
Abstract
Data sources
Cochrane Oral Health Group Trials Register, the Cochrane Central Register of Controlled Trials (CENTRAL), Medline, Embase, ISI Web of Science, ISI Web of Science Conference Proceedings, BIOSIS, OpenSIGLE. Reference lists of all eligible trials and review articles, and their reference lists were searched.
Study selection
Trials were selected if they met the following criteria: randomised or quasi-randomised controlled trial, involving replacement and repair of amalgam restorations.
Data extraction and synthesis
Titles and abstracts were assessed independently by two authors. Full papers were obtained for relevant articles. Data synthesis was to follow Cochrane Collaboration statistical guidelines.
Results
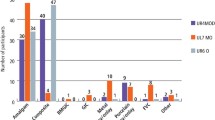
145 potentially eligible studies were identified. Only three studies were analysed further but none of these met the inclusion criteria and all were excluded from this review.
Conclusions
There are no published randomised controlled clinical trials (RCTs) relevant to this review question. There is a need for methodologically sound RCTs reported according to the Consolidated Standards of Reporting Trials (CONSORT) statement (www.consort-statement.org/). Further research needs to explore qualitatively the views of patients on repairing versus replacement and investigate themes around pain, distress and anxiety, time and costs.
Similar content being viewed by others


Commentary
Amalgam has been used for over 200 years. The fact that it is inexpensive, durable, easy to use, presumably biocompatible and somewhat bacteriostatic made it so popular as to revolutionise dentistry when first introduced. The average amalgam may last 5–10 years, and often over 20 years before it needs replacement or repair.
The extensive search, in several ‘English language only’ databases retrieved 145 studies. The very strict selection criteria meant only three RCTs were selected.
A good study design involves minimising all possible sources of bias. In two of the RCTs evaluated, neither random allocation to treatment groups nor blinding of patients was carried out, sample size was poor and need for longer follow-up time necessary. Finally, none of the studies was considered appropriate for inclusion. The authors concluded that there is a need for methodologically sound RCTs.
In one of the studies rejected,1 all of the patients received both repair and replacement fillings. This served as both experimental and control in the same patient. Although the study lacked clear randomisation, it had a number of features which should have made it worthy of consideration. The fact that patients acted as their own controls and the clinicians evaluating the fillings were blinded, may have given the study more power than if it had randomised people more clearly. Another important issue is that of repairing amalgam with amalgam. In many countries the use of amalgam is controversial because of the mercury content and appropriate amalgam disposal. Its use has even been banned in some countries. It is worth noting, that the focus of the review on amalgam repair with only amalgam may have been too narrow.
Resin composites have become a modern day alternative, providing conservation of tooth structure and good sealant properties. The authors of this review have highlighted the need for better RCTs, taking into consideration the new generation of repair materials.
Although the authors found no data available for analysis, and therefore, no definitive answer to the effectiveness of amalgam repair with amalgam vs. amalgam replacement, the review still presented some positive findings. The authors noted that the articles retrieved suggested that repair of restorations could be effective, as survival rate after 2 years was good. Since repairs are less stressful to the patient, take less time to do, and involve less pain and costs, these are findings worthwhile considering.
Practice point
-
Weak evidence suggests that repair of amalgam restorations could be as effective as replacement in the short term. The fact that repairs are less stressful for the patient makes them worthwhile for consideration.
References
Moncada G, Martin J, Fernández E, Hempel MC, Mjör IA, Gordan VV . Sealing, refurbishment and repair of Class I and Class II defective restorations: a three-year clinical trial. J Am Dent Assoc 2009; 140: 425–432.
Author information
Authors and Affiliations
Additional information
Address for correspondence: Luisa Fernandez Mauleffinch, Review Group Co-ordinator, Cochrane Oral Health Group, MANDEC, School of Dentistry, University of Manchester, Higher Cambridge Street, Manchester M15 6FH, UK. E-mail: luisa.fernandez@manchester.ac.uk
Sharif MO, Catleugh M, Merry A, Tickle M, Dunne SM, Brunton P, Aggarwal VR. Replacement versus repair of defective restorations in adults: resin composite. Cochrane Database Syst Rev. 2010; issue 2
Rights and permissions
About this article
Cite this article
Levenson, D., Keenan, A. Defective amalgams – repair or replace?. Evid Based Dent 11, 111 (2010). https://doi.org/10.1038/sj.ebd.6400756
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ebd.6400756
