumatic cyclodialysis clefts.
Methods
Retrospective consecutive case series of 17 eyes of 17 patients. All eyes showing signs of ocular hypotony were treated with either cleft cyclocryotherapy and/or direct surgical cycloplexy. Cycloplexy was performed by directly suturing the ciliary body to the scleral spur under a double-lamellar limbal-based scleral flap. The main outcome measures were IOP, best-corrected visual acuity (BCVA), and the occurrence of postoperative complications.
Results
The cyclodialysis clefts were post-traumatic in all the 17 eyes and extended for 2.1±1.6 clock-hours (range, 0.5–6 clock-hours). The mean follow-up time was 43.7±24.6 months (range, 12–110 months). Preoperatively, the mean IOP was 6.9±4.0 mm Hg (range, 2–14 mm Hg). Postoperatively, painful reversible IOP spikes of up to 70 mm Hg developed in 13 eyes. The final mean postoperative IOP was 12.2±4.1 mm Hg with no cases of secondary glaucoma. Preoperatively, BCVA was 6/12 or better in 4 eyes (24%), which rose to 12 eyes (71%) at final follow-up. Of the 12 patients who underwent direct cycloplexy, 75% achieved a final BCVA of 6/12 or better. There were no serious complications related to direct cycloplexy, including suprachoroidal haemorrhage or endophthalmitis.
Conclusions
Successful cyclodialysis cleft repair can lead to a good long-term visual prognosis and stable IOP control, even in cases with a protracted history of ocular hypotony.
Similar content being viewed by others


Introduction
A cyclodialysis cleft results from the disinsertion of the longitudinal ciliary muscle fibres from the scleral spur.1 This forms an abnormal connection between the anterior chamber and the suprachoroidal space. The newly created pathway results in increased uveoscleral outflow via the suprachoroidal space and a reduction in aqueous production due to diminished blood supply to the ciliary body.1, 2 The sequelae of cyclodialysis include chronic ocular hypotony, anterior chamber shallowing, cataract, choroidal effusions, retinal and choroidal folds, hypotonous maculopathy, and loss of vision.3
Cyclodialysis cleft formation occurs almost exclusively as a result of blunt ocular trauma or anterior segment surgery. Gonioscopy remains the gold standard for the identification of cyclodialysis clefts; however, slit-lamp gonioscopy can be made difficult due to chronic hypotony, hyphaema, or corneal opacity. Assessment of the drainage angle may be further complicated by the presence of angle recession, peripheral anterior synechiae (PAS), and adjacent iridodialyses. In cases where direct visualisation is difficult, high frequency ultrasound biomicroscopy (UBM) can be used to visualise the irido-corneal angle configuration.4, 5 In cases where there is a high suspicion of a cleft, but the view is poor, then clefts can be identified by filling the anterior chamber with viscoelastic and performing on-table gonioscopy.
Small clefts may close spontaneously or sometimes with the use of topical cycloplegic agents, which help to relax the ciliary muscle and promote apposition of the detached longitudinal ciliary muscle fibres to the sclera.6 In larger cyclodialysis clefts, various techniques have been described for repair, including direct surgical cycloplexy,7 scleral buckling,8 vitrectomy with gas tamponade,9 argon or diode cyclophotocoagulation,10 and cleft cryotherapy.11 However, there is limited data on the long-term visual prognosis and intraocular pressure (IOP) control after cleft surgery. We describe the long-term outcomes of direct and indirect surgical cycloplexy in a large, single-centre consecutive case series of patients with hypotony secondary to cyclodialysis clefts.
Methods
Clinical data of 17 eyes of 17 patients who underwent indirect and/or direct surgical cycloplexy for repair of a cyclodialysis cleft were analysed retrospectively. All eyes had persistent ocular hypotony with optic disc swelling, macular folds, or macular oedema. Ethical approval was granted from the South Staffordshire local research ethics committee (reference number 10/H1203/3). All cases were operated upon by a single surgeon (PS).
Preoperative gonioscopic evaluation of the anterior chamber angle was performed in order to identify and delineate the extent of the cyclodialysis cleft(s). If the view of the drainage angle was compromised due to a shallow anterior chamber or convex peripheral iris configuration, then further evaluation was undertaken in the operating theatre using an intracameral ophthalmic viscosurgical device (OVD) and on-table gonioscopy. Additional UBM (Aviso, Quantel Medical, Inc., Bozeman, MT, USA) was performed in order to confirm the presence of the cyclodialysis cleft and to identify other potential clefts concealed on gonioscopy. The initial management of all the small clefts (<1.5 clock-hours) was a trial of cycloplegia using G. Atropine 1% twice daily for 6 weeks. Surgery was performed in all the cases of persistent hypotony.
Cleft cryotherapy
Examination under local or general anaesthesia was performed. The AC was deepened with an OVD, and on-table gonioscopy identified the extent of the cyclodialysis cleft(s) and the configuration of the remaining angle configuration (extent of the PAS and angle recession). Cleft cryotherapy using a double freeze-thaw technique was applied to the full extent of the cleft. Transconjunctival cryotherapy was applied to the sclera with a standard retinal cryoprobe, which was placed with its centre 1.5 mm behind the limbus. Overlapping applications, each with a duration of approximately 2–3 s and a temperature −80 °C, were applied over the extent of the cyclodialysis cleft(s).
Direct cyclopexy
Direct cyclopexy was undertaken in all the cases where initial management with cryotherapy and G. Atropine 1% was unsuccessful in cleft closure. All patients had surgery under general anaesthesia and were admitted for at least 24 h post operation. All patients received G. Apraclonidine 1% 1 h preoperatively to reduce anterior segment vascularity and help prevent postoperative IOP spikes.12
Careful attention was paid to marking the exact location of the cyclodialysis cleft(s) with on-table gonioscopy after the AC was deepened with viscoelastic (Healon, Abbott Medical Optics Inc., Chicago, Illinois, USA). A conjunctival peritomy, which extended 1 clock-hour on either side of the marked cleft, was created. A double-lamellar limbal-based scleral flap technique was used, extending half a clock-hour on either side of the marked cleft and 3 mm posterior to the limbus. The superficial lamellar flap was 50% scleral thickness, and the deep scleral flap was full-thickness down to uveal tract. As the deep scleral flap was opened, it was possible to precisely locate the region of the cyclodialysis cleft(s). The ciliary body was sutured under direct vision to the undersurface of the deep scleral flap and onto the scleral spur, using two rows of 9-0 Nylon horizontal mattress sutures. The deep and superficial scleral flaps were re-approximated using buried 10-0 Nylon interrupted sutures. The conjunctiva and Tenon’s layer were then approximated with buried 8-0 Vicryl mattress sutures. Cryotherapy was applied, as described above, in order to excite an inflammatory reaction and aid cyclodialysis cleft closure. At the end of the procedure, care was taken to remove all the viscoelastic from the anterior chamber. Subconjunctival betamethasone sodium phosphate 0.1% and cefuroxime (125 mg/ml) were administered. The initial postoperative treatment consisted of G. Predforte 1% 6 × day, G. Chloramphenicol 0.5% QDS and G. Atropine 1% OD. Patients were asked to report any significant postoperative pain, to alert clinicians to check the IOP within the first 6–12 h. To control early IOP spikes, systemic (acetazolamide) and/or topical glaucoma medications were used based on the IOP.
Preoperative data collection included patient age, laterality, Snellen best-corrected visual acuity (BCVA), immediate preoperative IOP, number and size of the cyclodialysis clefts identified, the presence of PAS or angle recession, duration of cyclodialysis cleft(s) before closure, and pre-existing ophthalmic pathology. For the purpose of data analysis, the immediate preoperative IOP was used; however, all patients with cyclodialysis cleft(s) demonstrated fluctuating IOP between periods of frank hypotony (≤6 mm Hg) and other periods in which the IOP was low but within the normal range (>6 mm Hg). Postoperative data was collected at days 1, 3, week 1, months 1, 3, 6, 12, and yearly thereafter up to the latest clinic visit. Data collected included IOP, BCVA, time to BCVA improvement (BCVA≥1 Snellen line preoperative BCVA), and time to IOP normalisation (IOP≤21 mm Hg without antiglaucoma medication).
Results
Cleft repair was undertaken in 17 eyes of 17 patients (16 men, 1 woman; mean age, 42±14 years; age range, 16–62 years). Cryrotherapy was initially performed in 14 patients but was successful in cleft closure in 5 patients; direct cycloplexy was required in 12 patients (71%). Initial cleft cryotherapy was not undertaken in three patients, as it was thought that the cleft was too large or that it had previously been attempted at the referring unit. The data of the 17 patients are summarised in Tables 1 and 2. The mean follow-up time following cycloplexy was 43.7±24.6 months (range, 12–110 months). The cyclodialysis clefts were caused by blunt ocular trauma in 16 eyes and penetrating ocular trauma in 1 eye. They were most commonly located inferiorly (in 48% of eyes) followed by superiorly (in 29% of eyes) and equally between nasal and temporal quadrants (14% of eyes each). Intraoperative analysis under OVD identified the mean number of cyclodialysis clefts per eye was 1.5 (range, 1–3) with a mean extent of 2.1±1.6 clock-hours (range, 0.5–6 clock-hours). The mean cleft size between the cryotherapy and direct cycloplexy groups was 0.9±0.4 and 2.5±1.6 clock-hours, respectively. The mean clock-hours of PAS and angle recession were 3.2 and 4.9, respectively. In four eyes (cases 6, 8, 12, and 16), a two-staged direct cycloplexy was performed.
The mean immediate preoperative IOP was 6.9±4.0 mm Hg (range 2–14 mm Hg). In the cryotherapy group, the mean immediate preoperative IOP was 8.0±4.6 mm Hg (range, 3–12 mm Hg) compared with 6.4±3.8 mm Hg (range, 3–14 mm Hg) in the direct cycloplexy group. Postoperatively, painful reversible IOP spikes of up to 70 mm Hg developed in 13 eyes during the first 7 postoperative days. Ten of the 12 eyes (84%) treated with direct cycloplexy encountered an early postoperative IOP spike. The mean IOP during follow-up is illustrated in Figure 1. The final mean postoperative IOP was 12.2±4.1 mm Hg (cleft cryotherapy 11.6±2.1 mm Hg, direct cycloplexy 12.3±4.7 mm Hg). At final follow-up, no cases had persistent raised IOP or secondary glaucomatous optic neuropathy. There were no serious complications related to direct cycloplexy, including suprachoroidal haemorrhage or endophthalmitis.

IOP profile following direct cycloplexy in 12 patients.
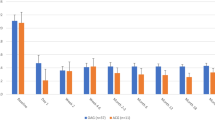
Preoperative BCVA was 6/12 or better in 4 eyes (24%), worse than 6/12 and better than 6/60 in 7 eyes (41%), and 6/60 or worse in 6 eyes (35%). Final BCVA was 6/12 or better in 12 eyes (71%), worse than 6/12 and better than 6/60 in 1 eye (6%), and 6/60 or worse in 4 eyes (24%). This is shown in Figure 2. Of the four eyes with a final BCVA of 6/60 or worse, one patient had a previous surgically repaired macula-off retinal detachment, one patient had a previous macular scar, one patient developed a significant epiretinal membrane, and one patient had persistent postoperative hypotony and declined further surgery. Of the 12 patients who underwent direct cycloplexy, a BCVA of 6/12 or better was present in 2 eyes (17%) preoperatively, which increased to 8 eyes (66%) at final follow-up. In four eyes, cataract surgery was performed following cyclodialysis cleft closure but failed to improve final visual acuity due to pre-existing retinal pathology (cases 3, 10, 11, and 12).

BCVA preoperatively and at final follow-up.
Discussion
The cyclodialysis cleft is an uncommon ophthalmic entity, which can be difficult to diagnose and treat effectively. Spontaneous closure of cyclodialysis clefts is rare and seems to occur only in smaller clefts within 6 weeks of trauma.13 Therefore, in eyes with a cyclodialysis cleft and persistent ocular hypotony, closure should be attempted to normalise IOP, reverse maculopathy, and improve visual acuity, as well as prevent permanent visual loss.
The published outcome data following the repair of cyclodialysis clefts are limited to case reports or small case series and have therefore failed to identify a clear ‘surgical gold standard management.’ In the current study, we evaluated the long-term IOP and visual prognosis in a series of 17 eyes of 17 patients who underwent cleft cryotherapy and/or direct cycloplexy for the repair of cyclodialysis, with a mean follow-up period of 44 months. In the 16 eyes (94%), cleft closure was successful with the resolution of ocular hypotony at final follow-up. In one patient (case 16), despite two direct cycloplexies, ocular hypotony persisted, and the patient declined further intervention. Cleft cryotherapy alone was used as the initial treatment modality in 14 eyes; however, it was successful in cleft closure in 5 eyes (36%). Cleft cryotherapy is particularly useful in the management of smaller clefts (eg, <1–1.5 clock-hours).1, 14 This was evident in our study, where the size of the cyclodialysis cleft requiring direct cycloplexy were almost three times larger than those successfully closed with cryotherapy (2.5 vs 0.9 clock-hours). There was no association between the size of the cleft and the magnitude of hypotony, as previously reported.15
Direct cycloplexy was performed using a double-lamellar limbal-based scleral flap technique.3, 10 An alternative to this technique involves constructing a full-thickness scleral flap as described by Kuche and Naumann7, who reported successful cyclodialysis cleft closure in 28 of the 29 cases. In our series, a double row of mattress sutures were used to oppose the ciliary body to the scleral spur under direct vision, protecting against reopening of the cyclodiaysis cleft(s) during the transient postoperative IOP spike. Reversible early postoperative spikes have been reported following successful cleft closure1, 3, 6, 7, 10, 11, 14, 16 and were observed in 10 of the 12 eyes that underwent direct cycloplexy (83%). As part of the study, we were interested in whether there was a correlation between the extent of anatomical angle damage (clock-hours of PAS and angle recession) and immediate postoperative and final IOP. The immediate postoperative IOP spike was not correlated with the degree of residual anatomical angle damage; implying that functional angle damage was an important additional factor in the acute postoperative rise in IOP. In our practice, we warn all patients that successful cleft closure is often associated with a significant early postoperative IOP spike and recommend a short period of inpatient admission, so that patients can receive intensive IOP and pain management. Despite the magnitude of the postoperative IOP spike, acceptable IOP control was achieved in all the patients by day 7 without the need for further surgical intervention (Figure 1).
The presence of extensive PAS or permanent trabecular dysfunction following a course of protracted ocular hypotony may increase the risk of secondary glaucoma following cleft repair. However, in our case series there were no patients who developed persistent raised IOP or glaucoma at 44 months of follow-up. It is interesting to postulate why this may be. We hypothesise that despite extensive residual anatomical and functional macroscopic cyclodialysis cleft closure, there may be microscopic aqueous drainage into the suprachoroidal space through the residual cyclodialysis cleft bed. The time to IOP normalisation ranged from 2 days to 9 months and has previously been shown to be independent of cleft duration. It has also been suggested that the trabecular dysfunction sustained through ocular hypotony can reverse following cleft closure and may partly explain the gradual normalisation of IOP.16
Prolonged periods of ocular hypotony may lead to irreversible macuolpathy and fibrosis.17 It has therefore been inferred that early intervention following cleft formation is necessary to optimise visual recovery. In our study, of the 12 patients who underwent direct cycloplexy the number achieving 6/12 or better visual acuity improved by 50% at the final follow-up. Furthermore, the visual acuity of a patient (case 13) who underwent direct cycloplexy 50 months after cyclodialysis improved from 6/24 to 6/9 and that of another patient (case 15) who underwent cycloplexy 27 months after cyclodialysis improved from 6/36 to 6/6. Similarly one patient (case 1) treated with cleft cryotherapy alone, 16 months after trauma, improved from 1/60 to 6/7.5 (Tables 1 and 2). This highlights that cyclodialysis cleft repair can be beneficial even in cases with protracted periods of hypotony and that surgical treatment should not be rejected based on the duration of hypotony.7, 16
In conclusion, the successful closure of cyclodialysis clefts through direct surgical cycloplexy and/or cleft cryotherapy can achieve a good long-term visual prognosis, with stable IOP control. A protracted history of hypotony should not necessarily deter the clinician from surgical intervention and should be considered before the onset of irreversible retinal pathology.

References
Ioannidis AS, Barton K . Cyclodialysis cleft: causes and repair. Curr Opin Ophthalmol 2010; 21: 150–154.
Shaffer RN, Weiss DL . Concerning cyclodialysis and hypotony. Arch Ophthalmol 1962; 68: 55–61.
Mushtaq B, Chiang MY, Kumar V, Ramanathan US, Shah P . Phacoemulsification, persistent hypotony and cyclodialysis clefts. J Cataract Refract Surg 2005; 31: 1428–1432.
Nolan W . Anterior segment imaging: ultrasound biomicroscopy and anterior segment optical coherence tomography. Curr Opin Ophthalmol 2008; 19: 115–121.
Dada T, Gadia R, Sharma A, Ichhpujani P, Bali SJ, Bhartiya S et al. Ultrasound biomicroscopy in glaucoma. Surv Ophthalmol 2011; 56: 433–450.
Ormerod LD, Baerveldt G, Green RL . Cyclodialysis clefts: natural history, assessment and management. In: Weinstein GW (ed). Open Angle Glaucoma. Churchill Livingstone: New York, NY, USA, 1986; 201–225.
Kuchle M, Naumann GOH . Direct cycloplexy for traumatic cyclodialysis with persisting hypotony; report in 29 consecutive patients. Ophthalmology 1995; 102: 322–233.
Mandava N, Kahook MY, Mackenzie DL, Olson JL . Anterior scleral buckling procedure for cyclodialysis cleft with chronic hypotony. Ophthalmic Surg Lasers Imaging 2006; 37: 151–153.
Hoerauf H, Roider J, Laqua H . Treatment of traumatic cyclodialysis with vitractomy, cryotherapy, and gas tamponade. J Cataract Refract Surg 1999; 25: 1299–1301.
Aminlari A, Callahan CE . Medical, laser, and surgical management of inadvertent cyclodialysis cleft with hypotony. Arch Ophthalmol 2004; 122: 399–404.
Krohn J . Cryotherapy in the treatment of cyclodialysis cleft induced hypotony. Acta Ophthalmol Scand 1997; 75: 96–98.
Sii F, Todd B, Shah P, Chiang M . Reduction of anterior-segment vascularity with preoperative topical apraclonidine 1%. J Cataract Refract Surg 2006; 32: 692–693.
Parnes RE, Dailey JR, Aminlari A . Hypotonous cyclodialysis cleft following anterior chamber intraocular lens removal. Ophthalmic Surg 1994; 25: 386–387.
Brown SVL, Mizen T . Transscleral diode laser therapy for traumatic cyclodialysis cleft. Ophthalmic Surg Lasers 1997; 28: 313–317.
Malandrini A, Balestrazzi A, Martone G, Tosi GM, Caporossi A . Diagnosis and management of traumatic cyclodialysis cleft. J Cataract Refract Surg 2008; 34: 1213–1216.
Hwang JM, Ahn K, Kim C, Park KA, Kee C . Ultrasound biomicroscopic evaluation of cyclodialysis before and after direct cycloplexy. Arch Ophthalmol 2008; 126: 1222–1225.
Costa VP, Arcieri ES . Hypotony maculopathy. Acta Ophthalmol Scand 2007; 85: 586–597.
Acknowledgements
The authors have received no external funding.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Disclaimer
Some consent practices reported are not in accordance with the RCOphth recommendations.
Rights and permissions
About this article
Cite this article
Agrawal, P., Shah, P. Long-term outcomes following the surgical repair of traumatic cyclodialysis clefts. Eye 27, 1347–1352 (2013). https://doi.org/10.1038/eye.2013.183
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/eye.2013.183
Keywords
This article is cited by
-
Management der posttraumatischen Bulbushypotonie
Der Ophthalmologe (2021)
-
Ciliary body suturing using intraocular irrigation for traumatic cyclodialysis: two case reports
Journal of Medical Case Reports (2020)
-
Cyclodialysis: an update
International Ophthalmology (2017)
-
Long-term outcomes of argon laser photocoagulation in small size cyclodialysis cleft
BMC Ophthalmology (2015)
