
Abstract
Corneal ectasias, among which keratoconus (KC) is the single most common entity, are one of the most frequent reasons for corneal grafting in developed countries and a threatening complication of laser in situ keratomileusis. Genome-wide association studies have previously found lysyl oxidase (LOX) and hepatocyte growth factor (HGF) associated with susceptibility to KC development. The aim of our study was to validate the effects of seven single-nucleotide polymorphisms (SNPs) within LOX and HGF over KC. Unrelated Czech cases with KC of European descent (108 males and 57 females, 165 cases in total) and 193 population and gender-matched controls were genotyped using Kompetitive Allele Specific PCR assays. Fisher’s exact tests were used to assess the strength of associations. Evidence for association was found for both of the tested loci. It was strongest for rs3735520:G>A near HGF (allelic test odds ratio (OR)=1.45; 95% confidence interval (CI), 1.06–1.98; P=0.018) with A allele being a risk factor and rs2956540:G>C (OR=0.69; 95% CI, 0.50–0.96; P=0.024) within LOX with C allele having a protective effect. This first independent association validation of rs2956540:G>C and rs3735520:G>A suggests that these SNPs may serve as genetic risk markers for KC in individuals of European descent.
Similar content being viewed by others


Introduction
Keratoconus (KC) is characterised by progressive corneal thinning and ectasia, leading to significant refractive error and potential scarring.1 KC prevalence in populations of European descent varies from 5.5 to 8.6 per 10 000 inhabitants2, 3 and is more common in males.4, 5
Although most KC cases are sporadic, familial aggregations and twin studies suggest a strong genetic component in the aetiopathogenesis of the disease.6, 7
Single-nucleotide polymorphisms (SNPs) in two genes, lysyl oxidase (LOX; OMIM *153455) and hepatocyte growth factor (HGF; OMIM *142409), identified by a genome-wide association study (GWAS) have been reported to increase susceptibility to KC.8, 9 In this study we attempted replication for seven SNPs in LOX and HGF in a Czech case-control cohort.
Materials and methods
The study followed the ethical standards of the Ethics Committee of the General Teaching Hospital in Prague and Charles University in Prague, and adhered to the tenets set out in the Declaration of Helsinki.
A total of 165 unrelated cases with KC were included in the study: 57 females and 108 males, average age at enrolment was 37.2±13.3 years (range 15–69 years). The diagnosis of KC was made in agreement by two cornea specialists. All cases exhibited KC pattern on anterior sagittal maps together with localised corneal thinning in at least one eye.1 Only patients with KC grade 1 or higher according to the Oculus topographic KC classification based on data obtained by Pentacam (Oculus Optikgeräte GmbH, Wetzlar, Germany) were included.10 Some eyes had advanced disease with typical signs such as Vogt striae, Fleischer ring and stromal scarring, but this was not an inclusion requirement for the purposes of this study. Bilaterally grafted patients for KC were also considered affected and thus included in the study.
193 unrelated Czech Caucasian individuals (79 females, 114 males average age of 39.5±13.7 years, range 20–81 years) were recruited as controls. They self-reported absence of any ocular conditions impairing vision, other than age-related cataract.
DNA was extracted from venous blood by conventional methods, in some patients Oragene saliva kit was used (Oragene OG-300, DNA Genotek, Ottawa, ON, Canada). SNPs reported to show the strongest associations, although not reaching genome-wide significance, in GWAS8, 9 were tested (Supplementary Table 1). Genotyping was performed using custom designed Kompetitive Allele Specific PCR (KASP) assays at LGC Genomics (LGC Genomics, Hoddesdon, UK). KASP enables bi-allelic discrimination through a competitive PCR harnessing the fluorescence resonance energy transfer principle and it has been shown to have high reliability (98.4–99.3%).11 For the purpose of this study KASP genotyping assays were designed towards sequences shown in Supplementary Table 1. For internal quality control 10 samples were randomly selected and PCR fragment containing rs1800449:C>T was Sanger sequenced.12 The concordance rate was 100%.
Fisher’s exact tests were used to calculate odds ratios (ORs) and probabilities of association. The primary model was the allelic test, which assumes co-dominance. Secondary analyses of association under assumptions of dominant and recessive models were also carried out for each SNP. All statistical analyses were done using STATA 12 (STATA Corp., College Station, TX, USA). An α<0.05 was chosen as the statistical significance threshold for validation, because the analysed variants were pre-selected on the basis of strong prior probabilities of association. Methodology used as well as results of our study were submitted to the GWAS Central database (http://www.gwascentral.org/study/HGVST1826).
Results
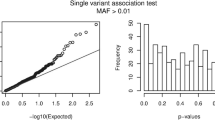
The genotype call rate for each SNP was >99.3%. All SNPs were in Hardy–Weinberg equilibrium (P>0.05) in both the controls and in the combined case-control panel. Allele frequencies in the control group were largely in line with those reported in panels of other European ethnic groups by the HapMap project (http://hapmap.ncbi.nlm.nih.gov/; Table 1).
Two out of the seven SNPs analysed showed significant association with KC in a co-dominant allelic test (Table 1). The rs2956540:G>C, located within in the fourth intron of the LOX gene (OR=0.69; 95% CI, 0.50–0.96 for allele C; P=0.024) and rs3735520:G>A located in genomic region upstream of the HGF transcription initiation site (OR=1.45; 95% CI, 1.06–1.98 for allele A; P=0.018). Explorations of alternative models of inheritance changed little the association significance for both loci, although genotypes homozygous for alleles increasing susceptibility to KC were associated with higher ORs than under the allelic (co-dominant) model, suggesting (although not proving) a possible recessive effect in both SNPs.
Discussion
Our study provides the first independent validation of rs2956540:G>C (minor allele serving as a protective factor) and rs3735520:G>A (minor allele serving as a risk factor) associations with KC in a population of European descent, further confirming that LOX and HGF genes have a role in the aetiology of the disease.8, 9
Details on previous association studies (population origin, genotyping methods used, number of KC and control samples and reported P-values) on the LOX and HGF locus are shown in Supplementary Table 2.
Recently, association of the HGF locus was also achieved in an independent study comprising population of European descent from Australia.13 However, alternative SNPs to those shown statistically significant associations with KC in GWAS were tested.8, 13
LOX enzyme catalyses the final enzymatic reaction required for cross-linking of two basic components of extracellular matrix, collagens and elastin. Although the underlying mechanism of common variants contributing to the disease development remains unknown, the potential effect could lie in affecting the biologic activity of LOX via tissue specific alternative splicing or regulation of expression.14 Mechanisms of how common variants within the HGF gene alter susceptibility to KC are yet to be determined, but involvement of inflammatory pathways has been previously suggested.8
The main statistics used here (allelic test) implicitly assume co-dominance, and is similar to the additive models assumed in the previous reports.8, 9, 13, 15 Although some caution is invited in the interpretation of our findings because of the relatively small sample size, the validation of rs2956540:G>C and rs3735520:G>A showing the same effect directions as previous studies in populations of European ancestry adds weight to the existing evidence.8, 9 Although not reaching a statistically significant threshold, the higher MAF of rs1800449:C>T and rs10519694:C>T in controls compared with the KC cases in our study, was consistent with protective effects of these alleles reported in another study using Caucasian case-control panels (Supplementary Table 2).9
rs1014091:G>A and rs17501108:G>T were previously also shown to have a protective effect,8 whereas in our study their MAF was higher in KC cases that, albeit not statistically significant, indicated a tendency towards the opposite direction of the effect. The failure to replicate the effect direction may be caused by differences in linkage disequilibrium patterns (Supplementary Table 3) between these markers and the causative variants within the same gene in the Czech population.
References
Vazirani J, Basu S : Keratoconus: current perspectives. Clin Ophthalmol 2013; 7: 2019–2030.
Kennedy RH, Bourne WM, Dyer JA : A 48-year clinical and epidemiologic study of keratoconus. Am J Ophthalmol 1986; 101: 267–273.
Nielsen K, Hjortdal J, Aagaard Nohr E, Ehlers N : Incidence and prevalence of keratoconus in Denmark. Acta Ophthalmol Scand 2007; 85: 890–892.
Ihalainen A : Clinical and epidemiological features of keratoconus genetic and external factors in the pathogenesis of the disease. Acta Ophthalmol Suppl 1986; 178: 1–64.
Weed KH, McGhee CN : Referral patterns, treatment management and visual outcome in keratoconus. Eye (Lond) 1998; 12: 663–668.
Burdon KP, Vincent AL : Insights into keratoconus from a genetic perspective. Clin Exp Optom 2013; 96: 146–154.
Tuft SJ, Hassan H, George S, Frazer DG, Willoughby CE, Liskova P : Keratoconus in 18 pairs of twins. Acta Ophthalmol 2012; 90: e482–e486.
Burdon KP, Macgregor S, Bykhovskaya Y et al: Association of polymorphisms in the hepatocyte growth factor gene promoter with keratoconus. Invest Ophthalmol Vis Sci 2011; 52: 8514–8519.
Bykhovskaya Y, Li X, Epifantseva I et al: Variation in the lysyl oxidase (LOX gene is associated with keratoconus in family-based and case-control studies. Invest Ophthalmol Vis Sci 2012; 53: 4152–4157.
Kanellopoulos AJ, Asimellis G : Revisiting keratoconus diagnosis and progression classification based on evaluation of corneal asymmetry indices, derived from Scheimpflug imaging in keratoconic and suspect cases. Clin Ophthalmol 2013; 7: 1539–1548.
Semang K, Babu R, Hearne S, Olsen M : Single nucleotide polymorphism genotyping using Kompetitive Allele Specific PCR (KASP): overview of the technology and its application in crop improvement. Mol Breeding 2013; 33: 1–14.
Liskova P, Hysi PG, Williams D et al: Study of p.N247S KERA mutation in a British family with cornea plana. Mol Vis 2007; 13: 1339–1347.
Sahebjada S, Schache M, Richardson AJ, Snibson G, Daniell M, Baird PN : Association of the hepatocyte growth factor gene with keratoconus in an Australian population. PLoS One 2014; 9: e84067.
Dudakova L, Liskova P, Trojek T, Palos M, Kalasova S, Jirsova K : Changes in lysyl oxidase (LOX) distribution and its decreased activity in keratoconus corneas. Exp Eye Res 2012; 104: 74–81.
Hasanian-Langroudi F, Saravani R, Validad MH, Bahari G, Yari D : Association of Lysyl oxidase (LOX) polymorphisms with the risk of Keratoconus in an Iranian population. Ophthalmic Genet 2014, e-pub ahead of print 6 February 2014.
Acknowledgements
This work was supported by GAUK 562313/2013 and PRVOUK-P24/LF1/3 programs of the Charles University in Prague. LD was also supported by SVV 260022/2014 and PL by UNCE 204011.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Supplementary Information accompanies this paper on European Journal of Human Genetics website
Rights and permissions
About this article

Cite this article
Dudakova, L., Palos, M., Jirsova, K. et al. Validation of rs2956540:G>C and rs3735520:G>A association with keratoconus in a population of European descent. Eur J Hum Genet 23, 1581–1583 (2015). https://doi.org/10.1038/ejhg.2015.28
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/ejhg.2015.28
This article is cited by
-
Three novel variants identified within ECM-related genes in Chinese Han keratoconus patients
Scientific Reports (2020)
-
Do age-related macular degeneration genes show association with keratoconus?
Eye and Vision (2019)
-
Genetic Aspects of Keratoconus: A Literature Review Exploring Potential Genetic Contributions and Possible Genetic Relationships with Comorbidities
Ophthalmology and Therapy (2018)
-
Genetic associations for keratoconus: a systematic review and meta-analysis
Scientific Reports (2017)
-
Genetics in Keratoconus: where are we?
Eye and Vision (2016)
