
Abstract
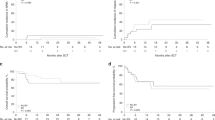
We analyzed 113 patients with lymphoma who underwent allogeneic transplantation with reduced-intensity conditioning (allo-RIC) regimens at a single institution, from February 2001 through November 2009, searching for factors predictive of the outcome. At the time of transplantation, 60% of patients were in CR, 29% in PR and 11% had progressive or stable disease. At a median follow-up of 34 months (confidence interval (CI) 17–45), the 3-year OS and PFS were 59% (CI 48–68%) and 51% (CI 41–61%), respectively. The 100-day and 2-year nonrelapse mortalities (NRM) were 6% and 28% (CI 20–35%), respectively. Grade II–IV acute GVHD (aGVHD) incidence was 38%, and the global incidence of chronic GVHD was 33%. In univariate analysis, OS was influenced by disease status before allo-RIC; aGVHD negatively affected on survival. Similarly, PFS was influenced only by disease status. Histological subtype did not affect OS or PFS. We conclude that disease status at the time of transplantation significantly influences survival in patients receiving allo-RIC for lymphoma, whereas histological subtype does not. This reinforces the need to administer more effective debulking treatments to lymphoma patients, for optimal benefit of allogeneic immune recognition of minimal residual disease, independently from lymphoma histology.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout





Similar content being viewed by others


References
Robinson SP, Goldstone AH, Mackinnon S, Carella A, Russell N, de Elvira CR et al. Chemoresistant or aggressive lymphoma predicts for a poor outcome following reduced-intensity allogeneic progenitor cell transplantation: an analysis from the lymphoma working party of the European Group for blood and bone marrow transplantation. Blood 2002; 100: 4310–4316.
Rezvani AR, Norasetthada L, Gooley T, Sorror M, Bouvier ME, Sahebi F et al. Non-myeloablative allogeneic haematopoietic cell transplantation for relapsed diffuse large B-cell lymphoma: a multicentre experience. Br J Haematol 2008; 143: 395–403.
Sureda A, Canals C, Arranz R, Caballero D, Ribera JM, Brune M et al. Allogeneic stem cell transplantation after reduced intensity conditioning in patients with relapsed or refractory Hodgkin’s lymphoma. Results of the HDR-ALLO study - a prospective clinical trial by the Grupo Español de Linfomas/Trasplante de Médula Osea (GEL/TAMO) and the lymphoma working party of the European Group for blood and marrow transplantation. Haematologica 2012; 97: 310–317.
Le Gouill S, Milpied N, Buzyn A, De Latour RP, Vernant JP, Mohty M et al. Graft-versus-lymphoma effect for aggressive T-cell lymphomas in adults: a study by the Société Francaise de Greffe de Moëlle et de Thérapie Cellulaire. J Clin Oncol 2008; 26: 2264–2271.
Khouri IF, Saliba RM, Giralt SA, Lee MS, Okoroji GJ, Hagemeister FB et al. Nonablative allogeneic hematopoietic transplantation as adoptive immunotherapy for indolent lymphoma: low incidence of toxicity, acute graft-versus-host disease, and treatment-related mortality. Blood 2001; 98: 3595–3599.
Tam CS, Bassett R, Ledesma C, Korbling M, Alousi A, Hosing C et al. Mature results of the M. D. Anderson Cancer Center risk-adapted transplantation strategy in mantle cell lymphoma. Blood 2009; 113: 4144–4152.
Chakraverty R, Mackinnon S . Allogeneic transplantation for lymphoma. Clin Oncol 2011; 29: 1855–1863.
Kyriakou C, Canals C, Finke J, Kobbe G, Harousseau JL, Kolb HJ et al. Allogeneic stem cell transplantation is able to induce long-term remissions in angioimmunoblastic T-cell lymphoma: a retrospective study from the lymphoma working party of the European group for blood and marrow transplantation. J Clin Oncol 2009; 27: 3951–3958.
Milpied N, Fielding AK, Pearce RM, Ernst P, Goldstone AH . Allogeneic bone marrow transplant is not better than autologous transplant for patients with relapsed Hodgkin’s disease. European Group for Blood and Bone Marrow Transplantation. J Clin Oncol 1996; 14: 1291–1296.
Akpek G, Ambinder RF, Piantadosi S, Abrams RA, Brodsky RA, Vogelsang GB et al. Long-term results of blood and marrow transplantation for Hodgkin’s lymphoma. J Clin Oncol 2001; 19: 4314–4321.
Sorror M, Storer B, Sandmaier BM, Maloney DG, Chauncey TR, Langston A et al. Hematopoietic cell transplantation-comorbidity index and Karnofsky performance status are independent predictors of morbidity and mortality after allogeneic nonmyeloablative hematopoietic cell transplantation. Cancer 2008; 112: 1992–2001.
Armand P, Kim HT, Ho VT, Cutler CS, Koreth J, Antin JH et al. Allogeneic transplantation with reduced-intensity conditioning for Hodgkin and non-Hodgkin lymphoma: importance of histology for outcome. Biol Blood Marrow Transplant 2008; 14: 418–425.
Corradini P, Dodero A, Farina L, Fanin R, Patriarca F, Miceli R et al. Allogeneic stem cell transplantation following reduced-intensity conditioning can induce durable clinical and molecular remissions in relapsed lymphomas: pre-transplant disease status and histotype heavily influence outcome. Leukemia 2007; 21: 2316–2323.
Kahl C, Storer BE, Sandmaier BM, Mielcarek M, Maris MB, Blume KG et al. Relapse risk in patients with malignant diseases given allogeneic hematopoietic cell transplantation after nonmyeloablative conditioning. Blood 2007; 110: 2744–2748.
Blaise D, Tabrizi R, Boher JM, Le Corroller-Soriano AG, Bay JO, Fegueux N et al. Randomized study of 2 reduced-intensity conditioning strategies for human leukocyte antigen-matched, related allogeneic peripheral blood stem cell transplantation: prospective clinical and socioeconomic evaluation. Cancer, (e-pub ahead of print 14 August 2012; doi:10.1002/cncr.27786).
Mohty M, Bay JO, Faucher C, Choufi B, Bilger K, Tournilhac O et al. Graft-versus-host disease following allogeneic transplantation from HLA-identical sibling with antithymocyte globulin-based reduced-intensity preparative regimen. Blood 2003; 102: 470–476.
Morris E, Thomson K, Craddock C, Mahendra P, Milligan D, Cook G et al. Outcomes after alemtuzumab-containing reduced-intensity allogeneic transplantation regimen for relapsed and refractory non-Hodgkin lymphoma. Blood 2004; 104: 3865–3871.
Robinson SP, Sureda A, Canals C, Russell N, Caballero D, Bacigalupo A et al. Reduced intensity conditioning allogeneic stem cell transplantation for Hodgkin’s lymphoma: identification of prognostic factors predicting outcome. Haematologica 2009; 94: 230–238.
Vigouroux S, Michallet M, Porcher R, Attal M, Ades L, Bernard M et al. Long-term outcomes after reduced-intensity conditioning allogeneic stem cell transplantation for low-grade lymphoma: a survey by the French Society of Bone Marrow Graft Transplantation and Cellular Therapy (SFGM-TC). Haematologica 2007; 92: 627–634.
Hari P, Carreras J, Zhang MJ, Gale RP, Bolwell BJ, Bredeson CN et al. Allogeneic transplants in follicular lymphoma: higher risk of disease progression after reduced-intensity compared to myeloablative conditioning. Biol Blood Marrow Transplant 2008; 14: 236–245.
Armand P, Gibson CJ, Cutler C, Ho VT, Koreth J, Alyea EP et al. A disease risk index for patients undergoing allogeneic stem cell transplantation. Blood 2012; 120: 905–913.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Castagna, L., Boubdallah, R., Furst, S. et al. Disease status is a more reliable predictive factor than histology in lymphoma patients after reduced-intensity conditioning regimen and allo-SCT. Bone Marrow Transplant 48, 794–798 (2013). https://doi.org/10.1038/bmt.2012.225
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/bmt.2012.225
