
Abstract
Data sources
The Cochrane Oral Health Groups Trial Register, Medline, Embase and PsycINFO.
Study selection
Randomised controlled trials (RCTs), controlled clinical trials (CCTs), cohort studies or case-control studies were considered. Only studies in patients aged 18 or older with pre-existing periodontal disease and clearly stating a psychological model or theory had been used were included. Studies exploring smoking cessation were not included.
Data extraction and synthesis
All data were collected by a single author using pre-decided parameters. The reviewers used the Cochrane criteria to assess risk of bias in clinical trials and the Newcastle Ottawa Scale for observational studies. Marked heterogeneity from the wide variety of psychological approaches used in the studies prevented meta-analysis.
Results
Fifteen papers relating to 14 different studies were included from an initial 722 articles identified. This included three cohort studies, ten RCTs and a before/after study. A total of 1,106 patients were included across the studies. Of the 19 psychological models included in the initial search, seven were shown to have some form of impact on oral hygiene motivation, demonstrated by observed behavioural and clinical outcomes.
Conclusions
The authors concluded that, in adult patients with pre-existing periodontal disease, understanding of the seriousness of periodontal disease and the benefits of behavioural change resulted in improved adherence to oral hygiene instructions. They concluded that goal-setting, self-monitoring and indeed planning can be useful in improving oral health-related behaviours.
Similar content being viewed by others
Commentary
The need for improved plaque control in periodontal disease, and for that matter caries, has long been considered one of the main factors contributing to optimal oral health. A dental care professional would be remiss for not discussing, and actively demonstrating to a patient how to achieve good oral health.
The evidence however for the effectiveness of standard oral hygiene advice given in a practice setting is low. Harris1 demonstrated that one to one dietary interventions could change behaviour, but the evidence behind one-to-one interventions and changing sugar consumption was less convincing. The need for innovative ways for dental care professionals to influence oral health is welcome, and mechanisms which rely on psychological constructs such as motivational interviewing have shown promise.2
A systematic review summarises the results of available studies.3 The authors searched Cochrane, Medline, Embase and PsycINFO. Although there were no language restrictions on their search, it would have been useful to include searches in other languages, and databases which include other languages, eg Chinese, and Latin American publications. The age group was appropriate given the periodontal disease focus, however it would have been interesting to see how age would have influenced psychological constructs in a younger group. It is interesting that Werner,2 in a similar paper, included people 13 years or older.
In many of the papers reviewed, as the authors point out, sample sizes seemed quite low; in Weinstein et al.'s paper4 there were only 20 participants, in Stenman's5 there were 44 and in Jonsson's6 there were 37 participants. Even though the literature does not specifically state what is a minimum sample size for randomised controlled trials, it does seem difficult with such small sample sizes to be convinced if the conclusion and statistical vigour is somehow biased due to the small size of the sample; with the result perhaps not related to the intervention but relating to the variability within the small number of participants.
As well as the questionnaire sample sizes, for at least one of the studies the follow-up was only three months,7 long enough perhaps to measure change in behaviour, but not long enough to determine if the behaviour change is long-term. A clinician is interested in longer term behavioural changes (ie changes in one or two years) and most of the studies reviewed regrettably measured behavioural changes for only 12 months.
It is noted that the searches were conducted by one author who also assessed the studies by examining titles, etc. It may have added to the quality of the systematic review if this had been conducted along the lines of Cochrane methodology with two authors assessing studies.7 For the unenlightened reader, although not an aim of the paper, it would have also been useful to have a written brief description of what the models meant.
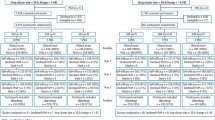
The authors include a complete list of the search terms used to enable the review to be easily completed, with a clear consort diagram showing the number of records identified, screened, deemed eligible and included. The authors should be commended for not only including a table of included studies but also a table of excluded studies for completeness. Listing excluded papers is not reliably part of systematic reviews and does help aid in transparency in the review process. Similarly, the summary of key studies enables a reader to determine their own view of the quality of the papers reviewed. To understand the relevance of this study to a particular patient group it would have been useful to know more about the studies' participants. Factors such as age, smoking status and socio-economic status are all known to influence behaviour8 and it would have been good to have included these details.
Newton included a risk of bias suggested by the Cochrane reviewers' handbook for RCTs, and the Newcastle Ottawa Quality Assessment scale for cohort and case control studies. To add to the readability it would have been handy perhaps to have plotted risk of bias as a Cochrane inspired red, amber, green (traffic light) figure.9
Newton concludes that there is a relationship between the perception of a patient of the benefits of behavioural change and the seriousness of the disease. He also adds that interventions based on the use of goal-setting, self-monitoring and planning are effective in improving oral health-related behaviours.
Newton is right of course, there is a relationship, but as he acknowledges it is probably weak due to the sheer heterogeneity of the different studies, based on different theories and constructs, in addition to the flaws discussed above. The papers all had a psychological construct as their basis, but included just two based on a health belief model, one on a health locus of control, three on social learning theory, one on the theory of planned behaviour, one on implementation intention, two on cognitive behavioural interaction and three on motivational interviewing. As Newton also suggested the interactions weren't always conducted as one would expect. In all three motivation interviewing interventions, which should have appropriate time allowed, 15 minutes was allocated to the psychological intervention, which may not be sufficient time to be effective at improving outcomes.10
Newton's conclusions should also be considered by the reader along with the recent publication by Weiner.2 Weiner's systematic review looked at ‘psychological interventions for poor oral health’ rather than oral hygiene in periodontal disease with a differing, but perhaps supportive conclusion; psychological interventions should not yet be routinely provided in dental care for patients with poor oral health, and they should be restricted in patients if the benefits, risks, cost-effectiveness and ethical aspects are taken into account.
Practice point
-
Practitioners should consider that oral hygiene advice based on a psychological construct may be more effective than oral health advice without.
References
Harris R, Gamboa A, Dailey Y, Ashcroft A . One-to-one dietary interventions undertaken in a dental setting to change dietary behaviour. Cochrane Database Syst Rev, 2012, 3: Art. No. CD006540. DOI: 10.1002/14651858.CD006540.pub2.
Werner H, Hakeberg M, Dahlström L, et al. Psychological Interventions for Poor Oral Health: A Systematic Review. J Dent Res 2016; 95: 506–514. doi: 10.1177/0022034516628506. Epub 2016 Jan 29.
Cochrane Handbook for Systematic Reviews of Interventions. Available at: http://consumers.cochrane.org/what-systematic-review (accessed October 2016).
Weinstein R, Tosolin F, Ghilardi L, Zanardelli E . Psychological intervention in patients with poor compliance. J Clin Periodontol, 1996; 23: 283–288.
Stenman J, Lundgren J, Wennström JL, Ericsson JS, Abrahamsson KH . A single session of motivational interviewing as an additive means to improve adherence in periodontal infection control: a randomized controlled trial. J Clin Periodontol 2012; 39: 947–954. doi: 10.1111/j.1600-051X.2012.01926.x.
Jönsson B, Lindberg P, Oscarson N, Öhrn K . Improved compliance and self-care in patients with periodontitis--a randomized control trial. Int J Dent Hyg 2006; 4: 77–83. doi:10.1111/j.1601-5037.2006.00175.x
Higgins JPT . Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available at http://handbook.cochrane.org (accessed February 2016).
Albarracin D, Gillette JC, Earl AN, Glasman LR, Durantini MR . A test of major assumptions about behaviour change: A comprehensive look at the effects of passive and active HIV-prevention interventions since the beginning of the epidemic. Psychol Bull 2005; 131: 856–897.
Cochrane Handbook for Systematic Reviews of Interventions. Available at: http://handbook.cochrane.org/chapter_8/figure_8_6_c_example_of_a_risk_of_bias_summary_figure.htm (accessed March 2017).
Miller WR, Rollnick S . Ten things that motivational interviewing is not. Behav Cogn Psychother 2009; 37: 129–140. doi: 10.1017/S1352465809005128.
Author information
Authors and Affiliations
Additional information
Address for correspondence: J Timothy Newton, Social & Behavioural Sciences Population & Patient Health, King's College London Dental Institute, Guy's Hospital campus, London, UK. E-mail: tim.newton@kcl.ac.uk
Newton JT, Asimakopoulou K. Managing oral hygiene as a risk factor for periodontal disease: a systematic review of psychological approaches to behaviour change for improved plaque control in periodontal management. J Clin Periodontol 2015; 42: S36–46.
Rights and permissions
About this article

Cite this article
Duane, B. Psychological approaches to behaviour for improving plaque control. Evid Based Dent 18, 3–4 (2017). https://doi.org/10.1038/sj.ebd.6401213
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ebd.6401213
This article is cited by
-
Management of plaque in people experiencing homelessness using 'peer education': a pilot study
British Dental Journal (2019)
