
Abstract
Data sources
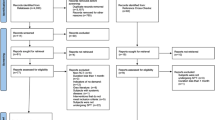
Medline, Embase, The Cochrane Oral Health Group's Trials Register, CENTRAL, UK National Research Register, ISI Proceedings, hand search of relevant journals for 2000-2008. References from selected articles and contact with authors.
Study selection
Randomised controlled trials in any language comparing scaling and root planing (SRP) alone and SRP with PDT in patients with chronic periodontitis, with a mean follow up of at least 12 weeks. The primary outcome measure was the change in clinical attachment loss (CAL). Secondary outcomes were changes in probing depth (PD) and gingival recession (GR).
Data extraction and synthesis
Data were extracted by a single reviewer using a standard extraction form. Quality was assessed using both the Jadad scale and the allocation concealment component of the Cochrane risk of bias tool. Meta-analysis was conducted using the random effects model. Heterogeneity was assessed using the chi-squared-based Q statistic method and Higgins' I2 test.
Results
Four trials with 101 participants were included. The risk of bias of these trials was considered to be moderate. The mean difference in CAL at 12 weeks was 0.29 mm (95% CI 0.08–0.50, p=0.007). Heterogeneity was high using both the Chi2 and I2 tests.
Conclusions
The review suggests there may be a minor improvement in clinical attachment loss at 12 weeks. It is unclear whether this is a clinically meaningful improvement.
Similar content being viewed by others


Commentary
In the introduction, the author explains the microbiological aetiology of periodontitis (although the references may be too old), and justifies the adjunctive use of Antimicrobial Photodynamic therapy (aPDT) in periodontal therapy, based on their antimicrobial effects and on the limitations of other adjunctive therapies (such as local and systemic antimicrobials). Among these limitations, the increase in bacterial resistance and biofilm resistance are enumerated, although the second one should not be included, when these therapies are used as adjuncts to mechanical debridement.
This review aimed to compare scaling and root planing (SRP) plus aPDT versus SRP alone. An extensive search lead to the evaluation of 14 full-text papers, and four of them were excluded due to the use of 'high-level lasers', a criterion that was not mentioned in the paper. Finally, four papers were included, two of them performed by the same research group.
The studies presented some heterogeneity, with one of them following a split mouth-design. One of the most important issues of the review is that it is not reported how many sites were measured in each patient and how the sites were selected. In addition, it seems that the author has performed a site-based analysis, according to the data provided in the figures.
Meta-analyses of the four studies were performed for the primary outcome variable (Clinical Attachment Level –CAL- changes) and one of the secondary outcomes (Probing Pocket Depth –PPD- changes). Surprisingly, gingival recession was selected as one of the variables in the inclusion criteria, when it just represents the difference between CAL and PPD. Bleeding on probing (BOP), a more meaningful clinical variable, and microbiological variables (highlighted in the introduction) were only marginally considered.
A significant difference of 0.29mm in CAL change was calculated in the meta-analyses, and a non-significant difference of 0.11mm in PPD change, both favouring the adjunctive therapy, at the 12-week evaluation. The differences were of small magnitude with no associated adverse effects. However, the differences among the studies were obvious, with two studies with a clear impact in both variables 1, 2 , and two studies (those performed by the same group) with smaller impact and minor differences among groups.3, 4 The first two studies had a 12-week follow up, while the last two had a 24-week duration, although the 12-week results were included in the meta-analysis. In addition, one of last two studies included patients in supportive periodontal therapy (already treated and following a secondary prevention program), despite the inclusion criterion of the review of 'untreated chronic periodontitis'.
In the discussion, the limitations of this systematic review are acknowledged, including the design of the review with just one examiner. No mention is made of the need for patient-based analysis as opposed to site-based analysis. Site-based analysis is not considered adequate in periodontal therapy, since all the sites from the same patient are influenced by the same systemic factors (such as smoking or genetics), and therefore all the sites from different patients should not be combined. In addition, 12 weeks of follow-up may only be considered as short-term. Longer follow-ups are needed to define the real benefits of a therapy.
In a recent commentary5, another systematic review on the topic was evaluated.6 It included five papers, three papers in common with those included in the present review.1, 2, 3 Two additional papers were included.7, 8 Meta-analysis for changes in CAL (two studies) demonstrated a significant benefit for the SRP plus aPDT of 0.34 mm (95% CI 0.05-0.63) and for PPD (three studies) of 0.25 mm (95% CI 0.04-0.45), which is similar to the results reported in the present review. However, in the review by Azarpazhooh et al. (2010) a clear patient-based approach was taken.
Practice point
-
Patient-based analysis should be carried out when evaluating periodontal treatments. Statistically significant differences may not represent significant clinical benefits when assessing. In addition, a 12-week follow-up is very limited and longer-term studies are clearly needed.
References
Andersen R, Loebel N, Hammond D, Wilson M . Treatment of periodontal disease by photodisinfection compared to scaling and root planing. J Clin Dent 2007: 18: 34–38.
Braun A, Dehn C, Krause F, Jepsen S . Short-term clinical effects of adjunctive antimicrobial photodynamic therapy in periodontal treatment: a randomized clinical trial. J Clin Periodontol 2008; 35: 877–884.
Christodoulides N, Nikolidakis D, Chondros P, et al. Photodynamic therapy as an adjunct to non-surgical periodontal treatment: a randomized controlled clinical trial. J Periodontol 2008; 79: 1638–1644.
Chondros P, Nikolidakis D, Christodoulides N, Rössler R, Gutknecht N, Sculean A . Photodynamic therapy as adjunct to non-surgical periodontal treatment in patients on periodontal maintenance: a randomized controlled clinical trial. Lasers Med Sci 2008; 24: 681–688.
Herrera D . Insufficient evidence for photodynamic therapy use in periodontitis. Evid Based Dent 2011; 12: 46
Azarpazhooh A, Shah PS, Tenenbaum HC, Goldberg MB . The effect of photodynamic therapy for periodontitis: a systematic review and meta-analysis. J Periodontol 2010; 81: 4–14.
de Oliveira RR, Schwartz-Filho HO, Novaes AB Jr., Taba M Jr . Antimicrobial photodynamic therapy in the non-surgical treatment of aggressive periodontitis: A preliminary randomized controlled clinical study. J Periodontol 2007; 78: 965–973.
Yilmaz S, Kuru B, Kuru L, Noyan U, Argun D, Kadir T . Effect of gallium arsenide diode laser on human periodontal disease: a microbiological and clinical study. Lasers Surg Med 2002; 30: 60–66.
Author information
Authors and Affiliations
Additional information
Address for correspondence: MA Atieh, Sir John Walsh Research Institute, School of Dentistry, University of Otago, PO Box 647, Dunedin, New Zealand. E-mail: maatieh@gmail.com
Atieh MA. Photodynamic therapy as an adjunctive treatment for chronic periodontitis: a meta-analysis. Lasers Med Sci 2010; 25; 605–613. Epub 2009 Dec 19.
Rights and permissions
About this article
Cite this article
Herrera, D. Photodynamic therapy for chronic periodontitis. Evid Based Dent 12, 78–79 (2011). https://doi.org/10.1038/sj.ebd.6400810
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ebd.6400810
